")
Back to Journals » Risk Management and Healthcare Policy » Volume 15
Health Care Waste Management and Associated Factors During Covid-19 Pandemic Among Public Health Facilities in Hadiya Zone, Southern Ethiopia: A Cross-Sectional Study
Authors Berhanu S , Beyamo A , Desalegn T
Received 1 May 2022
Accepted for publication 17 August 2022
Published 22 August 2022 Volume 2022:15 Pages 1553—1559
DOI https://doi.org/10.2147/RMHP.S370438
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Solomon Berhanu,1 Abera Beyamo,2 Tariku Desalegn3
1Department of Biotechnology, College of Natural and Computational Sciences, Wachemo University, Hosaena, Southern Ethiopia; 2School of Public Health, College of Medicine and Health Sciences, Wachemo University, Hosaena, Southern Ethiopia; 3School of Medicine, College of Medicine and Health Sciences, Wachemo University, Hosaena, Southern Ethiopia
Correspondence: Abera Beyamo, School of Public Health, College of Medicine and Health Sciences, Wachemo University, P.O.Box 667, Hosaena, Southern Ethiopia, Tel +251923371542, Email [email protected]
Background: During the SARS-CoV-2 epidemic, also known as the COVID-19 pandemic, developing and poor African countries face severe challenges in controlling infectious trash. As a result, the goal of this report is to assist decision-makers in determining the waste management approach accessible during the COVID-19 epidemic.
Objective: To assess health-care waste management and associated variables in public health institutions in Hadiya Zone, Southern Ethiopia, during the covid-19 pandemic.
Methods: A facility-based cross-sectional study was undertaken at public health facilities in the Hadiya zone from March 15 to March 30, 2021. The information gathered was entered into EpiData software (version 3.1). SPSS software was used to conduct the analysis (version 20). We computed descriptive statistics. At 95% confidence intervals, a p-value of 0.05 was considered statistically significant for health care waste management.
Results: A total of 411 people participated, with a response rate of 97.8%. The overall proportion of acceptable health care waste management was 231% (56.2%). In multivariable logistic regression, study participants with 5 years of service were 1.59 times more likely than their counterparts to handle health care waste appropriately (AOR 95% CI=1.59(1.02– 2.48)). Those who received waste management training were 1.94 times more likely than their counterparts. Those who had enough PPE were 2.14 times more likely than those who did not to handle health care waste appropriately (AOR 95% CI=2.14(1.35– 3.34)).
Conclusions and Recommendation: The proportion of acceptable health care waste management was found to be low in the study. Service year, waste management training, the availability of suitable personal protective equipment (PPE), and prior waste-related injury experience are all required. It is advised that health-care facility administration offer training and personal protection equipment for healthcare workers.
Keywords: COVID-19, waste management in health care, solid waste
Introduction
The term “health care waste” refers to a facility’s whole waste stream, which includes both potentially infectious and non-infectious trash. Infectious waste includes infected sharps and infectious non-sharp materials. Infectious Sharps include things like syringes and other needles, knives, infusion sets, broken glass, and other objects that might cause direct damage. Infectious non-sharps include contaminated materials that have come into contact with human blood or derivatives, bandages, swabs, or items soaked in blood, isolation wastes from highly infectious patients (including food residues), used and obsolete vaccine vials, bedding, and other contaminated materials infected with human pathogens. Non-infectious wastes are items that have not come into contact with patients, such as paper and plastic packaging, metal, glass, and other household debris.1
COVID-19 exacerbates the problem of waste management in developing countries. Inadequate and incorrect medical waste treatment can have serious public health consequences as well as a significant environmental impact. Sound waste management is thus a vital component of environmental and health protection, in addition to municipal solid waste (MSW) and other fast expanding waste streams such as electronic rubbish (E-waste), construction and demolition (C&D) waste, and industrial waste. The importance of good healthcare waste management has garnered even more attention since the recent discovery of the COVID-19 pandemic in late 2019.2 Starting with source segregation, storage, collection/transport, treatment, and final disposal, proper management of healthcare waste must be based on waste hierarchy principles and consider integrated and/or holistic management.3
The coronavirus illness (COVID-19) outbreak in late 2019 is much more than a worldwide health emergency. It has a significant impact on our society and economies, as well as our daily lives. In March 2020, the World Health Organization (WHO) proclaimed the COVID-19 outbreak a pandemic,2 and the number of victims is still quickly increasing over the world. While safeguarding lives and restoring livelihoods are at the forefront of national and municipal policies and actions, proper waste management, including household, healthcare, and other hazardous waste, is a critical civic function that helps to mitigate potential health and environmental consequences.1,2,4
Developing countries are disproportionately prone to waste management problems during the epidemic. As a result, developing countries and cities are fighting COVID-19 while also preventing threats to the environment and human health, including those posed by COVID-19-related garbage, including those posed by waste employees.3,5
Health-care facilities are one of the major areas that has seen tremendous improvement in recent decades all around the world.6 Health-care activities, on the other hand, can result in the development of numerous types of waste, which can have negative consequences for human health and the environment.2,7 Wastes generated by health-care facilities and laboratories are known as health-care wastes.2,8 Sharps, non-sharps, blood, body parts, chemicals, medications, medical gadgets, and radioactive materials are all examples of these wastes. The majority of these materials are toxic, damaging, carcinogenic, and infectious.
Health-care waste makes up around 1–2% of urban garbage, which is a major public health concern since it endangers both human and environmental health.9
Despite the fact that current medical waste management techniques differ from hospital to hospital, the problematic regions are the same in all health-care facilities. According to a review of hospital waste management in 22 developing nations, the proportion of healthcare facilities using unsuitable waste disposal methods ranges from 18% to 64%.9,10 Healthcare personnel, janitors, patients, and the hospital environment are all affected by poor waste management practices.10
In recent decades, health-care waste management has received insufficient attention in economically developing countries. Many findings on health-care waste management in underdeveloped nations found that trash segregation, collection, and storage in isolated areas were not sufficient.1,5 In Ethiopia, health care facilities are expanding faster than ever before in order to meet the community’s fundamental health needs and accomplish the Sustainable Development Goals (SDG).11
The best way to stop the spread of the infectious disease is to use effective health care waste management practices. SNNPR, on the other hand, has done very little research on health-care waste management. To comprehend the gap and reinforce existing solutions, it’s crucial to determine the level of health care waste management and identify its factors. As a result, the aim of the research is to find out how public health officials in Hadiya Zone handle medical waste and what factors influence them.
Methods and Materials
Study Area, Period, and Design
The facility-based cross-sectional study was done in public health facilities in Hadiya zone, southern Ethiopia, from March 15 to March 30, 2021. Hadiya zone is part of the SNNP regional state, which is 194 kilometers south of Hawasa, the southern regional state’s capital, and 230 kilometers southwest of Addis Ababa, Ethiopia’s capital. The zone’s anticipated population for 2020/2021 was roughly 1,573,841, according to data acquired from the zonal health department. There is one comprehensive hospital, three primary hospitals, 61 health facilities, and 305 health posts.
Study Population and Sampling
The sample size will be calculated using a single population proportion formula, with 53.5%11 of public health institutions having good waste management practices, a 95% confidence level, and a margin of error of 5%, n = (Zα/2)2 p(1-p)/d2 = (1.96)2 (0.535*0.465)/(0.05)2 = 382. With the inclusion of 10% non-response, the final sample size is 420. Randomly selected health professionals from Hadiya Zone public health facilities took part in the study. The information was gathered from 65 public health facilities in the Hadiya zone. The whole sample was distributed proportionally to each of the health institutions in the zone based on the size of their health care workers. Then, using a simple random sampling procedure, health care workers were chosen.
Data Collection Technique and Instrument
A self-administered structured questionnaire was used to collect data. Eight diploma nurses and four BSc in health supervisors were hired as data collectors and supervisors, respectively. The respondent’s socio-demographic and socioeconomic variables, as well as health care facility-related features and knowledge-related qualities, are all included in the questionnaire.
Data Quality Control
The English version of the questionnaire was translated into Amharic, and then back translated by other people to guarantee that no meaning was lost and that the consistency was maintained.
Before the actual data collecting days, the questionnaire was pre-tested on 5% of the sample in Silte Zone public health care facility staff. Data collectors and supervisors were also intensively trained in data gathering over two days. During data collection, supervisors and principal investigators checked the filled questionnaire at the end of each day for completeness.
Result
Socio-Demographic Characteristics
Four hundred eleven (411) participants responded with a response rate of 97.8%. Two hundred sixty-eight (65.1%) of health care providers were degree in educational status. Two hundred fifty-seven (62.5%) of the study participants have 6 years and above of work experience. Two hundred twenty-eight (64.2%) of the study participants were female in sex. Two hundred thirty-two (65.4%) were married and two hundred twenty-two (62.5%) were Hadiya by ethnic group (Table 1).
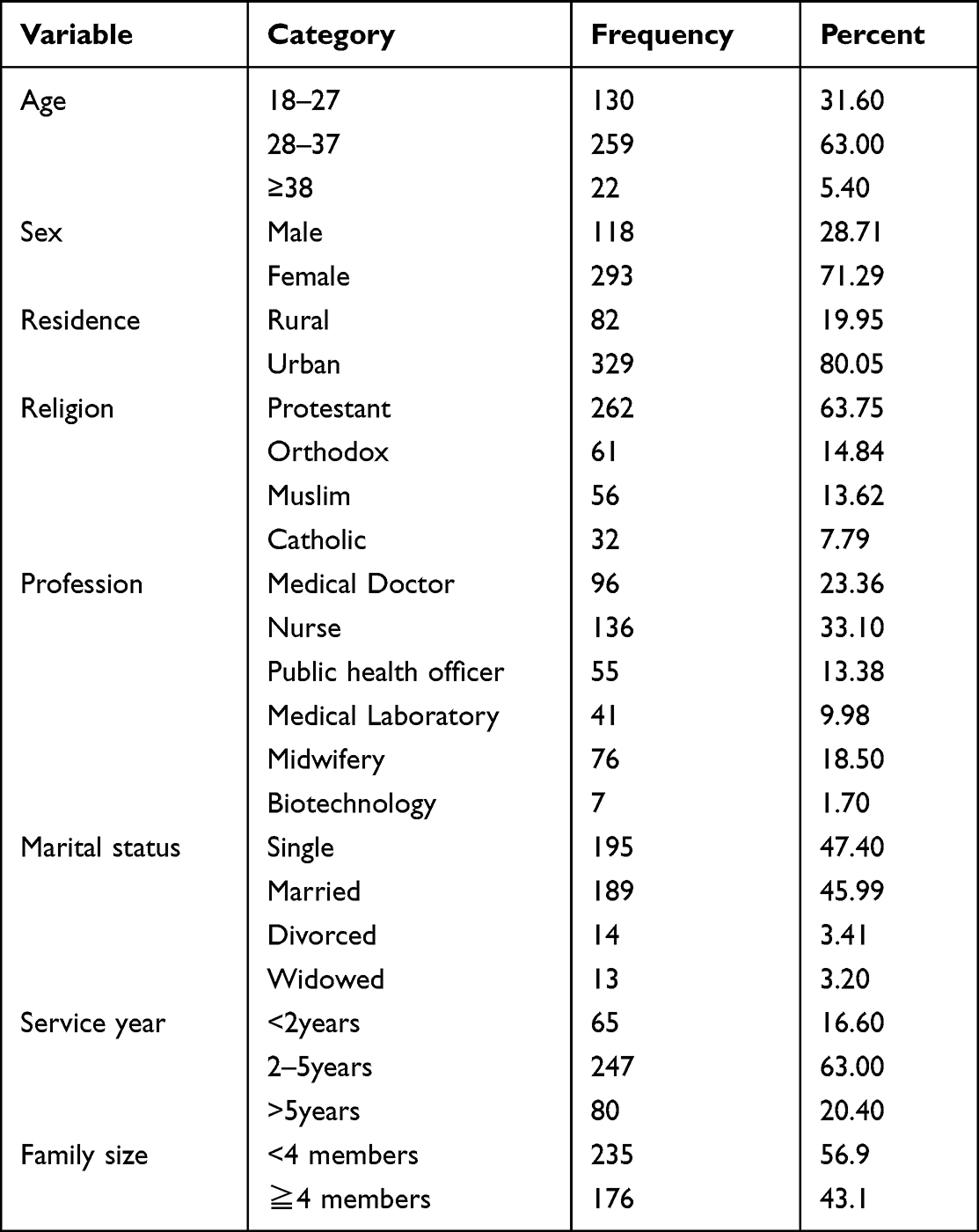 |
Table 1 Socio Demographic Characteristics of Health Care Waste Management and Associated Factors During Covid-19 Pandemic Among Public Health Facilities in Hadiya Zone, Southern Ethiopia, April, 2021 (n=411) |
Facility Related Characteristics
Of the study participants, 209 (50.85%) did not get training on waste management, 294 (71.50%) did not know the presence of waste management rules in their facility, 285 (69.30%) did not know the availability of health care waste management committee in the facility, 224 (54.50%) have reported that there is no regular training on waste management for the staffs, 264 (64.20%) did not have Personal Protective Equipment (PPE), and 75 (18.25%) experienced waste-related injuries (Table 2).
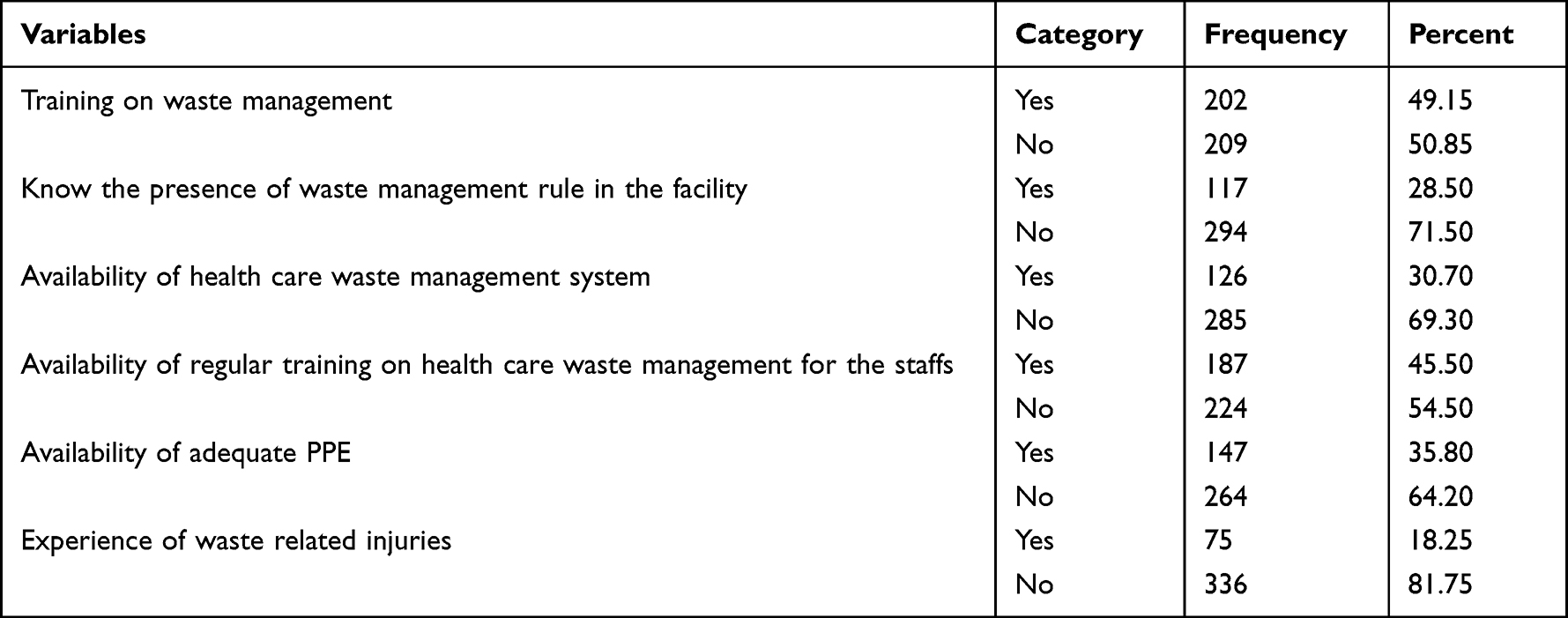 |
Table 2 Facility Related Characteristics of Health Care Waste Management and Associated Factors During Covid-19 Pandemic Among Public Health Facilities in Hadiya Zone, Southern Ethiopia, April, 2021 (n=411) |
Prevalence of Health Care Waste Management
The overall prevalence of appropriate health care waste management in this study was 231 (56.2%) (See Figure 1).
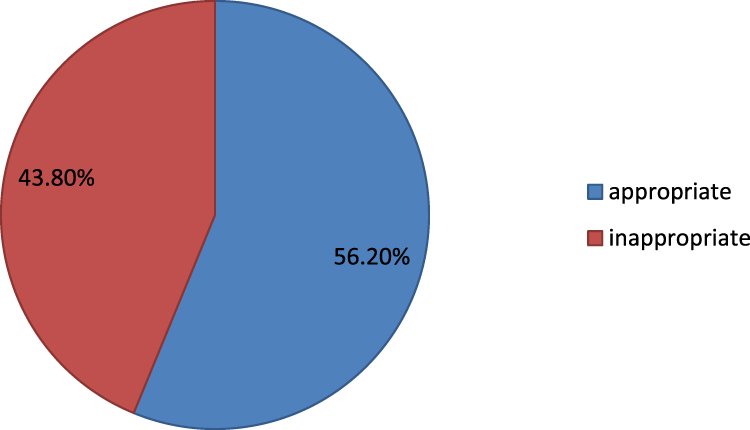 |
Figure 1 Shows the prevalence of health care waste management among public health facilities in Hadiya Zone, Southern Ethiopia (n=411). |
Factors Associated with Health Care Waste Management
The candidate variables identified for multivariable logistic regression on Bivariate analysis were Sex, age, residence, service year, Training in waste management, knowing the presence of waste management rules in the facility, Availability of health care waste management committee, Availability of adequate PPE, and Experience of waste-related injuries. In multivariable logistic regression, those study participants with service years ≧5 years were 1.59 times more likely to handle health care waste appropriately (AOR 95% CI=1.59(1.02–2.48)) than their counterparts. Those study participants who get training on waste management were 1.94 times more likely to handle health care waste appropriately (AOR 95% CI=1.94(1.12–3.22)) than those who did not get training. Those study participants having adequate PPE were 2.14 times more likely to handle health care waste appropriately (AOR 95% CI=2.14(1.35–3.34)) than those who did not have (Table 3).
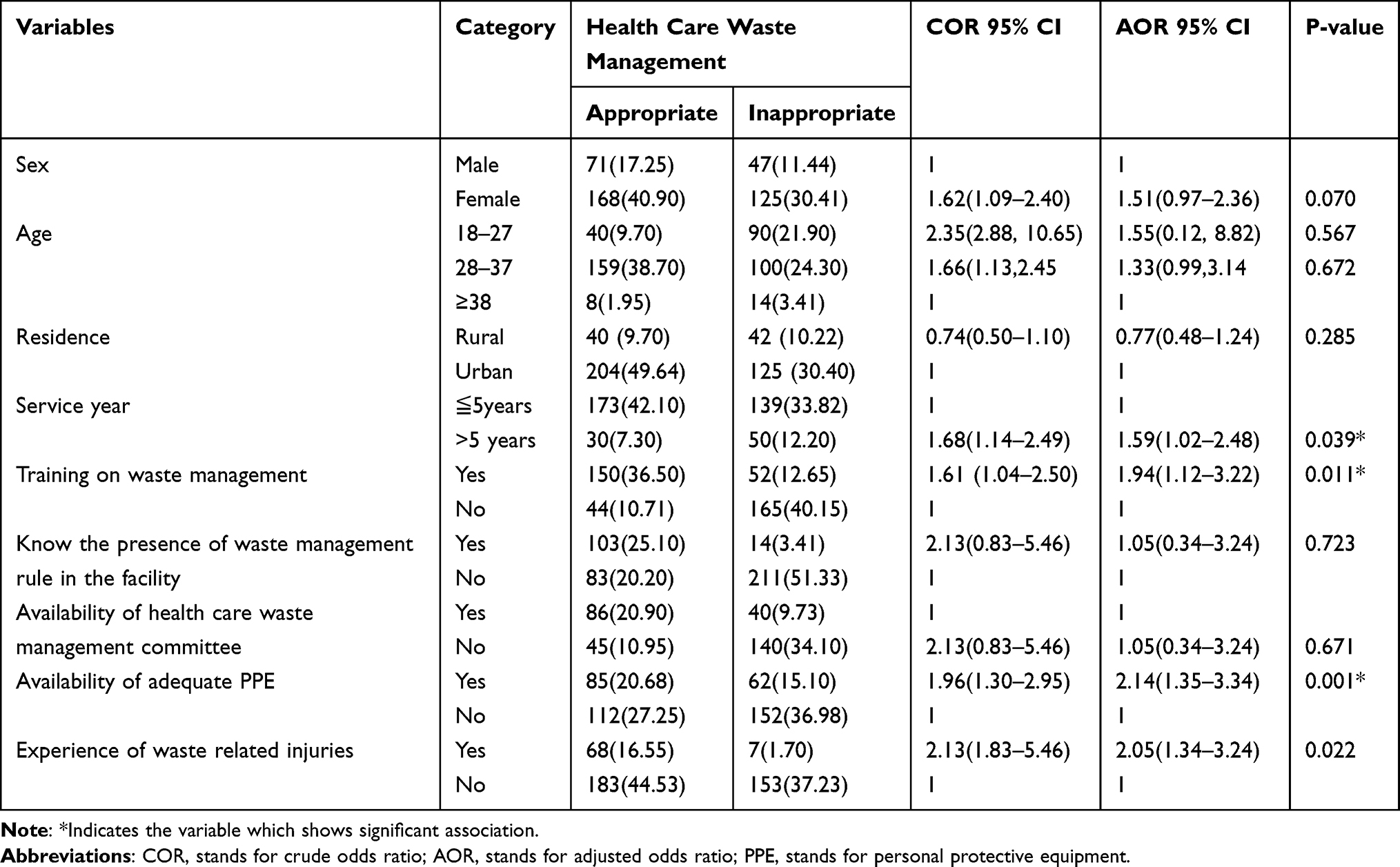 |
Table 3 Bivariate and Multivariate Analysis of Factors Associated with Health Care Waste Management Among Public Health Facilities in Hadiya Zone, Southern Ethiopia, April, 2021 (n=411) |
Discussion
The Hadya Zone’s health-care waste management procedures and associated factors were investigated in this study. The Hadiya zone public health facilities has (56.2%) prevalence of good health-care waste management practices.
This finding was higher than findings in Bangladesh (54%),3 Adama Hospital, Ethiopia, 34.9%,12 and Gondar Town, 31.5%.13 The possible reason for this difference might be the difference in the study period, study area, and sample size used. This study’s finding was lower than previous studies conducted in Nigeria (62%), and Pakistan (66.6%).14 The possible reason for this discrepancy could be the difference in the study setting.
This study has revealed that healthcare workers who had served >5 years had about 1.59 times more likely practice appropriate health care waste management practices compared to those who have served ≤5 years. This could be since those health care workers who stay more in the facilities might get the chance of getting training and learning through practice.
In addition to this those study participants who get training on waste management were 1.61 times more likely to practice appropriate health care waste than their counterparts. This study finding was supported by previously conducted studies in Nepal. The observed significant association could be because those who get training will give more focus than those who were not trained.
The current study identified that those study participants reporting the Availability of adequate personal protective equipment (PPE) were 2.14 times more likely to practice appropriate health care waste than those who report the absence of adequate personal protective equipment. A possible reason for this observed association could be the reality that those who have adequate personal protective equipment did not feel fear experiencing of injury.
This study revealed that those study participants who have experienced waste-related injuries have 2.05 times more likely to practice appropriate health care waste than those who did not have experience of waste-related injuries.
Conclusion and Recommendation
The study revealed that the proportion of appropriate health care waste management was low. A service year, training on waste management, availability of adequate personal protective equipment (PPE), and experience of waste-related injuries were significantly associated factors. The Health care facility management is recommended to provide training and personal protective equipment for health-care professionals.
Abbreviation
AOR, Adjusted Odds Ratio; CI, Confidence Interval; HCW, Health Care Worker; PPE, Personal Protective Equipment; SDG, Sustainable Development Goal; SPSS, Statistical Package for Social Sciences; SNNP, Southern Nation Nationality and People; WHO, World Health Organization.
Data Sharing Statement
The data are available from the corresponding author upon reasonable request.
Ethical Consideration
Permission to carry out the study was sought from the Ethical review committee of Wachemo University with Ref Number 1030/21, and a letter of cooperation was taken from Hadiya Zone health department to concerned woreda health offices and then the authority wrote a letter of cooperation to each health facility. Written informed consent was taken from all the study participants. Besides this, all the information collected from the study subjects was handled confidentially and data was used for the research purpose only. We confirm that our study complies with the declaration of Helsinki.
Acknowledgments
The authors would like to thank the data collectors, supervisors, study participants, and wachemo University for their cooperation and help during the data collection.
Disclosure
The authors declare that they have no conflicts of interest.
References
1. World Health Organization. Management of Solid Health-Care Waste at Primary Health-Care Centres: A Decision-Making Guide. World Health Organization; 2005:9241592745.
2. Tripathi A, Tyagi VK, Vivekanand V, Bose P, Suthar S. Challenges, opportunities and progress in solid waste management during COVID-19 pandemic. Case Stud Chem Environ Eng. 2020;2:100060. doi:10.1016/j.cscee.2020.100060
3. Rahman MM, Bodrud-Doza M, Griffiths MD, Mamun MA. Biomedical waste amid COVID-19: perspectives from Bangladesh. Lancet Glob Health. 2020;8(10):e1262. doi:10.1016/S2214-109X(20)30349-1
4. World Health Organization. Water, Sanitation, hygiene, and waste management for the COVID-19 virus. World Health Organization. 2020.
5. Sinha R, Michelsen JD, Ackura E, Njie L. COVID-19ʹs Impact on the Waste Sector. In: International Finance Corporation, World Bank Group; 2020.
6. Mbuvi C, Kyulu T, Makobu K. Proposed Solutions to address the challenges of medical Waste Management in Health Facilities in Kamukunji Sub-County, Nairobi City County, Kenya. J Med Nurs Public Health. 2022;5:1. doi:10.53819/81018102t6006
7. Zikargae MH. COVID-19 in Ethiopia: assessment of how the Ethiopian government has executed administrative actions and managed risk communications and community engagement. Risk Manag Healthc Policy. 2020;13:2803. doi:10.2147/RMHP.S278234
8. Kassegn A, Endris E. Review on socio-economic impacts of ‘Triple Threats’ of COVID-19, desert locusts, and floods in East Africa: evidence from Ethiopia. Cogent Soc Sci. 2021;7(1):1885122. doi:10.1080/23311886.2021.1885122
9. Belhadi A, Kamble SS, Khan SAR, Touriki FE, Kumar MD. Infectious waste management strategy during COVID-19 pandemic in Africa: an integrated decision-making framework for selecting sustainable technologies. Environ Manage. 2020;66(6):1085–1104. doi:10.1007/s00267-020-01375-5
10. Sarkodie SA, Owusu PA. Impact of COVID-19 pandemic on waste management. Environ Dev Sustain. 2021;23(5):7951–7960. doi:10.1007/s10668-020-00956-y
11. Assemu DM, Tafere TE, Gelaw YM, Bantie GM. Healthcare waste management practice and associated factors among private and public hospitals of Bahir Dar City administration. J Environ Public Health. 2020;2020. doi:10.1155/2020/7837564
12. Hayleeyesus SF, Cherinete W. Healthcare waste generation and management in public healthcare facilities in Adama, Ethiopia. J Health Pollut. 2016;6(10):64–73. doi:10.5696/2156-9614-6-10.64
13. Azage M. Healthcare waste management practices among healthcare workers in healthcare facilities of Gondar town, Northwest Ethiopia. Health Sci J. 2013;7(3):1
14. Badar S. Health care waste management practices in public and private sector hospitals. J Rawalpindi Med Coll. 2014;18(1):145–147.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.