")
Back to Journals » ClinicoEconomics and Outcomes Research » Volume 6
Health economic analyses in medical nutrition: a systematic literature review
Authors Walzer S, Droeschel D, Nuijten M, Chevrou-Séverac H
Received 27 August 2013
Accepted for publication 17 October 2013
Published 10 March 2014 Volume 2014:6 Pages 109—124
DOI https://doi.org/10.2147/CEOR.S53601
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Stefan Walzer,1,2 Daniel Droeschel,1,3 Mark Nuijten,4 Hélène Chevrou-Séverac5
1MArS Market Access and Pricing Strategy GmbH, Weil am Rhein, Germany; 2State University Baden-Wuerttemberg, Loerrach, Germany; 3Riedlingen University, SRH FernHochschule, Riedlingen, Germany; 4Ars Accessus Medica BV, Amsterdam, the Netherlands, 5Nestlé Health Science, Vevey, Switzerland
Background: Medical nutrition is a specific nutrition category either covering specific dietary needs and/or nutrient deficiency in patients or feeding patients unable to eat normally. Medical nutrition is regulated by a specific bill in Europe and in the US, with specific legislation and guidelines, and is provided to patients with special nutritional needs and indications for nutrition support. Therefore, medical nutrition products are delivered by medical prescription and supervised by health care professionals. Although these products have existed for more than 2 decades, health economic evidence of medical nutrition interventions is scarce. This research assesses the current published health economic evidence for medical nutrition by performing a systematic literature review related to health economic analysis of medical nutrition.
Methods: A systematic literature search was done using standard literature databases, including PubMed, the Health Technology Assessment Database, and the National Health Service Economic Evaluation Database. Additionally, a free web-based search was conducted using the same search terms utilized in the systematic database search. The clinical background and basis of the analysis, health economic design, and results were extracted from the papers finally selected. The Drummond checklist was used to validate the quality of health economic modeling studies and the AMSTAR (A Measurement Tool to Assess Systematic Reviews) checklist was used for published systematic reviews.
Results: Fifty-three papers were identified and obtained via PubMed, or directly via journal webpages for further assessment. Thirty-two papers were finally included in a thorough data extraction procedure, including those identified by a “gray literature search” utilizing the Google search engine and cross-reference searches. Results regarding content of the studies showed that malnutrition was the underlying clinical condition in most cases (32%). In addition, gastrointestinal disorders (eg, surgery, cancer) were often analyzed. In terms of settings, 56% of papers covered inpatients, whereas 14 papers (44%) captured outpatients, including patients in community centers. Interestingly, in comparison with the papers identified overall, very few health economic models were found. Most of the articles were modeling analyses and economic trials in different design settings. Overall, only eight health economic models were published and were validated applying the Drummond checklist. In summary, most of the models included were carried out to quite a high standard, although some areas were identified for further improvement. Of the two systematic health economic reviews identified, one achieved the highest quality score when applying the AMSTAR checklist.
Conclusion: The reasons for finding only a few modeling studies but quite a large number of clinical trials with health economic endpoints, might be different. Until recently, health economics has not been required for reimbursement or coverage decisions concerning medical nutrition interventions. Further, there might be specifics of medical nutrition which might not allow easy modeling and consequently explain the limited uptake so far. The health economic data on medical nutrition generated and published is quite ample. However, it has been primarily based on database analysis and clinical studies. Only a few modeling analyses have been carried out, indicating a need for further research to understand the specifics of medical nutrition and their applicability for health economic modeling.
Keywords: systematic review, medical nutrition, health economics
Introduction
Medical nutrition is a specific nutrition category either covering specific dietary needs and/or nutrient deficiencies in patients or providing nourishment for patients who are unable to eat normally. Medical nutrition is available in different formulations and consistencies, providing energy, protein, fluid, electrolyte, mineral, micronutrient, and fiber needs. It depends on activity levels and the underlying clinical condition, for example, catabolism, pyrexia, gastrointestinal tolerance, potential metabolic instability, risk of refeeding problems, and likely duration of nutrition support, among others. There are different options available for the administration of nutrition support, including oral, enteral, and parenteral formulations, by application of special devices like infusions, tubes, probes, or perfusions. Use of medical nutrition needs skilled health care professionals who are trained in nutritional requirements and methods of nutrition support to ensure that the treatment support given provides a suitable nutrient intake for patients.
Medical nutrition is regulated by a specific bill in both Europe and in the US, with specific legislation and guidelines, and is provided for patients with specific nutritional needs and indications for nutrition support. Therefore, like prescription pharmaceuticals, medical nutrition products are delivered on medical prescription under the supervision of health care professionals.
Although these products have existed for more than 2 decades, the health economic evidence of medical nutrition interventions tends to be scarce. In the field of health technology research, including pharmacoeconomics, health economics research is usually described according to its methods, including cost-effectiveness analysis, cost-utility analysis, and budget impact analyses. In addition, in health economics, research concepts concerning the financial burden of disease are widely used to highlight the financial implications of a disease from the societal perspective at a regional or national level.
To get a better understanding of medical nutrition-related health economics and to advance the greater picture of application of health economics in medical nutrition, this systematic literature review was undertaken to assess the current evidence.
Methods
The research question of particular interest was formulated as: “What is the evidence of health economics in medical nutrition, what concepts are applied, and what is their quality?” The research question was defined in more detail applying the PICO (population [P], intervention [I], comparison [C], and outcome(s) [O]) criteria1 to conduct a literature review most suitable to answer the research question (see Table 1).
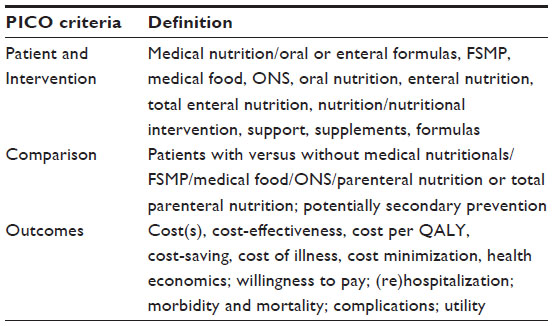 | Table 1 PICO criteria for the systematic literature search |
A systematic literature search was initiated and performed based on a predefined search protocol. Before a final set of search terms was defined, a pilot search was conducted to assess the relevant terms to be included. The following search terms were used at the pilot stage:
- “health economics”, “cost of illness”, “cost minimization”, “cost(s)”, “cost-effectiveness”, “cost utility”, “budget impact”
- “medical nutrition”, “medical food”, “FSMP”, “EN”, “nutritional support/supplement”.
Finally, some preliminary considerations were made regarding feasibility and in order to not compromise the results. Hence, it was validated that the same results could be gained when using the term “cost” with different wordings as a search term, eg, in comparison with “costs”, “cost of illness”, “cost minimization”, cost-effectiveness”, “cost utility”, and “cost benefit”. Consequently, the term “economic assessment” was taken out because this was also captured under the term “health technology assessment”; the same was true for the term “cost(s)” because this was captured by all cost papers with the other terms. Additionally, the term “health economics” was not considered because it was seen that only health policy papers turned out. Relevant papers which would have shown up under these terms were also captured by the other search terms used. Finally, it was decided to take out the term “oral nutrition supplement” because this was shown to be covered by the term “nutrition(al) supplement”. Final search terms were identified accordingly:
- terms “a” for medical nutrition included economics: a1) economic evaluation; a2) health technology assessment; a3) cost effectiveness; a4) cost of illness; a5) cost minimization; a6) cost benefit; a7) cost utility; a8) budget impact
- terms “b” for medical nutrition were defined as follows: b1) medical food; b2) medical nutrition; b3) nutritional support; b4) nutrition supplement; b5) enteral nutrition; b6) food for special medical purpose; b7) FSMP.
Terms covered with “a” were then combined with all terms “b” during the actual systematic literature search. In order to narrow the search to more recent relevant articles, only papers published between 2000 and 2012 and in the Dutch, English, French, German, Italian, or Spanish language were included in the final review process.
Full-text publications were obtained for abstracts that met the predefined inclusion criteria. Abstracts that did not meet the search criteria were excluded. Based on these full-text reports, it was decided whether each study met the selection criteria. The area of interest was therefore defined as: only articles with content related to food for special medical purpose (EU terminology [FSMP]) or medical food (US terminology), known as medical nutrition in an oral or enteral format. Further, this search was solely focused on health economic data in the context of medical nutrition, so only papers with an explicit health economic content, verified by the common methods applied, met the selection criteria and were assessed further. Publications without a health economic component/analysis were excluded.
The relevant data in the identified papers were captured on a data extraction sheet. All health economic (modeling) studies identified were assessed for quality using the Drummond checklist.2 Further, all reviews identified were assessed using the AMSTAR (A Measurement Tool to Assess Systematic Reviews) checklist.3
Results
A first run of the systematic literature search was done in PubMed using a search strategy with sequenced search loops whereby each term could be searched individually (see Figure 1). Utilization of the connected terms by Boolean operator were utilized and a second run (for “true” findings) was run. For the terms “FSMP”, “food for special medical purpose”, and “enteral nutrition”, it was felt not to be meaningful to use the same Boolean operators due to the already limited number of findings. Hence, it seemed to be more useful to connect the latter term with another Boolean operator, ie, “NOT”. The results for any economic term in combination with “FSMP” or with “food for special medical purpose” appeared as “0”. The only exception, ie, “food for special medical purpose” AND “economic evaluation”, yielded an output of “1”. In total, 38 articles were identified using this process and were subjected to further investigation. In a third search sequence, each economic term was searched in combination with nutritional terms. In total, 419 articles were identified for further investigation, including those of the first two search loops.
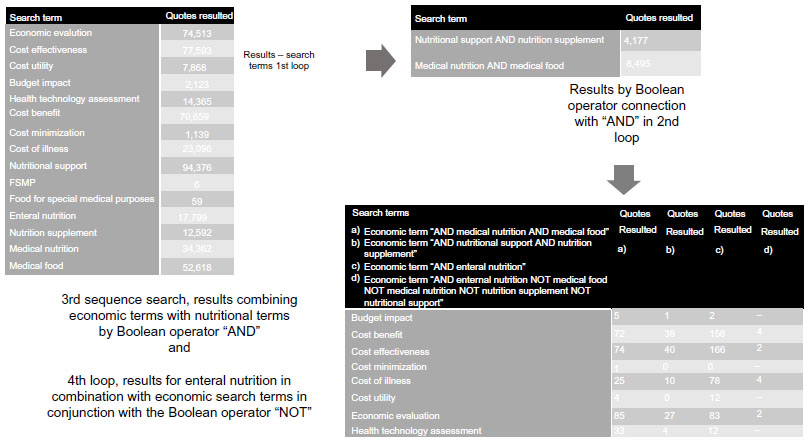 | Figure 1 Process and findings of the systematic literature search for health economics in medical nutrition. |
Another search within the National Health Service Economic Evaluation Database was conducted specifically for the economic term “economic evaluation” in combination with all “nutritional” terms. This was appropriate given that this database is a repository only for economic evaluations. For this search, 75 articles were retrieved for further investigation.
A search of the Health Technology Assessment Database was done only for the economic term “health technology assessment” in combination with all nutritional terms. This was considered appropriate because this database is a repository only for health technology assessments. Used in addition to the term “enteral nutrition”, no other nutrition search term provided any result. Twenty articles were identified for further investigation.
Within the fourth and final search loop for the 553 papers identified, the abstracts were analyzed for individual search terms and checked for alternative wording and variations within the context. Papers that included health economic data in conjunction with medical nutrition(s) were included in the further assessment. Within this final step, all duplications were identified. In total, 328 articles were excluded. A total of 225 abstracts were identified for the detailed review and the data were inserted into a data extraction sheet.
Within this narrative scrutiny of the data, all articles with a focus on primary prevention were excluded, as well as all articles solely focusing on clinical data without a health economic component/analysis. For the abstracts that finally met the predefined inclusion criteria, full-text publications were obtained.
Fifty-three articles were identified and obtained via PubMed, or directly via the journal webpage for further assessment. After a detailed review of the full-text papers, 32 publications were included in a thorough data extraction procedure, including those identified by a “gray literature search” utilizing the Google search engine and cross-reference searches.
Clinical basis for evaluation and setting
When checking the clinical basis, it appeared that malnutrition was the underlying disease covered in most papers. In addition, gastrointestinal disorders (eg, surgery, cancer) were often included. More importantly, a rather large mix of different diseases were the subject of various studies, so it is rather difficult to determine a trend except for the two categories just mentioned.
However, reviewing the results of the identified studies (see Figure 2), it became apparent that the majority of studies included interventions using enteral nutrition and oral nutritional support (seven and nine, respectively) with standard of care and parenteral nutrition as the comparator (ten and six, respectively).
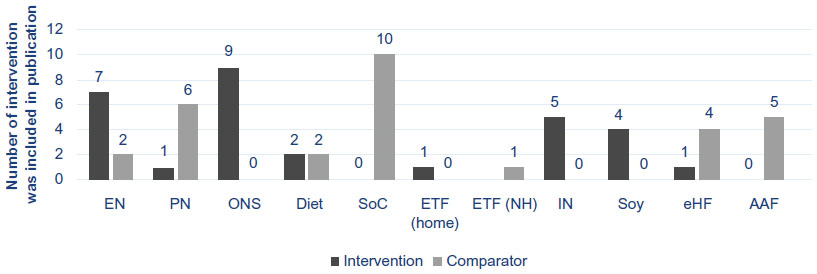 | Figure 2 Interventions and comparators included in the health economic analyses identified by a systematic literature search. |
In terms of settings, 63% of papers (20 studies) covered inpatients whereas 41% of papers (14 studies) captured outpatients, including patients in community centers. When analyzing the countries where the studies were conducted, most of the papers were from the US and UK (seven studies each, together comprising 44% of all studies included). The Netherlands and Italy followed, with five and four papers, respectively, even though in both countries the same groups of researchers dominated those papers (Nuijten et al4 in the Netherlands and Braga et al5 in Italy). Most other countries had only one paper, with the exception of Germany, which had three.
Specific indications
In order to draw indication and disease-specific conclusions, the results were divided into the following areas: malnutrition, gastrointestinal surgery, cow milk protein allergy (CMPA), and others.
Malnutrition
Of the extracted papers, roughly one third (eleven papers, 34%) covered the indication of malnutrition. Prerequisite, according to the particular interest of this survey, the papers identified covered the indication of malnutrition related to patients in developed countries only, as opposed to the common definition of malnutrition in developing countries. Of the eleven studies identified, five included hospitalized patients only, two included outpatients only, and three papers stated that community-based patients were included. Most of those papers considered more than one health economic endpoint. Six studies evaluated a form of cost analyses (eg, total cost, physician cost, prescription cost), and three had cost-effectiveness (or cost-utility) analyses defined as an endpoint. Budget impact and length of stay were each the subject of two papers. The economic results reported introduction of oral nutritional support as being cost-effective, even though the incremental cost-effectiveness ratios ranged significantly between studies. Interestingly, even though the introduction of oral nutritional support in comparison with a standard of care approach normally generates higher costs (and more efficacy), it was shown by different authors to be cost-saving from a budget impact perspective.
Gastrointestinal surgery
The second most studied indication identified was gastrointestinal surgery (nine studies, 28%). One paper was a systematic review, and the remaining eight had a direct hospital perspective. One paper had a national perspective, although also covering the hospital setting. All papers including the total cost of treatment as well as the cost of potential complications concluded that medical nutrition was superior in terms of cost over any comparator. Budget impact analyses showed similar results. In a few studies, cost-effectiveness results were also presented, and were also in favor of oral nutritional support. However, these results need to be interpreted with caution because no incremental cost-effectiveness ratios were calculated or provided.
Cow milk protein allergy
Another disease area, primarily analyzed by one research group led by Guest (see Table 2, studies 25–30) was CMPA. All studies were based in the community health care setting. In each of the studies, a decision model was used, including specific country input data, although the base case clinical and economic data were provided from a real-life UK database. Studies for the UK, Finland, Australia, the Netherlands, and South Africa descriptively analyzed the budget impact and cost situation for the health care systems, newly introducing a treatment for patients with CMPA. Cost-effectiveness or cost-comparison analyses were missing. In conclusion, the authors reported the current cost of managing those patients. Further, in some countries, they showed that inclusion of clinical nutrition in the reimbursement schemes would result in cost savings due to lower follow-up costs.
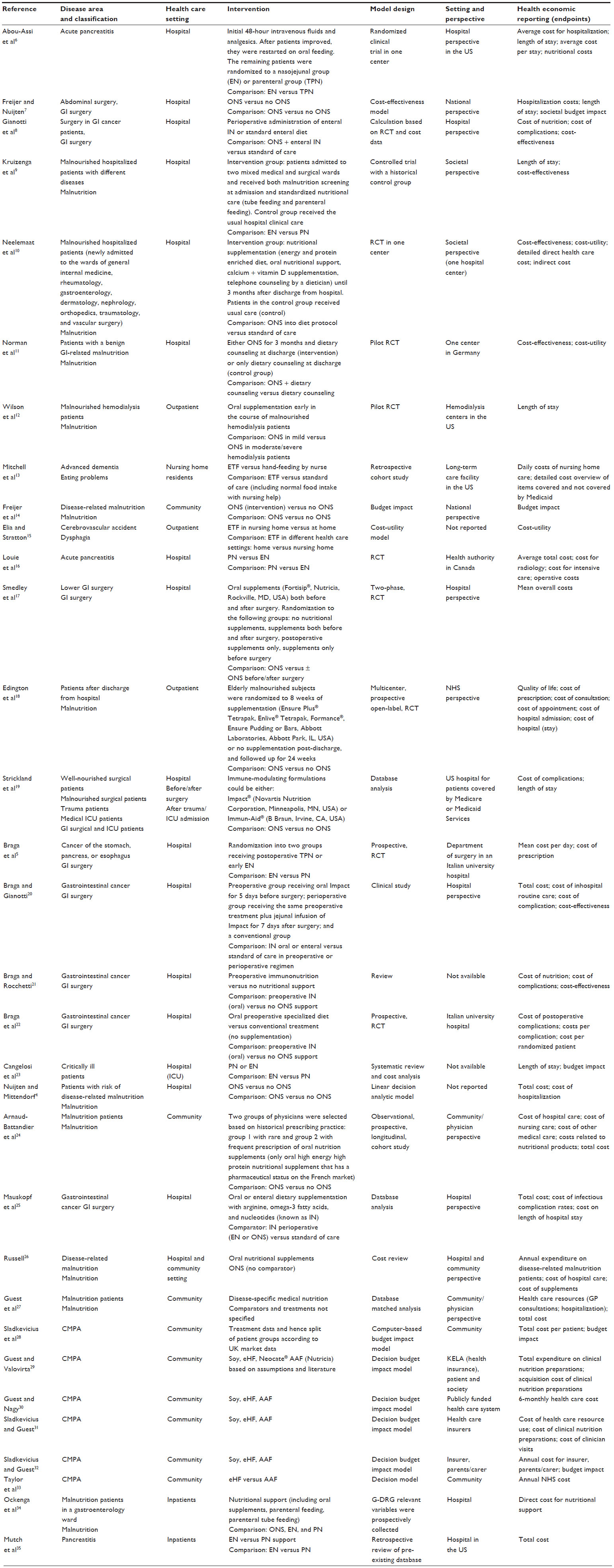 | Table 2 Detailed overview of papers identified with respect to key study items |
Other indications
In addition to the three most analyzed disease areas, some studies covered the following areas: pancreatitis, eating problems, dysphagia, and critically ill patients. For pancreatitis, two different studies were performed and both showed that enteral feeding was cost-saving in comparison with parenteral feeding. Such a cost-saving has also been found in critically ill patients. An analysis of patients with advanced dementia and eating problems showed that support with feeding tubes was cost-saving. For dysphagia, administration of enteral feeding tube was compared to normal diet while delivered at home versus nursing home. The analysis demonstrated that enteral tube feeding is cost-effective compared to no intervention independent of the setting.
Modeling approaches
In comparison with the articles identified overall, only a very few health economic model analyses were found. Overall, eleven models (34% of all studies extracted) were published, of which only eight could be considered health economic models and could be validated applying the Drummond checklist within this survey (see Table S1). The others usually did not describe their cost and modeling approach and therefore could not be fully identified as health economic models. Most of the papers that included health economic outcomes in medical nutrition were studies using different methods, eg, randomized controlled trials, observational trials, or cluster studies. Thirteen studies were identified, corresponding to 38% of all identified papers. Other designs included reviews, database analyses, and population-based models. All details of the selected papers can be seen in Table 2.
For all the health economic modeling papers selected, a study quality assessment was conducted using the Drummond checklist (for details, see Table S1). Overall, the included models were implemented with quite a high standard of quality, even though some areas were identified for further improvement (eg, sensitivity analysis and databases). Further, in the papers reported by Guest and Nagy30 in 2009 and Guest et al27 in 2011, the main weaknesses was poor reporting of the underlying and used effectiveness basis in the models.
Two systematic reviews on health economic studies in medical nutrition were found during the literature search process, and the AMSTAR checklist was used to assess them. Of these reviews, the one by Cangelosi et al23 achieved the highest quality scores applying the AMSTAR checklist (for details, see Table S2). Most questions could be answered, and the paper included all relevant information. An important difference between this review and the one published by Braga and Rocchetti21 in 2011 was that Canegelosi et al also searched the gray literature and reported both included and excluded studies.
Discussion
A couple of cost-effectiveness, cost comparison, and budget impact analyses were published in recent years. However, most of the cost-effectiveness (cost utility) analyses normally being published were based on health economic models and not actually run semi-clinical studies with a health economic endpoint as it was shown in the retrieved evidence for medical nutrition. As this systematic literature search has shown, potential reasons for such a difference might be that there is not only interest in health economics and its application in medical nutrition, but also some activities ongoing, increasingly adopting the use of health economic modeling. Further burdens compared with the established pharmaceutical and medical device regulations might include differences in terms of reimbursement and market access requirements for medical nutrition products. This seems especially true given that cost-effectiveness analyses were mainly associated with drug and medical device reimbursement decisions, where, in many countries, financial considerations of affordability may be as important as clinical efficacy and cost-effectiveness.36
Conclusion
The health economic data on medical nutrition generated and published is quite ample. However, they have been primarily based on database analysis and clinical studies. Few modeling analyses have been carried out, indicating a need for further research to understand the specifics of medical nutrition and their applicability in health economic modeling.
Disclosure
This study was funded by Nestlé Health Science. The authors have no other conflicts of interest in this work.
References
Thabane L, Thomas T, Ye C, Paul J. Posing the research question: not so simple. Can J Anaesth. 2009;56(1):71–79. | |
Drummond M, O’Brien B, Stoddart GL, Torrance GW, editors. Methods for the Economic Evaluation of Health Care Programmes. 2nd ed. Oxford, UK: Oxford University Press; 1997. | |
Shea BJ, Grimshaw JM, Wells GA, et al. Development of AMSTAR: a measurement tool to assess the methodological quality of systematic reviews. BMC Med Res Methodol. 2007;7:10. | |
Nuijten MJC, Mittendorf T. [The health economic impact of oral nutritional supplements in Germany]. Aktuel Ernahrungsmed. 2012;37:126–133. German. | |
Braga M, Gianotti L, Gentilini O, Parisi V, Salis C, Di Carlo V. Early postoperative enteral nutrition improves gut oxygenation and reduces costs compared with total parenteral nutrition. Crit Care Med. 2001;29:242–248. | |
Abou-Assi S, Craig K, O’Keefe SJ. Key issues in the success of community-based management of severe malnutrition. Food Nutr Bull. 2006;27(Suppl 3):S49–S82. | |
Freijer K, Nuijten MJ. Analysis of the health economic impact of medical nutrition in The Netherlands. Eur J Clin Nutr. 2010;64:1229–1234. | |
Gianotti L, Braga M, Frei A, Greiner R, Di Carlo V. Health care resources consumed to treat postoperative infections: cost saving by perioperative immunonutrition. Shock. 2000;14:325–330. | |
Kruizenga HM, Van Tulder MW, Seidell JC, Thijs A, Ader HJ, van Bokhorst-de van der Schueren MA. Effectiveness and cost-effectiveness of early screening and treatment of malnourished patients. Am J Clin Nutr. 2005;82:1082–1089. | |
Neelemaat F, Bosmans JE, Thijs A, Seidell JC, van Bokhorst-de van der Schueren MA. Oral nutritional support in malnourished elderly decreases functional limitations with no extra costs. Clin Nutr. 2012;31:183–190. | |
Norman K, Pirlich M, Smoliner C, et al. Cost-effectiveness of a 3-month intervention with oral nutritional supplements in disease-related malnutrition: a randomised controlled pilot study. Eur J Clin Nutr. 2011;65:735–742. | |
Wilson B, Fernandez-Madrid A, Hayes A, Hermann K, Smith J, Wassell A. Comparison of the effects of two early intervention strategies on the health outcomes of malnourished hemodialysis patients. J Ren Nutr. 2001;11:166–171. | |
Mitchell SL, Buchanan JL, Littlehale S, Hamel MB. Tube-feeding versus hand-feeding nursing home residents with advanced dementia: a cost comparison. J Am Med Dir Assoc. 2003;4:27–33. | |
Freijer K, Nuijten MJ, Schols JM. The budget impact of oral nutritional supplements for disease related malnutrition in elderly in the community setting. Front Pharmacol. 2012;3:78. | |
Elia M, Stratton RJ. A cost-utility analysis in patients receiving enteral tube feeding at home and in nursing homes. Clin Nutr. 2008;27:416–423. | |
Louie BE, Noseworthy T, Hailey D, Gramlich LM, Jacobs P, Warnock GL. 2004 MacLean-Mueller prize enteral or parenteral nutrition for severe pancreatitis: a randomized controlled trial and health technology assessment. Can J Surg. 2005;48:298–306. | |
Smedley F, Bowling T, James M, et al. Randomized clinical trial of the effects of preoperative and postoperative oral nutritional supplements on clinical course and cost of care. Br J Surg. 2004;91:983–990. | |
Edington J, Barnes R, Bryan F, et al. A prospective randomised controlled trial of nutritional supplementation in malnourished elderly in the community: clinical and health economic outcomes. Clin Nutr. 2004;23:195–204. | |
Strickland A, Brogan A, Krauss J, Martindale R, Cresci G. Is the use of specialized nutritional formulations a cost-effective strategy? A national database evaluation. JPEN J Parenter Enteral Nutr. 2005;29(Suppl 1):S81–S91. | |
Braga M, Gianotti L. Preoperative immunonutrition: cost-benefit analysis. JPEN J Parenter Enteral Nutr. 2005;29(Suppl 1):S57–S61. | |
Braga M, Rocchetti S. Preoperative immunonutrition: cost-benefit analysis. In: Watson RR, Gerald JK, Preed VR. Nutrients, Dietary Supplements, and Nutriceuticals: Cost Analysis Versus Clinical Benefits. 1st ed. New York, NY, USA: Humana Press; 2011. | |
Braga M, Gianotti L, Vignali A, Schmid A, Nespoli L, Di Carlo V. Hospital resources consumed for surgical morbidity: effects of preoperative arginine and omega-3 fatty acid supplementation on costs. Nutrition. 2005;21:1078–1086. | |
Cangelosi MJ, Auerbach HR, Cohen JT. A clinical and economic evaluation of enteral nutrition. Curr Med Res Opin. 2011;27:413–422. | |
Arnaud-Battandier F, Malvy D, Jeandel C, et al. Use of oral supplements in malnourished elderly patients living in the community: a pharmaco-economic study. Clin Nutr. 2004;23:1096–1103. | |
Mauskopf JA, Candrilli SD, Chevrou-Séverac H, Ochoa JB. Immunonutrition for patients undergoing elective surgery for gastrointestinal cancer: impact on hospital costs. World J Surg Oncol. 2012;10:136. | |
Russell CA. The impact of malnutrition on healthcare costs and economic considerations for the use of oral nutritional supplements. Clin Nutr. 2007;Suppl 1:25–32. | |
Guest JF, Panca M, Baeyens J-P, et al. Health economic impact of managing patients following a community-based diagnosis of malnutrition in the UK. Clin Nutr. 2011;30:422–429. | |
Sladkevicius E, Nagy E, Lack G, Guest JF. Resource implications and budget impact of managing cow milk allergy in the UK. J Med Econ. 2010;13:119–128. | |
Guest JF, Valovirta E. Modelling the resource implications and budget impact of new reimbursement guidelines for the management of cow milk allergy in Finland. Curr Med Res Opin. 2008;24:1167–1177. | |
Guest JF, Nagy E. Modelling the resource implications and budget impact of managing cow milk allergy in Australia. Curr Med Res Opin. 2009;25:339–349. | |
Sladkevicius E, Guest JF. Budget impact of managing cow milk allergy in The Netherlands. J Med Econ. 2010;13:273–283. | |
Sladkevicius E, Guest JF. Modelling the health economic impact of managing cow milk allergy in South Africa. J Med Econ. 2010;13:257–272. | |
Taylor RR, Sladkevicius E, Panca M, Lack G, Guest JF. Cost-effectiveness of using an extensively hydrolysed formula compared to an amino acid formula as first-line treatment for cow milk allergy in the UK. Pediatr Allergy Immunol. 2012;23:240–249. | |
Ockenga J, Freudenreich M, Zakonsky R, Norman R, Pirlich M, Lochs H. Nutritional assessment and management in hospitalised patients: implication for DRG-based reimbursement and health care quality. Clin Nutr. 2005;24:913–919. | |
Mutch KL, Heidal KB, Gross KH. Cost-analysis of nutrition support in patients with severe acute pancreatitis. Int J Health Care Qual Assur. 2011;24:540–547. | |
Schoonveld E. The Price of Global Health. Farnham, UK: Gower Publishing Ltd; 2011. |
Supplementary materials
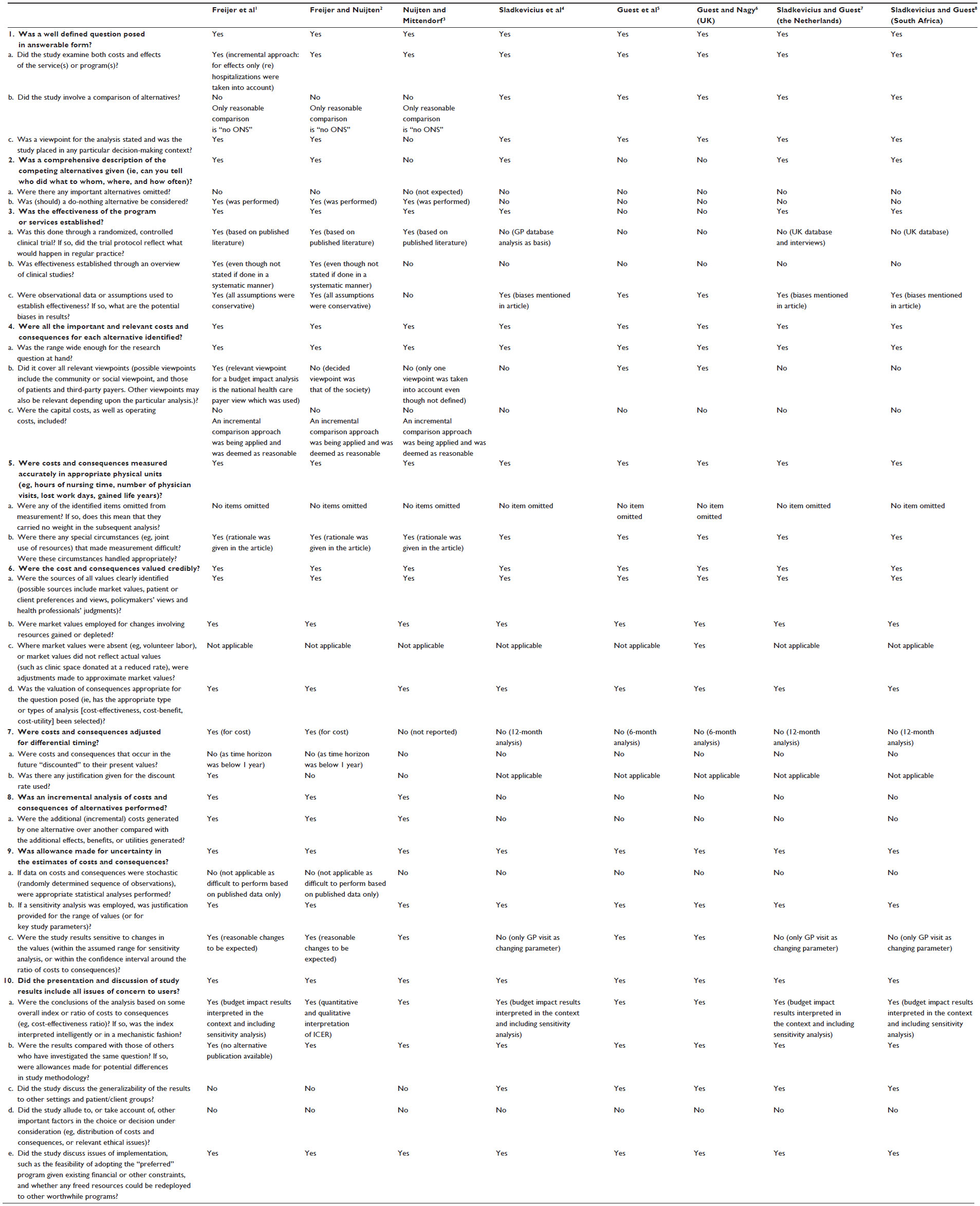 | Table S1 Quality assessment of health economic modeling studies according to the Drummond checklist |
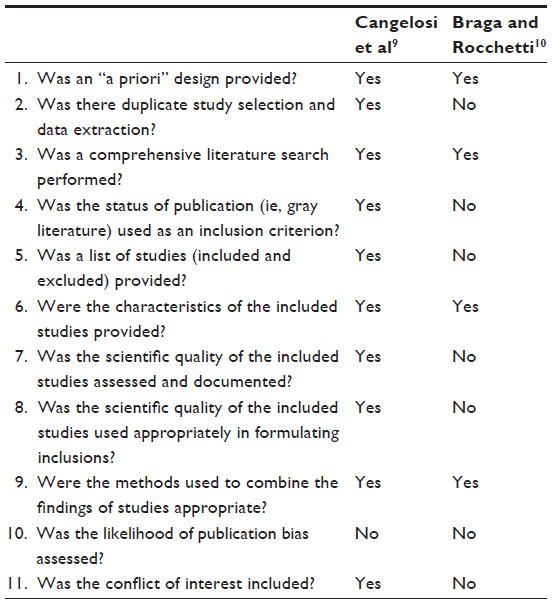 | Table S2 Health economic review quality assessment applying the AMSTAR (A Measurement Tool to Assess Systematic Reviews) checklist |
References
Freijer K, Nuijten MJ, Schols JM. The budget impact of oral nutritional supplements for disease related malnutrition in elderly in the community setting. Front Pharmacol. 2012;3:78. | |
Freijer K, Nuijten MJ. Analysis of the health economic impact of medical nutrition in The Netherlands. Eur J Clin Nutr. 2010;64:1229–1234. | |
Nuijten MJC, Mittendorf T. [The health economic impact of oral nutritional supplements in Germany]. Aktuel Ernahrungsmed. 2012;37:126–133. German. | |
Sladkevicius E, Nagy E, Lack G, Guest JF. Resource implications and budget impact of managing cow milk allergy in the UK. J Med Econ. 2010;13:119–128. | |
Guest JF, Panca M, Baeyens J-P, et al. Health economic impact of managing patients following a community-based diagnosis of malnutrition in the UK. Clin Nutr. 2011;30:422–429. | |
Guest JF, Nagy E. Modelling the resource implications and budget impact of managing cow milk allergy in Australia. Curr Med Res Opin. 2009;25:339–349. | |
Sladkevicius E, Guest JF. Budget impact of managing cow milk allergy in The Netherlands. J Med Econ. 2010;13:273–283. | |
Sladkevicius E, Guest JF. Modelling the health economic impact of managing cow milk allergy in South Africa. J Med Econ. 2010;13:257–272. | |
Cangelosi MJ, Auerbach HR, Cohen JT. A clinical and economic evaluation of enteral nutrition. Curr Med Res Opin. 2011;27:413–422. | |
Braga M, Rocchetti S. Preoperative immunonutrition: cost-benefit analysis. In: Watson RR, Gerald JK, Preed VR. Nutrients, Dietary Supplements, and Nutriceuticals: Cost Analysis Versus Clinical Benefits. 1st ed. New York, NY, USA: Humana Press; 2011. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.