")
Back to Journals » Risk Management and Healthcare Policy » Volume 16
Health Literacy Among Young People in Africa: Evidence Synthesis
Authors Amanu A A , Birhanu Z, Godesso A
Received 15 December 2022
Accepted for publication 10 March 2023
Published 23 March 2023 Volume 2023:16 Pages 425—437
DOI https://doi.org/10.2147/RMHP.S399196
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Adamu Amanu A,1 Zewdie Birhanu,1 Ameyu Godesso2
1Department of Health, Behaviour, and Society, Jimma University, Jimma, Oromia, Ethiopia; 2Department of Sociology, Jimma University, Jimma, Oromia, Ethiopia
Correspondence: Adamu Amanu A, Email [email protected]; [email protected]
Background: Health literacy has critical health implications. Health literacy in young people is a pressing matter as it determines their current and future health. Although health literacy research is increasing, there are limited health literacy studies from Africa. The aim of this study was to provide a coherent summary and synthesis of the available health literacy studies among young people in Africa.
Methods: A systematic scoping review was chosen to attain the aim of this study. PubMed, CINAHL, AJOL, JBI EBP, EBSCO, and Google Scholar were searched for evidence. Based on JBI’s methodology for reviews, a three-step search strategy was employed. The search was conducted up to April 20, 2022. The PRISMA flow diagram guideline was used to ensure a transparent reporting of the review process.
Results: The search for evidence identified 386 records, of which 53 were selected and their full texts were assessed for eligibility. Nine studies matched the eligibility criteria. The main findings of the eligible studies are: health literacy levels, association between health literacy and health outcomes, and predictors of health literacy among young people. Low health literacy was common among young people, and there was a significant association between low health literacy and negative health outcomes among this group. Health literacy among young people was impacted by a wide range of socio-demographic factors.
Conclusion: Health literacy studies among young people in Africa were rare. Although the reviewed studies shed some light on health literacy levels, the association between health literacy and health outcomes, and the predictors of health literacy among young people, they may not give an accurate picture of health literacy among young people, for several reasons. Both primary and secondary health literacy studies are needed to fully understand the issue, and to develop and guide policies and interventions in Africa.
Keywords: health literacy, young people, Africa, developing countries, scoping review
Plain Language Summary
Health literacy determines an individual’s health behavior and healthcare utilization. Therefore, it is a critical matter in both clinical and health promotion contexts. Health literacy in young people is an especially pressing matter, as health behavior and knowledge which are established at a young age affect an individual’s health throughout his or her life course. In particular, in low-income countries, such as in Africa, it is a critical issue to reduce health and social problems associated with teenage pregnancy and STIs, to combat poverty, and to promote the overall well-being of society. Therefore, both primary and secondary health literacy studies are essential to understand health literacy in young people and to develop effective public health policies and make evidence-based interventions.
Background
Health literacy (HL) refers to the knowledge, motivation, and abilities of individuals to acquire, understand, evaluate, and use health information in order to make judgments and decisions regarding healthcare, disease prevention, and health promotion to safeguard and enhance quality of life in everyday life.1 It is a key to a healthy lifestyle.2,3 People with adequate HL status are usually more likely to engage in health-promoting practices, whereas individuals with low HL status are more likely to have unhealthy behaviors, including smoking, alcohol abuse, and substance use.3–5 In association with these unhealthy behaviors, many health complications, including cardiovascular diseases, could arise.5–7 HL also influences the interactions within and the use of the healthcare system.8 Individuals with low HL levels are more likely to miscommunicate with health professionals, more likely to make mistakes when taking medicines, less likely to manage their health situations, and more vulnerable to the risk of longer hospitalization.9,10 Thus, low HL status is related to poorer health status and outcomes, higher health system costs, and increased mortality.11,12
Therefore, HL has critical implications for individual and population health.1,11,13 HL in young people is an especially pressing matter1,14 because health-related knowledge, attitudes, and behaviors develop at a young age, and they become deeply rooted into personal characteristics and are difficult to modify or change later, at an adult stage.15,16 Health behaviors such as those related to drug use, smoking, unhealthy diet, risky sexual behavior, and physical inactivity which are established at a young age not only affect the current health of young people but also track into health in later life and may also determine the health status of one’s future children.17,18 Therefore, young age is a critical stage of life during which behaviors and attitudes that can positively or negatively affect the future health of individuals and populations are consolidated.18–21 Thus, young people need an appropriate level of HL knowledge and skills to invest not only in their health but also in the health of their families, communities, and nations. Failing to address HL in this group may cause a huge risk for both individuals and society, as it may result in poorer health status, poorer health outcomes, and greater healthcare costs.22,23
These days, the literature on HL is rapidly increasing; however, compared with that of the adult population, HL in young people is underresearched, especially in low-income settings.24–26 Furthermore, even though the need for HL is widely being acknowledged across the world, interest in HL studies has been mainly concentrated in developed countries.1 Thus, there have been limited HL studies from developing countries.27 In particular, empirical studies examining the HL of people in Africa are scarce.28 Besides, existing evidence around young people’s HL in Africa has not been synthesized. Also, a preliminary search of Open Science Frameworks and the Joanna Briggs Institute (JBI) Database of Systematic Reviews register indicated that there are no current or ongoing reviews on HL in young people in Africa.
However, without synthesis of the available body of studies on HL in young people, it is difficult to understand the progress attained and to identify gaps in the research. Therefore, the aim of this review was to provide a summary and synthesis of the existing HL studies on young people in Africa. Specifically, it was concerned with identifying and mapping the available evidence, synthesizing the main findings, and discussing the implications, including the gaps in the research.
Methods
A scoping review was chosen to achieve the aim of this study as it helps in relation to the following main purposes: 1) to examine the nature, scope, and range of all the available studies; 2) to determine whether systematic review and meta-analysis would be valuable; 3) to summarize and disseminate findings of the existing studies; and 4) to reveal the existing research gaps.29 This review was mainly concerned with the last two purposes. The study was guided by the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) statement.30
Inclusion and Exclusion Criteria
B its purpose, this study was concerned with identifying and mapping all of the available HL studies concerned with young people in Africa, regardless of their design, approach, and year of publication, but fulfilling the following eligibility criteria.
The inclusion criteria that were used to identify relevant studies for this research were: 1) study with clear objectives and methods; 2) study focused on generic health literacy; 3) study with a full manuscript; 4) study written in the English language; 5) study conducted in Africa; and 6) study population was young people. The World Health Organization31 regards young people as those aged 10–24 years. Accordingly, the study populations of the studies eligible for this review were young people within the age range of 10–24 years, although the age of a very few of the study participants, in only three of the studies, exceeded 24 years.
Accordingly, the exclusion criteria included: 1) study focused on domain-specific HL; 2) study focused on only measuring health knowledge; 3) study without a full manuscript; 4) study written in a language other than English; 5) study conducted outside Africa; 6) study that did not exclusively deal with young people; and 7) study that failed to meet any of the above eligibility criteria.
Sources of Information and Search Strategies
The databases searched were: PubMed, CINAHL, African Journals Online (AJOL), Joanna Briggs Institute EBP Database, and EBSCO host. Also, Google Scholar and Google searches were undertaken to access the gray literature. The search was conducted up to April 20, 2022. A three-step search technique was undertaken based on the JBI’s methodology for reviews for this study.32 First, PubMed and Google Scholar searches were conducted and the words in the title, abstract, and index terms of the accessed studies were analyzed based on the identified review purpose. Next, for all of the identified databases, full searches were conducted using all of the identified keywords and terms. Both search strategies and keywords/index terms were adapted and used for all of the included databases and sources of information. Finally, the reference lists for all of the studies that met the eligibility criteria were scanned to identify additional relevant research articles. Search concepts/terms utilized in this review include: “health literacy”, “young people”, “adolescent”, “teen”, “youth”, “young adult”, “student”, “developing country”, “low income country”, and “Africa”. Relevant Boolean operators (AND, OR), field codes ([ti], [tiab]), and truncation (*) were used wherever needed. While undertaking Google Scholar searches, a number of African countries’ names were used in addition to the above search terms. Full search strategies and search dates for all of the aforementioned databases are detailed in Supplementary S1 (in Supplementary Material).
Study Selection
After completion of the search, all of the identified results were imported to EndNote X9, and duplicates were removed. Then, the study screening and selection process was started, using the PRISMA flow diagram guideline to ensure transparent reporting of the review process.30 First, all of the titles and abstracts of the identified studies were screened and any articles that were irrelevant to the review were removed. Next, based on the eligibility criteria for this study, the full texts of the remaining studies were assessed in detail. Those articles that met the eligibility criteria were selected for the study. Then, the references of all studies that met the inclusion criteria were also checked to identify additional potential articles. The details of the study selection processes and results are shown in Figure 1.
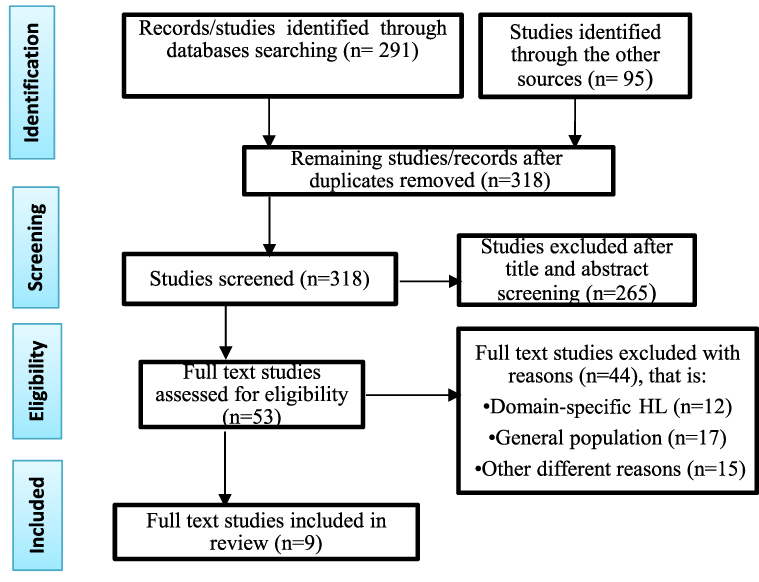 |
Figure 1 Eligible studies selection process and results (PRISMA flow diagram). Note: Adapted from Moher D, Liberati A, Tetzlaff J, Altman DG, PRISMA Group. Reprint—Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Phys Ther. 2009;89(9):873–880.30, |
Data Extraction and Presentation
The data extraction instrument/tool from the JBI’s methodology guidance for scoping reviews was adapted and used for this scoping review32 (see Supplementary S2 in Supplementary Material). All of the selected articles were carefully read to extract the required information. The extracted data included information on author, country where the study was conducted, year of publication, objective of the study, study method/design, study context/setting, study subjects/population, sampling technique, sample size, tool utilized to measure health, and summary of the important findings. After completing the readings of the selected articles and extracting of the required information, the data extraction process was revised to ensure its accuracy.
The extracted data from all the selected articles were reviewed, compiled, summarized, and mapped in a table format. Based on the information extracted, the main headings of the table include the author of the article, year of publication, study country, purpose/objective of the study, study design and method, study setting, study population, sampling design, sample size, HL measures, and summary of important findings (Table 1). This table is accompanied by a narrative summary and synthesis of the findings.
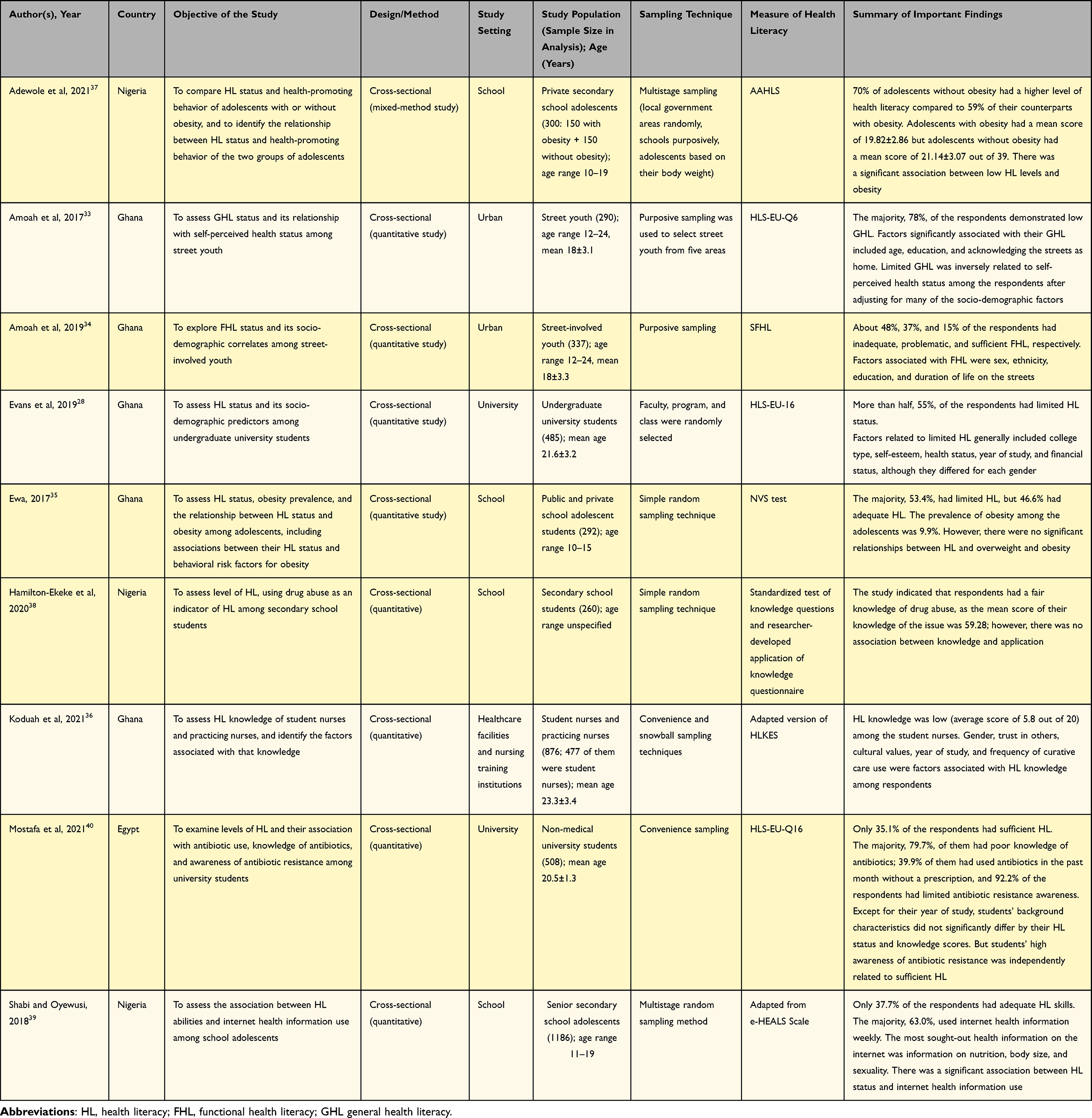 |
Table 1 Overview of the Articles/Studies Included in This Study |
Results
As shown in Figure 1, the search for evidence identified 386 records in total. After removing 68 records, which were duplicates, 318 records were left. The titles and abstracts of all of the remaining 318 records were evaluated for suitability, and 265 of them failed to be considered for further assessment. Then, the full texts of all of the remaining 53 studies were evaluated for their eligibility for inclusion in the review. Thus, 44 of them were excluded as they did not matching the inclusion criteria, yielding a total of nine studies for inclusion in this study, as no additional articles or studies were obtained through screening the references of the selected studies. The overviews of the nine studies/articles that were included in this study are shown in Table 1. Detailed reasons for the exclusion of the 44 full-text studies that failed to meet the eligibility criteria are provided in Supplementary S3 (in Supplementary Material).
Characteristics of the Included Articles/Studies
More than half of the eligible studies (five out of nine studies)28,33–36 were conducted in Ghana; three of them37–39 were conducted in Nigeria, and the remaining one40 was carried out in Egypt. All of these studies were cross-sectional. Eight of these studies were quantitative studies, and the remaining study37 was a mixed method study that combined a self-administered questionnaire and an in-depth interview. In eight of the nine studies, it was clearly indicated that both sexes had participated in the studies. In terms of age, study participants were of a young age, 10–24 years old, although a very few of them were older than this age limit in three of the studies.28,36,40 In one of the studies,38 the age range and sex of the participants were not clearly specified. However, since this study was conducted on secondary school students, in terms of age, the study participants would be less than 24 years old.
Four of the studies35,37–39 were conducted in school settings (both public and private), on primary/secondary school adolescents; three studies28,36,40 were conducted in university/college settings on undergraduate students (the second one was conducted in healthcare facilities and nursing colleges, on student nurses and practicing nurses, but the focus of this review was on the nursing students as practicing nurses were mostly adults), and the remaining two studies33,34 were conducted in urban areas, on street youth. In order to select study participants, four of the studies28,35,38,39 utilized simple random sampling techniques; three of the studies used purposive sampling techniques,33,34,37 and the remaining two studies36,40 employed convenience sampling techniques (the first one of these additionally used a snowball sampling technique).
Health Literacy Tools Utilized in the Included Articles/Studies
The articles included in this study used different HL assessment tools, ranging from standardized measures to researcher-developed questionnaires (Table 1). To measure general health literacy (GHL) among street youth, Amoah et al33 used the short-short version of European Health Literacy Survey Questionnaire (HLS-EU-Q6),41 which comprises six items with five response categories. The response categories for this tool are: 1=very difficult, 2=difficult, 3=easy, 4=very easy, and “don’t know/refused”=99 (missing value). In this study, HL level was scored based on the mean of every case, and the mean scores of the measures were then used to create three HL levels, namely, inadequate HL (score <2); problematic HL (score 2–3), and sufficient HL (score 3–4). A fourth category of GHL, that is, limited GHL, was constructed by combining inadequate and problematic GHL scores.
To measure functional health literacy (FHL) among street youth, Amoah et al34 used the Swedish Functional Health Literacy (SFHL) scale. The SFHL scale consists of a five-item tool with five response categories.42 In this study, the response labeled in the original tool as “seldom” was replaced by “not often”, and “always” was replaced by “all the time”. Based on the recommendations given by the developers of the tool, the SFHL was scored by assigning values to each of the five response options. Accordingly, response to options “never” and “not often” (1 and 2) were labeled with a value of 1000; option “sometimes” (3) was labeled with a value of 100; and options “often” and “all the time” (4 and 5) were labeled with a value of 1. Only respondents with at least four valid responses out the five options were included in the analysis. The results of the measure were summed, and values <100 were regarded as sufficient FHL, values 100–1000 were regarded as problematic FHL, and values >1000 were regarded as inadequate FHL.42
Evans et al28 used the 16-item short version of the HLS-EU-Q (HLS-EU-Q16)41 to assess HL levels among undergraduate students. The 16 items have four responses, with the following values/codes: very difficult=1; difficult=2; easy=3; very easy=4; and do not know=0 (coded as missing in the analyses). Mean scores, in this study, were calculated for all of the items on the scale and converted to an index using the following formula: Health literacy index score = (Mean − 1) × (50/3), where mean refers to the mean of items on the scale, 1 is equal to the minimal possible value of the mean, which leads to a minimum value of the index of 0, 3 is equal to the range of the mean, and 50 is equal to the chosen maximum value of the new index scores. Thus, the index scores ranged from a minimum of 0 to a maximum of 50. The HL levels were grouped into four categories: excellent (>42 to 50), sufficient (>33 to 42), problematic (>25 to 33), and inadequate (from 0 to 25). These HL categories were dichotomized as: limited HL (combining inadequate and problematic HL levels) and adequate HL (combining sufficient and excellent HL levels) for logistic regression analyses. Likewise, Mostafa et al40 used a modified short version of the HLS-EU-Q1643,44 to measure HL levels among non-medical university students. In this study, the four categories of responses were dichotomized as follows: “very easy” and “fairly easy” options were given a value of “1”, and “fairly difficult” and “very difficult” were given a value of “0”; “do not know” responses were regarded as missing. Respondents were categorized under three levels of HL: “sufficient” HL (score ≥13), “problematic” HL (score 9–12), and “inadequate” HL (score ≤8).
Adewole et al37 used the All Aspects of Health Literacy Scale (AAHLS)45 to assess the HL status of adolescents with and without obesity. The AAHL is a three-point Likert scale, with 1=“rarely”, 2=“sometimes”, and 3=“often”, which uses three subscales of functional, communication, and critical literacy, consisting of 13 items/questions, with 39 as the maximum obtainable score. A score of 0–19.99 was rated as poor HL and a score of 20–39 was rated as good HL, using a mean score of 20. Koduah et al36 used a modified version of the Health Literacy Knowledge and Experience Survey (HLKES) instrument46 to assess the HL knowledge of nursing students. This instrument consists of 20 items; hence, the correct score of respondents could range from 0 to 20, unlike the original tool, which scores from 0 to 29. All of the correct responses were scored as “1” and incorrect responses were scored as “0” for the purpose of analysis, and to obtain a total score of HL knowledge out of 20, all scores were summed.
Shabi and Oyewusi39 used the adapted version of the eHealth Literacy Scale (e-HEALS)47 to assess school-aged adolescents’ HL status. The e-HEALS is an eight-item measure of HL that measures a consumer’s knowledge and perceived skill in finding, appraising, and using internet health information for his or her health matters. Ewa35 used the Newest Vital Sign (NVS) test to assess the HL of adolescent students in public and private schools, and the HL scores were categorized into limited HL and adequate HL, according to the literature stating the categorization of HL when using this instrument.48 The remaining study, by Hamilton-Ekeke et al,38 used a standardized test of knowledge questions and a researcher-developed application of a knowledge questionnaire to measure HL levels among secondary school students, using drug abuse as an indicator of HL status. The knowledge measure questionnaire about drug abuse was adapted from a standardized measure of knowledge questions on drug abuse (from Senior School Certificate Examinations) and the application of knowledge of drug abuse (for instance, in making informed health decisions) questionnaire was developed by the researchers in Likert format.
Main Findings of the Included Articles/Studies
The important findings of the articles included in this study can be categorized into three groups: HL levels, relationship between HL and health outcomes, and predictors of HL among young people.
Health Literacy Levels Among Young People
All nine of the selected studies measured HL levels among their participants; however, they used different tools to measure HL, as indicated in Table 1. Using the HLS-EU-Q6, in a study conducted on street youth in Ghana, Amoah et al33 revealed that the majority (52.4%) of the youth had a problematic GHL (score of 2–3); 26% had inadequate HL (score <2), and only 21.6% had sufficient HL (score of 3–4). That is, about 78% of the youth were found to have limited GHL. In another study conducted on street-involved youth in the same country, using the SFHL, Amoah et al34 found that about 48%, 37%, and 15% of the respondents had inadequate, problematic, and sufficient FHL, respectively. That is, the majority, 85%, of the respondents had limited FHL (inadequate and problematic HL combined).
Using the HLS-EU-Q16, in a study conducted on undergraduate university students in Ghana, Evans et al28 found that about 55% of the respondents had limited HL (20.4% of them had inadequate HL and 34.2% of them had problematic HL). According to this report, almost one in every five students had inadequate HL. Similarly, in a study conducted in Egypt on non-health university students, using a modified version of the HLS-EU-Q16, Mostafa et al40 found that only about 35.1% of respondents had sufficient HL, about 49.3% had problematic HL, and about 15.6% had inadequate HL. And in a study conducted on private secondary school adolescents in Nigeria, with the use of the AAHLS measure, Adewole et al37 found that the majority, 70%, of adolescents without obesity and 59% of those with obesity had higher HL levels. According to this study, respondents with obesity had lower mean scores than respondents (adolescents) without obesity for all subscales of the HL scale, and respondents with obesity had a mean score of 19.82 (±2.86) while respondents without obesity had a mean score of 21.14 (±3.07) out of 39.
Using an adapted version of the HLKES, in study conducted on student nurses in Ghana, Koduah et al36 found that there was generally low HL knowledge among the respondents (average score of 5.8 out of 20). Likewise, in another study conducted in Ghana, on public and private school adolescent students, using the NVS test, Ewa35 found that the prevalence of low HL was 53.4% and the prevalence of adequate HL was 46.6%.
In a study conducted in Nigeria on senior secondary school adolescents, using the adapted version of the e-HEALS, Shabi and Oyewusi39 found that only 37.7% the respondents had adequate (good) health HL skills and 59.0% of them had average HL skills. They reported that in-school adolescents in general have inadequate HL skills, although they showed relatively high levels of internet health information use. Finally, in an assessment of HL levels, in the same country, using drug abuse as an indicator of HL among secondary school students, using a standardized test of knowledge questions and a researcher-developed application of knowledge questionnaire, Hamilton-Ekeke et al38 found that the mean score for knowledge of drug abuse among the respondents was 59.28, but their finding showed that there was no relationship between knowledge and application; there was a weak negative association between knowledge of drug abuse and its application (r=−0.04, n=205).
Relationship Between Health Literacy and Health Outcomes Among Young People
From all the nine studies selected for this review, one study33 assessed the association between HL and perceived health status among street youth. This study found that 64% of the respondents perceived their health status as poor. Both inadequate GHL (β=−0.50, p<0.01) and problematic GHL (β=−0.39, p<0.01) were negatively associated with self-perceived health status, after controlling for many socio-demographic factors. Accordingly, the respondents with limited GHL were likely to perceive their health status as poor while those with adequate GHL were likely to perceive it as good.
Five of the included articles assessed the relationship between HL and health behaviors.34,35,37,39,40 The health behaviors and practices discussed in these studies are concerned with food habits, alcohol consumption, smoking behavior, physical activity, drug and antibiotic use, and use of internet health information. In a study conducted on private secondary school adolescents, Adewole et al37 found a significant association between HL and health-promoting behavior among with adolescents with obesity (r=0.29, p=0.001) and among adolescents without obesity (r=0.85, p=0.015). In this study, adolescents without obesity reported a greater level of good health-promoting behavior than adolescents with obesity. They found that the majority of the adolescents without obesity engaged in positive habits such as proper eating, consuming enough fruits and vegetables, and drinking plenty of water daily. However, many of the adolescents with obesity practiced negative habits such as skipping/avoiding meals, eating junk food or non-nutritional food, and using drugs for the reduction of weight, and they did not engage in regular exercise. This study noted that the adolescents did not regularly participate or engage in health-promoting activities, irrespective of their obesity status. It reported that irrespective of the obesity status, adolescents’ health-promoting behavior was significantly related to their HL status.
In a study conducted on street-involved youth, Amoah et al34 found that about 37% of the youth had previously consumed alcohol and about 14% of them had ever smoked cigarettes. In this study, alcohol consumption was significantly associated with inadequate FHL, but smoking was not, and street-involved youth whose FHL levels were inadequate were about 10 times more likely to have consumed alcohol compared with those who had adequate FHL levels. In a study conducted on public and private school adolescent students, Ewa35 found that the prevalence of obesity was 9.9%, and behavioral risk factors for obesity among the adolescents included food habits and level of physical activity. However, there was no significant difference between the score on the mean food habits checklist and the score for physical activity among those adolescents with low or adequate HL, and there was no significant relationship between HL and obesity and overweight.
In a study conducted on university (non-medical) students, Mostafa et al40 found that approximately 38.0% of the respondents reported that they had used antibiotics a month ago and about 62.3% of them had used them within the past 12 months; and about 39.9% of the respondents reported using antibiotics within the past month without a prescription. However, according to this study, there were no statistically significant differences in the respondents’ use of antibiotics between the three HL levels (inadequate, problematic, and sufficient). In an assessment of the extent of internet health information use among senior secondary school adolescents, Shabi and Oyewusi39 found that only about 13.1% of the respondents used internet health information regularly/daily and 49.9% utilized it weekly. According to this study, the adolescents used internet health information for health issues such as healthy diet or nutritional issues (3.08±1.04), concerns about their body size, shape, image, and physique (2.91±1.05), and issues regarding sexually transmitted infections (2.72±1.10); matters of sexuality were among the major reasons for using internet sources. The chi-squared test results showed that there was a significant association between the use of internet health information and health information literacy skills among the adolescents.
Predictors of Health Literacy Among Young People
Six of the nine articles included in this study28,33–36,40 identified predictors of HL among their participants. The predictors of HL identified in these studies include age, sex, education, type of school, type of college, self-esteem, health situation, financial status, study year, frequency of curative care use, cultural values, and awareness.
For instance, Amoah et al33 showed that age, sex, education, and whether the youth considered the street as home were significantly correlated with GHL levels among the respondents. According to this study, older youths were less likely to have limited GHL compared with younger youths (β=−0.32, p<0.01). Female respondents (β=0.26, p<0.05) were more likely to have limited HL (inadequate and problematic HL combined) compared with males. Limited GHL was lower among males (75%) than females (82%). Living on the streets for more than three years (β=0.29, p<0.05) was significantly related to limited HL, and regarding the streets as home (β=0.254, p<0.05) was a strong positive predictor of limited GHL. This implies that the longer they engage in street life, the more their HL status worsens. Similarly, in another study conducted on street-involved youth, Amoah et al34 found that ethnicity, gender, religious affiliation, education level, length of street life, and regarding the street as their home were significantly associated with FHL. According to this study, only about 12% of females had sufficient FHL while 19% of males had sufficient FHL; that is, female youths were more likely to have poorer FHL. Ethnicity also significantly predicted inadequate FHL. Furthermore, the study reported that people with more education had lower odds of having low FHL; and youths who lived longer on the street had poorer FHL.
A study conducted on public and private school adolescent students by Ewa35 reported type of school as a predictor of HL, as children from public schools were found to have significantly lower HL scores compared to those from private schools. In a study conducted on undergraduate university students, Evans et al28 found that factors related to HL included type of college, self-esteem, health situation, financial status, and study year, although the results were not similar for each gender. In this study, limited HL among male respondents was 59% while it was 48.6% for the female respondents. The groups with the highest percentage of limited HL among these respondents were those with a poor financial background/status (82.4%) and those who had low self-esteem (80%). According to this study, respondents in the lower years of study were about 1.7 times more likely to have limited HL compared with those in the upper years of study (95% CI: 1.05, 2.69). Likewise, students from non-health science colleges had higher odds of having limited HL compared with students from health sciences college (OR 1.78; 95% CI: 1.22, 2.59). Respondents who perceived their health status as unsatisfactory were two times more likely to have limited HL compared with those who perceived their health status as satisfactory (95% CI: 1.24, 3.65). Similarly, respondents with low self-esteem were more likely to have limited HL compared with students with high self-esteem (OR 3.47; 95% CI: 1.38, 8.72). This study reported that type of college and study year were related to limited HL among male students, while among female students, factors significantly associated with limited HL were type of college, health situation, and self-esteem.
In a study carried out on nurse students, Koduah et al36 found that cultural beliefs/values (B=0.276, p<0.001) and study year (B=0.244, p<0.05) showed positive relationships with HL knowledge, whereas gender/sex (being male, B=−0.499, p<0.01), frequency of use of curative care (B=−0.236, p<0.05), and trusting others (B=−0.874, p<0.001) were negatively related with HL knowledge. Finally, in a study conducted on non-medical university students, Mostafa et al40 found that except for year of study, the students’ socio-demographic background characteristics did not significantly differ by HL levels or scores of knowledge. In multivariable logistic regression analysis, a good level of knowledge on antibiotic resistance among the students was significantly higher among those in advanced years of study, specifically third year students (adjusted OR 4.5; 95% CI: 1.7, 11.8) and fourth year students (adjusted OR 4.4; 95% CI: 1.4, 13.5), but it was not related to sufficient HL. Sufficient HL was independently related to students’ high antibiotic resistance awareness (adjusted OR 2.8; 95% CI: 1.3, 5.9).
Discussion and Implications
The aim of this study was to identify and provide a coherent summary of the available HL studies among young people in Africa, and to identify and inform gaps in the literature. There were limited HL studies among young people in Africa. All of the studies/ articles included in this study assessed HL levels among young people; however, they used different tools. The HL measurement tools used in these studies include adapted or modified versions of HLS-EU-16, HLS-EU-Q6, SFHL, AAHLS, HLKES, e-HEALS, and NVS, including a researcher-developed questionnaire. Although most of these studies were conducted in school, university, or college contexts, almost all of them reported that there were low HL levels among the respondents (young people). For instance, in a study conducted on undergraduate university students, Evans et al28 found that about 54.6% of the respondents had limited HL. Likewise, in a study conducted on non-medical university students, Mostafa et al40 reported that about 49.3% of the respondents had problematic HL while about 15.6% had inadequate HL. Also, even in a study conducted on student nurses, Koduah et al36 found that there was generally low HL knowledge among the respondents (with an average score of 5.8 out of 20).
Six of the articles considered for this study33–35,37,39,40 examined the association between HL and health outcomes, such as perceived health status, health knowledge, and health behaviors, including food habits, consumption of alcohol, cigarette smoking, physical exercise, drug/antibiotic use, and internet health information use. Most of these studies found that low HL was significantly related to negative health behavior and practices, with regard to those listed above. A number of HL studies confirm this fact, indicating that unhealthy behaviors and practices are common among people with low HL.3–5
Again, six of the nine reviewed studies28,33–36,40 identified predictors of HL among young people. The predictors of HL identified in these studies include age, gender, ethnicity, level of education, type of school, type of college, self-esteem, health condition, financial status, study year, frequency of use of curative care, cultural values, and awareness. Each of these studies reported that a number of these factors significantly predicted HL among their respondents. HL research also confirms that HL is impacted by different factors, including age, gender, education, race, genetics, life experiences, knowledge, socio-economic status, health disparities, social norms, public policy, and the built environment.1,12,13
Although the studies included in this review had shed some light on the HL levels, the relationship between HL and health outcomes, and predictors of HL among young people in the African countries where they were conducted, the following points need to be noted. First, the study samples in many of these studies may not be representative of the populations from which they were selected, and thus, their findings may not be generalizable. This is because the respondents in these studies were recruited through convenience or purposive sampling techniques; for instance, Koduah et al36 and Mostafa et al40 employed convenience sampling techniques (the former study used a snowball sampling technique in addition), and Adewole et al37 and Amoah et al33,34 used purposive sampling techniques. Second, all of the eligible studies in this review were conducted in school, university, and urban contexts, where respondents are expected to be more health literate than people in other contexts. Third, the studies used HL tools which are designed in developed countries, so that they may not be appropriate in the context of developing countries, as in Africa. Fourth, the wide age range of study participants (10–24 years, and in some studies exceeding 24 years) is a problem as it may create variation in their HL levels and related issues.
In addition, this review has a number of limitations, in addition to the issues raised above. 1) Quality assessments of the included studies were not conducted, in order to include all studies that met the specified eligibility criteria. 2) Only five databases, namely, PubMed, CINAHL, AJOL, JBI EBP, and EBSCO host, were searched, besides Google Scholar; thus, some relevant literature from other sources may have been missed. 3) The included studies used different HL measures, and individuals were categorized in different ways based on their HL levels across the studies; this is a problem when concluding that HL levels in young people are low/high. 4) Only papers written in English were eligible for this review, so some relevant studies that were written in other languages may have been missed. Besides, since almost all of the studies found to be eligible for this review were from only a few countries, the results of the current review may not be generalizable to the rest of Africa.
Therefore, there is much work to be done with regard to HL among young people in Africa. Both primary and secondary studies are needed to address the above limitations and to provide a better understanding of HL among young people in Africa. HL levels, the relationship between HL and health outcomes, and HL predictors among young people need to be investigated further. Young people’s perceptions and perspectives of HL need to be assessed to fully understand HL among young people in Africa. Also, HL intervention research is needed to identify effective evidence-based HL promotion activities and to build and enhance HL in young people in Africa. In addition, taking into consideration the socio-economic and cultural variations, HL tools need to be developed and validated, in the context of African countries, to ensure the better assessment of HL among young people.
Conclusion
This study provided a coherent summary and synthesis of HL among young people in Africa. It indicated that HL studies among young people in Africa are rare. The review of the available eligible studies revealed that low HL was common among young people, although most of these studies were conducted in school/university contexts on students. It also found that there was a significant relationship between low HL and negative health outcomes among young people. It showed that HL among young people was impacted by a wide range of factors, including sex, age, ethnicity, level of education, type of school (private/public), type of college, self-esteem, health condition, financial status, study year, healthcare use experience, cultural values, and awareness. However, owing to several limitations, particularly with regard to the small number of eligible studies and their limited distribution across countries, the sampling design employed in these studies, and their study settings, this review may not give an accurate picture of HL among young people in Africa. Therefore, both primary and secondary HL studies are needed to fully understand HL among young people in Africa and to develop and guide policies and interventions.
Disclosure
The authors of this manuscript declare that there are no conflicts of interest.
References
1. Sørensen K, Van den Broucke S, Fullam J, et al. Health literacy and public health: a systematic review and integration of definitions and models. BMC Public Health. 2012;12(1):1–13. doi:10.1186/1471-2458-12-80
2. Mubarokah K. Health literacy and health behavior in the rural areas. KnE Life Sci. 2018;29:8–16.
3. Kickbusch I, Pelikan JM, Apfel F, Tsouros AD. The Solid Facts: Health Literacy. Denmark: World Health Organization, Regional Office for Europe; 2013.
4. Aaby A, Friis K, Christensen B, Rowlands G, Maindal HT. Health literacy is associated with health behaviour and self-reported health: a large population-based study in individuals with cardiovascular disease. Eur J Prev Cardiol. 2017;24(17):1880–1888. doi:10.1177/2047487317729538
5. Liu Y-B, Liu L, Li Y-F, Chen Y-L. Relationship between health literacy, health-related behaviors and health status: a survey of elderly Chinese. Int J Environ Res Public Health. 2015;12(8):9714–9725. doi:10.3390/ijerph120809714
6. Angus C, Henney M, Webster L, Gillespie D, Street R. Alcohol-Attributable Diseases and Dose-Response Curves for the Sheffield Alcohol Policy Model Version 4.0. Sheffield, UK: ScHARR, University of Sheffield; 2018.
7. Degenhardt L, Charlson F, Ferrari A, et al. The global burden of disease attributable to alcohol and drug use in 195 countries and territories, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Psychiatry. 2018;5(12):987–1012. doi:10.1016/S2215-0366(18)30337-7
8. Paasche-Orlow MK, Wolf MS. The causal pathways linking health literacy to health outcomes. Am J Health Behav. 2007;31(1):S19–S26. doi:10.5993/AJHB.31.s1.4
9. Manafo E, Wong S. Health literacy programs for older adults: a systematic literature review. Health Educ Res. 2012;27(6):947–960. doi:10.1093/her/cys067
10. Koh HK, Berwick DM, Clancy CM, et al. New federal policy initiatives to boost health literacy can help the nation move beyond the cycle of costly “crisis care”. Health Aff. 2012;31(2):434–443. doi:10.1377/hlthaff.2011.1169
11. Eichler K, Wieser S, Brügger U. The costs of limited health literacy: a systematic review. Int J Public Health. 2009;54(5):313–324. doi:10.1007/s00038-009-0058-2
12. Berkman ND, Sheridan SL, Donahue KE, Halpern DJ, Crotty K. Low health literacy and health outcomes: an updated systematic review. Ann Intern Med. 2011;155(2):97–107. doi:10.7326/0003-4819-155-2-201107190-00005
13. Kickbusch IS. Health literacy: addressing the health and education divide. Health Promot Int. 2001;16(3):289–297. doi:10.1093/heapro/16.3.289
14. Bröder J, Okan O, Bollweg TM, Bruland D, Pinheiro P, Bauer U. Child and youth health literacy: a conceptual analysis and proposed target-group-centred definition. Int J Environ Res Public Health. 2019;16(18):3417. doi:10.3390/ijerph16183417
15. Bhagat K, Howard DE, Aldoory L. The relationship between health literacy and health conceptualizations: an exploratory study of elementary school-aged children. Health Commun. 2018;33(2):131–138. doi:10.1080/10410236.2016.1250188
16. Meng L, Maskarinec G, Lee J, Kolonel LN. Lifestyle factors and chronic diseases: application of a composite risk index. Prev Med. 1999;29(4):296–304. doi:10.1006/pmed.1999.0538
17. Graham H, Power C. Childhood Disadvantage and Adult Health: A Lifecourse Framework. London: Health Development Agency; 2004.
18. Peñafiel-Saiz C. Young people, health and the internet. Perceptions, attitudes and motivations of young people in relation to health information. Revista Latina de Comunicación Soc. 2017;72:1317–1340.
19. Cesnaviciene J, Kalinkeviciene A, Ustilaite S. Young adult health literacy on health promotion as social determinant of health: challenges for health education practice in Lithuania. In: Book Young Adult Health Literacy on Health Promotion as Social Determinant of Health: Challenges for Health Education Practice in Lithuania. EDP Sciences; 2018:02005.
20. Fritzell J, Ringbäck Weitoft G, Fritzell J, Burström B. Life course inequalities–generations and social class. Soc Sci Med. 2007;65:2474–2488. doi:10.1016/j.socscimed.2007.06.031
21. Nunes C. Health literacy in younger age groups: health care perceptions: informed people will be more prepared people. Open Access Library J. 2020;7(3):1.
22. Borzekowski D. Considering children and health literacy: a theoretical approach. Pediatrics. 2009;124:S282–S288. doi:10.1542/peds.2009-1162D
23. Velardo S, Drummond M. Emphasizing the child in child health literacy research. J Child Health Care. 2017;21(1):5–13. doi:10.1177/1367493516643423
24. Guo S, Armstrong R, Waters E, et al. Quality of health literacy instruments used in children and adolescents: a systematic review. BMJ Open. 2018;8(6):e020080. doi:10.1136/bmjopen-2017-020080
25. Bröder J, Okan O, Bauer U, et al. Health literacy in childhood and youth: a systematic review of definitions and models. BMC Public Health. 2017;17(1):1–25. doi:10.1186/s12889-016-3954-4
26. Manganello JA. Health literacy and adolescents: a framework and agenda for future research. Health Educ Res. 2008;23(5):840–847. doi:10.1093/her/cym069
27. Rababah JA, Al-Hammouri MM, Drew BL, Aldalaykeh M. Health literacy: exploring disparities among college students. BMC Public Health. 2019;19(1):1–11. doi:10.1186/s12889-019-7781-2
28. Evans A-Y, Anthony E, Gabriel G. Comprehensive health literacy among undergraduates: a Ghanaian university-based cross-sectional study. Health Literacy Res Pract. 2019;3(4):e227–e237.
29. Arksey H, O’Malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol. 2005;8(1):19–32. doi:10.1080/1364557032000119616
30. Moher D, Liberati A, Tetzlaff J, Altman DG, Group P. Reprint—preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Phys Ther. 2009;89(9):873–880. doi:10.1093/ptj/89.9.873
31. World Health Organization. Adolescent Health in the South-East Asia Region. World Health Organization, Regional Office for South-East Asia; 2021.
32. Peters MD, Godfrey C, McInerney P, Munn Z, Tricco AC, Khalil H. Chapter 11: scoping reviews (2020 version). In: Aromataris E, Munn Z, editors. JBI Manual for Evidence Synthesis. The Joanna Briggs Institute; 2020.
33. Amoah PA, Phillips DR, Gyasi RM, Koduah AO, Edusei J. Health literacy and self-perceived health status among street youth in Kumasi, Ghana. Cogent Med. 2017;4(1):1275091. doi:10.1080/2331205X.2016.1275091
34. Amoah PA, Koduah AO, Gyasi RM, Gwenzi GD, Anaduaka US. The relationship between functional health literacy, health-related behaviours, and sociodemographic characteristics of street-involved youth in Ghana. Int J Health Promo Educ. 2019;57(3):116–132. doi:10.1080/14635240.2018.1552835
35. Ewa V. The Association Between Health Literacy and Obesity Among Adolescents in Selected Schools in Adentan Municipality. University of Ghana; 2017.
36. Koduah AO, Amoah PA, Nkansah JO, Leung AY. A comparative analysis of student and practising nurses’ health literacy knowledge in Ghana. In: Book a Comparative Analysis of Student and Practising Nurses’ Health Literacy Knowledge in Ghana. Multidisciplinary Digital Publishing Institute; 2021:38.
37. Adewole KO, Ogunfowokan AA, Olodu M. Influence of health literacy on health promoting behaviour of adolescents with and without obesity. Int J Africa Nurs Sci. 2021;15:100342. doi:10.1016/j.ijans.2021.100342
38. Hamilton-Ekeke J-T, Abam RP, Ogobiri E. Health literacy in the promotion of wellness among secondary school students in Bayelsa State, Nigeria. J Health Educ Teach. 2020;11(1):1–7.
39. Shabi IN, Oyewusi FO. Health literacy and internet health information use among in-school adolescents in Osun State, South-West, Nigeria. J Consum Health Internet. 2018;22(1):25–41. doi:10.1080/15398285.2017.1402636
40. Mostafa A, Abdelzaher A, Rashed S, et al. Is health literacy associated with antibiotic use, knowledge and awareness of antimicrobial resistance among non-medical university students in Egypt? A cross-sectional study. BMJ open. 2021;11(3):e046453. doi:10.1136/bmjopen-2020-046453
41. Pelikan J, Röthlin F, Ganahl K, Peer S. Measuring comprehensive health literacy in general populations—le HLS-EU instruments. In: Book Measuring Comprehensive Health Literacy in General populations—le HLS-EU Instruments. Elsevier; 2014.
42. Wångdahl JM, Mårtensson LI. Measuring health literacy–the Swedish functional health literacy scale. Scand J Caring Sci. 2015;29(1):165–172. doi:10.1111/scs.12125
43. Sørensen K, Van den Broucke S, Pelikan JM, et al. Measuring health literacy in populations: illuminating the design and development process of the European Health Literacy Survey Questionnaire (HLS-EU-Q). BMC Public Health. 2013;13(1):1–10. doi:10.1186/1471-2458-13-948
44. Wångdahl J, Lytsy P, Mårtensson L, Westerling R. Health literacy among refugees in Sweden–a cross-sectional study. BMC Public Health. 2014;14(1):1–12. doi:10.1186/1471-2458-14-1030
45. Chinn D, McCarthy C. All Aspects of Health Literacy Scale (AAHLS): developing a tool to measure functional, communicative and critical health literacy in primary healthcare settings. Patient Educ Couns. 2013;90(2):247–253. doi:10.1016/j.pec.2012.10.019
46. Cormier CM. Health literacy: the knowledge and experiences of senior level baccalaureate nursing students. 2006.
47. Norman CD, Skinner HA. eHEALS: the eHealth literacy scale. J Med Internet Res. 2006;8(4):e27. doi:10.2196/jmir.8.4.e27
48. Warsh J, Chari R, Badaczewski A, Hossain J, Sharif I. Can the newest vital sign be used to assess health literacy in children and adolescents? Clin Pediatr. 2014;53(2):141–144. doi:10.1177/0009922813504025
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.