")
Back to Journals » ClinicoEconomics and Outcomes Research » Volume 6
Health care-resource utilization before and after natalizumab initiation in multiple sclerosis patients in the US
Authors Bonafede M, Johnson B, Watson C
Received 11 October 2013
Accepted for publication 13 November 2013
Published 19 December 2013 Volume 2014:6 Pages 11—20
DOI https://doi.org/10.2147/CEOR.S55779
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Machaon M Bonafede,1 Barbara H Johnson,1 Crystal Watson2
1Truven Health Analytics, Cambridge, MA, USA; 2Biogen Idec, Weston, MA, USA
Objectives: To evaluate multiple sclerosis (MS)-related health care-resource utilization and costs prior to and after initiating natalizumab in the US.
Materials and methods: A retrospective administrative claims analysis was conducted using the Truven Health MarketScan Databases to identify adults diagnosed with MS who initiated natalizumab (index date) between January 1, 2007 and December 31, 2010. Patients had ≥24 months of continuous enrollment (12 months before [preperiod] and 12 months after [postperiod] the index date) and remained on natalizumab for the 12-month postperiod. Patients with and without other disease-modifying treatment (DMT) during the preperiod were examined. Patient characteristics, MS-related inpatient stays, and corticosteroid use were compared in the pre- and postperiods using paired statistical tests, where appropriate.
Results: The study comprised 1,458 patients, mean age 45.2 years (standard deviation 10.5), 74.2% female. The majority (70.3%) used a DMT during the preperiod. After initiating natalizumab, there was a significant reduction in the percentage of patients with MS-related inpatient stays (7.6% versus 2.4%, P<0.001), MS-related inpatient costs (median US $12,078 versus US $9,784, P<0.001), and length of stay (7.12 days versus 6.26 days, P=0.005). Both cohorts showed a reduction in the percentage of patients with MS-related inpatient stays and costs with greater reductions for patients without DMTs in the preperiod (–6.2% [P<0.001] and –US $1,496 [P=0.056], respectively) compared to those with a DMT in the preperiod (–4.8% and –US $1,262, respectively, P<0.001 for both). Compared to the preperiod, there were significant reductions in intravenous and oral corticosteroid use for natalizumab initiators (–60.1% and –52.9%, respectively, P<0.001 for both). These utilization reductions correspond to mean corticosteroid cost-per-patient reductions of –US $101 across all natalizumab users (P<0.001).
Conclusion: The initiation of natalizumab was associated with significant decreases in MS-related inpatient stays, and corticosteroid use with corresponding decreases in length of stay and costs among natalizumab users with and without DMTs in the prior year.
Keywords: multiple sclerosis, natalizumab, health care-resource utilization, health care costs
Background
Approximately 400,000 people in the US and 2.5 million people worldwide have multiple sclerosis (MS).1 For most MS patients, initial symptoms of the disease occur between the ages of 20 and 40 years.2 Symptoms that are commonly associated with MS include fatigue, impairment of walking and normal mobility, spasticity (muscle tightness), and problems with balance and coordination. In addition to the problems MS symptoms present for patients in their daily life, MS has been shown to reduce life expectancy by 4–7 years in one study,3 and 10–12 in another.4 The exact causes of MS remain relatively unknown.5 The most common type of MS is the relapsing–remitting type (RRMS), which is characterized by slow, gradual progression of the disease with relapses (attacks, flares, or exacerbations) interspersed with periods of remission. Relapses can result in significant residual deficits, leading to sustained progression of disability.6 There are a number of disease-modifying therapies (DMTs) available that can be used to help achieve the therapeutic goals of slowing the progression of the disease and reducing the frequency, duration, and severity of relapses, and there is a benefit of early diagnosis and DMT use for reducing disability and curtailing the progressive phase of MS.7,8 Natalizumab is an established DMT for relapsing forms of MS, and has been shown to reduce annualized relapse rates by 68%9–81%10 relative to placebo.
Patients with MS who have relapses are treated with corticosteroids and are sometimes admitted to the hospital, contributing to the overall cost of managing the disease.11 A patient’s relapse status remains a significant cost factor,12 and increased costs have been shown to be associated with an increase in disease severity.13–15 For example, O’Brien et al estimated that the average costs for treating a relapse ranged from $243 for mild relapses requiring low-intensity care to $12,870 for severe relapses requiring high-intensity care including hospitalization (2002 US dollars),15 which is equivalent to $353 and $18,686, respectively, in 2012 US dollars. Thus, treatment strategies leading to a reduction in the frequency and severity of relapse (such as the use of DMTs) could have a significant impact on the overall cost of managing MS.13
The objective of this study was to compare MS-related and all-cause inpatient health care-resource utilization, health care costs, corticosteroid utilization, and corticosteroid costs in a real-world setting among adult patients with MS in the US before and after initiating natalizumab. Although natalizumab was originally approved for treatment of MS in the US in 2004, to our knowledge there has been limited research quantifying the impact of natalizumab on health-resource utilization and expenditure. Two posters by Pill and Gilkin used data on 349 natalizumab initiators from 2006 to 2008. They reported reductions in inpatient costs, emergency room costs, and supportive care, defined as corticosteroids, antispastic agents, and benzodiazepines following natalizumab initiation.16,17
Materials and methods
Data sources
Study data came from the Truven Health MarketScan® Commercial Claims and Medicare Supplemental Databases for the period from January 1, 2006 to December 31, 2011. The MarketScan Commercial Claims Database contains the health care experience of privately insured individuals less than 65 years of age covered under a variety of fee-for-service, fully capitated, and partially capitated health plans. The health plans include preferred provider organizations, health maintenance organizations, point-of-service plans, and indemnity plans. The database includes the claims of the primary coverage-holding employee and any covered dependants. The MarketScan Medicare Supplemental and Coordination of Benefits Database contains the health care experience of retirees with Medicare supplemental insurance paid by employers. In both databases, medical claims are linked to retail and mail-order prescription-drug claims and person-level enrollment information, and both the patient and plan portions of claims are represented. The Medicare Supplemental Database also includes the portion of the claim paid by Medicare (represented as “Coordination of Benefits Amount,” or COB), in addition to the portions paid by the employer-sponsored supplemental plan and the patient. During 2006–2011, the commercial database included an average of 33.9 million patients annually who had both medical and prescription coverage, and the Medicare Supplemental Database included an average of 2.9 million such patients annually.
Sample selection
Inclusion in the study required being an adult (patients were required to be at least 18 years of age on their index date) MS patients initiating natalizumab between January 1, 2007 and December 31, 2010. The service date of a patient’s first claim for natalizumab between January 1, 2007 and December 31, 2010 was designated as their index date. Patients were required to have ≥24 months of continuous enrollment in the database (at least 12 months before and 12 months after their index date). The 12-month period ending on the day before the index date was considered the preperiod; the 12-month period starting on the index date was considered the postperiod. Patients were required to have a medical claim with an International Classification of Diseases, ninth revision, clinical modification (ICD-9-CM) diagnosis code for MS (ICD-9-CM code 340) during their 12-month preperiod. Patients who had claim evidence of pregnancy or delivery anytime during their 24-month study period were excluded from the study. Patients were required to have no claims for natalizumab during their 12-month preperiod. Patients were required to remain on natalizumab for the 12-month postperiod, which was verified by the presence of at least one claim for natalizumab during the fourth quarter (months 9 to 12) of their postperiod.
Patient groups
In addition to reporting results for the entire sample of natalizumab initiators, results are reported for two subgroups: natalizumab initiators who used another DMT during the 12-month preperiod (prior DMT use), and natalizumab initiators who had no other DMT (interferon beta-1a, interferon beta-1b, glatiramer acetate, or fingolimod) during the 12-month preperiod (no prior DMT use).
Outcome measures
All outcome measures were evaluated during the 12-month preperiod and again during the 12-month postperiod. The change in each outcome between time periods was also calculated (postperiod value minus preperiod value). Inpatient health care resource-utilization outcomes were evaluated on both all-cause admissions and a subset analysis using MS-related admissions. MS-related inpatient admissions were identified by the presence of a primary diagnosis code for MS (ICD-9-CM code 340) on the claim; MS-related inpatient admissions are a subset of all-cause inpatient admissions, which includes inpatient admissions for any reason or diagnosis. The specific outcome measures of inpatient utilization and cost were mean inpatient expenditure among all patients, number and percentage of patients with an inpatient admission, median inpatient expenditure among patients with at least one admission, and average length of inpatient stay among patients with at least one admission. In addition, mean corticosteroid expenditure among all patients and the number and percentage of patients with a claim for a corticosteroid were measured for three different classifications of corticosteroids: all corticosteroids, intravenous (IV) corticosteroids, and oral corticosteroids.
Demographic and clinical characteristics
The following demographic characteristics were measured at the patient’s index date: age, sex, geographic region, and insurance type. The presence of each of the following comorbid conditions was evaluated during the 12-month preperiod: anxiety, arthritis (rheumatoid arthritis and osteoarthritis), depression, diabetes, gastrointestinal disease and symptoms, high blood pressure, neuropathic pain, nonskin cancer, other chronic pain, skin cancer, thyroid disease, and urinary tract infection.
Statistical analyses
Categorical variables were summarized by frequency and percentage. Continuous variables were reported by mean and standard deviation (SD). Demographic and clinical measures for natalizumab initiators with and without prior DMT use were compared using χ2 tests for categorical variables and two-sample t-tests for continuous variables. Preperiod versus postperiod comparisons were performed using paired tests of significance (paired t-tests for comparisons of means and χ2 tests for comparison of proportions). Median inpatient expenditure is reported for the subset of patients who had at least one inpatient hospitalization; comparisons of median inpatient expenditure were performed using Wilcoxon sign-rank tests which incorporated all patients. All expenditure data were adjusted to 2012 US dollars using the Medical Care Component of the Consumer Price Index. All analyses were performed using Treatment Pathways (Truven Health Analytics, Cambridge, MA, USA) and Stata version 12.1 (StataCorp, College Station, TX, USA).
Results
Patient selection
The final study sample consisted of 1,458 adult MS patients initiating natalizumab. The majority (70.3%, n=1,025) had prior DMT use during the 12-month preindex period, while 30% (n=433) had no prior DMT use. Of the patients with DMT use in the year prior to natalizumab initiation, 90% used one DMT, 10% used two DMTs, and <0.3% used three DMTs in the year prior to natalizumab initiation.
Figure 1 provides detailed information on patient attrition at each step in the sample-selection process. Demographic and clinical characteristics of the final sample on all natalizumab initiators, patients with and without prior DMT use are shown in Table 1. The final sample had a mean age of 45.2 years (SD 10.5), and 74.2% were female. Patients with and without prior DMT use were similar in terms of baseline demographic and clinical characteristics, with one exception: although the mean ages were similar, when age was evaluated categorically, patients with no prior DMT use appeared to be slightly younger than patients with prior DMT use (P=0.036). Overall, 17.1% of study patients had a diagnosis of hypertension, 15.8% had a depression diagnosis, and 14.3% had gastrointestinal disorders or symptoms.
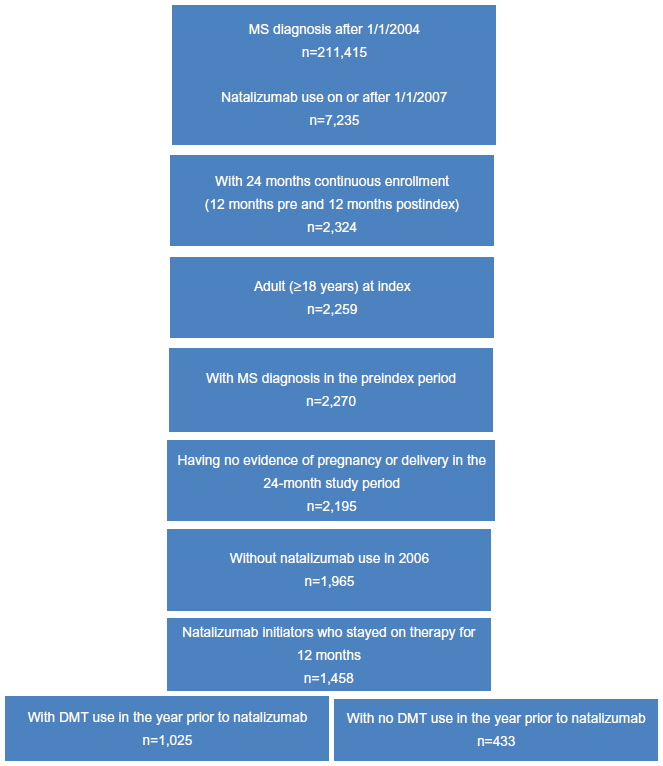 | Figure 1 Sample attrition. |
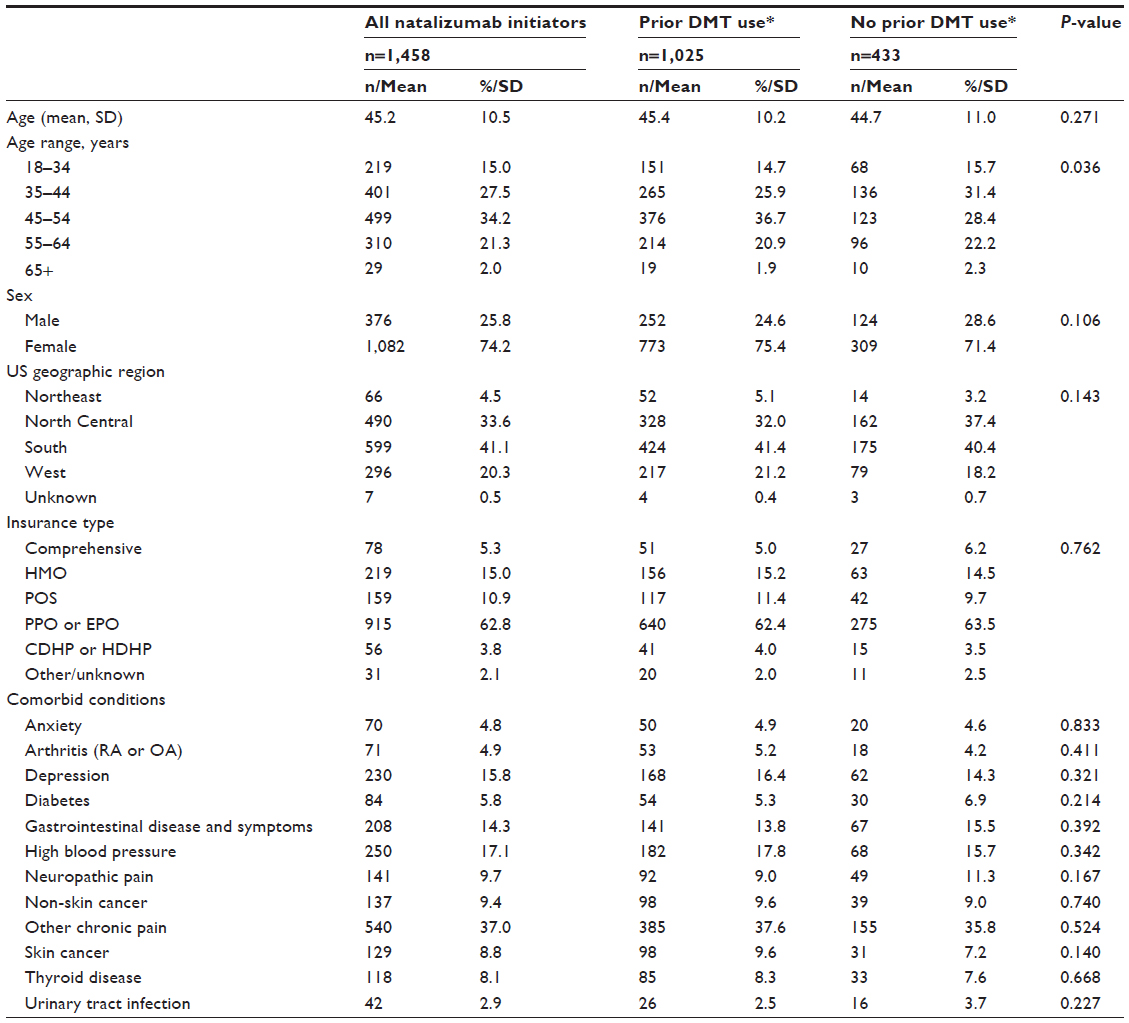 | Table 1 Baseline demographic and clinical characteristics |
Inpatient health care-resource utilization and costs
As shown in Table 2 and Figure 2, among the full sample of all natalizumab initiators, a significant decrease was observed in the proportion of patients with MS-related inpatient admissions (7.6% preperiod versus [vs] 2.4% postperiod, P<0.001). This represents a 68.5% reduction in the number of patients having an MS-related inpatient admission. Among patients with an MS-related inpatient admission, the mean length of hospital stay decreased by 12.1% from the preperiod (7.12 days) to the postperiod (6.26 days) (P=0.005). Likewise, a 28.5% reduction was found in all-cause inpatient admissions (14.2% preperiod vs 10.3% postperiod, P<0.001), with a corresponding 12.0% decrease in mean length of stay among patients with an inpatient admission (9.13 days preperiod vs 8.03 days postperiod, P=0.024).
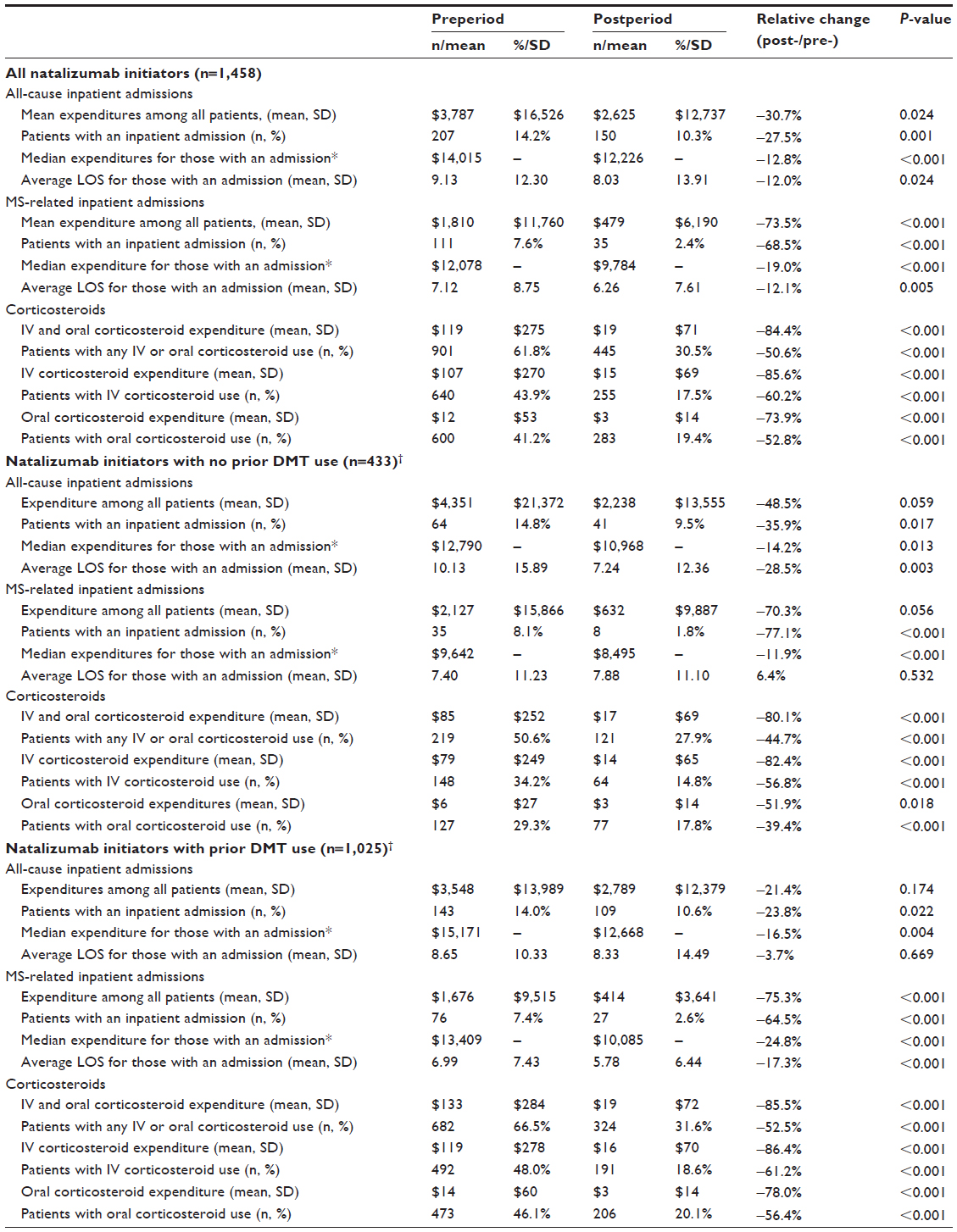 | Table 2 Comparison of pre- versus postperiod inpatient and corticosteroid utilization and expenditures by group (2012 US $) |
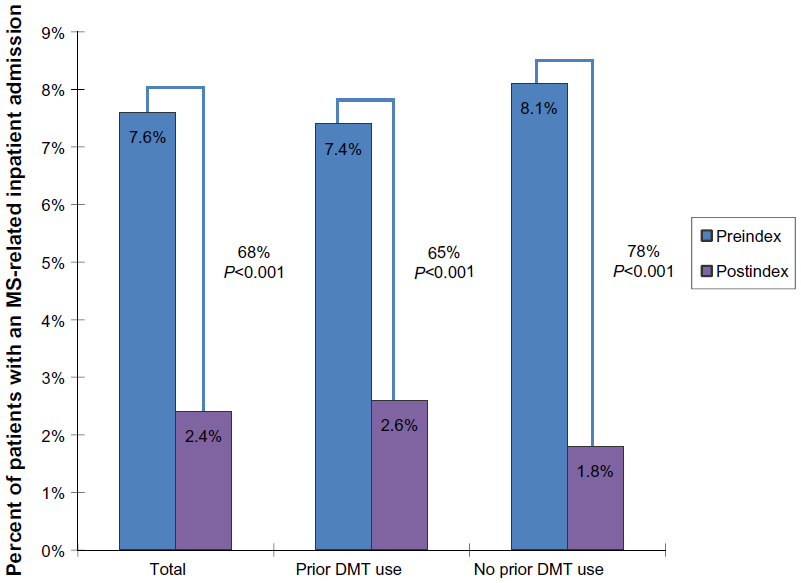 | Figure 2 MS-related inpatient utilization in the years prior to and following natalizumab initiation. |
Average per-patient MS-related inpatient expenditure for all study patients decreased by 73.5% following natalizumab initiation ([US] $1,810 preperiod vs $479 postperiod, P<0.001) (Figure 3). Median MS-related inpatient costs per patient decreased by 19.0% after natalizumab initiation among patients with at least one admission ($12,078 preperiod vs $9,784 postperiod, P<0.001). Overall, there was a 30.7% reduction in average all-cause inpatient expenditure per patient ($3,787 preperiod vs $2,625 postperiod, P=0.024). A 12.8% decrease in the median was observed among the subset of patients with at least one admission ($14,015 preperiod vs $12,226 postperiod, Wilcoxon sign-rank test P<0.001).
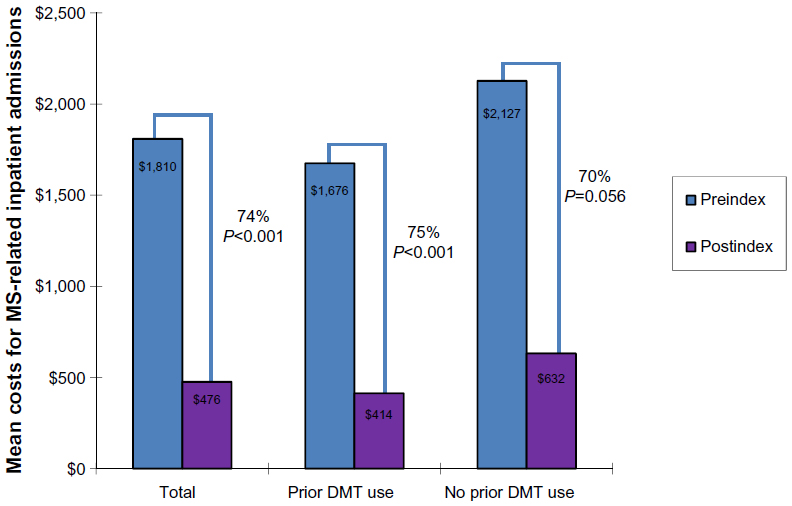 | Figure 3 MS-related inpatient utilization and costs (2012 US $) in the years prior to and following natalizumab initiation. |
Table 2 contains data on pre- and post-natalizumab initiation utilization and expenditure stratified by patients with and without prior DMT use. In general, the results from the overall analysis were present in each of the treatment subgroups. Among patients with prior DMT use, the prevalence of MS-related and all-cause inpatient admissions was significantly lower following natalizumab initiation (7.4% preperiod vs 2.6% postperiod, P<0.001, 14.0% preperiod vs 10.6% postperiod, P=0.022, respectively) (Figure 2); preperiod MS-related inpatient admissions were more common for patients with two DMT therapies in the year prior to natalizumab initiation (11.0%), while the prevalence of preperiod all-cause inpatient stays was similar regardless of number of prior DMT therapies. Likewise, among the prior DMT-use cohort, there was a 17.3% decrease in mean length of stay for MS-related inpatient admissions (7.0 days preperiod vs 5.8 days postperiod, P<0.001); mean length of stay for all-cause inpatient admissions was not statistically significantly different in the year after natalizumab initiation (8.65 days preperiod vs 8.33 days postperiod, P=0.669). Among patients with no prior DMT use, the prevalence of both MS-related inpatient admissions (8.1% preperiod vs 1.8% postperiod, P<0.001) and all-cause inpatient admissions (14.8% preperiod vs 9.5% postperiod, P=0.017) was significantly lower in the year following natalizumab initiation. Among patients with an MS-related inpatient stay, the mean length of stay among patients with no prior DMT use was unchanged in the year following natalizumab initiation (7.4 days preperiod vs 7.9 days postperiod, P=0.543), while there was a significant 28.5% decrease in mean length of stay for all-cause inpatient admissions (10.1 days preperiod vs 7.2 days postperiod, P=0.003).
Among patients with prior DMT use, average all-cause inpatient expenditure decreased 21.4% after natalizumab initiation ($3,548 preperiod vs $2,789 postperiod). While the mean cost was not statistically significant (P=0.174), median all-cause inpatient expenditure was significantly lower after initiation of natalizumab ($15,171 vs $12,668, P=0.004) (Table 2). Although the no prior DMT-use cohort had a smaller sample size with hospitalization (n=64 in the preperiod, n=41 in the postperiod), trends of reducing inpatient expenditure from before to after initiating natalizumab can be seen. The average all-cause inpatient expenditure for patients with no prior DMT use decreased 48.5% after initiating natalizumab ($4,351 preperiod vs $2,238 postperiod, P=0.059). Similarly, there was a 70.3% reduction in average MS-related expenditure in patients with no prior DMT use ($2,127 preperiod vs $632 postperiod, P=0.056) (Figure 3).
Corticosteroid utilization and costs
Overall, the proportion of patients with IV corticosteroid use significantly decreased by 60.2% during the 12 months after natalizumab initiation (43.9% preperiod vs 17.5% postperiod, P<0.001). Similarly, the proportion of patients with oral corticosteroid use significantly decreased by 52.8% after initiation of natalizumab (41.2% preperiod vs 19.4% postperiod, P<0.001). Overall, the proportion of patients using either IV or oral corticosteroids significantly decreased by 50.6% (61.8% preperiod vs 30.5% postperiod, P<0.001). Per-patient costs for corticosteroids were also significantly lower in the 12 months after initiating natalizumab; mean per-patient expenditure for IV corticosteroids decreased by 85.6% (P<0.001), while mean per-patient expenditures for oral corticosteroids decreased by 73.9% (P<0.001). Combined expenditures for both IV and oral corticosteroids decreased by 84.4% after initiating natalizumab, from a per-patient mean of $119 preperiod to $19 postperiod (P<0.001). These corticosteroid utilization and expenditure patterns were also present among patients with and without prior DMT use, where oral and IV corticosteroid utilization and expenditures were statistically significantly lower for both cohorts (Table 2).
Discussion
This study showed significant reductions in corticosteroid use and MS-related inpatient hospitalizations during the 12-month period after patients initiated treatment with natalizumab in a real-world setting. Reductions in these indicators of MS relapse were associated with significant cost savings per patient. Using administrative claims data from commercially insured MS patients, this study demonstrated a 68% reduction in the prevalence of MS-related inpatient stays, a $1,331 reduction in MS-related inpatient costs, and significant reductions in both oral and IV corticosteroid utilization and costs in the year following natalizumab initiation.
In this study, two-thirds of natalizumab initiators used another DMT therapy in the prior year. Reductions in costs and utilization were greater for patients with no prior DMT use than for those with prior DMT use who switched to natalizumab. Further, average DMT costs in the year prior to natalizumab initiation were $17,648 (SD $9,574), suggesting substantial DMT use prior to natalizumab initiation, particularly among patients who used two DMT therapies during the preperiod, where the average cost was $21,713 (SD $13,269, data not shown). By virtue of switching to natalizumab, patients who used another DMT in the prior year were not adequately responding to their prior DMT therapy. Preperiod utilization and costs support this inference as 7.4% of patients with prior DMT use had an MS-related inpatient stay and 66.5% used an IV or oral corticosteroid in the year prior to initiating natalizumab. By comparison, 8.1% of patients without DMT use in the prior year had an MS-related inpatient stay, and 50.6% used a corticosteroid during the prior year.
The findings from this analysis may be bolstered by similar published work showing that switching to natalizumab may be more effective than switching from one platform therapy to another platform therapy. Prosperini et al18 found that patients who switched to natalizumab had better clinical outcomes after 2 years than those who switched to another platform therapy after failing initial platform therapy. Similarly, Castillo-Trivino et al19 reported a significant reduction in MS relapses among patients with breakthrough relapsing MS who switched from another DMT to natalizumab.
Several published cost-effectiveness models have indicated that natalizumab is a cost-effective treatment option relative to fingolimod20–25 and other DMTs.20 Since a key effectiveness measure in DMT clinical trials is the number of MS relapses avoided, several studies have reported that natalizumab is more cost-effective than other DMTs in terms of cost per MS relapse avoided.21–23 An analysis by Chiao and Meyer found that the fewer relapses associated with natalizumab resulted in a lower estimated cost per relapse avoided ($56,594) than the interferon-betas and glatiramer acetate ($87,791 to $103,665).21 An analysis by Bakhshai et al showed similar results,22 while an analysis by O’Day et al reported that natalizumab dominated fingolimod because natalizumab was both more effective at preventing relapses and less expensive.23 A review article by Sharac et al that evaluated 51 studies concluded that cost-effectiveness “findings for natalizumab appear favorable,” while those for other DMTs were inconsistently cost-effective relative to either natalizumab or even placebo.24
Cost-effectiveness findings are important, given the overall burden of MS in the US, where average direct medical costs are $23,434 per year.25 Given that DMTs are costly, channeling patients to the most appropriate therapy earlier in their treatment trajectory remains a priority from both a humanistic and economic standpoint. These current findings suggest that the known beneficial effect of natalizumab on relapse rates is associated with substantial reductions in health care-resource utilization and costs.
Substantial reductions in health care-resource utilization and costs were observed among patients initiating natalizumab with and without prior DMT use. Future research should continue to explore the effectiveness of natalizumab (as well as other DMTs) in real-world settings to inform economic modeling efforts and to aid in medical decision making.
Limitations
There are several limitations to this study. First, this study utilized administrative claims data, which cannot distinguish different types of MS due to limitations in ICD-9-CM diagnosis coding. Studies suggest that patients with secondary progressive MS may have different treatment patterns (and potentially different cost and utilization outcomes) than those with the more common RRMS.26,27 Further, this analysis does not have effectiveness measures and did not utilize a validated effectiveness measure to evaluate the presence of relapse. Similarly, corticosteroid use was evaluated as a dichotomous outcome, and corticosteroid-dosing changes around natalizumab were not evaluated; future research should expand on this, describing corticosteroid dosing over time. This study required a 12-month preindex period to establish new natalizumab use. This time period, however, does not allow for a complete record of a patient’s history with MS, including disease duration, prior treatment, or relapses, which may differ over time.28 Finally, this study utilized administrative claims data from patients with commercial health insurance; these results may not be generalizable to patients with other types of health insurance (eg, Medicaid, Veteran’s Affairs) or the uninsured. Further, these study results may not be generalizable to pregnant women, who were excluded from this analysis.
Conclusion
The results of this study suggest that the benefits of natalizumab in clinical trials have been translated to real-world reduction in MS-related inpatient stays, all-cause inpatient stays, and corticosteroid use. Reductions in these indicators of MS relapse were associated with significant cost savings per patient, both among patients initiating DMT therapy with natalizumab and patients switching to natalizumab from another DMT.
Disclosure
Truven Health Analytics was awarded a research contract by Biogen Idec to conduct this study. Two authors (MMB and BHJ) are employees of Truven Health Analytics. The third author (CW) is an employee and shareholder of Biogen Idec.
References
Pelletier D, Hafler DA. Fingolimod for multiple sclerosis. N Engl J Med. 2012;366:339–347. | |
Confavreux C, Vukusic S. Natural history of multiple sclerosis: a unifying concept. Brain. 2006;129:606–616. | |
Sadovnick AD, Ebers GC, Wilson RW, Paty DW. Life expectancy in patients attending multiple sclerosis clinics. Neurology. 1992;42:991–994. | |
Brønnum-Hansen H, Koch-Henriksen N, Stenager E. Trends in survival and cause of death in Danish patients with multiple sclerosis. Brain. 2004;127:844–850. | |
Compston A, Coles A. Multiple sclerosis. Lancet. 2008;372:1502–1517. | |
Bosca I, Coret F, Valero C, et al. Effect of relapses over early progression of disability in multiple sclerosis patients treated with beta-interferon. Mult Scler. 2008;14:636–639. | |
Elovaara I. Early treatment in multiple sclerosis. J Neurol Sci. 2011;311:S24–S28. | |
McDonald WI, Compston A, Edan G. Recommended diagnostic criteria for multiple sclerosis: guidelines from the International Panel on the Diagnosis of Multiple Sclerosis. Ann Neurol. 2001;50:121–127. | |
Polman CH, O’Connor PW, Havrdova E, et al. A randomized, placebo-controlled trial of natalizumab for relapsing multiple sclerosis. N Engl J Med. 2006;354:899–910. | |
Hutchinson M, Kappos L, Calabresi P, et al. The efficacy of natalizumab in patients with relapsing multiple sclerosis: subgroup analyses of AFFIRM and SENTINEL. J Neurol. 2009;256:405–415. | |
Weinstock-Guttman B, Galetta SL, Giovannoni G, et al. Additional efficacy endpoints from pivotal natalizumab trials in relapsing-remitting MS. J Neurol. 2012;259:898–905. | |
Tyas D, Kerrigan J, Russell N, Nixon R. The distribution of the cost of multiple sclerosis in the UK: how do costs vary by illness severity? Value Health. 2007;10:386–389. | |
Naci H, Fleurence R, Birt J, Duhig A. Economic burden of multiple sclerosis: a systematic review of the literature. Pharmacoeconomics. 2010;28:363–379. | |
Bourdette DN, Prochazka AV, Mitchell W, Licari P, Burks J. Health care costs of veterans with multiple sclerosis: implications for the rehabilitation of MS. VA Multiple Sclerosis Rehabilitation Study Group. Arch Phys Med Rehabil. 1993;74:26–31. | |
O’Brien JA, Ward AJ, Patrick AR, Caro J. Cost of managing an episode of relapse in multiple sclerosis in the United States. BMC Health Serv Res. 2003;3:17. | |
Pill M, Gilkin B. Measuring the impact of natalizumab therapy on health care utilization in a commercially managed multiple sclerosis population. Poster presented at ISPOR 16th Annual International Meeting, Baltimore, MD, May 21–25, 2011. Value Health. 2011;14:A1–A214. | |
Pill M, Gilkin B. Economic trends associated with natalizumab therapy in a commercially managed multiple sclerosis population. Poster presented at ISPOR 16th Annual International Meeting, Baltimore, MD, May 21–25, 2011. Value Health. 2011;14:A1–A214. | |
Prosperini L, Gianni C, Leonardi L, et al. Escalation to natalizumab or switching among immunomodulators in relapsing multiple sclerosis. Mult Scler. 2012;18:64–71. | |
Castillo-Trivino T, Mowry EM, Gajofatto A, et al. Switching multiple sclerosis patients with breakthrough disease to second-line therapy. Plos One. 2011;6:e16664. | |
Gani R, Giovannoni G, Bates D, Kemball B, Hughes S, Kerrigan J. Cost-effectiveness analyses of natalizumab (Tysabri) compared with other disease-modifying therapies for people with highly active relapsing-remitting multiple sclerosis in the UK. Pharmacoeconomics. 2008;26:617–627. | |
Chiao E, Meyer K. Cost effectiveness and budget impact of natalizumab in patients with relapsing multiple sclerosis. Curr Med Res Opin. 2009;25:1445–1454. | |
Bakhshai J, Bleu-Lainé R, Jung M, et al. The cost effectiveness and budget impact of natalizumab for formulary inclusion. J Med Econ. 2010;13:63–69. | |
O’Day K, Meyer K, Miller RM, Agarwal S, Franklin M. Cost-effectiveness of natalizumab versus fingolimod for the treatment of relapsing multiple sclerosis. J Med Econ. 2011;14:617–627. | |
Sharac J, McCrone P, Sabes-Figuera R. Pharmacoeconomic considerations in the treatment of multiple sclerosis. Drugs. 2010;70:1677–1691. | |
Owens GM, Olvey EL, Skrepnek GH, Pill MW. Perspectives for managed care organizations on the burden of multiple sclerosis and the cost-benefits of disease-modifying therapies. J Manag Care Pharm. 2013;19:S41–S53. | |
Rio J, Porcel J, Téllez N, et al. Factors related with treatment adherence to interferon beta and glatiramer acetate therapy in multiple sclerosis. Mult Scler. 2005;11:306–309. | |
O’Rourke KE, Hutchinson M. Stopping beta-interferon therapy in multiple sclerosis: an analysis of stopping patterns. Mult Scler. 2005;11:46–50. | |
Scalfari A, Neuhaus A, Degenhardt A, et al. The natural history of multiple sclerosis, a geographically based study 10: relapses and long-term disability Brain. 2010;133:1914–1929. |
 © 2013 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2013 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.