")
Back to Journals » Risk Management and Healthcare Policy » Volume 13
Health Professionals’ Perception of Psychological Safety in Patients with Coronavirus (COVID-19)
Authors Mohammadi F , Farjam M, Gholampour Y, Tehranineshat B , Oshvandi K, Bijani M
Received 7 May 2020
Accepted for publication 25 June 2020
Published 14 July 2020 Volume 2020:13 Pages 785—794
DOI https://doi.org/10.2147/RMHP.S261410
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Marco Carotenuto
Fateme Mohammadi,1 Mojtaba Farjam,2 Yousef Gholampour,2 Banafsheh Tehranineshat,3 Khodayar Oshvandi,4 Mostafa Bijani5
1Chronic Diseases (Home Care) Research Center and Autism Spectrum Disorders Research Center, School of Nursing and Midwifery, Department of Nursing, Hamadan University of Medical Sciences, Hamadan, Iran; 2Noncommunicable Diseases Research Center (NCDRC), Fasa University of Medical Sciences, Fasa, Iran; 3Community-Based Psychiatric Care Research Center, Department of Nursing, School of Nursing and Midwifery, Shiraz University of Medical Sciences, Shiraz, Iran; 4Mother and Child Care Research Center, School of Nursing and Midwifery, Hamadan University of Medical Sciences, Hamadan, Iran; 5Department of Medical Surgical Nursing, Fasa University of Medical Sciences, Fasa, Iran
Correspondence: Mostafa Bijani
Department of Medical Surgical Nursing, Fasa University of Medical Sciences, Fasa 81936-13119, Iran
Tel +98 9173308451
Email [email protected]
Background: Medical personnel act as the protectors of people’s health by preventing, controlling, and treating emerging diseases, including the coronavirus infection. COVID-19 is a highly infectious and contagious disease which has presented the Iranian healthcare system with a variety of clinical challenges. There is a lack of research on clinical challenges in health crises especially those caused by emerging diseases, hence a need for more exploration of these clinical challenges and dilemmas. The present study aims to determine the different aspects of health professionals’ perception of the psychological safety of patients infected with the coronavirus (COVID-19).
Methods: The present study is a qualitative work which uses conventional content analysis. The participants were 17 health professionals who were responsible for COVID-19 patients and met the inclusion criteria. They were selected via purposeful sampling. The study lasted from February to March 2020. Data were collected through semi-structured, individual interviews which were conducted via video call. The collection of data was kept up to the point of saturation. The collected data were analyzed using the conventional content analysis method.
Results: Three themes such as “respect for dignity”, “comprehensive support” and “peaceful environment” with 11 categories were extracted from the findings of the study.
Conclusion: According to the results of the present study, patients infected with the coronavirus should be given care in a peaceful environment where they receive comprehensive support and have their dignity respected. Such conditions can guarantee the psychological safety of these patients and produce positive behavioral results on their part. Thus, it is essential that the cultural, professional, and organizational prerequisites of protecting all the dimensions of the psychological safety of these patients be provided.
Keywords: Patient Safety, Safety Management, medical personnel, emerging diseases, coronavirus, qualitative research
Background
Safety is essential for humanity’s peace, growth, prosperity, full realization of its potentials, and achievement of virtues.1 Accordingly, in many psychological, sociological, political, and management theories, need for safety is referred to as one of the fundamental needs of humans.2
One of the social environments where safety is of utmost importance is medical centers, including hospitals. In healthcare systems, patient safety has started to receive attention since the latter half of the 1990s and in recent years, it has become a high priority in medical and clinical policies.3,4 Thus, by carefully designing systems and processes, healthcare systems are trying to minimize potentially harmful factors, and patients are at the center of these policies.5 Feeling safe is an essential need of hospitalized patients and vital to feeling well, reducing pain, and improving the quality of care6–10.
In recent years, however, emerging and reemerging viral diseases have threatened the psychological safety of humans in general and patients in particular.11 Emerging diseases are defined as diseases which appear for the first time in a region or the whole world, have high severity, and rapidly affect a large population.11,12 According to World Health Organization, over recent years, more than 30 emerging infections of varying types, extensions, and severities have appeared in different parts of the world.13 And since there is not a specialized treatment for many of these emerging diseases, they take on epidemic or pandemic proportions over wide geographic areas, increase the number of the infected and deaths, and raise medical costs.11
In 2019, a new disease introduced to “COVID-2019” that etiological agent is severe acute respiratory syndrome coronavirus 2: “SARS-CoV-2“started from China and rapidly spread in over 100 countries, including Iran. In addition, COVID-2019 in China, Italy and Iran have similar infection patterns, this disease has killed thousands of people in these countries.14,15 The initial symptoms of the disease are similar to those of influenza, but the infection gradually develops and affects the respiratory, cardiac, and renal systems.The patients who are transferred to medical centers often have signs of dyspnea, tachypnea, and respiratory failure16 There has not been a treatment or vaccine for COVID-2019 up to now and medical personnel can only provide supportive care to the patients.17,18
As the first and most important protectors of people’s health, the medical personnel in the world are faced with various caring and ethical challenges and issues in dealing with this highly infectious and contagious disease. Some studies have shown that caregivers of patients with COVID-2019 are exposed to psychological crises, including stress, anxiety and depression, also physical crises, such as high blood pressure and fatigue.19,20 But one major challenge in caring for COVID-19 patients is protecting their psychological safety which has a direct impact on the quality of care provided to these patients. The present study is the first work of qualitative research addressing the psychological safety of COVID-19 patients in Iran and other countries. Due to the high contagiousness of the disease and quarantine restrictions, it is neither possible nor ethical to explore the concept of psychological safety from the perspective of the patients infected with the coronavirus. The patients’ health professionals who have the closest contact with the patients and spend long periods with them have the best understanding of the patients and their conditions. Accordingly, the focus of the present study is on the health professionals’ perception of the psychological safety of COVID-19 patients in Iran. The researchers hope that the findings of the study will help health administrators and health professionals provide a supportive atmosphere where the rights and dignity of the patients and health professionals are properly respected. The present study aims to determine health professionals’ perception of the psychological safety of patients infected with the coronavirus (COVID-19).
Methods
The present study is a work of qualitative research which relies on conventional content analysis. In qualitative research, conventional content analysis is employed when little is known about the subject under study. As a review of literature showed that the concept of psychological safety of COVID-19 patients had not been studied before, the researchers used the above-mentioned approach.21,22
The participants consisted of 17 health professionals (6 doctors and 11 nurses) who provided care to COVID-19 patients. Selected via purposeful sampling, the participants represented a wide variety in terms of age, gender, work experience, marital status, etc. The inclusion criteria were: being Iranian, having a good command of Farsi, being in practice in an infection unit for COVID-19 patients, and being able to provide adequate and rich information. Data were collected through 17 semi-structured individual interviews and field notes to the point of saturation from February to April 2020. The interviews were conducted at times and places chosen by the participants in the hospitals designated for the coronavirus infection during the epidemic period of the disease in Iran.
Each interview began with a few general questions, including: “Can you describe your typical day of caring for COVID-19 patients?”, “How do you perceive the psychological safety of COVID-19 patients?”, “What factors affect the psychological safety of these patients?”, and “What conditions can threaten their psychological safety?” Subsequently, based on the respondents’ answers to the initial questions, follow-up questions would be asked to add to the clarity of the data: “Can you explain further?”, “What do you mean by that?”, and “Can you give an example?”. The interviews were conducted in line with the main objective of the study. Lasting from 30 to 45 minutes, each interview was immediately transcribed and read and re-read several times by the first author. Data were analyzed immediately after each interview and the next interview was designed based on the information gathered from its predecessors. The interviews were continued to the point where no new categories could be extracted from the data and information on the dimensions of each category had reached saturation. At the same time as they were collected, the data were analyzed using the conventional content analysis method, ie considering the explicit and implied content of the units of meaning, key points were extracted from the text as open codes. Based on their differences and similarities, the codes were categorized this process was continued until themes could be extracted.23
Rigor
The trustworthiness of the data was tested using Lincoln and Guba’s criteria.24 Accordingly, to increase the credibility and accuracy of the data, the researchers used a combination of sources semi-structured interviews, field notes, member check, and peer check. To achieve proportionality, a sampling technique with a maximum variation (age, gender, and work experience) was used. To fulfill the transferability criterion, a full description of the results, the data analysis, and quotations of the participants’ statements were provided.
Ethical Considerations
All participants gave written informed consent to participate in the study and included publication of their responses. The present study was conducted in accordance with the principles of the revised Declaration of Helsinki, a statement of ethical principles which directs physicians and other participants in medical research involving human subjects. Moreover, the study was approved by the local Ethics Committee of Fasa University of Medical Sciences, Fasa, Iran (IR.FUMS.REC.1398.195).
Results
In the present study, 17 health professionals who were responsible for COVID-19 patients in public medical centers were interviewed. The participants consisted of 6 doctors and 11 nurses. Table 1 shows the participants’ demographics.
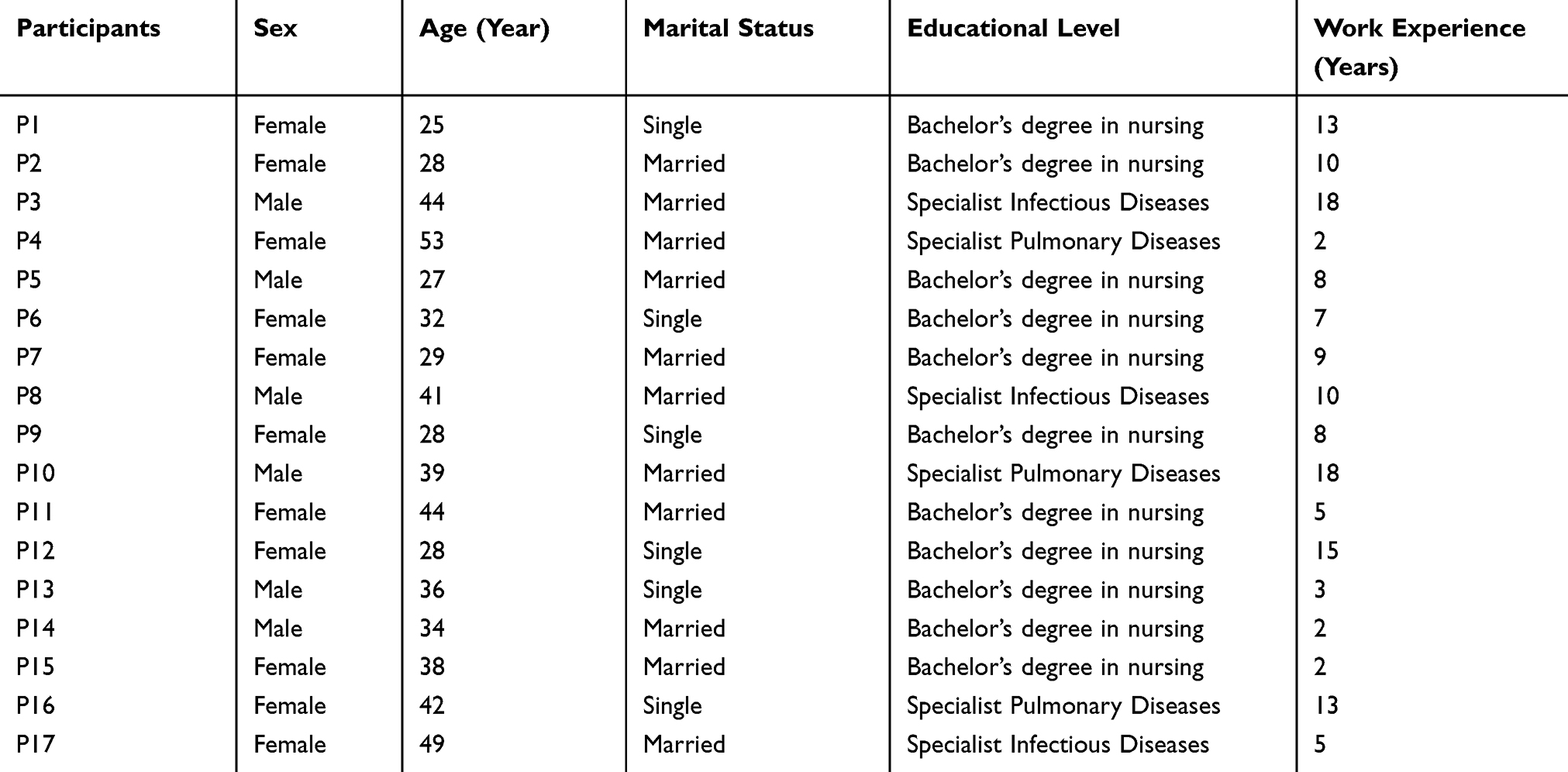 |
Table 1 Individual Social Characteristics of the Participants |
Three main themes “respect for dignity”, “comprehensive support” and “peaceful environment” with 11 categories were extracted from the data (Table 2).
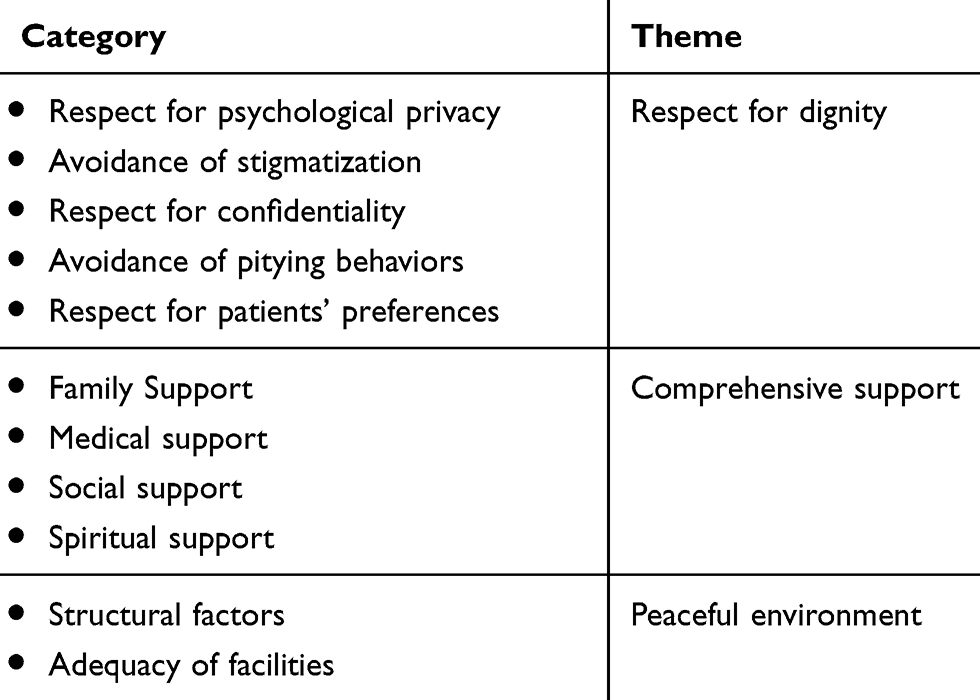 |
Table 2 Themes and Categories Extracted from Content Analysis |
Respect for Dignity
The participants stated that respecting the psychological privacy and confidentiality of hospitalized COVID-19 patients was essential to maintaining their dignity. They also mentioned that it was important to avoid pitying behaviors and labeling the patients (stigmatization) and to provide care in a fair manner. The theme of respect for dignity is comprised of five categories: respect for psychological privacy, respect for confidentiality, avoidance of pitying behaviors, avoidance of stigmatization, and respect for patients’ preferences.
Respect for Psychological Privacy
The interviewed health professionals attached great importance to respecting the psychological privacy of COVID-19 patients. These patients suffer from a disease which is still incurable, have to be under quarantine, and are worried about themselves and their families, all of which facts distress them and occasionally cause the patients or their families to become aggressive toward health professionals’. However, health professionals are expected to understand these patients’ stressful conditions and respect their psychological privacy in their interactions with them.
Conditions are critical here in Iran due to the coronavirus epidemic and the number of the infected is increasing every day. The health professionals are very active and are risking their lives to care for these patients. But we lack equipment and resources and there aren’t enough masks and gloves available. Sometimes, patients have to wait to be tested or when their companions ask for a mask, there aren’t any available. They may get agitated and become aggressive and insult the staff. But the health professionals must understand the conditions the patients and their companions are dealing with and consider their difficult psychological conditions while they are interacting with them. (Participant 2)
Avoidance of Stigmatization
According to the participants, labeling the patients or their families as coronavirus-stricken can threaten the social relationships of the patients and their families even after recovery and put their psychological safety at risk.
Right after an individual tests positive for coronavirus, all their family members are tested too and their home is disinfected. Often, family members test negative and are not infected. Healthy family members and recovered patients return home of course. But people avoid them because of their terror and may even stop them from entering their neighborhood and stores and label them coronavirus carriers. Such behaviors cause emotional distress to the patients and their families. (Participant 17)
Respect for Confidentiality
In addition, the participants mentioned that health professionals must not reveal information about the patients and their medical conditions and the number of deaths via photos or videos on social media. They stressed that the medical personnel must not disclose this information to anyone except the authorities.
In this coronavirus crisis, though it is important to keep people informed about the critical conditions in the country, maintaining patient confidentiality is still essential. The health professionals should not spread any personal or public information related to the number of the infected, deaths, or the patients’ identity on social media. This kind of information should be revealed only through medical and legal channels. The medical information of these patients will remain confidential and their psychological safety and the psychological safety of their families will be respected. (Participant 5)
Avoidance of Pitying Behaviors
From the participants’ perspective, to maintain the dignity of these patients, especially those whose condition is critical, health professionals should avoid taking undue pity on them.
Some of the patients are from the slums or are peddlers who live and work in unpleasant financial and environmental conditions. They are admitted and given care when they are in critical conditions. Well, in this crisis, these people are at higher risk of getting the disease. Even before this, you felt sorry for them when you saw them. However, in their interactions with these patients, the medical personnel should avoid pitying behaviors or looks despite the fact that they feel sympathetic towards them. (Participant 10)
Respect for Patients’ Preferences
Showing respect for the COVID-19 patients’ preferences is another important category under the theme of respect for their dignity. The health professionals believed that the patients’ preferences and decisions regarding self-care, being quarantined at home, and religious beliefs should be respected.
Some of the patients in better health conditions have medical education or are highly-educated and wealthy and it is possible for them to be quarantined at home and continue the process of their recovery there. Maybe those can be allowed to decide where they want to be quarantined. This can even raise their chances of recovery as they won’t have to be near other patients infected with the virus and they will have more peace and feel that their dignity has been respected. (Participant 15)
Comprehensive Support
Based on the participants’ responses, comprehensive support of patients infected with the coronavirus is a key factor in maintaining and improving their psychological safety. Accordingly, these patients must be provided with full family, medical, social, and spiritual support. This theme consists of four categories: family support, medical support, social support, and spiritual support.
Family Support
The participants stated that family support is crucial to patients’ psychological safety, especially the respect that children show their infected parents and their willingness to stay with them and help with caring for them despite the fact that COVID-19 is highly contagious.
The families of the infected patients won’t leave their patients alone; especially the children of those who are not in critical conditions insist that they will take all precautions to be allowed to stay with their parents. This makes the patients who are infected with the coronavirus, especially the older ones, feel better and be more cooperative in their treatment and thus have better psychological safety. (Participant 4)
Medical Support
The participants also referred to the role of health professionals in improving the psychological safety of COVID-19 patients: as the most important and closest individuals to these patients, health professionals are in constant contact with the patients and can, through kind behaviors, create a sense of safety for them in their critical conditions.
The medical personnel (the doctors and the nurses) don’t leave the patients alone for a second even when it’s very dangerous to be close to them. Even when the patients are very depressed and start to cry, they give them hugs and try to soothe them and this makes the patients feel more peaceful and secure. (Participant 1)
Social Support
According to the participants, this disease has terrified people and caused them to ostracize the infected. Social support of the patients by public and non-profit organizations in the form of educating the public about COVID-19 and how to interact with the infected and providing medical and sanitary equipment and facilities can contribute to the psychological safety of the patients in the society.
This disease has created a lot of fear in people. Organizations run by the government and NGOs can inform people about the disease, its incubation period, and the manner of dealing with the infected before and after recovery so people can overcome their fear and behave more appropriately toward the patients and their families, especially after they recover. This way, the patients will feel better. On the other hand, the government and NGOs have started to supply medical masks and gowns and other protective equipment. Well, these social bodies have been able to decrease people’s terror to a great extent and teach them that by taking precautions, they can interact with the patients more respectfully and support them in this crisis. (Participant 9)
Spiritual Support
Another source of support referred to by the participants was the COVID-19 patients’ belief in God and His blessings: the patients perceive God as having supernatural powers and control over every aspect of their lives and a reliable source of support which will help them get over these hard times with the hope of recovery.
On many occasions I’ve seen patients whispering prayers and asking God to be cured. They also ask us to pray for their recovery. Their belief in God and divine powers gives them feelings of peace and safety. (Participant. 12)
Peaceful Environment
According to the participants, since patients infected with the coronavirus have to stay for 2–3 weeks in the infection units designated for COVID-19 patients and their physical contact with the outside world is forbidden, a well-structured environment with adequate and satisfactory facilities can help them have peace and psychological safety. This theme has two categories: structural factors and adequacy of facilities.
Structural Factors
The health professionals stated that the areas designated for COVID-19 patients—both those whose conditions are critical and are in intensive care units and those whose cases are mild—must have a proper structure in terms of hygiene, temperature, silence, and bed so that the patients can have peace in those environments and be willing to receive care there.
It is true that this infection was so sudden and has become widespread and the number of the infected is huge, but we need clinical environments with a good structure—they should be clean and quiet, air-conditioned, and regularly disinfected. This will make the patients feel secure and want to stay in this environment. (Participant 15)
Adequacy of Facilities
The participants stated that facilities which match the patients’ age groups, including access to the Internet, television, books, etc. are integral to a peaceful environment and the psychological safety of the patients.
We should allow the patients, as long as it is safe, to have access to at least one or two things which entertain them in the ward. For example, all the patients have cellphones which are properly disinfected and then returned to them. They also have access to free Internet and television so they can have more fun, comfort, and peace in the clinical environment. (Participant 13)
Discussion
Caring for patients suffering from emerging or reemerging diseases is a taxing job posing myriad clinical challenges to health professionals.25,26 One major clinical challenge in caring for patients, especially those infected with the coronavirus, is maintaining and improving their psychological safety.27 Health professionals are expected to respect and consider their patients’ psychological safety as an important of their job.4 The COVID-19 pandemic which has spread in over 100 countries and is responsible for the infection and death of an increasing number of people has created such terror of the disease and the infected that the psychological safety of the patients in medical centers and the society is at risk. Thus, the present study was an attempt at determining health professionals’ perception of the psychological safety of the patients infected with the virus. Three main themes were extracted from the collected data: respect for dignity, comprehensive support, and peaceful environment.
Respecting the dignity of hospitalized patients is an important responsibility of health professionals and is essential to maintaining their psychological safety.21,28 In the present study, the theme of respect for the dignity of COVID-19 patients was found to be comprised of five categories: respect for psychological privacy, respect for confidentiality, avoidance of pitying behaviors, avoidance of stigmatization, and respect for preferences.28,29
Similarly, recent studies in Iran stress the significance of respecting patients’ dignity, psychological privacy, and confidentiality in systematic and ethical care, which is indicative of the high status of patient dignity in Iranian cultures. However, these studies report that, occasionally, due to work overload, extended and consecutive shifts, and shortage of workforce and equipment, health professionals fail to provide ethical care which demands respect for patient dignity.28,30,31
However, in Iran, as a result of the common cultural beliefs, the current environmental conditions, and insufficiency of medicine and equipment due to the sanction, COVD-19 patients are experiencing increased tension in the life-and-death situation they are in. The patients and their families are given such labels as “corona-stricken” and avoided by people. All this psychological tension causes the patients and their families to occasionally lose control over their thoughts and behaviors and become aggressive towards the medical teams. Health professionals are expected to understand their situation, avoid stigmatizing them, and treat them kindly toward maintaining their dignity. Yet, at times, health professionals grow impatient with the patients’ disrespectful manners and react harshly, which threatens the patients’ psychological safety. The interviewed health professionals mentioned that it is important to the patients and their families that their identity and medical information remain confidential and out of reach of the non-medical staff and other patients. Only authorities should be allowed to announce the number of the infected and deaths without revealing any names. Similarly, many other studies stress the importance of maintaining patient confidentiality as a main aspect of respect for patient dignity.32–34
Avoidance of pitying behaviors is another important category extracted from the data. Even though sympathizing with patients is a significant aspect of the supportive role of health professionals, they need to avoid pitying looks and words or any extreme compassion and kindness that destroys human’s dignity. Inappropriate pitying may make COVID-19 patients disturbed and aggressive and undermine their self-confidence. Studies show that sympathizing with patients helps them feel better and get over the hard part of their diseases more easily, but inappropriate expressions of pity are detrimental to the patients’ self-confidence and psychological safety.10 Although, health professionals, due to the care of these patients have reported more fatigue, depression and stress than before the coronavirus crisis but health professionals are the most important people who have close interaction and communication with patients with COVID 2019, therefore, they play an important and key role in providing psychological support and empathy to these patients. Interaction, kindness, conversation, and empathy away from pity improve patients’ senses.35,36
According to the participants’ views, showing respect for the preferences of patients infected with the coronavirus is very important to maintaining and improving their psychological safety. The health professionals should respect the patients’ decisions regarding their type of treatment and, if possible, the location of their stay in the hospital or at home. Considering the facts that many people have become infected and medical environments are contaminated, patients in good financial conditions and the possibility to receive care at home in rooms separate from their families should be allowed to recover at home under the care of a family member or a private health professionals. These conditions will minimize their exposure to the coronavirus and assure them that they are less likely to transfer their disease to their families or the medical personnel. This will give the patients more peace and psychological safety. The study of Matiti (2008) shows that in order for patient dignity to be maintained, patients should be allowed to participate in their medical decision-making process, which is consistent with the findings of the present study.37 Likewise, Bagheri et al (2012) refer to the participation of patients with cardiac diseases in their treatment plans as the most important factor in maintaining their dignity.29 Thus, it is likely that allowing COVID-19 patients to participate in the making of medical decisions which apply to them will cause them to feel more valuable and psychologically secure.
Another theme extracted from the data is comprehensive support of COVID-19 patients. The participants stated that full support (family, medical, social, and spiritual support) of the patients is an important factor in maintaining and improving their psychological safety. Family members, as the most important sources of support for patients, play a vital role in their care. Even when the infected patients are receiving care from the healthcare system, the support of the family continues and makes the members feel closer to each other.38 In a similar vein, many studies report that family and social support of patients, regardless of their disease, facilitates their adaptation to their condition, thereby improving their psychological safety.27 Similarly, the study of Bailey et al shows that family support reduces patients’ anxiety and helps them adapt to their disease and feel better.39
Another source of support referred to by the participants is the health professionals who can inspire the patients with hope by being kind to them and smiling at them. Also, by singing and playing music for the patients, health professionals help improve the patients’ morale and sense of psychological safety. Hearing the soothing and reassuring words of the doctors and nurses reduces fear and anxiety in the patients and largely satisfies their need for psychological safety.40 Similarly, Mollon et al stress the supportive role of medical personnel in alleviating the pain and suffering of patients.41
The participants also mentioned that social support, both from the government and non-governmental organizations, can prove very effective in controlling the coronavirus crisis, reducing anxiety, and consequently improving the psychological safety of the infected. Along the same lines, many other studies report that social organizations and bodies which support hospitalized patients and vulnerable groups in the society play an important role in the enhancement of the psychological safety of patients.10,27,32
In the present study, another category under the theme of comprehensive care is spiritual support which is perceived as divine blessings and help from supernatural sources. As the essence of humanity, spirituality is visible in humans’ interactions with God, including prayers and invocations, which are performed in the hope of achieving love, faith, and hope.42,43 Though there is mention of the contribution of spiritual support to creating peace and comfort in patients in several studies, divine support, as a factor in psychological safety, has received little attention. The Iranians’ strong religious beliefs account for their perception of divine support as a major factor in their achievement of psychological safety.
The final theme extracted from the data in the present study is peaceful environment with the categories of structural factors and adequacy of facilities. The equipment in the environment where patients are cared for plays a key role in their achievement of psychological safety.41,44 Contracting a disease and being placed in the unfamiliar environment of a hospital result in patients’ feeling terrified and insecure, a common cause of stress for patients. An unsatisfactory structure in a clinical environment has an adverse effect on the physical and psychological well-being of patients.1,10,27 On the other hand, studies report that a proper structure in clinical environments, including good light, ventilation, cleanliness, and silence, has a positive impact on the recovery of patients, which is consistent with the findings of the present study. Structural factors become especially important in the case of patients with special conditions or a critical illness.45
Adequacy of facilities, the other dimension of peaceful environment, refers to access to comforts and entertainment. Over time, mankind has become increasingly dependent on digital and electronic devices for entertainment and losing access to these facilities can be stressful. The participants believed that there is need for easy access to modern means of entertainment in the units designated for COVID-19 patients. In a similar vein, Nadighara et al (2016) state that access to facilities significantly contributes to patients’ feeling secure.46
In conclusion, maintaining and improving the psychological safety of COVID-19 patients in Iran is a major challenge in providing high-quality care to these patients. From the perspective of the participants of the present study, to feel psychologically secure, the patients infected with the coronavirus should be given comprehensive support, have their dignity respected, and receive care in a peaceful environment.
Limitations
One of the limitations of the present study is that, due to the very high contagiousness of COVID-19, data were collected only through individual interviews via video call. It is suggested that future studies employ other methods of collecting qualitative data, including field notes, observation, and focus group interviews, to add to the richness of the collected data.
Conclusion
The spread of the COVID-19 pandemic in all the provinces of Iran and the increasing number of the infected and deaths has posed the most serious clinical challenge to the healthcare system in the present decade. Meanwhile, maintaining and enhancing the psychological safety of the infected is an important issue in this crisis, thus the need for identifying and understanding the factors which threaten the psychological safety of these patients. The findings of the present study show that receiving care in a peaceful environment where their dignity is respected and they are given comprehensive support is central to the patients’ achievement of psychological safety. It follows that there is an urgent need for proper cultural, professional, and organizational efforts to provide COVID-19 patients with an environment where they are given care while their psychological safety is respected. Health officials and policy-makers can use the findings of the present study to create a supportive environment free of clinical tension which addresses the various aspects of the psychological safety of patients to provide high-quality care.
Acknowledgment
This paper was extracted from a research project with the ethical code (IR.FUMS.REC.1398.195) in Fasa University of Medical Sciences, Fasa, Iran. The authors appreciate Fasa University of Medical Sciences for financially supporting this research.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Jamalimoghadam N, Yektatalab S, Momennasab M, Ebadi A, Najaf Z. How do hospitalized adolescents feel safe? A qualitative study. J Nurs Res. 2019;27(2):e14. doi:10.1097/jnr.0000000000000285
2. Melender HL, Lauri S. Experiences of security associated with pregnancy and childbirth: a study of pregnant women. Int J Nurs Pract. 2002;8(6):289–296. doi:10.1046/j.1440-172X.2002.00382.x
3. Glasper A, Coad J, Richardson J. Children and Young People’s Nursing at a Glance. John Wiley & Sons; 2014.
4. Sadeghi T, Dehghan Nayyeri N, Karimi R. Nursing-patient relationship: a comparison between nurses and adolescents perceptions. Iran J Med Ethics Hist Med. 2011;4(3):69–78.
5. Nieva V, Sorra J. Safety culture assessment: a tool for improving patient safety in healthcare organizations. BMJ Qual Saf. 2003;12(suppl2):ii17–ii23. doi:10.1136/qhc.12.suppl_2.ii17
6. Adib-Hajbaghery M, Aghajani M. Patients dignity in nursing. Nurs Midwifery Stud. 2015.
7. Baillie L, Matiti M. Dignity, equality and diversity: an exploration of how discriminatory behaviour of healthcare workers affects patient dignity. Diversity Health Soc Care. 2013;10(1):5–12.
8. Manookian A, Cheraghi MA, Nasrabadi AN. Factors influencing patients’ dignity: a qualitative study. Nurs Ethics. 2014;21(3):323–334. doi:10.1177/0969733013498526
9. Mohammadi F, Bijani M, Cheraghi F, Kyle H. Dignity: the cornerstone of nursing care among hospitalized mothers of infants in Neonatal Intensive Care Unit. J Perinatal Neonatal Nurs. 2020;26(7–8):22–31.
10. Mohammadi F, Rakhshan M, Molazem Z, Zareh N, Gillespie M. Caregivers’ perception of dignity in teenagers with autism spectrum disorder. Nurs Ethics. 2019;26(7–8):2035–2046. doi:10.1177/0969733018796679
11. Borycki E, Cummings E, Dexheimer J, et al. Patient-centred coordinated care in times of emerging diseases and epidemics. Yearb Med Inform. 2015;24(01):207–215. doi:10.15265/IY-2015-019
12. Suwantarat N, Apisarnthanarak A. Risks to healthcare workers with emerging diseases: lessons from MERS-CoV, Ebola, SARS, and avian flu. Curr Opin Infect Dis. 2015;28(4):349–361. doi:10.1097/QCO.0000000000000183
13. Elo S, Kyngäs H. The qualitative content analysis process. J Adv Nurs. 2008;62(1):107–115. doi:10.1111/j.1365-2648.2007.04569.x
14. Coronavirus disease 2019 (COVID-19) Situation Report – 46. Word Health Organization; 2020. Available from: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200306-sitrep-46-covid-19.pdf?sfvrsn=96b04adf_2.
15. Sorbello M, El-Boghdadly K, Di Giacinto I, et al. The Italian coronavirus disease 2019 outbreak: recommendations from clinical practice. Anaesthesia. 2020;75:724–732. doi:10.1111/anae.15049
16. Wu Z, McGoogan JM Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: summary of a report of 72 314 cases from the Chinese Center for Disease Control and Prevention. JAMA. 2020.
17. Ai T, Yang Z, Hou H et al. Correlation of chest CT and RT-PCR testing in coronavirus disease 2019 (COVID-19) in China: a report of 1014 cases. Radiology. 2020:200642.
18. Lai -C-C, Shih T-P, Ko W-C, Tang H-J, Hsueh P-R. Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and corona virus disease-2019 (COVID-19): the epidemic and the challenges. Int J Antimicrob Agents. 2020;55(3):105924. doi:10.1016/j.ijantimicag.2020.105924
19. Chew NW, Lee GK, Tan BY, et al. A multinational, multicentre study on the psychological outcomes and associated physical symptoms amongst healthcare workers during COVID-19 outbreak. Brain Behav Immun. 2020.
20. Tan BY, Chew NW, Lee GK, et al. Psychological impact of the COVID-19 pandemic on health care workers in Singapore. Ann Intern Med. 2020.
21. Mohammadi F, Oshvandi K. Male nursing students’ perception of dignity in neonatal intensive care units. Nurs Ethics. 2019:0969733019848040.
22. Wildemuth BM. Applications of Social Research Methods to Questions in Information and Library Science. ABC-CLIO; 2016.
23. Speziale HS, Streubert HJ, Carpenter DR. Qualitative Research in Nursing: Advancing the Humanistic Imperative. Lippincott Williams & Wilkins; 2011.
24. Guba EG, Lincoln YS. Competing paradigms in qualitative research. Handbook Qual Res. 1994;2(163–194):105.
25. Dikid T, Jain S, Sharma A, Kumar A, Emerging NJ. Re-emerging infections in India: an overview. Indian J Med Res. 2013;138(1):19.
26. Hessels AJ, Kelly AM, Chen L, Cohen B, Zachariah P, Larson EL. Impact of infectious exposures and outbreaks on nurse and infection preventionist workload. Am J Infect Control. 2019;47(6):623–627. doi:10.1016/j.ajic.2019.02.007
27. Jamalimoghadam N, Yektatalab S, Momennasab M, Ebadi A, Zare N. Hospitalized adolescents’ perception of dignity: a qualitative study. Nurs Ethics. 2019;26(3):728–737. doi:10.1177/0969733017720828
28. Ebrahimi H, Torabizadeh C, Mohammadi E, Valizadeh S. Patients’ perception of dignity in Iranian healthcare settings: a qualitative content analysis. J Med Ethics. 2012;38(12):723–728. doi:10.1136/medethics-2011-100396
29. Bagheri H, Yaghmaei F, Ashktorab T, Zayeri F. Patient dignity and its related factors in heart failure patients. Nurs Ethics. 2012;19(3):316–327. doi:10.1177/0969733011425970
30. Mason VM, Leslie G, Clark K, et al. Compassion fatigue, moral distress, and work engagement in surgical intensive care unit trauma nurses: a pilot study. Dimen Crit Care Nurs. 2014;33(4):215–225. doi:10.1097/DCC.0000000000000056
31. Shorideh FA, Ashktorab T, Yaghmaei F. Iranian intensive care unit nurses’ moral distress: a content analysis. Nurs Ethics. 2012;19(4):464–478. doi:10.1177/0969733012437988
32. Mohammadi F, Tabatabaei H, Mozafari F, Gillespie M. Caregivers’ perception of women’s dignity in the delivery room: a qualitative study. Nurs Ethics. 2020;27(1):116–126. doi:10.1177/0969733019834975
33. Webster C, Bryan K. Older people’s views of dignity and how it can be promoted in a hospital environment. J Clin Nurs. 2009;18(12):1784–1792. doi:10.1111/j.1365-2702.2008.02674.x
34. Woogara J. Privacy and dignity of cancer patients: a qualitative study of patients privacy in UK National Health Service patient care settings. J Cancer Educ. 2005;20(2):119–123. doi:10.1207/s15430154jce2002_14
35. Legido-Quigley H, Asgari N, Teo YY, et al. Are high-performing health systems resilient against the COVID-19 epidemic? The Lancet. 2020;395(10227):848–850. doi:10.1016/S0140-6736(20)30551-1
36. Sasangohar F, Jones SL, Masud FN, Vahidy FS, Kash BA. Provider Burnout and Fatigue During the COVID-19. pandemic: lessons learned from a high-volume intensive care unit. Anesthesia and analgesia; 2020.
37. Matiti MR, Trorey GM. Patients’ expectations of the maintenance of their dignity. J Clin Nurs. 2008;17(20):2709–2717. doi:10.1111/j.1365-2702.2008.02365.x
38. Gooding JS, Cooper LG, Blaine AI, Franck LS, Howse JL, Berns SD. Family Support and Family-Centered Care in the Neonatal Intensive Care Unit: Origins, Advances, Impact. Seminars in Perinatology. Elsevier; 2011.
39. Bailey JJ, Sabbagh M, Loiselle CG, Boileau J, McVey L. Supporting families in the ICU: a descriptive correlational study of informational support, anxiety, and satisfaction with care. Intensive Crit Care Nurs. 2010;26(2):114–122. doi:10.1016/j.iccn.2009.12.006
40. Wassenaar A, Schouten J, Schoonhoven L. Factors promoting intensive care patients’ perception of feeling safe: a systematic review. Int J Nurs Stud. 2014;51(2):261–273. doi:10.1016/j.ijnurstu.2013.07.003
41. Mollon D. Feeling safe during an inpatient hospitalization: a concept analysis. J Adv Nurs. 2014;70(8):1727–1737. doi:10.1111/jan.12348
42. Bingham VL. The Recovery Experience for Persons with a Myocardial Infarction and Their Spouses/Partners. The University of Alabama at Birmingham; 2007.
43. Rankin EA, DeLashmutt MB. Finding spirituality and nursing presence: the student’s challenge. J Holistic Nurs. 2006;24(4):282–288. doi:10.1177/0898010106294423
44. Avdagic M, Carlström E. The path to patient safety in primary health care—a study of nurses’ and general practitioners’ perceptions in Sweden. J Nurs Educ Pract. 2014;4(7):85–94. doi:10.5430/jnep.v4n7p85
45. Schweitzer M, Gilpin L, Frampton S. Healing spaces: elements of environmental design that make an impact on health. J Altern Compl Med. 2004;10(Supplement1):
46. Nadighara AA, Abedi G, Abedi E, Designing RF. Validating a scale to measure the sense of security in hospitalized patients. J Mazandaran Univ Med Sci. 2016;26(139):178–189.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.