")
Back to Journals » Advances in Medical Education and Practice » Volume 11
Health Professionals’ Readiness and Its Associated Factors to Implement Electronic Medical Record System in Four Selected Primary Hospitals in Ethiopia
Authors Awol SM , Birhanu AY, Mekonnen ZA , Gashu KD , Shiferaw AM, Endehabtu BF , Kalayou MH , Guadie HA, Tilahun B
Received 3 October 2019
Accepted for publication 4 January 2020
Published 21 February 2020 Volume 2020:11 Pages 147—154
DOI https://doi.org/10.2147/AMEP.S233368
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Balakrishnan Nair
Shekur Mohammed Awol, 1 Abreham Yeneneh Birhanu, 1 Zeleke Abebaw Mekonnen, 1, 2 Kassahun Dessie Gashu, 1 Atsede Mazengia Shiferaw, 1 Berhanu Fikadie Endehabtu, 1 Mulugeta Haylom Kalayou, 1 Habtamu Alganeh Guadie, 1 Binyam Tilahun 1
1Department of Health Informatics, Institute of Public Health, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia; 2Health Systems Directorate, Ministry of Health, Addis Ababa, Ethiopia
Correspondence: Berhanu Fikadie Endehabtu
Department of Health Informatics, Institute of Public Health, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia
Tel +251921013129
Email [email protected]
Background: Incorporating electronic medical record systems (EMRs) into the healthcare system is not only about modernizing the health system, but is about saving lives by facilitating communication and practicing evidence-based decision. Globally, more than 50% of EMR projects fail before they reach their target. Even though EMRs are an essential tool for health care, their adoption and utilization remains low in developing countries including Ethiopia.
Objective: The aim of this study was to determine health professionals’ readiness and associated factors toward the implementation of EMRs in four selected primary hospitals in Ethiopia.
Methods: An institutionbased cross-sectional study supplemented with a qualitative approach was conducted on 414 health professionals from March 2 to May 5, 2018 in four selected primary hospitals in Ethiopia. A self-administered questionnaire was used to collect the quantitative data and in-depth interviews were employed for the qualitative data. The data were analyzed using SPSS version 20 software. Descriptive statistics, bivariable, and multivariable logistic regression analyses were done. An adjusted odds ratio (AOR) with 95% CI was used to determine the association between the determinants and the outcome variable.
Results: More than half (258; 62.3%) of health professionals were ready to use the electronic medical recording system. EMR knowledge (AOR = 2.64; 95% CI: [1.62, 4.29]), attitude (AOR = 1.63; 95% CI: [1.01, 2.63]), computer literacy (AOR = 3.30; 95% CI: [2.05, 5.31]), and EMR training (AOR = 3.63, ;5% CI: [1.69, 5.80]) were significantly associated with EMR readiness.
Conclusion and Recommendation: In general, the overall readiness of health professionals for EMR implementation was found to be low. Comprehensive packages of capacity-building are crucial to raise the level of knowledge, attitude, and computer skill among health workers.
Keywords: electronic medical record system, EMR implementation, readiness, health professionals, Ethiopia
Introduction
Information communication technologies (ICTs) are currently being used in developed and developing countries to improve access, effectiveness, and efficiency of health care.1 The electronic medical record system (EMR) as one of the supportive systems has great potential to address the main challenges of healthcare systems.2 Incorporating EMRs into the healthcare system is not all about modernizing the health system, but is about saving lives by facilitating communication and practicing evidence-based decision-making.3
Even though the EMR is an essential tool for the healthcare sector, the adoption and utilization of EMRs remains low in developing countries.4 Numerous healthcare facilities across the globe have implemented EMR systems to improve the information recording process, but only a few have been successful.5
The percentages of failures are alarmingly higher in adoption to meet the desired benefits from the implementation. Globally, more than 50% of EMRs projects failed before they reached their target.6 However, there is significant variation across countries. More than 90% of healthcare institutions in Denmark have fully functioning EMRs.4 More than 70% in Canada, less than 25% in Chile, about 50% in China, less than 30% in Iran, and more than 60% in Botswana of their health are institutions have successfully implemented EMRs.4
A study conducted in Afghanistan Bamyan on health needs and eHealth readiness assessment of healthcare organizations found that core readiness for EMR system was 66.7%.7 A study conducted in Iran also showed the overall readiness of health professionals on EMRs implementation was 57.2%.8
As in many countries, the Ethiopian Ministry of Health has recognized the importance of ICT for quality improvement in healthcare provision. In 2013, the Ethiopian Ministry of Health adapted an EMR and planned to scale it up to all hospitals,9 but few healthcare institutions implemented EMRs. A study conducted at three hospitals in North West Ethiopia showed the overall readiness of health professionals was 54.1%.10
Multiple reasons are given for low EMR adoption, such as resistance, opposition in changing from the paper-based systems to electronic systems, lack of pre-implementation preparations, lack of organizational readiness, unavailability of technology, funding and lack of technical and computer skills of personnel.11–13
The successful introduction of EMR in health care requires the examination of complex technical, organizational, infrastructural, and human factors.14 Adoption of eHealth is a change process which is not purely a technical process, rather demanding many behavioral modifications in the work environment for health workers.15 Any contradictory points need to be addressed before starting any eHealth project.16,17 Studies show that preparedness of healthcare providers can play an important role in the adoption of electronic health records.18
Readiness assessment, as a comprehensive measure in order to provide a proper image of existing conditions and the preparedness of healthcare organization to change, is also a way to identify potential causes of failure in innovation.19 This study therefore aims to assess the readiness and associated factors among health professionals towardEMR implementation in the selected hospitals.
Methods
Study Design and Setting
An institutional-based cross-sectional study was conducted from March 2, 2018 to May 5, 2018 in four selected primary hospitals in Ethiopia. Those four primary hospitals were Assosa, Hidar 11, Sanja, and Wogera which are 686, 500, 806, and 775 km from Addis Ababa (the capital city), respectively.
Sample Size, Study Participants, and Sampling Procedure
The sample size was calculated using a single population proportion formula, considering the following assumptions: 54.1% prevalence of EMR readiness in North Gondar, Ethiopia,10 95% level of confidence, 5% margin of error, and 10% non-response rate. Finally, a minimum sample size of 418 was obtained. All the 451 health professionals who were working in four selected primary hospitals (135 at Hidar 11 hospital, 59 at Sanja hospital, 47 at Wogera hospital, and 210 at Assosa hospital) were included in the study. Health professionals who had been practicing for less than six months in that hospital were excluded from the study. For the qualitative in-depth interview, eight key informants were included until saturation of required information was reached.
Data Collection Tool and Procedure
Quantitative data were collected using a self-administered questionnaire. Socio-demographic, behavioral, technical, and organizational variables were included in the questionnaire. Qualitative data were collected using in-depth interviews; the in-depth interview included eight key informants. Unit heads in the hospital were involved as the key informant in the in-depth interview. Six health information technicians who have good communication skills were recruited for data collection and three health officers with experience of research work supervised the data collection process.
One-day training was given for data collectors and supervisors on the objective of the study, data collection procedures, data collecting tools, respondents' approach, data confidentiality, and respondents' right prior to the data collection date.
Before the actual data collection, pretesting of the questionnaire was conducted in 45 health professionals at Gondar university hospital.
The pretest was conducted outside the study area but with similar characteristics to actual study participants. The necessary corrections were done based on the pretest findings.
Data Processing and Analysis
Data were analyzed using Statistical Package for Social Science (SPSS) version 20. Descriptive analyses were computed for different variables in the study. Bivariate logistic regression analysis was used to identify statistically significant independent variables to be included for the final model at a P value of 0.05. Multivariate logistic regression analysis analyses were carried out in order to assess the association between readiness and various explanatory variables after controlling for the effect of confounding variables. Adjusted odds ratios (AORs) and 95% confidence intervals (CIs) were calculated for each independent variable with health professional readiness as the dependent variable. The qualitative data collected using in-depth interview have been transcribed into text in the Amharic language and the Amharic text translated into English, then open code software was used for analysis using thematic analysis.
Operational Definition
In this study core readiness and engagement readiness were measured by a set of composite scores comprising four questions for each. Core readiness is defined as the realization of needs and expressed dissatisfaction with the current way of working, such as inefficient documentation, patient privacy, and data confidentiality.10 Engagement readiness is defined as active willingness for EMR implementation and volunteering to take necessary training for EMR.20
A study participant who scored 50% or more for core readiness and engagement readiness questions is assumed to have core readiness and engagement readiness, respectively.10 Overall readiness is the intersection of core readiness and engagement readiness. A health professional is said to have overall readiness if he or she has both engagement readiness and core readiness.20
We measured knowledge and attitude as a latent variable using composite items that address the usefulness and applicability of EMR for end users to facilitate their clinical work flow. Study participants who score 50% or more for the knowledge question were categorized as having good knowledge.10 Study participants who score median and above in the five-point Likert scale of attitude questions were categorized as favorable for EMR.21
Ethical Consideration
Informed verbal consent was accepted for this particular study and approved by the ethical review board of the University of Gondar.
Results
Socio-Demographic Characteristics of Study Participants
A total of 451 health professionals participated in the study with a response rate of 91.8%. Nearly half (212; 51.2%) of the participants were male. Nearly half (218; 52.7%) of the study participants were between the ages of 25 and 29. More than half (230; 55%) of the participants had a degree and only 13 (3.1%) of them had an MSc and above. More than-one third (157; 37.9%) of the study participants were nurses, 50 (12.1%) were medical doctors, and only 3 (0.7%) were optometrists. About 143 (34.5%) of the study participants had less than two years' working experience, whereas 128 (30.9%) had more than five years' working experience (Table 1).
 |
Table 1 Socio-Demographic Characteristics of Health Professionals in Four Primary Hospitals of Ethiopia, 2018 |
Readiness of Health Professionals for EMRs
From all study participants, 258 (62.3%), 95% CI (57.7, 66.9) had overall readiness for an EMR system (Figure 1). Among all the study participants, 274 (66.2%) had core readiness whereas 270 (65.2%) had engagement readiness (Figure 1).
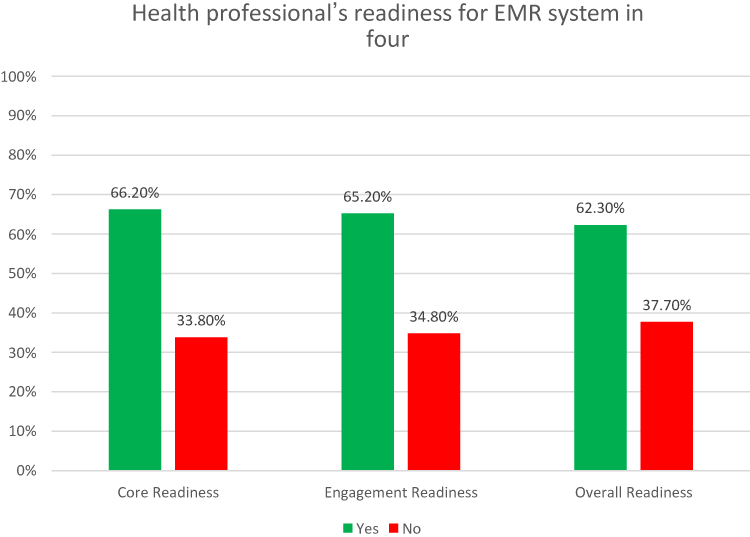 |
Figure 1 Core and engagement readiness of health professionals for EMR system in four primary hospitals, Ethiopia, 2018. |
The readiness of health professionals on the EMR system varies across work experience, age, educational status, and professional categories. Above two-thirds (64.1%) of respondents with five and above years of work experience had readiness on the EMR system. All study participants with a second degree and above were ready to use EMR systems. The majority (74%) of medical doctors and nurses (61%) were ready to use EMR systems (Table 2).
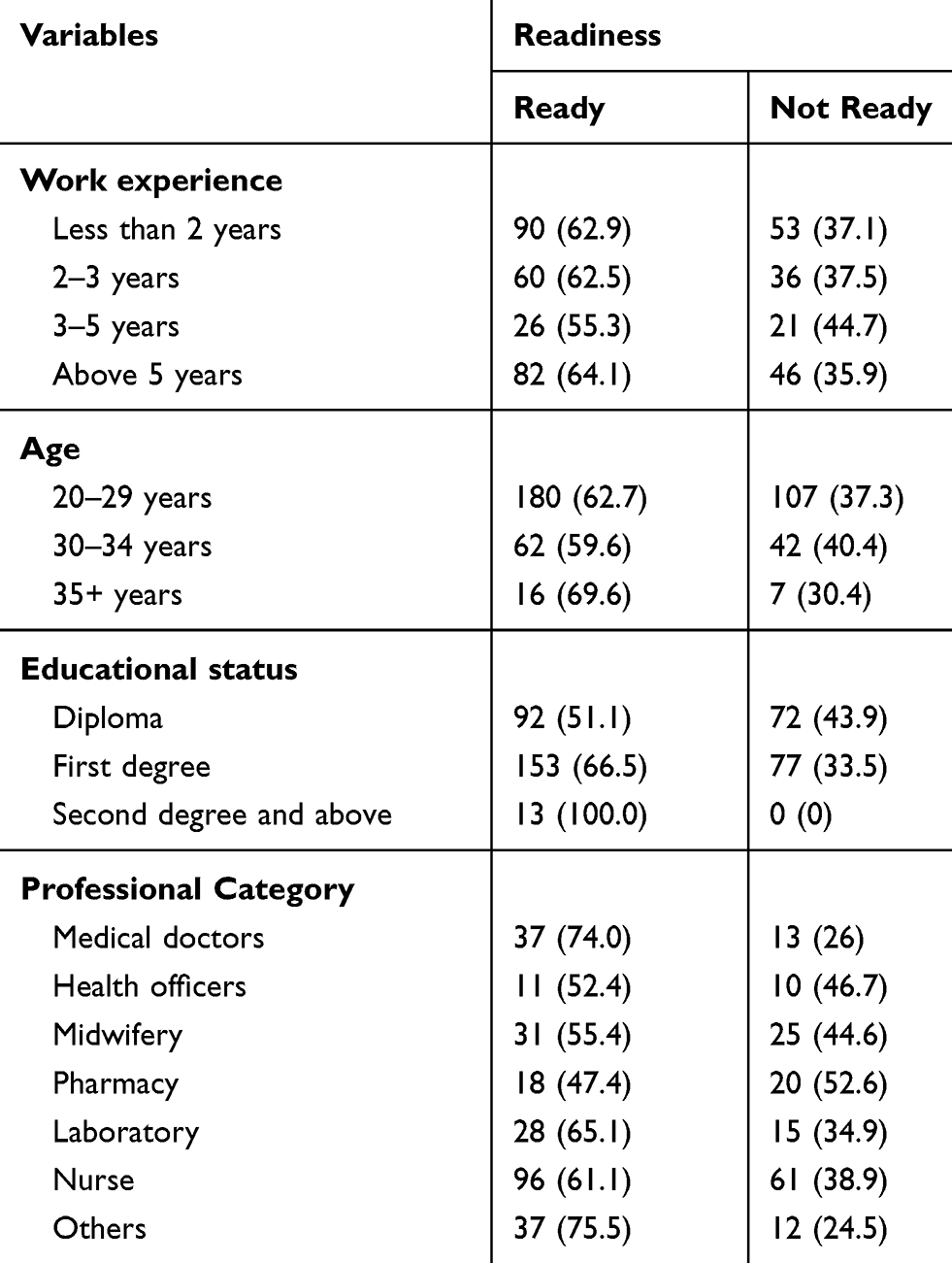 |
Table 2 Readiness of Health Professionals for EMR System by Their Socio-Demographic Characteristics in Four Primary Hospitals, Ethiopia, 2018 |
Knowledge and Attitude of Health Professionals Toward EMRs
In this study, 259 (62.6%) of the study participants had good knowledge. Similarly, 285 (60.1%) of the study participants had favorable attitude toward EMR (Figure 2).
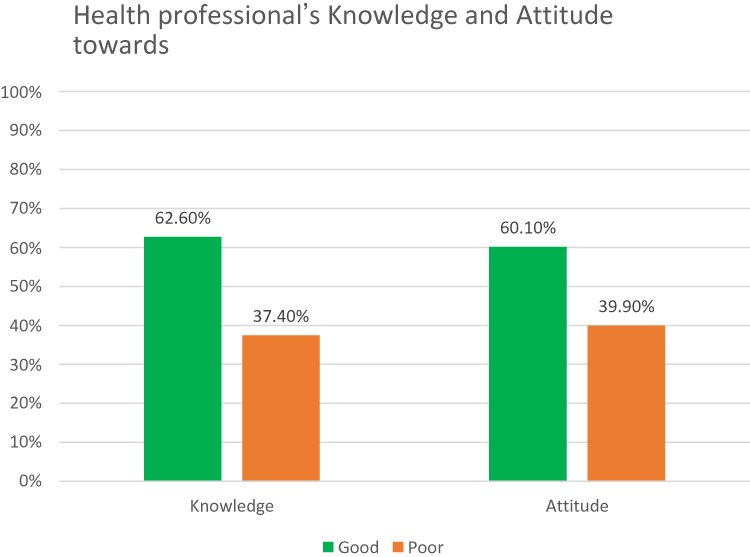 |
Figure 2 Health professionals knowledge and attitude toward EMR system in four primary hospitals, Ethiopia, 2018. |
Organizational and Technical Factors
Among 414 health professionals who participated in this study, only 106 (25.6%) of them had a computer at their office. Only 50 (12.1%) of the health professionals had internet access at their office. Seventy-three (68.9%) of the health professionals use their computer for data recording and report generation, 29 (27.4%) of them use it for reading, and 4 (3.7%) of them for other purpose, like video accessing. All primary hospitals had no active or functional IT department and IT technical person. All primary hospitals had a standby generator (Table 3).
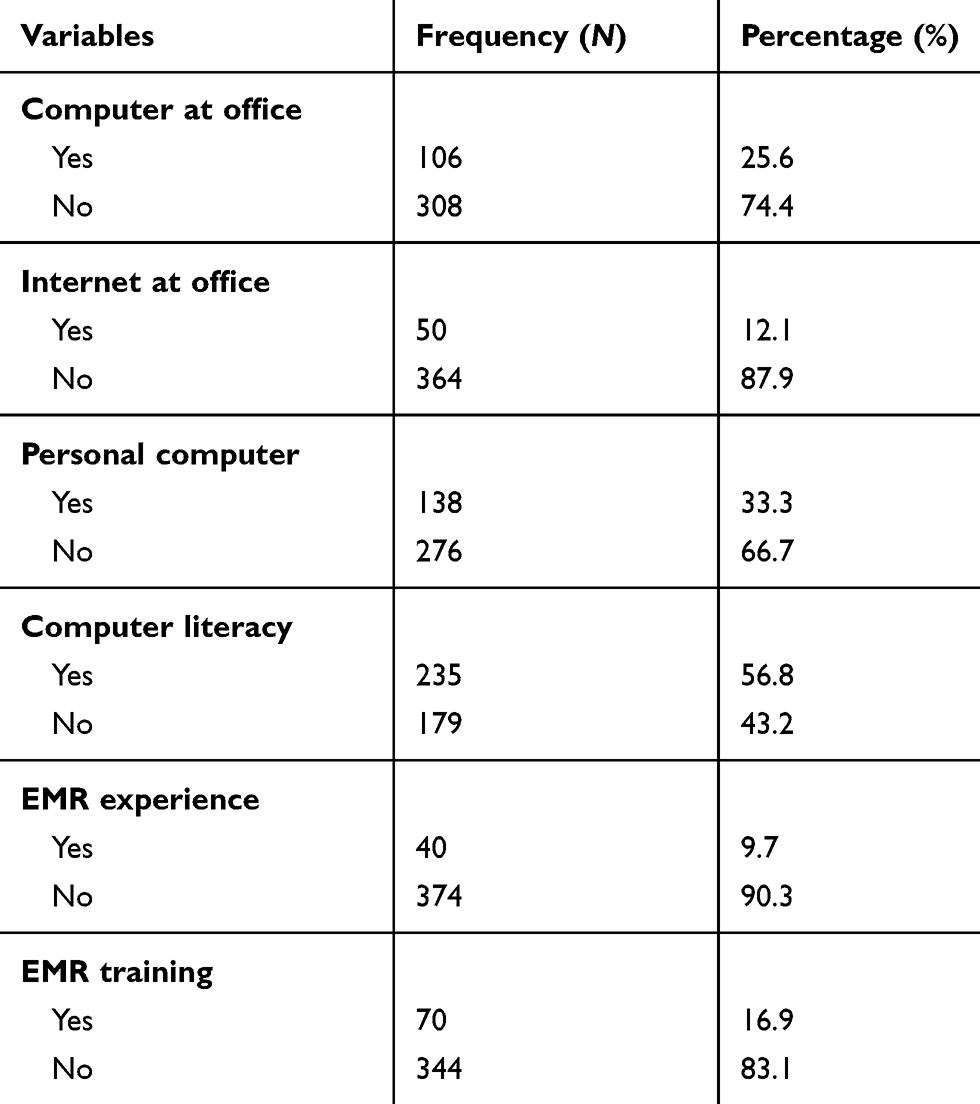 |
Table 3 Organizational and Technical Factors of Health Professionals in Four Primary Hospitals, Ethiopia, 2018 |
Nearly one-third (138; 33.3%) of the study participants had a private personal computer. More than half (235; 56.8%) of health professionals were computer-literate (Table 3).
About 40 (9.7%) study participants had worked with an EMR previously (EMR experience). Regarding training, 70 (16.9%) of the study participants had taken EMR training (Table 3).
Factors Associated with EMRs Readiness
As shown in Table 4, variables like EMRs knowledge, attitude toward EMRs, having a personal computer, computer literacy, and EMR training were associated with EMRs readiness.
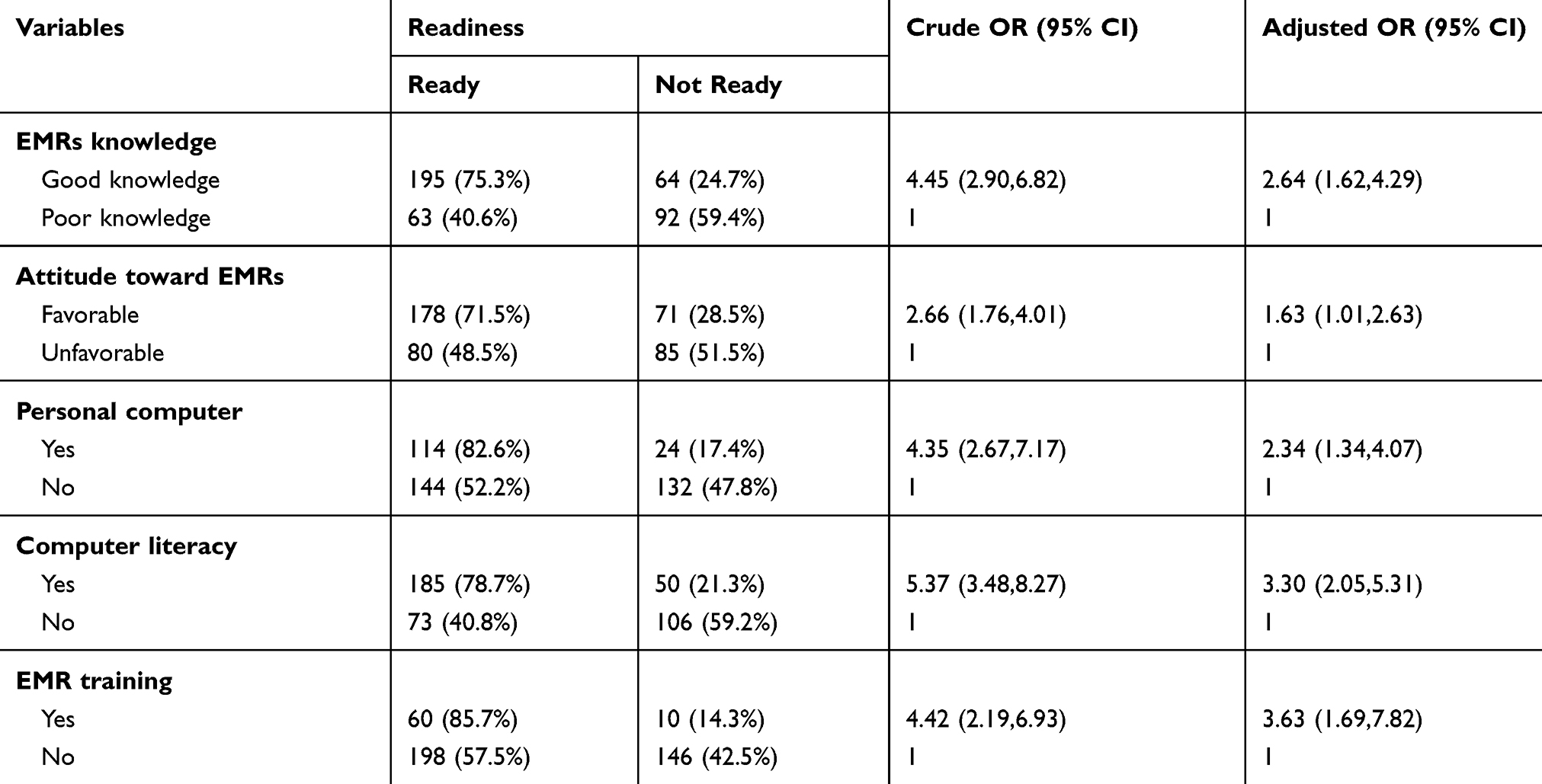 |
Table 4 Bivariate and Multivariate Analysis of Factors Associated with Readiness of Health Professionals for EMR System in Four Primary Hospitals, Ethiopia, 2018 |
Study participants who had good knowledge on EMR system were about 2.64 times more ready to use an EMR system as compared to those study participants with poor knowledge after controlling for other factors (AOR = 2.64, 95% CI: [1.62,4.29]). Health professionals who had a favorable attitude toward an EMR system were 63% more ready to use an EMR system than their counterparts (AOR = 1.63, 95% CI: [1.01, 2.63]).
Pertaining to computer access, study participants who had their own personal computer were about 2.34 times more ready to use an EMR system as compared to those study participants who had no personal computer (AOR = 2.34, 95% CI: [1.34,4.07]).
Study participants who were computer-literate were 3.3 times more ready to use an EMR system than their counterparts (AOR = 3.30, 95% CI: [2.05, 5.31]) after controlling for other variables. Similarly, health professionals who had taken EMR training were about 3.63 times more ready to use EMR system as compared to those health professionals who had not taken any EMR training before (AOR = 3.63, 95% CI: [1.69,5.80]) (Table 4).
Discussion
In this study, the readiness of health professionals for EMRs system in four primary hospitals that were in the frontline to implement an EMR system was assessed. The overall readiness of health professionals for an EMR system was 62.3% (with 66.2% core readiness and 65.3% engagement readiness). Health professionals’ readiness in this study was in line with a study done in Iran,8 but higher than a study conducted in Ethiopia.10 The difference could be due to the improvement and expansion of ICT infrastructure and the Ethiopian government also gives priority for digitization of health information system under its health sector transformation plan. The other reason could be the day-to-day exposure of health professionals to the global digital ecosystem. Moreover, currently, higher education institutions in Ethiopia have incorporated a generic health information system course for all health science students within their curriculum that can provide a clue about the EMR system.
In this study, health professionals who had good knowledge on the EMR system were about 2.64 times more likely to be ready for an EMR system as compared to health professionals with poor knowledge. Findings from different literature also support this.1,8,10,22 Another study conducted in Iran, Tehran teaching hospitals on nurse readiness to implement EMRs showed that those who had good knowledge were more likely to have readiness for an EMR system than their counterparts. This is may be due to health professionals who had good knowledge understanding how important an EMR is and their existing knowledge may facilitate their motives in actually practicing the EMR system.
Health professionals who had favorable attitude toward an EMR system were 2.63 times more likely to be ready than their counterparts. This is also supported by studies conducted in three hospitals in North West Ethiopia and other studies.8,10,18,22 This may be explained by the fact that having a good view to EMRs can influence health workers' readiness to integrate the EMR system in their routine activities. This result is supported with qualitative findings.
A 29-year-old participant said “I think electronic medical record system (EMRs) benefits outweigh from its possible drawbacks, and personally I can give all my effort to EMRs implementation.”
Study participants who had their own personal computer were about 2.34 times more ready for an EMR system as compared to those study participants who had no private or personal computer.
This may be due to the fact that study participants who had their own personal computer had seen how technology can simplify activities in their daily life, which in turn will be scaled up in the health sector.
Study participants who were computer-literate were 3.3 times more ready for an EMR system than their counterparts. Different literatures stated that computer literacy is one of the most significant factors for EMRs readiness. A study conducted in North West Ethiopia also showed that health professionals who were computer-literate are 2.55 times more ready for EMRs than their counterparts.10,13,18,22 This will be supported by the fact that computer-literates will not face as much difficulty in managing the EMR system if implemented for routine healthcare management. This result is supported with qualitative findings.
A 26-year-old participant said “For me electronic medical record system (EMRs) will not be difficult because I am skilled in computer utilization and I have the ability to operate any computer application.”
Health professionals who had taken EMR training were about 3.63 times more ready for an EMR system as compared to those health professionals who had not taken any EMR training before, and this is in line with other findings.10,22 This may be explained by the evidence that training and education usually change people’s views and perception. This result is supported with qualitative findings.
A 27-year-old participant said “One year ago I had been taking EMR training, that training helps me to understand the importance of technology and makes me more excited for such kind of system.”
The findings of this study could be generalizable to other primary hospitals in Ethiopia because all the primary hospitals have the same standard in ICT structure and other parameters.
Conclusion and Recommendation
In general, the overall readiness of health professionals for EMR system is low. EMRs knowledge, attitude toward an EMR system, having a personal computer, computer literacy, and EMR training were the significant factors for EMR readiness. Availing ICT infrastructure and provision of training for health professionals are crucial for the adoption of EMR systems. Promotion of EMR systems by the health program managers to the potential users is also important to increase adoption and success rate of EMR systems.
Abbreviations
eHealth, electronic Health; EMRs, electronic medical record system; ICT, Information Communication Technology.
Ethical Approval and Consent to Participate
Ethical clearance was obtained from the ethical review board of University of Gondar. Oral consent was obtained from each study participants. The data collection procedure was anonymous, and their privacy was also kept.
Data Sharing Statement
Data will be available upon request from the corresponding author.
Acknowledgment
We would like to thank University of Gondar institute of public health for the approval of ethical clearance. Respective health institutions and data collectors, supervisors and study participants.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Qureshi Q, Shah B, Nawaz A, Qureshi N. Readiness for eHealth in the developing countries like Pakistan. Int J Inf Technol. 2012;2(4):1–8.
2. Coleman A, Herselman M, Potass D E-health readiness assessment for E-health framework for Africa: a case study of hospitals in South Africa. DSpace Repository. 2011.
3. International Telecommunication Union. National eHealth Strategy Toolkit. ITU 2012. Available from: https://www.itu.int/pub/D-STR-E_HEALTH.
4. Atlas of eHealth Country Profiles: The Use of eHealth in Support of Universal Health Coverage: Based on the Findings of the Third Global Survey on eHealth 2015. Switzerland: WHO; 2015 Available from: www.who.int.
5. Hasanain R, Cooper H. Solutions to overcome technical and social barriers to electronic health records implementation in Saudi public and private hospitals. J Health Inform Dev Ctries. 2015;8(1).
6. Ketikidis P, Dimitrovski T, Lazuras L, PA B. Acceptance of health information technology in health professionals. Health Informatics J. 2012;18(2):124–34. doi:10.1177/1460458211435425
7. Durrani H, Khoja S, Naseem A, Scott R, Gul A. Health needs and eHealth readiness assessment of health care organizations in Kabul and Bamyan, Afghanistan. East Mediterr Health J. 2015.
8. Mahdi H-K, Reza S, Hamid B. Nurses readiness and electronic health records. Acta Inform Med. 2015;23:105.
9. Tilahun B, Fritz F. Comprehensive evaluation of EMR system use and user satisfaction at five low-resource setting hospitals in Ethiopia. JMIR Med Inform. 2015;3(2):e22. doi:10.2196/medinform.4106
10. Biruk S, Yilma T, Andualem M, et al. Health professionals’ readiness to implement electronic medical record system at three hospitals in Ethiopia: a cross sectional study. BMC Med Inform Decis Mak. 2014;14:115. doi:10.1186/s12911-014-0115-5
11. Kimaro H, Nhampossa JL. The challenges of sustainability of health information systems in developing countries: comparative case studies of Mozambique and Tanzania. J Health Inform Dev Ctries. 2009;1(1).
12. Electronic health records: manual for developing countries: WHO. 2014.
13. Ajami S, Ketabi S, Isfahani S, Heidari A. Readiness assessment of electronic health records implementation. Acta Inform Med. 2011;19:224. doi:10.5455/aim.2011.19.224-227
14. Jennett P, Jackson A, Healy T, et al. A study of a rural community‟s readiness for telehealth. J Telemedicine and telecare. 2003;9(5):259–63.
15. Qureshi QA. E-Readiness: a critical factor for successful implementation of ehealth projects in developing countries like Pakistan. 2014.
16. Brian SM, Wasko M, Vartabedian BS, Miller RS, Desirae DF, Maziar A. Understanding the factors that influence the adoption and meaningful use of social media by physicians to share medical information. J Med Internet Res. 2012;14:e117.
17. Li J, Seale H. E-health readiness assessment framework for public health services–pandemic perspective. Gomal Univ J Res. 2012;30(2):77–86.
18. Jebraeily M, Ahmadi M, Hajavi A, Gohari M, Sedghi Jahromi M. Electronic health records: personnel readiness assessment. J Health Administration. 2010;13(39):17–24.
19. Shah G, Leider J, Castrucci B, Williams KS, Luo H. Characteristics of local health departments associated with implementation of electronic health records and other informatics systems. Public Health Rep. 2016;131(2):272–82. doi:10.1177/003335491613100211
20. Li J, Land L, Ray P, Chattopadhyaya S. E-Health readiness framework from electronic health records perspective. Int J Internet Enterprise Manag. 2015;4.
21. Mary E, Morton R, Susan W. EHR acceptance factors in ambulatory care: a survey of physician perceptions. Perspect Health Inf Manag. 2010;7.
22. Habibi Koolaee M, Mirkarimi A, Behnampour N, javadkabir M. Readiness assessment of laboratory and imaging staff to implement electronic health records. Iran J Basic Med Sci. 2014;3:5–8.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.