")
Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 15
Health Care Needs Among People Living with HIV: The Implication of Continuum of Care
Authors Ibrahim K , Rahayuwati L , Herliani YK , Pramukti I
Received 3 January 2023
Accepted for publication 11 May 2023
Published 19 May 2023 Volume 2023:15 Pages 235—246
DOI https://doi.org/10.2147/HIV.S403510
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Olubunmi Akindele Ogunrin
Kusman Ibrahim,1 Laili Rahayuwati,2 Yusshy Kurnia Herliani,1 Iqbal Pramukti2
1Department of Medical and Surgical Nursing, Faculty of Nursing, Universitas Padjadjaran, Sumedang, West Java, Indonesia; 2Community Health Nursing, Faculty of Nursing, Universitas Padjadjaran, Sumedang, West Java, Indonesia
Correspondence: Kusman Ibrahim, Department of Medical and Surgical Nursing, Faculty of Nursing, Universitas Padjadjaran, Jl. Raya Bandung-Sumedang KM. 21, Jatinangor, Sumedang, West Java, 45363, Indonesia, Tel +62-81321281117, Fax +62 22-7795596, Email [email protected]
Background: Human immunodeficiency virus remains a major public health problem in Indonesia. People living with HIV (PLWH) have various health problems as result from disease progression that impacts their health care needs. This study aims to explore health care needs and to test the factors associated with health care needs among people living with HIV.
Methods: A cross-sectional descriptive study design was undertaken with 243 respondents completing a self-reported HIV-Health Care Need Questionnaire. Participants were recruited using the purposive sampling technique from six HIV clinics in West Java, Indonesia. The data were analyzed using descriptive and multiple logistic regression statistical techniques.
Results: The majority of the subjects were diagnosed within less than 5 years and have been receiving antiretroviral therapy. Nursing care was indicated as the most needed, offered, and received care. Emergency financial assistance, legal services, insurance premiums, and nutritional intervention were perceived as gaps between needed and received. Characteristics such as age, educational background, having HIV manager, and income were significantly correlated to nutritional care (p< 0.05). Nutritional care was increased by 3.96% if PLWH having HIV manager (CI: 1.17– 13.38, p< 0.05).
Conclusion: Addressing the gap between health care needs and health offered was important to ensure that care was received appropriately. Continuing assessment of health care needs can provide direction to deliver appropriate care and ensure a comprehensive continuum of care for PLWH.
Keywords: continuum of care, continuity of patient care, health services, HIV testing, needs
Introduction
Human immunodeficiency virus (HIV) and acquired immunodeficiency syndrome (AIDS) remain major health problems in many countries.1 In 2021, the United Nations Programme on HIV/AIDS (UNAIDS) reported that there were 38.4 million PLWH globally.2 Greater than 99% of PLWH in South-East Asia reside in five countries, namely, India, Indonesia, Myanmar, Nepal and Thailand.3,4 AIDS-related deaths and new HIV infections have declined in all affected countries except Indonesia.5 In Indonesia, the number of PLWH is approximately 520,000 with a 0.3% prevalence among adults.4 Additionally, a rapid increase in the number of AIDS-related deaths from 24,000 in 2010 to 38,000 in 2018 has been noted.6
People living with HIV (PLWH) represent a wide range of individuals and experience many problems due to AIDS and related treatment. The advancement of anti-retroviral therapy (ART) has changed drastically the course of disease and decreased HIV-associated morbidity and mortality. It has transformed HIV from an acute-fatal illness to a manageable long-term condition.7 Although ART allows PLWH to live longer, they still face many challenges related to major chronic complications and comorbidities as well as side effects of lifelong treatment.8 In addition, HIV/AIDS may cause a significant psychological burden. PLWH often reported depression and anxiety resulting from the HIV diagnosis and the difficulties of living with a chronic illness. Social stigma and discrimination in both community and health-care setting were still prevalent in many countries. The HIV-related health problems have a significant impact on health care needs and services of PLWH.9,10
Several studies have examined the factors influencing health care for PLWH, namely, individuals, relationships, communities, health care systems, policies11 and work environments.12 Proper health care is necessary to increase health-related quality of life and well-being of PLWH.10 Failure to address health care needs of PLWH may impact the success of halting HIV epidemic that has been targeted by the world leaders to be achieved in 2030. In addition, the health-care needs of PLWH can be addressed by preventive measures, counselling, diagnostic methods, treatment, and rehabilitation.13 Therefore, better understanding the health- care needs of PLWH is very important in motivating and keeping them engaged with care and in providing specific care that fit with their specific needs. When PLWH receive full attention and care that suit their characteristics and needs, they will be motivated to visit the clinic, adhere to treatment, and retain care, which subsequently leads to effective viral suppression. On the other hand, a better understanding and a continuum of care will probably increase the proportion of those initiating ART, engaging in sustained care, and achieving viral suppression.14 Nurses are the main health care providers who play a major role in providing nursing care for HIV patients. Nevertheless, nurses need to have a deep understanding of the healthcare needs of their patients to ensure comprehensive and continuous care.
Methods
Study Design
This study aims to examine the health care needs among people living with HIV as an implication of continuum care in Indonesia. A cross-sectional descriptive study design was undertaken in this study.
Sample
The study population was PLWH in five major cities, West Java, Indonesia. The sample of 243 respondents were recruited purposively from six hospital-affiliated HIV clinics in five major cities in West Java (Bandung City, Cirebon City, Cirebon Regency, Sumedang Regency, and Banjar City). The inclusion criteria were adult HIV-positive patients who has been living with HIV for at least 6 months since they were found to be HIV positive, able to read and write in Indonesia language, and willing to participate throughout the study. During the research process, no respondent resigned.
Data Collection
The data were collected from May to October 2017. This study was conducted according to the ethical guidelines of the Declaration of Helsinki. Informed consent was obtained from all respondents. The study was approved by the Research Ethics Committee of the Universitas Padjadjaran, Indonesia with the letter number 807/UN.6.C.10/PN/2017. The health care need data were collected using the self-reported HIV-Health Care Need Questionnaire (HIV-HCNQ), which was adapted from the Atlanta Ema Consumer Survey of People Living with HIV and AIDS.15 The instrument was adapted and modified to fit the contextual background of the targeted population. The questionnaire consisted of 48 items divided into three parts: demographic data, health characteristics, and health care needs. The questionnaire consists of open questions, multiple choice questions, and dichotomous questions. Two experts from Indonesia reviewed the content validity of the instrument, which yielded good agreement with a Cronbach alpha value of 0.821. The sociodemographic data including HIV clinic, gender, age, marital status, education level, monthly income, and occupation were collected. The health characteristic refers to the categorization of the health status into four categories including risk behavior and HIV test, anti-retroviral therapy (ART), care, and support. For health care related to support, the data was presented as “needed care”, “offered care”, “received care”, and “gap”. The needed care refers to the care needed by the PLWH, the offered care refers to the care offered by the HIV care provider, received care refers to the care received by the PLWH, and the gap refers to the difference between received care and needed care.
Data Analysis
Descriptive statistical techniques including frequency, percentage, and p-value significance level of 0.05 were used to describe the demographics, health characteristics, and care needs of the respondents. A logistic regression model was used to determine factors affecting health care needs. All variables with p values < 0.05 in the univariable analysis were entered in a multivariable analysis. The data were managed and analyzed using IBM SPSS 24.0 for windows.
Results
Demographic Characteristics
Demographic data of respondents (n=243) from six hospitals showed that the majority of the respondents were male (n=161, 66.3%), and most of the respondents were 30–39 years in age (n=108, 44.4%). Most of the respondents were married (n=109, 44.9%), and greater than half of the total respondents had a high school education (n=137, 56.4%). Respondents with an income of IDR >1,500,000–2,500,000 (n=66, 27%) had jobs as private employees (n=94, 38.7) (Table 1).
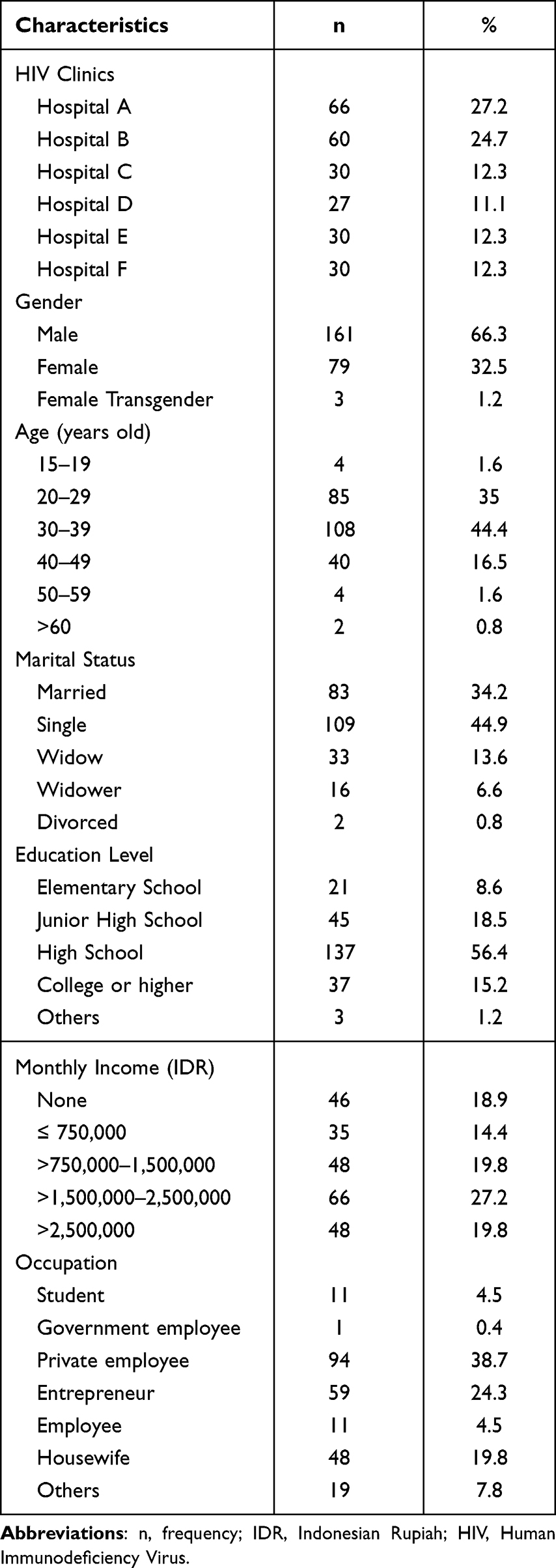 |
Table 1 Respondents’ Demographic Characteristics (n=243) |
Health Characteristics
The majority of the positive respondents diagnosed in less than five years were (n=187, 75.7%) homosexual (n=74, 30.5%), diagnosed as HIV positive between the ages of 20–29 years old (n=138, 56.8%), and had not been previously tested for HIV (n=151, 62.1%); therefore, the majority of positive respondents were likely to get HIV tests because they felt sick (n=61, 25.1%). The majority of respondents were receiving ART (n=216, 88.9%). Most of the respondents had been on ART for less than 5 years (n=167, 68.7%), participated in counselling (n=221, 97.5%), and never changed ART history (n=237, 97.5%). The majority of respondents did not miss the drug within the last 30 days (n=176, 72.4%). Most respondents had a recent CD4 count of 350–500 cells/mm³ (n=64, 26.3%) and did not know their recent result of the viral load test (n=139, 57.2). The majority reported that they had not been hospitalized due to HIV/AIDS-related conditions for the past 12 months (n=151, 62.1%). Government hospitals were chosen as the most visited health care facility (n=214, 88.1%). Approximately half of the respondents personally paid for their treatment cost (n=117, 48.1%). Additionally, one-third of the subjects reported having comorbid diseases, such as tuberculosis (TB), hypercholesterol, hypertension, asthma, and other chronic diseases. The majority did not report having hepatitis (n=219, 90.1%). The majority of respondents had not visited mental health services (n=199, 81.8%). Approximately half of the subjects who visited the service reported depression as their main reason (40.9%). Additionally, approximately half of the subjects had substance abuse counselling (n=119, 49%), and they talked about HIV mostly with health professionals (n=125, 51.4%) (Table 2).
 |
Table 2 Health Characteristics Among PLWH (n=243) |
Health Care Service and Support Needed
Table 3 shows the health care services and support needed by the subjects. Nursing care was reported to be mostly needed by the majority (n=234, 96.3%) followed by treatment compliance (n=227, 93.4%), peer group support (n=203, 83.5%), financial assistance for examinations (n=196, 80.7%), and premium insurance (n=195, 80.2%). However, they emphasized the wide gap between the needed and received services, particularly in terms of premium insurance, emergency financial assistance (EFA), nutritional care, and legal services. These results indicate that PLWH have a high need for those services, but only a few received them.
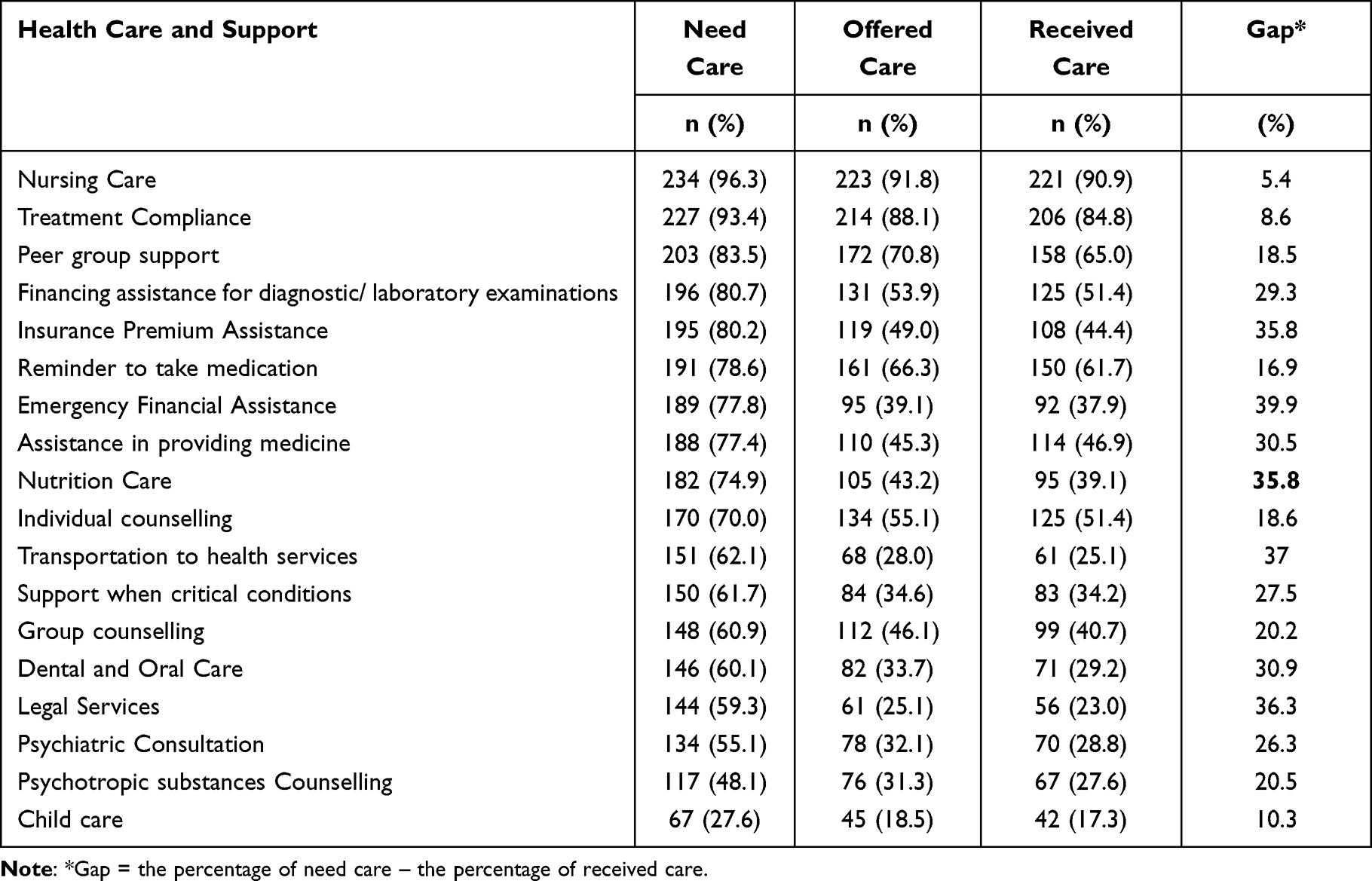 |
Table 3 Health Care and Support Needed (n=243) |
Multivariate Analysis
A logistic regression analysis was performed to examine the relationships between subjects’ characteristics and components of health care and support needed. The results showed some characteristics (age, educational background, having HIV manager, and income) were significantly correlated to nutritional care (Table 4). On a multivariate analysis, it was found that after controlled by age, education, and income; for all health care and support needed, having HIV manager remains significantly correlated to nutritional care. Nutritional care was increased by 3.96% if PLWH having HIV manager (Table 5).
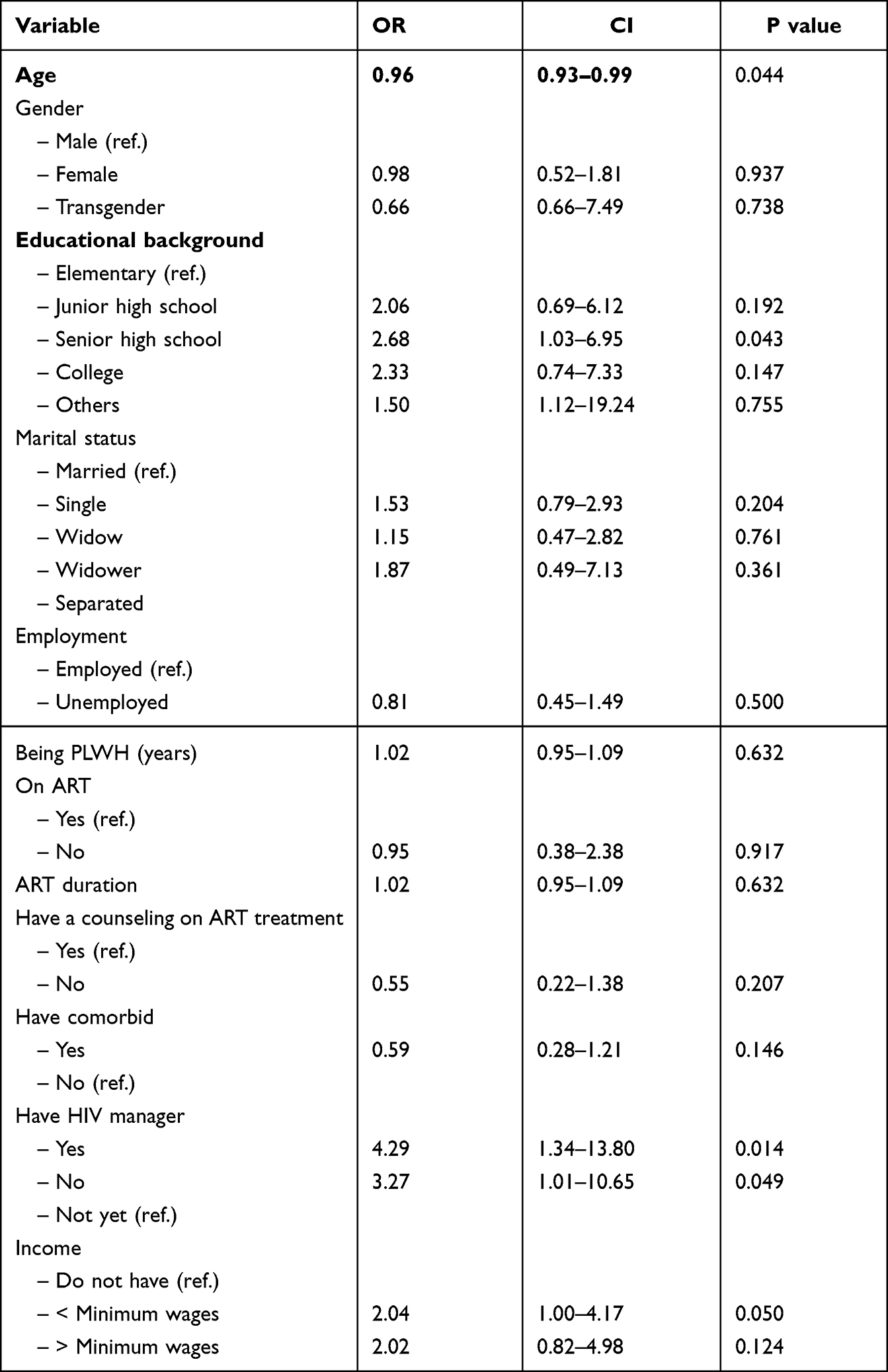 |
Table 4 Logistic Regression Analysis for Factors Affecting Healthcare Need on Nutritional Care |
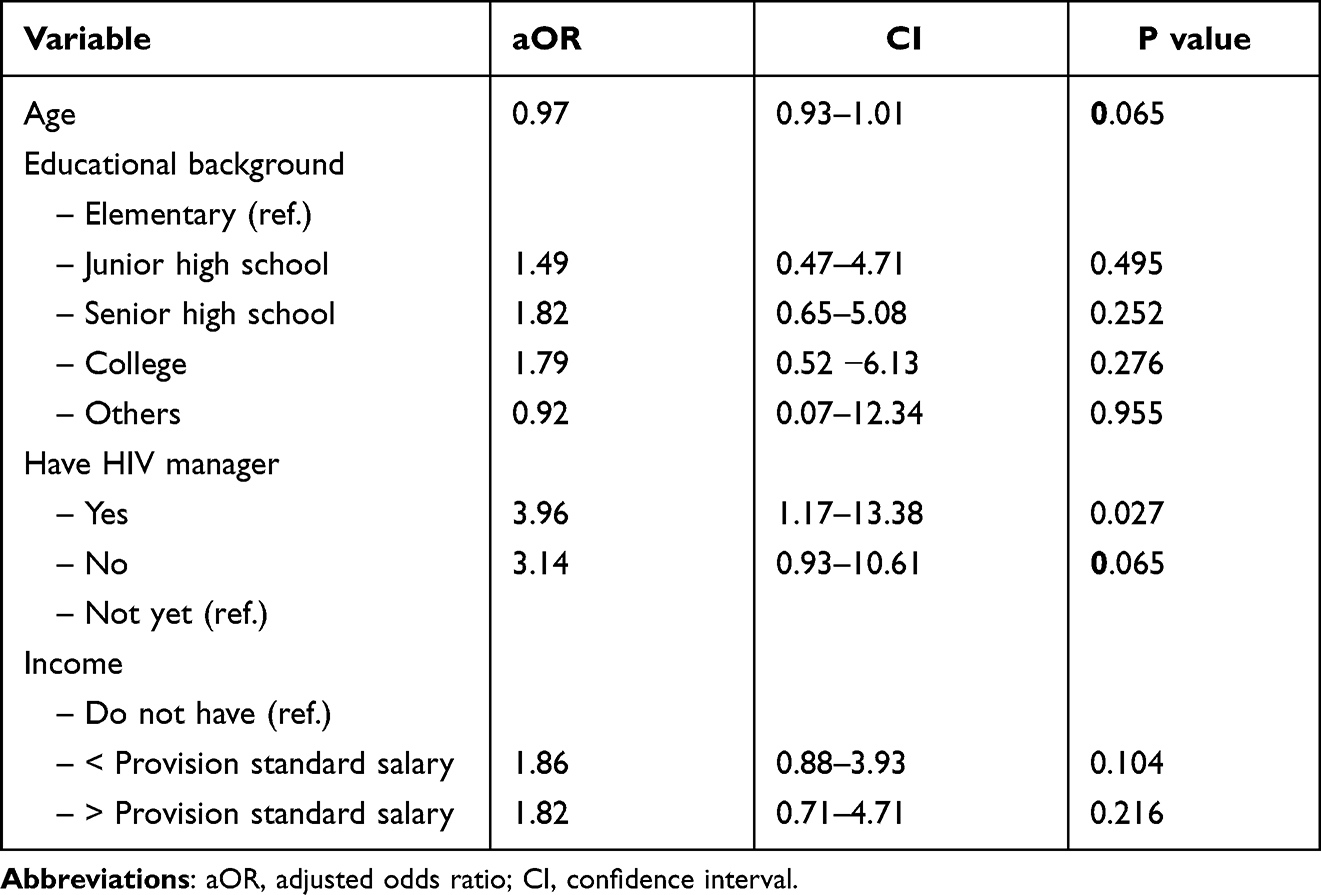 |
Table 5 Multivariate Logistic Regression Analysis for Factors Affecting Healthcare Need on Nutritional Care |
Discussion
The national HIV/AIDS strategy to improve health outcomes would not be achieved without proper understanding of the needs of PLWH. This study described the health characteristics, care, and support needed by PLWH, especially in West Java, Indonesia. Based on demographic data, the majority of respondents had HIV for less than five years and exhibited homosexual behaviours. In addition, the majority of PLWH were aged 20–29 years and had never had an HIV test before. In Indonesia, the majority of PLHW are at the productive age of 24–29 years.16 Additionally, the existence of homosexuality has a long pro-contra history. In the past, a large majority of Indonesians saw this practice as a taboo due to religious beliefs that considered it a sinful act.17
We also found a low awareness of the respondents to undergo HIV testing, and these respondents mainly underwent HIV testing when they were sick. Previous studies reported that participants chose self-prescription as the first choice of treatment for their illness followed by traditional and conventional medicines.18,19 Therefore, many people visit health care facilities only when their illness worsens or when self-treatment fails. In addition, we also found that media campaigns and community programs about HIV were still not highly prevalent. Previous research stated that media campaigns related to HIV were still low due to the high level of discrimination.20 This is a problem that must be resolved. The government can disseminate information related to HIV disease in educational and social environments.
Based on health characteristics data, we found that the majority of ART coverage was good. However, there were still PLWH who had not received ART, and there were still PLWH who did not routinely undergo counselling. Thus, adherence to ART regimens was also still lacking. Of course, this needs to be a concern for the Indonesian government, where the ART achievement rate is still 50% in 17 provinces.21 Previous research has suggested that counselling is a good medium for increasing adherence to ART regimens.22–24 Thus, the government is expected to increase the role of counsellors to increase ART consumption for PLWH. This notion is confirmed the findings of this study given that the subjects’ CD4 counts were less than 500 cell/mm³, and few had undetected viral loads. Studies have suggested that a lower CD4 count was associated with a higher probability of dropping out, which might subsequently contribute to a loss of economic productivity.25
Our findings showed that the majority of PLWH reported that they had not been hospitalized for HIV/AIDS-related conditions. However, PLWH are also being treated in the hospital due to their declining HIV condition and need to be considered. Many previous studies have reported that ART contributes to a good quality of life and reduces the transmission of HIV.26,27 Many PLWH use government hospitals for examinations. The hospital offers more complete services, so it becomes a resource for treatment for PLWH. However, we found that the majority of PLWH still used personal payments, and not all of them used health insurance. The Indonesian government states that the cost of PLWH maintenance and control can be assisted by health insurance with a special allocation from the government.28 Thus, this service can reduce the cost burden for PLWH. Data show that approximately 10% of PLWH still have infectious diseases, such as hepatitis. Previous studies have shown that HIV-positive individuals are more at risk for contracting and developing diseases, such as cardiovascular, metabolic, pulmonary, renal, bone and malignant diseases, compared with HIV-negative individuals.29,30
The majority reported that they had not visited any mental health services. Approximately half of those who received mental health services reported “depression” as their main reason. Additionally, approximately half underwent substance abuse counselling. Previous studies reported that many experienced depression, stress, anxiety, lack of social support, and poor coping strategies.31–35 Stigma and discrimination were regarded as the main causes of their psychological problems, which can lead to low self-esteem, depression, despair, and even suicidal thoughts. These individuals are afraid and ashamed to seek treatment and disclose their status. They mostly talked about HIV with health professionals compared with counsellors and case managers. This finding should represent a call for the government to increase the role of counsellors and case managers. The results of previous studies show that the counsellor and case manager play an important role in improving communication with PLWH for ART regimen continuation and control hospital visits.36,37
In this study, we observed a gap between needed care and received care, namely, insurance premiums, emergency financial assistance, nutrition care, and legal services. Insurance is important for PLWH during the treatment and consumption of ARVs. Insurance can reduce the economic and psychological burden of PLWH.38 Emergency financial assistance was found to represent a gap from the maintenance needed and obtained by PLWH. EFA can be applied for short-term or one-time financial assistance to assist with emergency expenses.39 In Indonesia, the government has facilitated the use of government health insurance.40 Furthermore, nutrition care is also a gap accepted by PLWH. PLWH need nutrition care to increase immunity such that CD4 and body mass index (BMI) can increase. Presentation of HIV manager was significantly increased nutritional care among PLWH. Previous research has shown supported this notion.41 We found legal services, such as health facilities, represent another gap. In West Java, there were significant improvements in widely distributed health care services that offered HIV tests, counselling care, and support. Approximately 180 clinics that offered HIV tests, care, and support. This is quite different from a study in Bandung City, which found that health care services for HIV/AIDS remained limited.42
In general, this study is limited to the type of descriptive research that presents data in terms of percentages. Research on a broader scale can provide a detailed description of health care needs among PLWH in Indonesia. In addition, the use of different development and study design approaches can provide more varied information.
Conclusion
This study demonstrated that the identified gaps, such as insurance premiums, emergency financial assistance, nutrition care, and legal services, represent a task that must be addressed by the health workers. The HIV manager was directly correlated to nutritional care among PLWH in this study. Addressing the gap between health care needs and health offered was important to ensure that care was received appropriately. Continuing assessment of health care needs can provide direction to deliver appropriate care and ensure a comprehensive continuum of care for PLWH. Nurses who are commonly as the most proportion of health care workers can take benefit from the study to understand and address the health care needs of PLWH to ensure comprehensive and continuous care. In terms of study design, developmental studies can provide more detailed and varied information about health care needs for the continuum of care among PLWH.
Acknowledgment
We would like to acknowledge the Ministry of Research, Technology and Higher Education of Indonesia for providing research grants and the University of Padjadjaran for their support. We would also like to thank the directors and nursing staff of the study hospitals for their permission and cooperation. Finally, we thank the participants for their time and the information they provided.
Funding
This study received funding from Ministry of Research, Technology, and Higher Education, The Republic of Indonesia, contract number: 718/UN6.3.1/PL/2017.
Disclosure
The authors declare that they have no conflicts of interest in this study.
References
1. World Health Organization. HIV/AIDS. World Health Organization; 2020.
2. UNAIDS. Fact sheet 2022: global HIV statistics. Available from: https://www.unaids.org/sites/default/files/media_asset/UNAIDS_FactSheet_en.pdf.
3. Singh PK. Special issue on Hiv aids response in WHO sear in journal of virus eradication. J Virus Eradicat. 2016;20:154.
4. UNAIDS. Global HIV & AIDS statistics — 2020 fact sheet; 2020. Available from: UNAIDS.unaids.org.
5. Pendse R, Gupta S, Yu D, Sarkar S. HIV/AIDS in the South-East Asia region: progress and challenges. J virus Erad. 2016;2(Suppl 4):1–6. doi:10.1016/S2055-6640(20)31092-X
6. World Health Organization. Indonesia HIV Country Profile 2019. World Health Organization; 2020.
7. Kurtyka D. From terminal disease to chronic illness: HIV infection in 2010. Adv Nurse Pract. 2010;18(1):33–38.
8. Deeks SG, Lewin SR, Ross AL, et al. International AIDS Society global scientific strategy: towards an HIV cure 2016. Nat Med. 2016;22(8):839–850. doi:10.1038/nm.4108
9. Ahmad A, Neelamegam M, Rajasuriar R. Ageing with HIV: health implications and evolving care needs. J Int AIDS Soc. 2020;23(9):e25621. doi:10.1002/jia2.25621
10. Bernard S, Tailor A, Jones P, Alexander DE. Addressing the medical and support service needs of people living with HIV (PLWH) through Program Collaboration and Service Integration (PCSI). Californian J Health Promot. 2016;14(1):1–14. doi:10.32398/cjhp.v14i1.1860
11. Mugavero MJ, Norton WE, Saag MS. Health care system and policy factors influencing engagement in HIV medical care: piecing together the fragments of a fractured health care delivery system. Clin Infect Dis. 2011;52(Suppl 2):S238–46. doi:10.1093/cid/ciq048
12. Genberg B, Wachira J, Kafu C, et al. Health system factors constrain HIV care providers in delivering high-quality care: perceptions from a qualitative study of providers in Western Kenya. J Int Assoc Provid AIDS Care. 2019;18:2325958218823285. doi:10.1177/2325958218823285
13. Moradi G, Mohraz M, Gouya MM, et al. Health needs of people living with HIV/AIDS: from the perspective of policy makers, physicians and consultants, and people living with HIV/AIDS. Iran J Public Health. 2014;43(10):1424–1435. doi:10.1111/scd.12056
14. Poudel KC, Jimba M. HIV care continuum for key populations in Indonesia. Lancet HIV. 2018;5(10):e539–40. doi:10.1016/S2352-3018(18)30169-3
15. DeMayo M, McFarlane A, Copeland B, Kevin H, Stephanie B, White KW. Atlanta EMA HIV/AIDS consumer survey. USA; 2012.
16. Ministry of Health of the Republic of Indonesia. Report on the progress of HIV/AIDS and infection sexuaal transmitted diseases the second quarter in 2019. Jakarta - Indonesia; 2019.
17. Kerr JC, Valois RF, DiClemente RJ, et al. The effects of a mass media HIV-risk reduction strategy on HIV-related stigma and knowledge among African American adolescents. AIDS Patient Care STDS. 2015;29(3):150–156. doi:10.1089/apc.2014.0207
18. Rahayuwati L, Ibrahim K. Health seeking behavior on breast cancer therapies: patients versus providers views. J Commun Public Heal Nurs. 2016;2(3):153.
19. Indonesia National Institute of Health Research and Development. Main Results of Baseline Health Research 2018. Jakarta: Ministry of Health of the Republic of Indonesia; 2018:66.
20. French RS, Bonell C, Wellings K, Weatherburn P. An exploratory review of HIV prevention mass media campaigns targeting men who have sex with men. BMC Public Health. 2014;14(1):616. doi:10.1186/1471-2458-14-616
21. Kemenko PMK. Menuju Indonesia Bebas AIDS 2030. Kementerian Koordinator Bidang Pembangunan Manusia dan Kebudayaan Republik Indonesia; 2020.
22. Dzansi G, Tornu E, Chipps J. Promoters and inhibitors of treatment adherence among HIV/AIDS patients receiving antiretroviral therapy in Ghana: narratives from an underserved population. PLoS One. 2020;15(3):e0230159. doi:10.1371/journal.pone.0230159
23. Musayón-Oblitas Y, Cárcamo C, Gimbel S. Counseling for improving adherence to antiretroviral treatment: a systematic review. AIDS Care. 2019;31(1):4–13. doi:10.1080/09540121.2018.1533224
24. Uusküla A, Laisaar K-T, Raag M, et al. Effects of counselling on adherence to antiretroviral treatment among people with HIV in Estonia: a randomized controlled trial. AIDS Behav. 2018;22(1):224–233. doi:10.1007/s10461-017-1859-6
25. Siregar AY, Pitriyan P, Wisaksana R. HIV patients drop out in Indonesia: associated factors and potential productivity loss. Acta Med Indones. 2016;48(3):207–216.
26. Liping M, Peng X, Haijiang L, Lahong J, Fan L. Quality of life of people living with HIV/AIDS: a cross-sectional study in Zhejiang Province, China. PLoS One. 2015;10(8):e0135705. doi:10.1371/journal.pone.0135705
27. Yaya I, Djalogue L, Patassi AA, et al. Health-related quality of life among people living with HIV/AIDS in Togo: individuals and contextual effects. BMC Res Notes. 2019;12(1):140. doi:10.1186/s13104-019-4171-x
28. Reynas A, Vincentius J, Lusius G. BPJS Kesehatan Tidak Jamin ARV Untuk Orang Dengan HIV. Tribun Kesehatan; 2019.
29. De Francesco D, Verboeket SO, Underwood J, et al. Patterns of co-occurring comorbidities in people living with HIV. Open Forum Infect Dis. 2018;5(11). doi:10.1093/ofid/ofy272
30. Schouten J, Wit FW, Stolte IG, et al. Cross-sectional comparison of the prevalence of age-associated comorbidities and their risk factors between HIV-infected and uninfected individuals: the AGEhIV cohort study. Clin Infect Dis. 2014;59(12):1787–1797. doi:10.1093/cid/ciu701
31. Bumb SS, Dodamani A. Stress, anxiety, and depression among human immunodeficiency virus / acquired immune deficiency syndrome patients. Int J Sci Study. 2019;6(12):2–7.
32. Silva RTS, da Silva RAR, Rodrigues ID, de Souza Neto VL, da Silva BCO, Souza FM. Coping strategies of people living with AIDS in face of the disease. Rev Lat Am Enfermagem. 2018;26. doi:10.1590/1518-8345.2284.2985
33. Deshmukh N, Borkar A, Deshmukh J. Depression and its associated factors among people living with HIV/AIDS: can it affect their quality of life? J Fam Med Prim Care. 2017;6(3):549. doi:10.4103/2249-4863.222016
34. Wang H, Zhang C, Ruan Y, Li X, Fennie K, Williams AB. Depressive symptoms and social support among people living with HIV in Hunan, China. J Assoc Nurses AIDS Care. 2014;25(6):568–576. doi:10.1016/j.jana.2014.02.001
35. Ibrahim K, Herliani YK, Rahayuwati L, Khadijah S, Sutini T. Healthcare needs of people living with human immunodeficiency virus: a qualitative descriptive study. Nurs Open. 2022;9(1):349–357. doi:10.1002/nop2.1071
36. Wilson MG, Husbands W, Makoroka L, et al. Counselling, case management and health promotion for people living with HIV/AIDS: an overview of systematic reviews. AIDS Behav. 2013;17(5):1612–1625. doi:10.1007/s10461-012-0283-1
37. Shelton RC, Golin CE, Smith SR, Eng E, Kaplan A. Role of the HIV/AIDS case manager: analysis of a case management adherence training and coordination program in North Carolina. AIDS Patient Care STDS. 2006;20(3):193–204. doi:10.1089/apc.2006.20.193
38. Nguyen QLT, Van Phan T, Tran BX, et al. Health insurance for patients with HIV/AIDS in Vietnam: coverage and barriers. BMC Health Serv Res. 2017;17(1):519. doi:10.1186/s12913-017-2464-0
39. Los Angeles County Commission on HIV. Emergency financial assistance standards care. Los Angeles; 2020.
40. BPJS. Pemanfaatan Data Jkn Untuk Perbaikan Sistem Kesehatan Di Indonesia. Info Bpjs Kesehatan; 2019.
41. Sidibé S, Delamou A, Kaba ML, et al. The effects of nutritional supplementation on body mass index and CD4 count among adult people living with HIV AIDS on antiretroviral treatment in Conakry, Guinea. J Public Health Africa. 2018;9(1):708.
42. Ibrahim K, Haroen H, Pinxten L. Home-based care: a need assessment of people living with HIV infection in Bandung, Indonesia. J Assoc Nurses AIDS Care. 2011;22(3):229–237. doi:10.1016/j.jana.2010.10.002
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.