")
Back to Journals » Risk Management and Healthcare Policy » Volume 15
Health Care Readiness in Management of Preeclampsia/Eclampsia in Ethiopia: Evidence from National Facility-Based Survey
Authors Meazaw MW, Chojenta C , Forder P, Taddele T, Loxton D
Received 11 March 2022
Accepted for publication 5 June 2022
Published 16 June 2022 Volume 2022:15 Pages 1225—1241
DOI https://doi.org/10.2147/RMHP.S366055
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Mecit Can Emre Simsekler
Maereg Wagnaw Meazaw,1,2 Catherine Chojenta,2 Peta Forder,2 Tefera Taddele,3 Deborah Loxton2
1Federal Ministry of Health, Addis Ababa, Ethiopia; 2Centre for Women’s Health Research, School of Medicine and Public Health, College of Health, Medicine and Wellbeing, University of Newcastle, Newcastle, NSW, Australia; 3Health System and Reproductive Health Directorate, The Ethiopian Public Health Institute, Addis Ababa, Ethiopia
Correspondence: Maereg Wagnaw Meazaw, The University of Newcastle, University Drive, Callaghan, NSW, 2308, Australia, Tel +61 402 290 013, Email [email protected]
Background: Early case detection, treatment, and timely referral for better services can significantly reduce the negative outcomes of preeclampsia and eclampsia. However, evidence on health facilities’ readiness to provide such services and the associated challenges is limited in Ethiopia. Therefore, this study aimed to assess the readiness of Ethiopian health care facilities to manage preeclampsia and eclampsia.
Methods: This study used the 2016 Ethiopia national emergency management of obstetrics and newborn care (EmONC) survey. This survey was a national cross-sectional census of health facilities that provided delivery services. Data on facility infrastructure, equipment and supplies were collected through a facility checklist, and interview health provider experiences. Cross tabulation, summarisation and chi square tests by facility type, location, and management authority were conducted.
Results: There were 3804 health facilities included in the survey across all regions of Ethiopia. The majority of facilities (92%) were public/government managed with only 1% of available hospitals located in rural areas. Poor availability of dipsticks for proteinuria tests (55.3%), caesarean sections (7.9%), and ambulance services (18.4%) were reported across health facilities with high variations in terms of facility type, location, and type of managing authority. Diazepam was a widely available anticonvulsant compared with magnesium sulfate (MgSO4), with more available in private for-profit facilities compared with public facilities. Nearly one third of health care providers were not trained to administer MgSO4 intravenously. The result indicated that the chi-square test was statistically significant at P < 0.001.
Conclusions and Recommendations: There were notable gaps in readiness of facilities in detection and management of preeclampsia/eclampsia that increase maternal and perinatal mortality in Ethiopia. Therefore, availability of essential supplies, medications, and referrals are required. In addition, refresher training to healthcare providers on screening, diagnosis and management of preeclampsia/eclampsia and continuous supervision should be provided.
Keywords: preeclampsia, eclampsia, facility readiness, Ethiopia, EmONC
Introduction
Globally, preeclampsia, defined as hypertension with proteinuria during pregnancy after 20 weeks of gestation, complicates 2–8% of pregnancies and contributes to 10–15% of maternal deaths.1 Eclampsia, defined as the occurrence of generalised tonic-clonic seizures in women with preeclampsia, where the seizures are not attributable to other causes (eg, epilepsy),2 is the most serious form of preeclampsia and the cause for most cases, of maternal morbidity and mortality. Preeclampsia has been disproportionately higher in developing countries with an incidence of 2.8% of live births compared with 0.4% of live births in developed countries.3 Preeclampsia/eclampsia were reported as the second leading cause of obstetric-related maternal mortality in Ethiopia.4 According to the 2008 national Emergency Obstetrics and Newborn Care (EmONC) survey, preeclampsia was responsible for 11% of maternal mortality reported from health facilities.5
Women with preeclampsia require detailed antenatal care (ANC), early diagnosis and follow up with appropriate management.6 Without close monitoring and treatment, preeclampsia may progress to eclampsia, putting the health and wellbeing of both mother and baby at risk. The only definitive cure for preeclampsia is delivering the placenta.7 However, the decision for delivery of a newborn depends on gestational age, fetal status, and the severity level of the disease at the time of evaluation.8 The diagnosis can be carried out at the primary health care level; however, timely referral with adequate pre-referral care is mandated if the condition worsens.9 If complications occur, the woman should be admitted and managed in a hospital with advanced care options, such as caesarean section delivery, and access to intensive care units.10
The current Ethiopian health policy recommends that all pregnant women receive at least four ANC visits per pregnancy, which is in accordance with the previous World Health Organization (WHO) recommendation (which was revised in 2016 to eight visits).11 Measuring blood pressure, urinalysis for proteinuria, assessments, and close monitoring of any preeclampsia/eclampsia related danger signs and symptoms are recommended for every antenatal appointment, during delivery, as well as postnatal visits.4 In 2010, there were 23 interventions that WHO recommended for prevention and management of preeclampsia and eclampsia.10 Important interventions and recommendations for prevention and management for preeclampsia and eclampsia are included in this document. Furthermore, the Federal Ministry of Health (FMoH) has also approved management protocols on selected obstetrics and gynaecological topics including the diagnosis and management of preeclampsia and eclampsia in 2010.12 A summary of the WHO recommendations and FMoH protocol to manage preeclampsia/eclampsia is presented in Table 1.
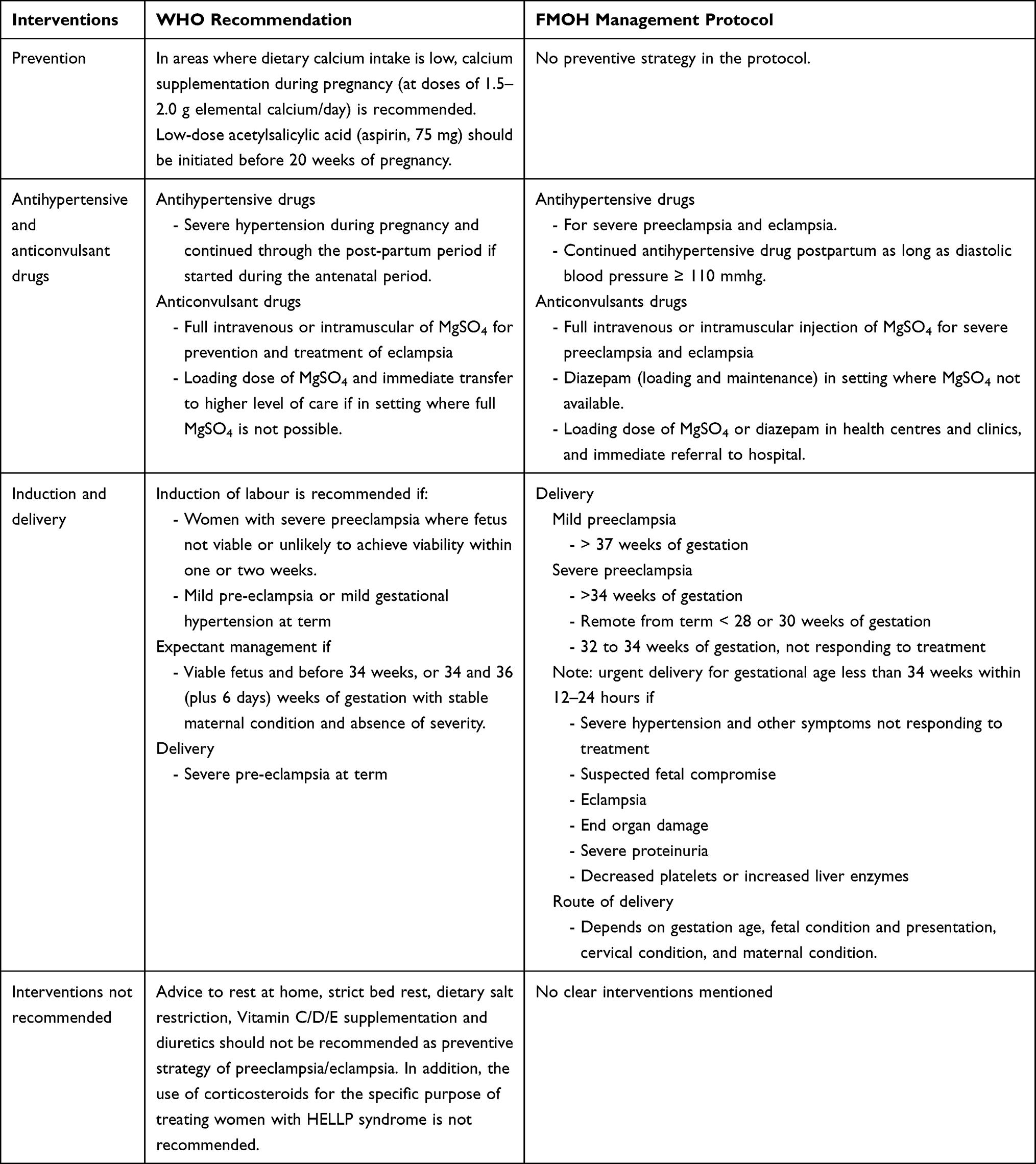 |
Table 1 Summary of the WHO Recommendations and FMOH Management Protocol Guide for Prevention and Management of Preeclampsia/Eclampsia |
Enabling health care providers to identify women with preeclampsia/eclampsia early and initiate timely management has been the focus worldwide in order to reduce maternal deaths and complications related to preeclampsia/eclampsia.13 Health facilities need to be provided with the necessary equipment and supplies for screening, management of preeclampsia/eclampsia including emergency services, and through the referral system. Meanwhile, health care providers need to be trained to screen all pregnant women over 20 weeks of gestation for high blood pressure, proteinuria, and to identify any danger signs or complications related to preeclampsia. If severe preeclampsia or eclampsia is diagnosed, health care providers need to be qualified to administer MgSO4 and facilitate a birth, either by timely referral or delivery as per the condition of the women.14 However, lack of basic equipment and supplies, shortages of health care professionals, limited skills of frontline providers, and a shortage of facilities with advanced care, all pose challenges to prevention and management of preeclampsia/eclampsia, especially in low and middle-income countries.13,15
In the last decade, despite the investment of the Ethiopian government in health infrastructure, gains in maternal health services have fallen short of optimal targets.4 Based on the Ethiopian demographic and health survey (EDHS) 2016, 62% of women had one ANC and 32% had four or more ANC visits compared with 33% and 19% respectively, in the 2011 EDHS report. Similarly, incidences of stillbirth have also increased from 10% in 2011 to 26% in the 2016 EDHS.16 However, Ethiopia is still one of the countries with the highest maternal mortality with 420 deaths per 100,000 live births, with preeclampsia/eclampsia remaining the main cause of death.16 In general, the survival of pregnant women and newborns highly depends on access to health care at the time of the emergency and the quality of service received at the health facility.17 Therefore, prevention, early diagnosis, and timely, appropriate treatment can significantly reduce the associated mortality and morbidity of patients with preeclampsia/eclampsia.
Preeclampsia and eclampsia management requires case detection and screening; availability of essential commodities such as MgSO4 and antihypertensive drugs; trained health care providers and having transportation available for timely referrals to appropriately equipped and staffed health facilities. Of the few studies on management of preeclampsia and eclampsia in Ethiopia, most analysed aspects of individual patient care,18 while the others examined specific geographical regions or health facilities.19,20 No studies have been conducted to examine the readiness of health facilities to prevent and treat preeclampsia and eclampsia in Ethiopia. Therefore, the aim of this study was to assess the readiness of health facilities in terms of essential equipment, supplies, medications, and healthcare provider’s readiness to diagnose and manage preeclampsia/eclampsia.
Methods
Study Setting and Design
The 2016 EmONC assessment, conducted between May and December, was a national cross-sectional census of public/government and private for profit/not-for-profit health facilities that provide delivery services. The 2016 EmONC was the second survey, the first being in 2008. The EmONC survey collected various data on maternal and neonatal health indicators from health facility's logbooks, registers, and interviews with health care providers.
Ethiopia follows a three-tiered health system that includes primary level (primary hospitals, health centres, and health posts), secondary level (general hospitals) and tertiary level (specialised hospitals) facilities. Primary level facilities are widely available in the country, from which most women receive pregnancy-related services. Health centres are typically the most readily available primary level facility and are usually staffed by health officers, nurses, and midwives. There are general physicians/general practitioners (GPs) in some health centres especially in urban areas, but not all health centres have assigned GPs. Health posts usually have two healthcare extension workers who operate under the supervision from catchment health centres. The main roles of healthcare extension workers working at health posts is to provide ANC in their cluster, identify high-risk pregnancies and refer the women to nearby health centres. There are no delivery/birth services at health post facilities. Primary hospitals provide emergency surgical services, including caesarean sections, and provide blood transfusion services as well as acting as a referral centre for health centres under its catchment area.4
The primary, referral, and specialised hospitals, which provide advanced services for maternal and newborn care and where most women referred for preeclampsia/eclampsia would receive advanced care and monitoring. MgSO4 can be administered at all health care levels, with the exception of health post. Surgical delivery and intensive care unit services are provided in all levels of hospital care settings only.
Data Collection
The Ethiopia Public Health Institute (EPHI) conducted the EmONC assessments in collaboration with the Averting Maternal Death and Disability Program (AMDD). Fourteen facility-based modules of data collection instruments were used in addition to modules for Woreda, zone, regional, and national levels. The data collection instruments were pretested in three rounds in different health facilities before fieldwork. The EPHI developed an electronic data collection template using CSPro 6.1, and various levels of quality assurance were used during fieldwork, data entry, and analysis.21
Facility Selection Criteria
Health facilities were eligible for inclusion where they met the following three criteria: (a) facility classified as a health centre or above; (b) facility reported providing birthing services in the last 12 months, and (c) facility considered as functional at the time of data collection. According to the Food, Medicine and Health Care Administration and Control Authority of Ethiopia (FMHACA), all health facilities (both public and private) health centres above can potentially provide services to birthing mothers, provide vaginal delivery services, and may treat women with preeclampsia/eclampsia.
Based on information from the FMHACA, Regional Health Bureaus, the Central Statistical Agency (CSA) and findings of the 2014 Ethiopia Service Provision Availability plus (SPA+) census,22 a master facility list was created. Based on the eligibility criteria, 11 health facilities were not accessible due to political and civil unrest and at an additional two facilities, staff refused to allow the data collection team to administer the questionnaires. Finally, 3804 health facilities, in all regional and city administrations in the country, were included in this survey (see Table S1).
Study Variable Selection
This study used the recommended management guidelines for women with preeclampsia and eclampsia (as provided by the Ethiopian Government12 and WHO10) to compare health facilities with respect to their preparedness for management of preeclampsia/eclampsia. In this study, we obtained information about essential drugs, equipment and supplies from different modules of the 2016 EmONC survey database to assess the readiness of the health facilities, specifically in the diagnosis and management of preeclampsia/eclampsia. In addition, the availability of equipment and supplies for screening and diagnosis of preeclampsia/eclampsia and fetal assessment such as blood pressure cuff and stethoscope dipstick for proteinuria tests were assessed. In addition, readiness of health facilities for providing emergency services and management of preeclampsia/eclampsia were assessed through the availability of an intravenous set, caesarean section delivery, intensive care units, ambulance services, and preeclampsia/eclampsia management protocols/guidelines. The recommended drugs for the prevention of preeclampsia (low dose calcium supplementation and Aspirin), antihypertensive and anticonvulsant medications were assessed within the 12 months and three months prior to data collection. The information was collected through interviews of the health facility directors, head of pharmacy, employees from the maternal and neonatal care unit and the laboratory unit.
Furthermore, regarding health professional experience perspectives, one health provider per facility was selected for interview on their experience of maternal and newborn care in general, including their experience of management in relation to preeclampsia/eclampsia. The criteria for selection of health provider were based on those who had delivered the largest number of babies in the past month at the time of data collection, and their availability to be interviewed at the time of the visit.
Definitions
The following definitions are according to the national EmONC survey operational definitions:
Preeclampsia: Systolic 140 mm Hg or higher and diastolic blood pressure of 90 mm Hg or higher and proteinuria of 2+ after 20 weeks of pregnancy with various signs and symptoms, including headache, hyperreflexia, blurred vision, oliguria, epigastric pain, and pulmonary edema. Eclampsia defined as occurrence of generalised seizures in women with pre-eclampsia, provided that the tonic–clonic seizures are not attributable to other causes (eg epilepsy).
Managing Authority: Health facility management body that is: public/government managed by the regional/federal government budget and administration; private for profit managed by a legally registered private owner; and private not-for-profit managed by a Non-Government Organisation (NGO), mission, or faith-based organisation. The managing authority variable categorized into three as “public/government managed” which was coded as “1”, “ private for profit” which was coded as “2” and “ private for not profit” which was coded as “3”.
Health facility EmONC service status: The health facility designated into two as Basic and Comprehensive EmONC facility. The facility designated as Basic EmONC (BEmONC) facility if able to provide seven obstetric services, known as ‘signal functions’, which include: (i) administration of parenteral antibiotics, (ii) administration of parenteral anticonvulsants, (iii) administration of parenteral oxytocin; (iv) manual removal of retained products; (v) manual removal of the placenta; (vi) assisted vaginal delivery; and (vii) neonatal resuscitation with bag and mask. Whereas, Comprehensive EmONC (CEmONC) if the facility provide surgical delivery (caesarean section) and blood transfusions in addition to the seven BEmONC signal functions. However, in this survey close to 1% of health centres/clinics designated as BEmONC facility provide caesarean section services.
EmONC facility functional status: The status of a health facility providing full services as per the designation basic or Comprehensive EmONC criteria. If the health facility missed at least one signal function, it categorised as partially functional. The functional status variable categorized into three as “CEmONC” which was coded as “1”, “ BEmONC” which was coded as “2” and “ partial”: which was coded as “3”.
Intravenous set: Availability of IV stands, fluid giving sets (catheter), IV cannulae, and any fluids such as normal saline, or ringer lactate. These variables were collected separately and aggregated as IV set for analysis.
MgSO4 dosage: The loading dose of MgSO4 given as 4 gm MgSO4 as 20% solution IV over 5 minutes and 10 gm MgSO4 as 50% solution IM divided into 5 gm (10 mL) injected into each buttock (add 2mL lidocaine 1% solution to syringe prior to administration). This continues for 24 hours after last convulsion or delivery, whichever occurs later. Whereas, maintenance dose of MgSO4 given as 5 gm (10 mL) magnesium sulphate with 1 mL of 2% lignocaine deep IM in alternate buttock every 4 hours. Continue for 24 hours after last convulsion or delivery, whichever occurs later.
Distance of facilities from surgery service: The estimated distance of a health facility that does not provide surgical services including caesarean section delivery from the nearest facilities that provide such services. The health providers were interviewed to estimate the distance of health facilities that provide surgical service distance in kilometres (km). For this study, the distance categorised as “less than 25 km” coded as “3”, “between 25–50 km” coded as “2”, “greater than 50 km” coded as “1” and “unknown” coded as “0”.
Data Analysis
Cross tabulation and summary of the findings of variables by type of health facility health centre/hospital, location (urban or rural), and management authority of the health facility (public/government, private for profit and private for non-profit) was conducted. Moreover, the management was compared with the national standards and WHO recommendations to evaluate compliance in the management and service provision to women with preeclampsia/eclampsia. A chi-square test was used to test for differences in health facility’s type, location, and managing authority in terms of facility readiness to screen and manage preeclampsia/eclampsia.
Ethical Review
The ethical review boards of Ethiopia Public Health Institute (EPHI) approved the 2016 national EmONC survey (approval number of SERO-67-6-2016; version 001) prior to the survey. Further, ethical approval was also received from the EPHI to do further analysis from their review (approval number of EPH-IRB-193-2019) on September 14, 2019. In addition, the University of Newcastle’s Human Research Ethics Committee granted approval to conduct this study (approval number: H-2019-0229) on August 27, 2019. Study was carried out in accordance with ethical guidelines of EPHI and University of Newcastle. Informed consent was obtained from participants.
Results
General Characteristics of Surveyed Health Facilities and Infrastructure
The 2016 EmONC survey included 3804 health care facilities across Ethiopia (Table 2). The majority of these facilities were health centres/clinics (92%) and were public/government managed (96%). Nearly two-thirds of the facilities (61%) were located in rural areas, with around 80% of the health facilities located in the three most populous regions of the country: Oromia (37%), Amhara (23%) and SNNPR (20%). Overall, two-thirds (65.5%) of the health centres were found in rural areas of the country while 92.7% of the hospitals/MCH speciality centres were in urban settings. Alternatively, 100% of private for-profit and 57.6% of private not-for-profit facilities were located in urban areas. Close to two-thirds (62.3%) of government-managed health facilities were located in rural areas. In regards to the location, 19.6% of health facilities located in urban areas were hospitals/MCH speciality centres, whereas only 1% of rural health facilities were hospitals/MCH speciality centres. Of the total government managed health facilities, only 6% of them were hospitals/MCH speciality centres compared with 73% of private for-profit and 32% of private not-for-profit (see Table 2).
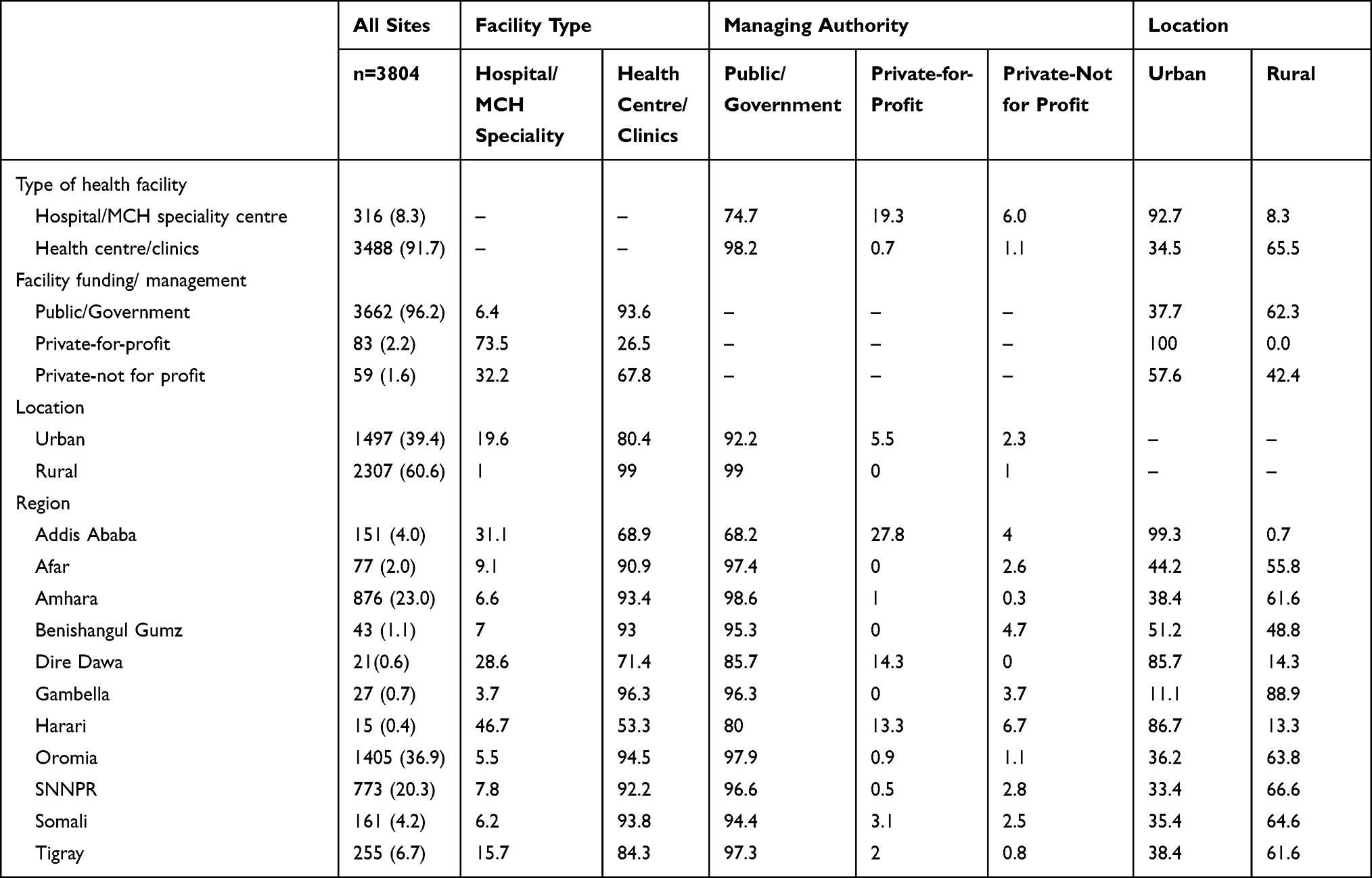 |
Table 2 The Background Characteristics of Health Facilities by Region, Facility Type, Managing Authority, Location in the 2016 National EmONC Survey, Ethiopia |
Of all surveyed health facilities, 2980 (78%) of them were identified as a government-designated EmONC facility. Furthermore, 83% of hospitals/MCH speciality centres and 78% of the health centres were designated as an EmONC facility. Of the total EmONC facilities, only 9% had comprehensive obstetric and neonatal services (eg Comprehensive EmONC facility). The majority of hospitals (87%) were designated Comprehensive EmONC facilities and most of them were managed by private for-profit health facilities (80%). However, only 7.9% of health facilities provided caesarean sections, with less than 1% located in rural areas. More than three fourths of private for-profit health facilities provided caesarean sections. Only one in ten health facility had a separate room for pregnant women with complications. One third of health facilities were greater than 50 km away from health facilities with surgical services that include caesarean sections (see Table 3).
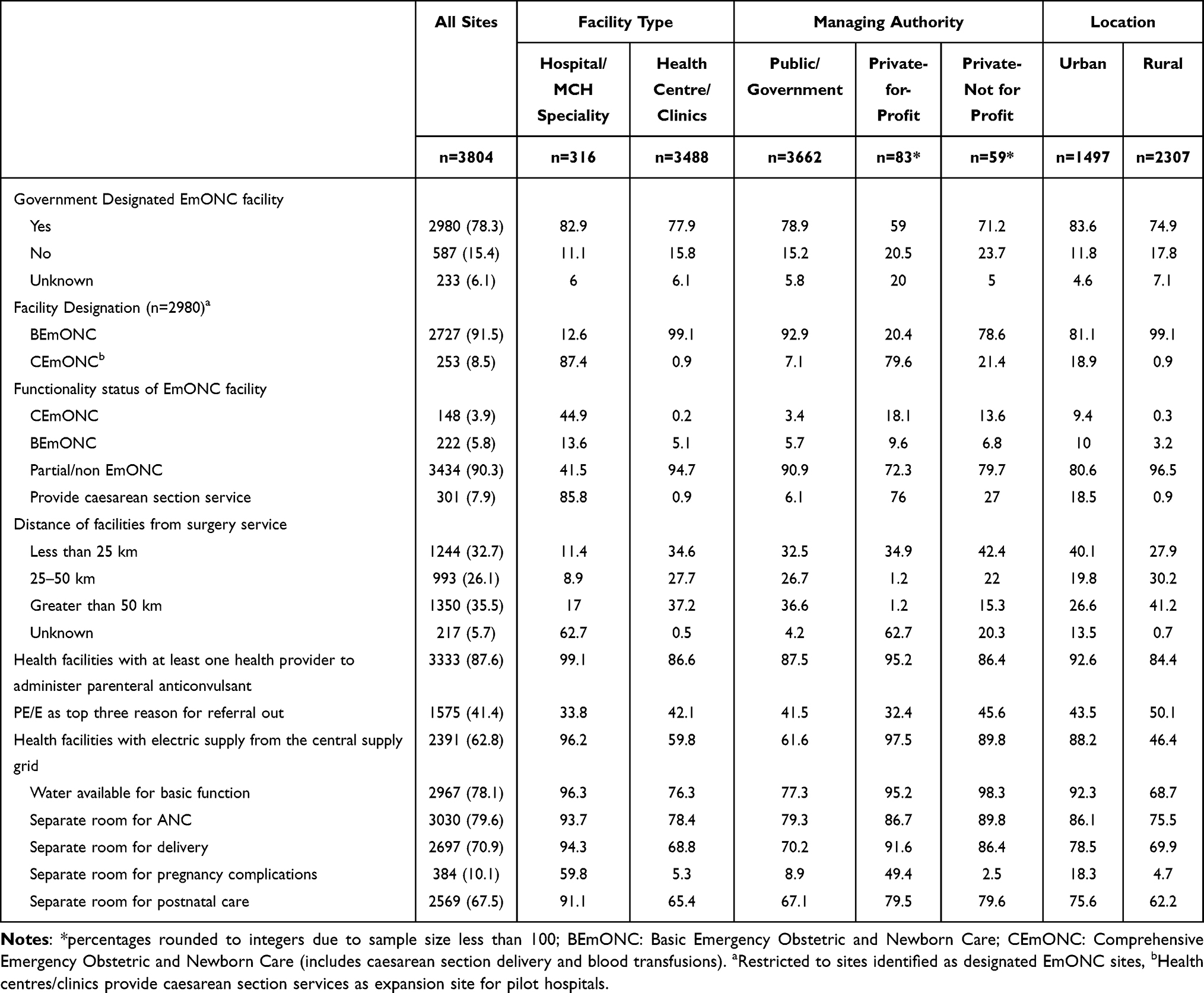 |
Table 3 Infrastructure and Service Delivery Attributes of 3804 Health Facilities by Region, Facility Type, Managing Authority, Location in the 2016 EmONC Survey, Ethiopia |
Readiness of the Health Facilities
Availability of Essential Services, Equipment and Supplies for Diagnosis and Treatment of Preeclampsia/Eclampsia
The majority of health facilities were equipped to provide focused ANC (at least four visits) (99%) and postnatal care services (97%). Basic screening and management equipment for preeclampsia/eclampsia is expected to be available across all health care facilities. Unfortunately, this was not observed for almost all health facilities. For instance, blood pressure cuffs were absent in 6% of the health facilities. Whereas dipsticks for proteinuria tests were not available in 45% of facilities, and more than 50% of rural health facilities do not have this test. Standard IV sets and stethoscopes (adult and fetal), were found to be missing to varying degrees. Nationally, only one in five health facilities had ambulances. Compared to health centres and public/governmental managed health facilities, hospitals and private for-profit health facilities had better access to ambulance services. Management protocols for selected obstetric topics were available in about half of the health facilities (52%) (see Table 4).
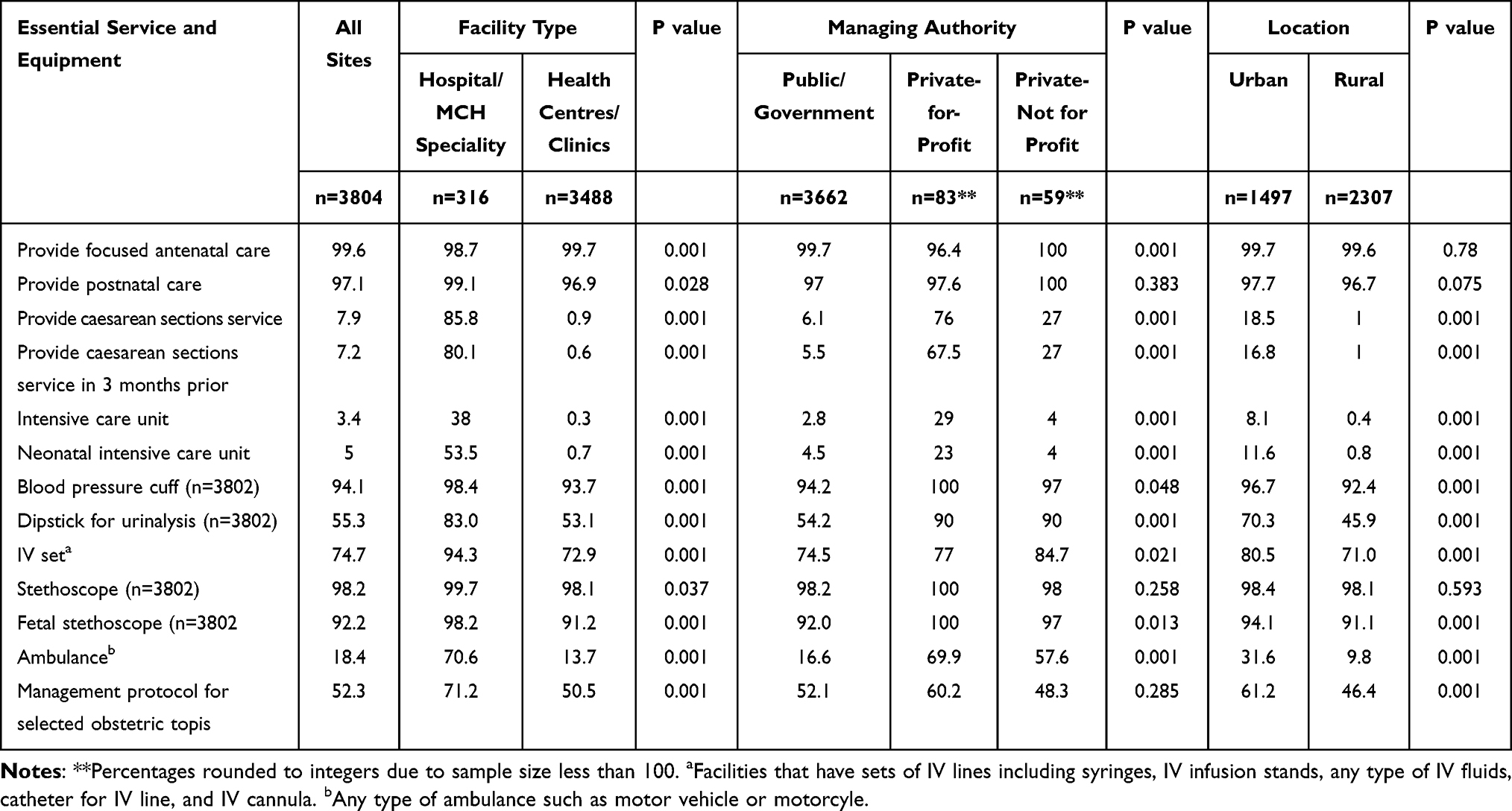 |
Table 4 Availability of Essential Services, Equipment, and Supplies for Diagnosis and Treatment of Preeclampsia/Eclampsia in the 2016 EmONC Survey, Ethiopia |
Essential Drugs for the Treatment and Prevention of Complications in Women with Preeclampsia/Eclampsia
Eighty-six percent of health facilities administered at least one or more parenteral anticonvulsants. In regards to the type of anticonvulsants, diazepam was by far the most commonly available anticonvulsant drug (78.6%), whereas MgSO4 (injection) in 50% concentration and other than 50% concentration was available in 55.4% and 10.1% of health facilities. The majority of health facilities (83.5%) provide MgSO4 to the mothers at no cost. Antihypertensive drugs were available in 92.4% of the health facilities. Antihypertensive drugs such as Methyldopa (80.7%), Nifedipine (66.1%), and Hydralazine (65.4%) were widely available. Conversely, only a quarter of health facilities had calcium gluconate for treatment of MgSO4 toxicity (24.4%), with more private health facilities (60.1%) having this drug compared with public/government health facilities (24.4%). These essential drugs were more available in hospitals and urban area health facilities compared with health centres and rural health facilities. There was a significant difference by the type of facility, managing authority, and whether the facility was urban or rural (P < 0.05) for most essential drugs (see Table 5).
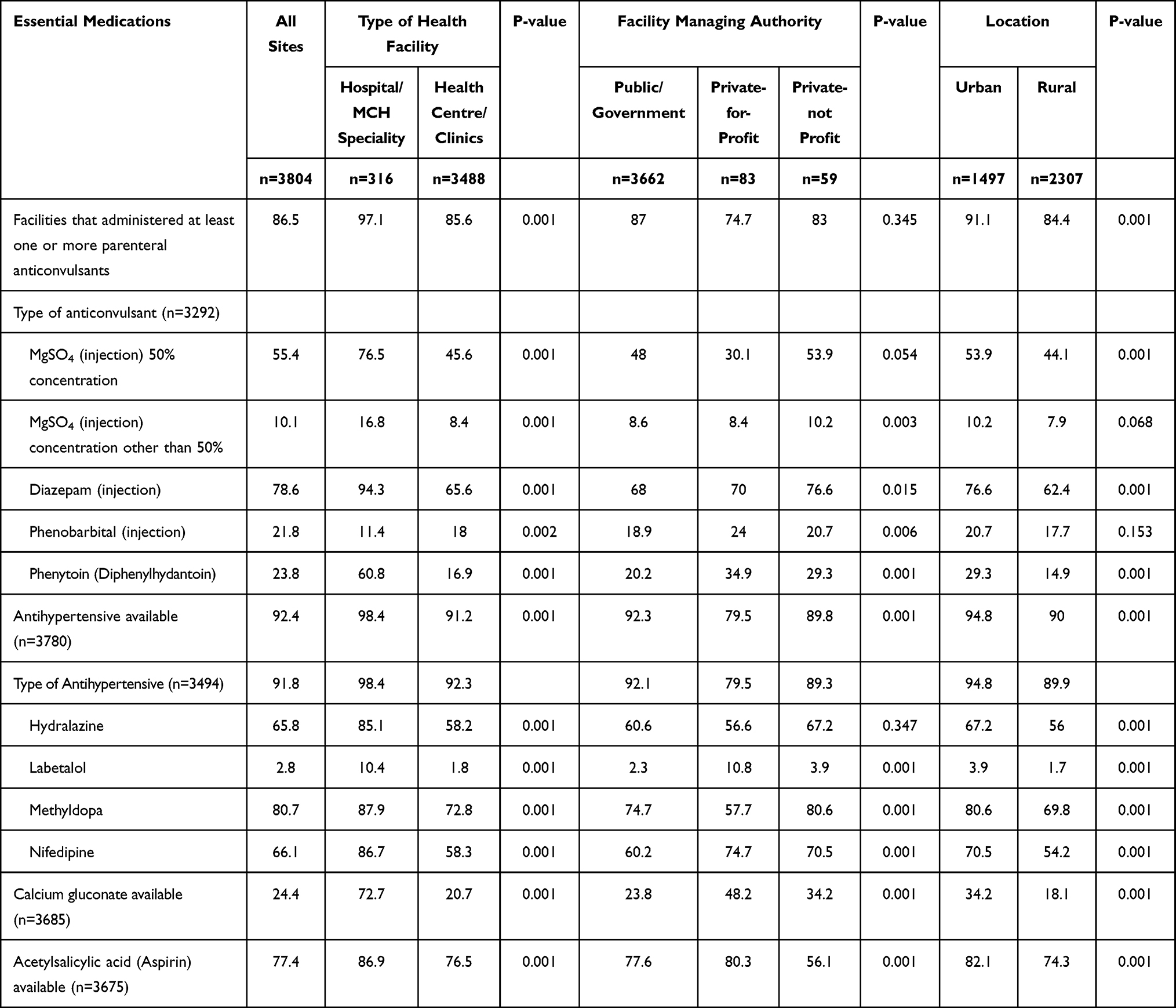 |
Table 5 The Availability of Essential Medication for Management of Preeclampsia/Eclampsia by Region, Facility Type, Managing Authority, Location in the 2016 National EmONC Survey, Ethiopia |
Availability of Anticonvulsants for Treatment of Preeclampsia/Eclampsia Three Months Preceding the Survey
Within the three months prior to data collection, only a quarter 1002 (26.3%) of health facilities had administered parenteral anticonvulsants and of those facilities 80% were hospitals/MCH specialised centres. Only one in four health facilities administered anticonvulsants in the past three months with only 20% of health centres administering these drugs. Despite more than half of health facilities reporting being out of stock of MgSO4 in the three months prior to the survey, the majority of health facilities administered MgSO4 only (54.9%), followed by diazepam only (29.3%), and both MgSO4 and diazepam (15.3%) were used as a drug of choice. Diazepam only was by far the most commonly administered drug in health centres/clinics compared with hospitals. The most frequently reported reason for not administering anticonvulsants was that there was no indication to administer the drug and lack of supplies/equipment at health facilities (see Table 6).
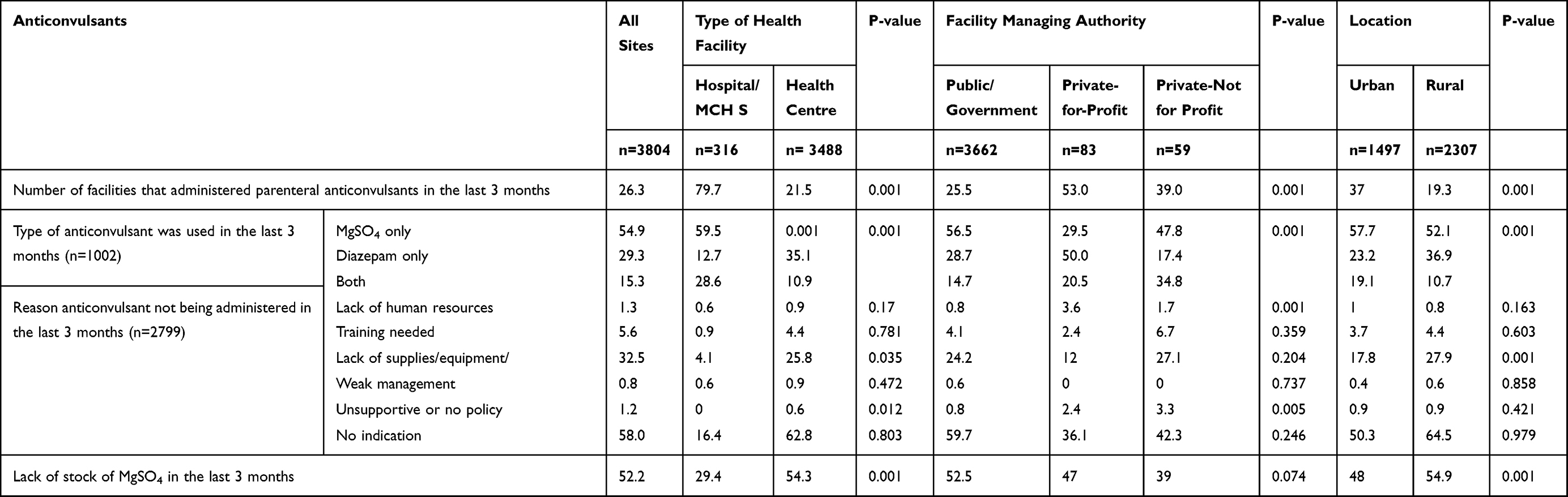 |
Table 6 Availability of Anticonvulsants for Management of Preeclampsia/Eclampsia by Region, Facility Type, Managing Authority, Location in the 2016 National EmONC Survey, Ethiopia |
Health Care Provider Training and Experience for Treatment of Preeclampsia/Eclampsia
In this study, health care providers who attended the most deliveries during the data collection time were interviewed for performance-related information with a focus on ANC and administering anticonvulsants. Of the total health care providers interviewed three-fourths mentioned that they focus on ANC, while 93% of them reported they provided focused ANC services. Nationally, close to 70% of health care providers reported that they received training on administering anticonvulsants; however, only 23% of them administered anticonvulsants. Only one in five health care providers in health centres and rural health facilities administered anticonvulsants in the three months prior to the survey. In comparison to midwives and health officers, a higher proportion of nurses did not administer anticonvulsants. While close to one-third of health care providers either never received any on-the-job training in maternal or newborn health, or received such training a year or more ago.
We analysed the health provider’s knowledge about when the women should receive a loading dose of MgSO4 and referral indication. About 5% of health care providers administered this drug when authorized by their superiors, however, this response doubled in hospitals (12.7%) and private for-profit (12%) health facilities compared with other facilities. More than two-thirds of providers responded that pregnant women with signs of severe preeclampsia (74.8%) and eclampsia (63.5%) are an indication for administering loading doses of MgSO4. Additionally, 83% of health care providers mentioned preeclampsia or eclampsia as a reason for referral or admission to hospitals. When we further analysed the knowledge of health care providers by type, location and managing authorities, the results were broadly similar (see Table 7).
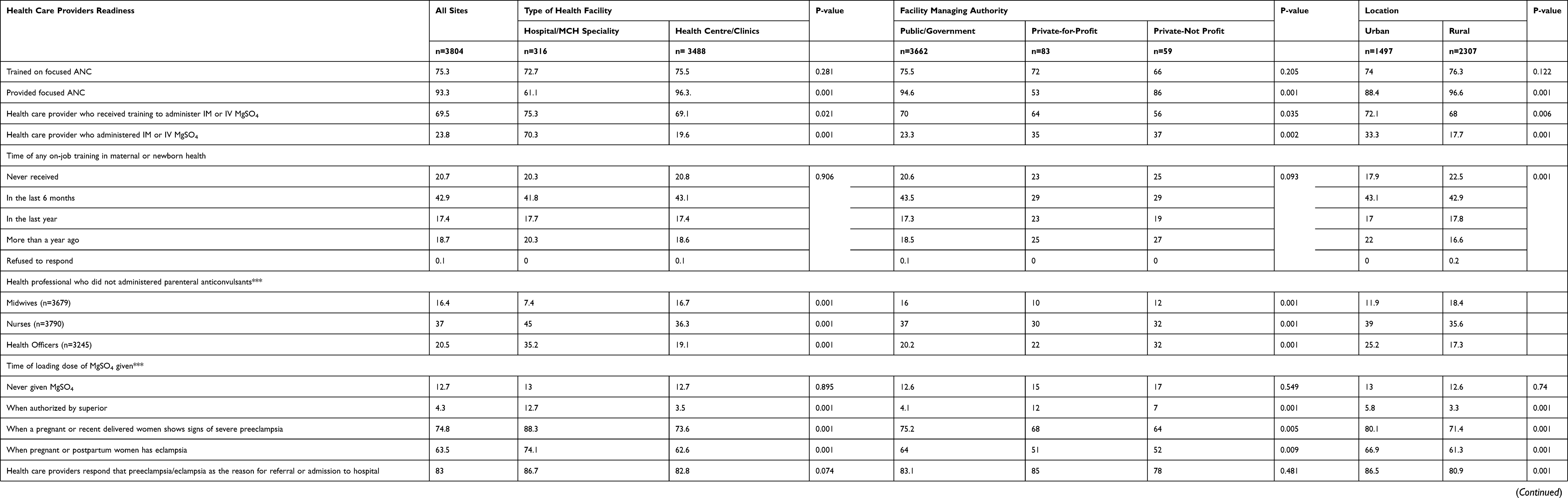 |
Table 7 The Health Care Providers’ Readiness in Management of Preeclampsia/Eclampsia Three Months Preceding the Survey in the 2016 National EmONC Survey, Ethiopia |
Discussion
This study analysed the 2016 EmONC survey data. Compared with the 2008 EmONC survey, the number of health facilities included in this survey increased five-fold from 749 health facilities (112 hospital and 639 health centres) to 3804 health facilities (316 hospitals and 3488 health centres) that provided delivery service. This is likely due to the high number of government health facilities having been built in Ethiopia since 2004.23 This construction program significantly improved key elements of maternity care such as facilities for delivery including caesarean section delivery, ANC, postnatal care, and child health.4 However, there are several barriers to equipping these health facilities with human resources, essential equipment and supplies, specific to providing services for women’s health in general and especially for women with preeclampsia and eclampsia.4 In this study, we analysed the availability of services for the diagnosis and treatment of preeclampsia/eclampsia in terms of health facility readiness such as providing basic equipment, supplies and human resource requirements as per the recommendations for the management of preeclampsia and eclampsia.
This study revealed that there is a wide discrepancy in availability of hospitals between urban and rural areas, with more than 85% of the population living in rural areas.16 However, less than 10% of available hospitals were located in rural areas for a population of more than 90 million, rather health centres were the most available type of health facility in rural areas to provide maternity services. This variation was especially high in terms of CEmONC facilities where less than 1% of them were located in rural areas. This might pose a question for the services provided for those women living in rural settings from the outset as they do not have access to appropriate services. Evidence shows women with preeclampsia/eclampsia are expected to receive advanced care and delivery services such as caesarean delivery and intensive care in a hospital level facility as recommended by the FMoH management of selected obstetrics protocol12 as well as WHO recommendations.10 The following of the protocol may result in a high number of referrals to hospitals in urban areas and this might compromise the quality of service for managing women with preeclampsia/eclampsia.24 Although there is a high government commitment in the expansion of pre-hospital ambulance services,25 we found that there is poor availability of ambulance services and this is even worse in rural areas and government managed health facilities, unlike private for-profit and non-profit health facilities. Moreover, Ethiopia topographically is mountainous and the use of traditional transportation means it is common for women residing in rural areas, to experience a greater delay accessingservices within the limited access of an ambulance. This may result in a delay in access to advanced care services for women with preeclamspsia/eclampsia, who may also spend more time in transportation. This delay may worsen the pregnancy outcome, and contribute to maternal and perinatal mortality.26,27
In this study, we found that the majority of health facilities had the basic equipment available for screening and diagnosis of preeclampsia and eclampsia. However, dipstick tests for proteinuria, one of the most important tools for diagnosis of preeclampsia/eclampsia and its severity level, were missing among half of the health facilities nationally, and even more in health centres and rural health facilities. This testing rate was lower than with other study findings from DR Congo (67.2%).28 This is in fact in conflict with the national as well as WHO diagnostic criteria of preeclampsia or eclampsia since the proteinuria level is an important element of diagnosis as well as in the measurement of the severity of the disease. The lower testing rate might be due to non-uniform service provisions toward screening and management of preeclampsia/eclampsia, since more than half of health facilities do not adhere to the national management protocol including a lack of on-the-job training, or lack of supplies and equipment as revealed in this study. These reasons for low testing rates were consistent with other studies from low- and middle-income countries.13,29 Therefore, this poses a question on the possibility of a significant gap in the management implementation towards preeclampsia/eclampsia. In addition, lack of supplies might increase misdiagnosis and misclassification of the severity of preeclampsia/eclampsia.
Preeclampsia can occur in the second half of pregnancy, during labour, or in the postpartum period.2 Hence, early detection of complications and other potential problems that can affect the outcomes of pregnancy is the main goal of focused ANC and has a big role in the prevention of complications and death related to preeclampsia and eclampsia.30,31 In this study, the majority of health facilities with a similar set-up across types of facilities, locations and managing authority provide antenatal and postnatal care services. However, in terms of healthcare provider’s readiness, there was a high-level of difference in all three perspectives. This study revealed the number of health professionals that provided focussed antenatal care exceeded who were actually trained to provide this service. This indeed might be a key gap in the diagnosis of the disease and might reflect the reason for the high prevalence of national reports of preeclampsia/eclampsia.32
The WHO recommends a supplement of low dose calcium supplementation and acetylsalicylic acid (Aspirin) during antenatal care used as a prevention of preeclampsia. Low dose calcium administration depends on individual intake levels in order to avoid risks related to excessive intake.10,33 In Ethiopia, studies on calcium supplementation during the antenatal period reported that most Ethiopian women consume insufficient calcium, which increases the risk of preeclampsia.34,35 This indicates that more calcium supplementation is needed to be available in health facilities as a prevention mechanism of preeclampsia and for health care providers to provide to pregnant women. In contrast, we found that FmOH management protocol does not include this recommendation as part of their prevention strategy. This might be explained by a lack of detail and clear guidelines on calcium supplementation in the country and less attention has provided that might be related to a lack of clear understanding about the severity of these issues.19 Therefore, further study is recommended in revising the management protocol in line with the WHO recommendation and identifying the geographical areas that need calcium supplementation in settings with low calcium intake. Based on that evidence health facilities should provide calcium supplementation as a prevention strategy of preeclampsia/eclampsia.
Several studies globally15,36 as well as in Ethiopia37,38 have concluded that the increased use of MgSO4 is likely to have a substantial impact on reducing maternal mortality. In our study, the majority of health facilities have stock of at least one or more anticonvulsant drugs; however, diazepam injections were more widely available compared with MgSO4. Our findings also indicate that, private for-profit health facilities and health centres had more diazepam in stock than MgSO4, as compared with hospitals and public/government health facilities. In addition, more than half of the health facilities reported no stock of MgSO4. The shortage of MgSO4, especially in health centres and private health facilities, is more concerning. Health centres are the first contact point where most pregnant mothers received their antenatal care and delivery services, and they are widely available both in urban and rural areas, rather than hospitals which are limited in rural areas. Health centres are expected to initiate anticonvulsant treatment and referred to the hospitals for those mothers who need advanced care. Studies have supported the fact that a single dose of MgSO4 significantly reduces the risk of eclampsia seizures as well as severe complications compared with other anticonvulsants, including diazepam.39 Furthermore, private for-profit health facilities are usually expected to have more MgSO4, since the affordability and procurement process to purchase the drugs may not be as difficult compared with that of public/government funded facilities. However, our study findings show that these facilities have more diazepam available than MgSO4, and nearly half of them have experienced similar issues with stock being unavailable. At present, these health facilities are becoming the preferred maternal and newborn care centres in urban areas and are becoming one of the most commonly visited by mothers to access maternal and newborn care services, and these facilities have received more referral cases as well. These facilities have also failed to use MgSO4, which resulted in more maternal complications and perinatal mortality. Furthermore, this study indicated close to one third of health care providers did not receive training on how to administer IV/IM MgSO4 and a significant proportion of them either received on-the-job training more than a year previously, or never received training in maternal or newborn care. Despite evidence from several studies indicating that administering MgSO4 requires training in order to prevent its toxicity related to not properly administering the drug.32,40 Health care providers should be competent enough to administer as well as to early identify complications related with toxicity. As a result, health care providers with out-of-date training, together with frequent lack of supply of MgSO4, may compromise the service delivery to women with preeclampsia and eclampsia.
Strengths and Limitations of the Study
The findings of this study are highly representative and can apply to all regions of Ethiopia, as we used a nationally representative dataset. These findings might also apply to other developing countries with similar socioeconomic characteristics and health care systems. The data collection process, along with standard survey tools, and overall survey process involved several international and local partners as well as researchers who have experience in maternal and newborn health areas, along with standard survey tools. This study is the first of its kind to assess health facility readiness on the management of preeclampsia/eclampsia in Ethiopia. However, this study is not without limitations. First, this study was cross-sectional, in which causal relationships could not be established. Although this study shows substantial findings for service-related preeclampsia and eclampsia management in Ethiopia, health facilities that provide only prenatal and postnatal care were not included in this study, as the provision of delivery services was the main eligibility criteria for facility selection. This might have resulted in cases not being detected, and its management in those segments of health care facilities remaining unexamined. Lastly, this survey covered only 12 months of service reports, logbook reviews, and health care providers’ interviews, which might hinder long-term challenges related with service provisions.
Policy Implications
Findings reported in this study provide vital evidence to inform policy and guide health practitioners to review the management practice of preeclampsia and eclampsia in alignment with the national and WHO recommendations, as evidence showed preeclampsia and eclampsia were the second most common cause of maternal mortality in Ethiopia. Hence, it will be a challenge to achieve the target to reduce maternal mortality in Ethiopia unless there is timely intervention and improvement in the capacity of health facilities to detect and manage these cases. The government’s top priority should be focused on making the MgSO4 drug available in every health care facility, especially in health centres, rural areas and public/governmentally managed health facilities, as the majority of the population are receiving health services from these facilities. This strategy needs to be supported by continuous updates as well as increasing the knowledge of health care providers through on-the-job training and supervision. For those women that develop complications and need immediate delivery, expanding health facilities with comprehensive emergency maternal and newborn care should be established and existing health facilities should be improved. This study has added evidence to the current health care facility’s management practice of preeclampsia and eclampsia services and has provided a stimulus for future research on future study on preeclampsia and eclampsia in Ethiopia.
Conclusion
Overall, there was limited readiness of health facilities in Ethiopia for managing women with preeclampsia/eclampsia. This study highlighted the poor availability of supplies and diagnostic equipment to prevent and treat preeclampsia/eclampsia within Ethiopia health facilities. The Ethiopian national guideline for management of preeclampsia/eclampsia lacks prevention intervention as WHO recommends. In addition, this study’s findings indicate that there is a wide variation in health facilities’ readiness in terms of facility type, location, and managing authority toward prevention and management of preeclampsia/eclampsia. The majority of public/government managed health centres and rural health facilities were found to have poor availability of supplies and infrastructure to manage and prevent complications. By contrast, private for-profit facilities showed relatively better readiness; however, they fell behind the recommendations in having essential supplies such as MgSO4 available.
Acknowledgments
The authors would like to thank the University of Newcastle, Australia, for providing a scholarship opportunity to pursue my studies, free digital access to the online library and Meg Vertigan for her assistance in language review to this document. We would also like to give thanks to the EPHI 2016 EmONC assessment team, data collectors, trainers, and health facility authorities that participated in this national survey.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no conflicts of interest in relation to this work.
References
1. Abalos E, Cuesta C, Grosso AL, Chou D, Say L. Global and regional estimates of preeclampsia and eclampsia: a systematic review. Eur J Obstet Gynecol Reprod Biol. 2013;170(1):1–7. doi:10.1016/j.ejogrb.2013.05.005
2. Vidaeff AC, Saade GR, Sibai BM. Preeclampsia: the need for a biological definition and diagnosis. Am J Perinatol. 2021;38(9):976–982. doi:10.1055/s-0039-1701023
3. Osungbade KO, Ige OK. Public health perspectives of preeclampsia in developing countries: implication for health system strengthening. J Pregnancy. 2011;2011:481095. doi:10.1155/2011/481095
4. FDRE Ministry of Health (FMoH). Health sector transformation plan (HSTP) 2015/16–2019/20. Addis Ababa, Ethiopia; 2015.S
5. Gaym A, Bailey P, Pearson L, Admasu K, Gebrehiwot Y; Ethiopian National Em ONCAT. Disease burden due to pre-eclampsia/eclampsia and the Ethiopian health system’s response. Int J Gynaecol Obstet. 2011;115(1):112–116. doi:10.1016/j.ijgo.2011.07.012
6. Sibai B, Dekker G, Kupferminc M. Pre-eclampsia. Lancet. 2005;365(9461):785–799. doi:10.1016/S0140-6736(05)17987-2
7. Duley L, Meher S, Abalos E. Management of pre-eclampsia. BMJ. 2006;332(7539):463–468. doi:10.1136/bmj.332.7539.463
8. Sibai BM. Diagnosis and management of gestational hypertension and preeclampsia. Obstet Gynecol. 2003;102(1):181–192. doi:10.1016/s0029-7844(03)00475-7
9. Liu C-M, Chang S-D, Cheng P-J. Comparison of referral and non-referral hypertensive disorders during pregnancy: an analysis of 271 consecutive cases at a tertiary hospital. Chang Gung Med J. 2005;28(5):326–334.
10. World Health Organization. WHO recommendations for Prevention and treatment of pre-eclampsia and eclampsia. Geneva; 2011.
11. World Health Organization. WHO recommendations on antenatal care for a positive pregnancy experience. Geneva; 2016.
12. Federal Ministry health of Ethiopia. Management protocols for selected obstetric complications. Ethiopia; 2010.
13. Firoz T, Sanghvi H, Merialdi M, von Dadelszen P. Pre-eclampsia in low and middle income countries. Best Pract Res Clin Obstet Gynaecol. 2011;25(4):537–548. doi:10.1016/j.bpobgyn.2011.04.002
14. World Health Organization. WHO recommendations: policy of interventionist versus expectant management of severe pre-eclampsia before term. Geneva: World Health Organization; 2018.
15. Rawlins B, Plotkin M, Rakotovao JP, et al. Screening and management of pre-eclampsia and eclampsia in antenatal and labor and delivery services: findings from cross-sectional observation studies in six sub-Saharan African countries. BMC Pregnancy Childbirth. 2018;18(1):346. doi:10.1186/s12884-018-1972-1
16. Central Statistical Agency - CSA/Ethiopia, ICF. Ethiopia demographic and health survey 2016. Addis Ababa, Ethiopia: CSA and ICF; 2017.
17. World Health Organization. Standards for improving quality of maternal and newborn care in health facilities. Geneva, Switzerland; 2016.
18. Wagnew M, Dessalegn M, Worku A, Nyagero J. Trends of preeclampsia/eclampsia and maternal and neonatal outcomes among women delivering in Addis Ababa selected government hospitals, Ethiopia: a retrospective cross-sectional study. Pan Afr Med J. 2016;25(Suppl 2):12. doi:10.11604/pamj.supp.2016.25.2.9716
19. Eclampsia TPCE. Exploring barriers and opportunities for preeclampsia and eclampsia prevention and management in Ethiopia; 2018.
20. Kea AZ, Tulloch O, Datiko DG, Theobald S, Kok MC. Exploring barriers to the use of formal maternal health services and priority areas for action in Sidama zone, southern Ethiopia. BMC Pregnancy Childbirth. 2018;18(1):96. doi:10.1186/s12884-018-1721-5
21. Ministry of Health. Ethiopian Emergency Obstetric and Newborn Care (EmONC) assessment 2016 - Final report; 2017.
22. Ethiopian Public Health Institute FMoH, ICF International. Ethiopia service Provision Assessment Plus (SPA+) survey; 2014.
23. Croke K, Telaye Mengistu A, Connell SD, Tafere K. The impact of a health facility construction campaign on health service utilisation and outcomes: analysis of spatially linked survey and facility location data in Ethiopia. BMJ Global Health. 2020;5(8):e002430. doi:10.1136/bmjgh-2020-002430
24. Yasin C, Geleto A, Berhane Y. Referral linkage among public health facilities in Ethiopia: a qualitative explanatory study of facilitators and barriers for emergency obstetric referral in Addis Ababa city administration. Midwifery. 2019;79:102528. doi:10.1016/j.midw.2019.08.010
25. Federal Democratic Republic of Ethiopia. Emergency care, referral, and critical care development strategy. Ethiopia; 2016–2020.
26. Mahran A, Fares H, Elkhateeb R, et al. Risk factors and outcome of patients with eclampsia at a tertiary hospital in Egypt. BMC Pregnancy Childbirth. 2017;17(1):435. doi:10.1186/s12884-017-1619-7
27. Thaddeus S, Maine D. Too far to walk: maternal mortality in context. Soc Sci Med. 1994;38(8):1091–1110. doi:10.1016/0277-9536(94)90226-7
28. Nkamba DM, Vangu R, Elongi M, et al. Health facility readiness and provider knowledge as correlates of adequate diagnosis and management of pre-eclampsia in Kinshasa, Democratic Republic of Congo. BMC Health Serv Res. 2020;20(1):926. doi:10.1186/s12913-020-05795-1
29. Warren CIS, Oginni AB, Adoyi G, Kirk KR, Dempsey A, Landscaping analysis for pre-eclampsia and eclampsia in Nigeria. Abuja: Population Council. 2015: 36.
30. Mol BWJ, Roberts CT, Thangaratinam S, Magee LA, de Groot CJM, Hofmeyr GJ. Pre-eclampsia. Lancet. 2016;387(10022):999–1011. doi:10.1016/S0140-6736(15)00070-7
31. WHO Guidelines Approved by the Guidelines Review Committee. WHO recommendations on antenatal care for a positive pregnancy experience. Geneva: World Health Organization. Copyright © World Health Organization 2016; 2016.
32. Altman D, Carroli G, Duley L, et al. Do women with pre-eclampsia, and their babies, benefit from magnesium sulphate? The Magpie Trial: a randomised placebo-controlled trial. Lancet. 2002;359(9321):1877–1890.
33. World Health Organization. WHO recommendation: calcium supplementation during pregnancy for prevention of pre-eclampsia and its complications. Geneva: World Health Organization; 2018.
34. Tesfaye B, Sinclair K, Wuehler SE, Moges T, De-regil LM, Dickin KL. Applying international guidelines for calcium supplementation to prevent pre-eclampsia: simulation of recommended dosages suggests risk of excess intake in Ethiopia. Public Health Nutr. 2019;22(3):531–541. doi:10.1017/S1368980018002562
35. Birhanu Z, Chapleau GM, Ortolano SE, Mamo G, Martin SL, Dickin KL. Ethiopian women’s perspectives on antenatal care and iron-folic acid supplementation: insights for translating global antenatal calcium guidelines into practice. Matern Child Nutr. 2018;14 Suppl 1(Suppl1). doi:10.1111/mcn.12424
36. Gordon R, Magee LA, Payne B, et al. Magnesium sulphate for the management of preeclampsia and eclampsia in low and middle income countries: a systematic review of tested dosing regimens. J Obstet Gynaecol Can. 2014;36(2):154–163. doi:10.1016/S1701-2163(15)30662-9
37. Kassie GM, Negussie D, Ahmed JH. Maternal outcomes of magnesium sulphate and diazepam use in women with severe pre-eclampsia and eclampsia in Ethiopia. Pharm Pract. 2014;12(2):400. doi:10.4321/S1886-36552014000200006
38. Getaneh W, Kumbi S. Use of magnesium sulfate in pre-eclampsia and eclampsia in teaching hospitals in Addis Ababa: a practice audit. Ethiop Med J. 2010;48(2):157–164.
39. Nagaria T, Mitra S, Banjare SP. Single loading low Dose MgSo(4) regimen: a simple, safe and effective alternative to Pritchard’s regimen for Indian women. J Clin Diagn Res. 2017;11(8):QC08–QC12.
40. Bain ES, Middleton PF, Crowther CA. Maternal adverse effects of different antenatal magnesium sulphate regimens for improving maternal and infant outcomes: a systematic review. BMC Pregnancy Childbirth. 2013;13(1):195. doi:10.1186/1471-2393-13-195
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.