")
Back to Journals » International Journal of Women's Health » Volume 9
Health care decision making autonomy of women from rural districts of Southern Ethiopia: a community based cross-sectional study
Authors Alemayehu M , Meskele M
Received 26 December 2016
Accepted for publication 31 March 2017
Published 19 April 2017 Volume 2017:9 Pages 213—221
DOI https://doi.org/10.2147/IJWH.S131139
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Mihiretu Alemayehu, Mengistu Meskele
School of Public Health, College of Health Sciences and Medicine, Wolaita Sodo University, Wolaita Sodo, Ethiopia
Introduction: Millions of women have little health care decision making autonomy in many cultures and tribes. African women are often perceived to have little participation in health care decisions. However, little has been investigated to identify factors contributing to decision making autonomy. Hence, it is important to obtain information on the contributing factors of decision making autonomy and disparities across different socio-cultural contexts.
Methodology: A cross-sectional study was conducted in Wolaita and Dawro zones, Southern Ethiopia from February to March 2015. A total of 967 women were selected through multi-stage sampling. A survey was administered face-to-face through an interview format. EpiData v1.4.4.0 and SPSS version 20 were used to enter and analyze data, respectively. Proportions and means were used to describe the study population. Variables with P-value <0.2 in bivariate analysis were selected for multivariable regression. Finally, variables with P-value <0.05 in multivariable logistic regressions were identified as independent predictors. Odds ratios along with confidence intervals were used to determine the presence of association.
Result: It was determined that 58.4% of women have autonomy, while 40.9% of study participants’ health care decisions were made by their husbands. The husband’s education (adjusted odds ratio [AOR] =1.91 [1.10, 3.32]), wealth index (AOR =0.62 [0.42, 0.92]), age (AOR =2.42 [1.35, 4.32] and AOR =7 [3.45, 14.22]), family size (AOR =0.53 [0.33, 0.85] and AOR =0.42 [0.23, 0.75]), and occupation (AOR =1.66 [1.14, 2.41]), were predictors of health care decision making autonomy.
Conclusion: Even though every woman has the right to participate in her own health care decision making, more than two fifths of them have no role in making health care decisions about their own health. Husbands play a major role in making health care decisions about their wives. A comprehensive strategy needs to be implemented in order to empower women, as well as to challenge the traditional male dominance. Special attention has to be given to women living in rural areas in order to reduce their dependency through education and income generating activities.
Keywords: decision making, women’s autonomy, health care decision, women’s empowerment, Wolaita, Dawro, Southern Ethiopia
Introduction
Autonomy is the power to obtain information and arrive at decisions about personal concerns.1 The ability of women to seek health services and visit health care facilities depends on their decision making autonomy. However, in developing countries, their status within the society mostly limits their decision making power regarding their own lives. The existing socio-cultural, religious, and tribal structures that define gender roles often determine the circumstances under which women would have autonomy in health care decision making.2
The autonomy of women in health care decision making is tremendously crucial for improved maternal and child health outcomes, and women’s empowerment.3 The 1994 United Nations International Conference on Population and Development widely asserted that increased gender equality among the family is a requirement for achieving advances in all matters of development. Its program of action highlighted the need for improving women’s status for the enhancement of their decision making capacity at all levels in all spheres of life.4 Evidence from developing countries indicated that women’s autonomy is the major contributing factor of maternal health care utilization.5 Accordingly, women with greater freedom of movement are more likely to receive and utilize antenatal and delivery care services; suggesting that women’s autonomy is equally as important as educational and economic levels. Evidence from African countries6 has shown that women with lower autonomy in household decision making were at higher risk of malnutrition. Besides, it is also stated that women’s autonomy is an important determining factor for child survival and pediatric health.7 Studies have also shown that higher female autonomy confers benefits including total fertility reduction, higher child survival rates, and allocation of resources in favor of children in the household.8
However, power disparities within wedlock can limit clear interaction between couples about reproductive health decisions and women’s access to the services. This can in turn contribute to poor health outcomes for the woman, her child, her family, and the community and a nation at large.9 Evidence from Africa and South-East Asian countries has shown that women usually have less power and decision making autonomy than men, concerning issues related to their own health care. Moreover, they usually have unequal access to nutrition, education, and health care, as well as a limited opportunity to earn income and have control over resources, as well as few effective legal rights.10
Gender impartiality renders women both increased decision making autonomy and better health outcomes such as reduction in fertility rate, increase in family planning utilization, and decrease in level of unmet need for contraception.11 Evidence has shown that age and family structure are strongly associated with decision making autonomy of women.12 Older women and women in a nuclear family are more likely to have better decision making autonomy. Besides, women who have a substantial role in their own reproductive health care tend to be more literate, involved in income generating activities, and marry later.13 Other evidence has also shown that the poor tend to be sicker and utilize health care facilities less frequently than their counterparts.14 Moreover, literate and employed partners are more likely to participate in the final decisions.15
Even though women from sub-Saharan African countries are often perceived to have less control over resources and participation in reproductive health decisions,16 this should not be over-generalized since the amount of control men have over their wives and the disparity between men and women vary from place to place, time to time, and involve several other factors. For instance, evidence from Ethiopian demographic and health surveys has shown that approximately six out of every ten married women were employed, whereas almost all currently married men aged 15–49 were employed in the 12 months preceding the survey. Besides, nearly a quarter of married women had no health care decision making autonomy.17
Even though gender equality gives women increased decision making authority and improved reproductive outcomes,11 millions of women have little autonomy in many cultures and tribes, thus it is important to obtain information on the contributing factors of decision making autonomy and disparities across different socio-cultural contexts. Therefore, this study was aimed at identifying factors which contribute to women’s decision making autonomy concerning their own health care. Besides, this study can also be replicated and extended to other rural communities of the nearby African countries, which have similar socio-cultural and economic systems as the study setting.
Methodology
Study design and area
A community based cross-sectional study was conducted in Southern Ethiopia from February 1 to March 30, 2015. Two zones, Wolaita and Dawro were purposively selected from the 13 zones of the region. Since women’s autonomy is relatively low among rural women, the current study exclusively dealt with decision making autonomy among rural dwellers. These zones were selected for their large proportion of rural population. Accordingly, 88.3% of Wolaita and 92.9% of Dawro zone inhabitants were rural dwellers.18 Based on the 2007 Ethiopian national census, Wolaita and Dawro zones had a projected total population size of 1,838,073 and 592,768 in 2014, respectively. Cumulatively, more than 2.4 million people reside in these zones.18
Sampling technique and sample size
A three stage sampling method was used to choose study participants. First, six districts were randomly selected out of the 17 rural districts of the two zones. Based on their population size (as elaborated under study area), proportional allocation of sample size was employed in order to assure representativeness. Hence, four districts were selected from Wolaita zone and two districts were selected from Dawro zone. At the second stage, two kebeles were randomly selected from each district through a computer generated technique using Microsoft Office Excel software. Lastly, based on proportional allocation of sample size to each district, study subjects were selected through systematic sampling technique after obtaining a sampling frame from their respective kebeles (health extension workers).
The total sample size needed for this study was calculated by using Epi-Info version 7: considering 95% confidence interval (CI) with 5% precision, 74.4% of women who had decision making autonomy concerning their own health care needs,17 10% non-response rate, and design effect of three, the total number of selected households were 967.
Data collection instruments and tools
A face-to-face interview was used to collect data from study participants. The questionnaire included socio-demographic variables of women and their husbands, variables of household wealth index measurements, knowledge, attitude, and practice of study participants toward maternal health service utilization, and decision making status of women. Household wealth index was measured by asking study participants about the presence or absence of household assets, utilities, and housing characteristics used to yield household wealth index in the Ethiopian Demographic and Health Survey.17 Women’ autonomy in health care decision making was assessed by asking women about who makes decisions concerning their own health care. Accordingly, their responses were classified in any of the following four choices: “mainly wife”; “wife and husband jointly”; “mainly husband”; or “someone else”. As a result, a woman was considered to be autonomous in health care decision making if she usually makes that decision alone or jointly with her husband.17
Data management and analysis
Data were entered using Epi-data version 1.4.4.0 and exported to SPSS version 20 for analysis. Household wealth index was analyzed by principal component analysis. Descriptive statistics were used to describe the study population by using proportions, means, and standard deviation. Bivariate logistic regression was used to identify candidate variables of maternal autonomy in health care decision making. The important predictors of health care decision making autonomy were determined using multivariable logistic regression. Odds ratios (ORs) along with CIs were used to determine the association between predictor variables and health care decision making autonomy of study subjects, considering significant association at alpha <0.05.
Quality control
Two-day intensive training was given to data collectors to ensure they had a common understanding of research work. A pre-test was done prior to actual research work among 5% of the total sample size. The questionnaire was adapted from demographic and health survey questionnaires and other similar study settings and guidelines. Daily supervision ensured the quality of data collection.
Ethical approval and consent to participate
The research activity commenced after Wolaita Sodo University ethics approval committee approved the study. Permission to conduct the study was received from the respective district health offices: 1) Damot Gale, 2) Boloso Sore, 3) Humbo, 4) Ofa, 5) Tocha, and 6) Mareka, and verbal consent was obtained from participants. Study participants were requested to give their consent after the objectives and benefits of the study were explained to them; as well as their right to participate or not. Furthermore, study participants were also informed about the confidentiality of their response.
Results
Socio-demographic characteristics of study participants
Out of 967 women, only ten women were excluded from the study due to their incomplete questionnaire data, resulting in 99% response rate. The age of all the study participants when they first got married was less than or equal to 30 years. However, the majority (83.4%) of them got married during their adolescence. The minimum and maximum age at marriage was 14 and 30 years respectively, with mean and standard deviation of 18.7 and 2.5 years, respectively. The majority was married at the time of the survey (96%), of protestant religion (74.4%), and from Wolaita ethnic group (70.5%). Less than one third (32.3%) of the households had a family size of less than five individuals/household, while 37.2% and 30.5% of them had a family size of 5–6 and more than six individuals/household, respectively (Table 1).
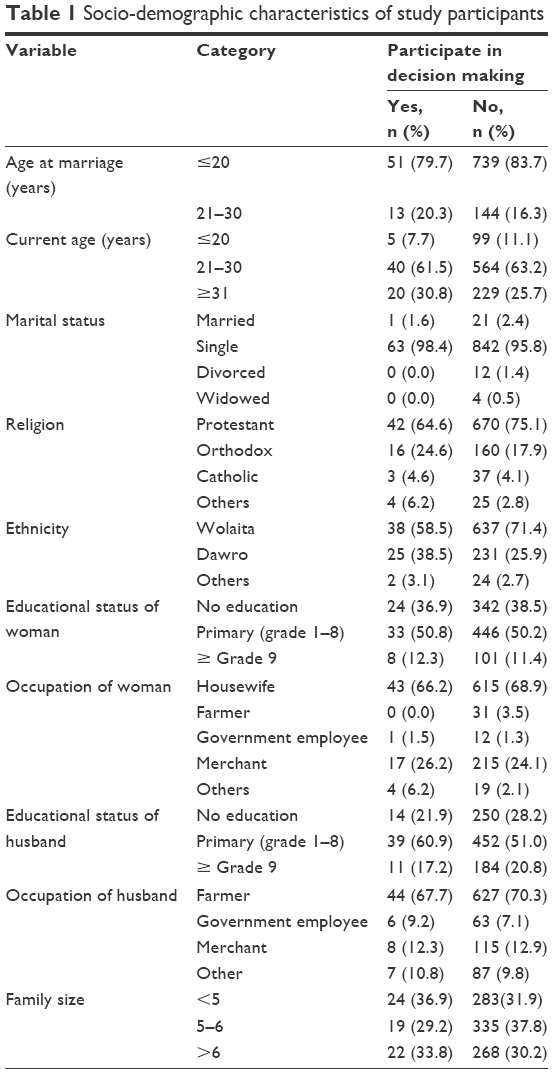 | Table 1 Socio-demographic characteristics of study participants |
Knowledge, attitude, and practice of study participants toward maternal health service utilization
The last pregnancy was unplanned among 29.5% of study participants. However, the majority (73.8%) accomplished the four World Health Organization recommended focused antenatal care visits. Besides, the majority (85.1%) of study participants had a favorable attitude toward skilled birth attendance. Nevertheless, only 37.5% of them gave birth to their last child at a health facility. Similarly, 86.5% of study participants had a favorable attitude toward postnatal care follow-up. However, only 23% had actually visited a health care facility for their postnatal care (Table 2).
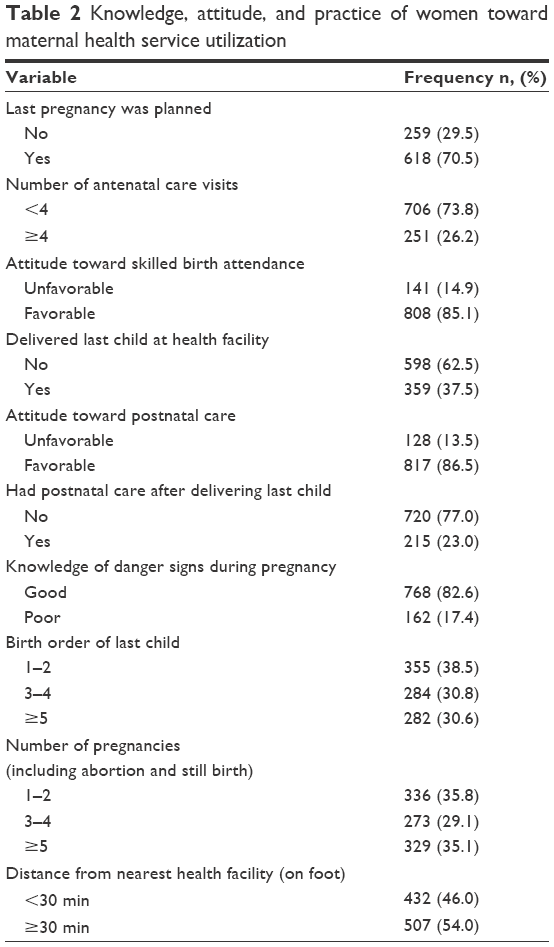 | Table 2 Knowledge, attitude, and practice of women toward maternal health service utilization |
Regarding knowledge of danger signs during pregnancy, the majority (82.6%) of study participants knew at least one danger sign. The most commonly known danger signs were bleeding, followed by severe headache and severe fatigue; while most of them did not know that convulsions, loss of consciousness, and difficulty breathing were danger signs during pregnancy. More than one third (35.1%) of women had experienced at least five pregnancies, whereas 29.1% had experienced three to four pregnancies (Table 2).
Health care decision making autonomy of women
Concerning women’ decision making autonomy with regards to their own health care, 20.6% of them usually made decisions themselves, whereas 37.8% made decisions jointly with their husbands. However, health care decisions of women are made by their husbands/partners among 40.9% of study participants. Overall, a woman was considered to participate in decision making if she usually makes that decision alone or jointly with her husband/partner. As a result, 58.4% of women had health care decision making autonomy either alone or jointly.
Factors associated with health care decision making autonomy of women
Bivariate logistic regression has revealed that woman’s and husband’s educational status, household wealth index, birth order, number of pregnancies, current age of woman, family size, husband’s and woman’s occupation are significantly associated with health care decision making autonomy (Table 3).
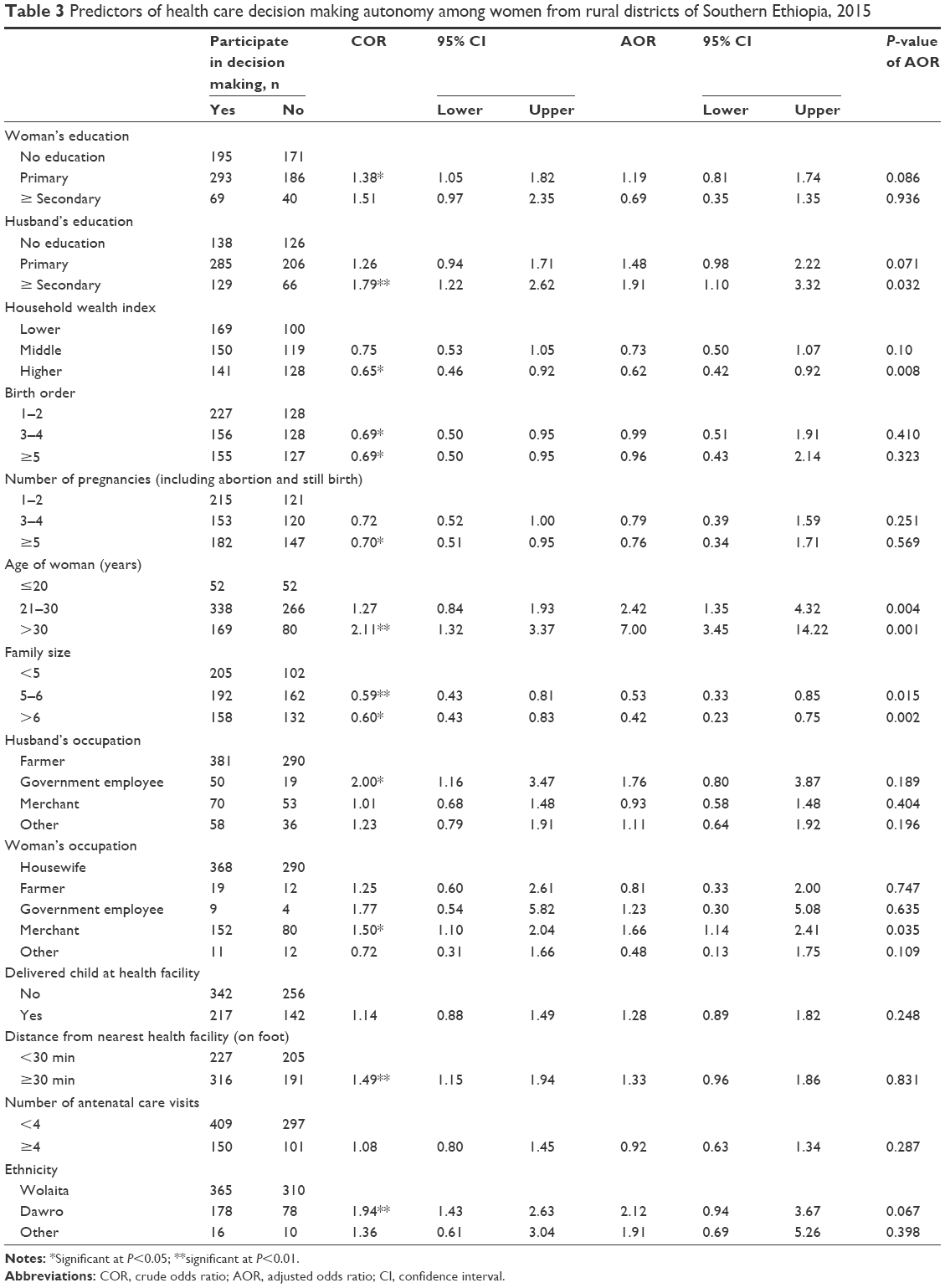 | Table 3 Predictors of health care decision making autonomy among women from rural districts of Southern Ethiopia, 2015 |
After controlling for confounding using backward stepwise multivariable logistic regression analysis, husband’s education, household wealth index, current age of woman, family size, and woman’s occupation were identified as independent predictors of woman’s health care decision making autonomy (Table 3).
Women whose husband’s educational status is secondary and above, are twice as likely to participate in health care decision making compared to women whose husbands have no formal education; adjusted odds ratio (AOR) =1.91 (95% CI: 1.10, 3.32). Women from higher wealth index households have a 38% lower chance of participating in decision making than those from lower wealth index households, AOR =0.62 (95% CI: 0.42, 0.92). Women’ participation in health care decision making increases with increase in age. Accordingly, women found in the age category of 21–30 years are twice as likely to participate in decision making compared to those aged below 20 years; AOR =2.42 (95% CI: 1.35, 4.32). Similarly, women aged 30 years and above are seven times more likely to participate in decision making compared to those aged below 20 years; AOR =7 (95% CI: 3.45, 14.22) (Table 3).
As family size increases, the probability of the woman participating in health care decision making decreases. In this study, women with a family size of five to six persons have a 47% lower chance of participating in health care decision making as compared to women with a family size of less than five persons; AOR =0.53 (95% CI: 0.33, 0.85). Similarly, women with a family size of six persons and above have a 58% lower chance of participating in decision making; AOR =0.42 (95% CI: 0.23, 0.75). Participation in income generating activities also has a positive association with women’s decision making autonomy. Accordingly, working women are more likely than housewives to participate in health care decision making; AOR =1.66 (95% CI: 1.14, 2.41) (Table 3).
Discussion
Women’s autonomy is likely to vary according to characteristics at the individual, interpersonal, community, and macro political and societal level. The present study assessed women’s health care decision making autonomy and associated factors among women living in rural districts of Southern Ethiopia. Accordingly, 58.4% of study participants have autonomy in making health care decisions either alone or jointly. This finding is lower than that of a study conducted in Dabat, Northern Ethiopia, and of an Ethiopian demographic and health survey in which 66.7% and 74.4% of study participants had autonomy in making health care decisions either alone or jointly with their husbands, respectively.17,19 This difference might be the result of discrepancy in the scope of studies, where the current study only involved rural women while the former studies incorporated both rural and urban women. It is known that urban women have relatively better education, economy, and information. Hence, the current study found a relatively lower rate of health care decision making autonomy than the aforementioned studies.
This study identified important factors which are associated with women’ health care decision making autonomy. After controlling for confounding using backward stepwise multivariable logistic regression analysis; husband’s education, household wealth index, current age of woman, family size, and woman’s occupation were identified as independent predictors of maternal health care decision making autonomy.
Women whose husbands are educated above secondary level, were twice as likely to participate in health care decision making compared to women whose husbands have no formal education; AOR =1.91 (95% CI: 1.10, 3.32). This might be due to the fact that the more a husband is educated, the more he will accept gender equality and believe in equal participation in decision making. However, unlike other studies, this study did not show a significant association between maternal educational status and decision making autonomy. This could be due to the presence of very few educated women in the study as the majority (88.6%) of them had an educational status below secondary education.
Ownership and control of property is one of the most important contributors to the gap created by gender role in the community with regard to health care seeking behavior, economic well-being, social status, and women empowerment.20 Household economic status has emerged as a significant factor for women’s involvement in health care decision making. This study found that women from higher household wealth quantiles had a 38% lower chance of participating in decision making than those from a lower wealth quantile; AOR =0.62 (95% CI: 0.42, 0.92). This indicates that as the household gets richer, they are less likely to take part in decision making. This finding is supported by a study from Nepal.21 Besides, results of a study conducted by Bernasek and Bajtelsmit show that wealthier households show significantly less female involvement in financial decision making.22 The negative influence of higher household economy on health care decision making autonomy of women could be the consequence of less involvement of women in household assets as a result of limited participation in household income. In the current study 68.8% of study participants are housewives who are not participating in income generating activities, which in turn can be the cause of women’s dependency on their husbands’ income, hence their autonomy is handicapped.
Women’ participation in health care decision making increases with increase in age. This study has also revealed that women in the age category of 21–30 years were twice as likely to participate in decision making compared to those aged below 20 years; AOR =2.42 (95% CI: 1.35, 4.32). Similarly, women aged 30 years and above were seven times more likely to participate in decision making than those aged below 20 years; AOR =7 (95% CI: 3.45,14.22). This finding is in line with a study from the Philippines which reported that the percentage of women who usually participate in decision making increases with age.23 It is also supported by a study conducted among migrant weavers in Addis Ababa, Ethiopia which found younger women and middle-aged women to be less likely to participate in reproductive health decision making compared to older women.24
As family size increases, the probability of the woman participating in health care decision making decreases. In this study women with a family size of five to six persons/household had a 47% lower chance of participating in health care decision making as compared to women with a family size of less than five persons/household; AOR =0.53 (95% CI: 0.33, 0.85). Similarly, women with a family size of six persons/household and above had a 58% lower chance of participating in health care decision making; AOR =0.42 (95% CI: 0.23, 0.75). This finding is supported by a study conducted by Delbiso in which having fewer children was associated with better reproductive health decision making.24 In addition, women who have less than three children have greater control over their reproductive health than women who have three or more children.25 As a result, having a smaller family would help women exercise freedom of health care decision making, and end male dominance in a family.
Women’ independence in generating income also has a positive association with their decision making autonomy. Accordingly, working women were twice as likely to participate in health care decision making than housewives; AOR =1.66 (95% CI: 1.14, 2.41). This finding is consistent with a study from Addis Ababa, Ethiopia, in which working women (women generating their own income) were more likely to participate in contraceptive use decision making than non-working women.24 Besides, participating in income generating activities increases women’s economic independence and challenges the traditional belief of male dominance in decision making, and hence improves spousal communication in household decision making.26
Conclusion and recommendation
Women’s autonomy in health care decision making is essential in a range of situations, from health care seeking and utilization to choosing among treatment options. Since empowering women is crucial for the achievement of sustainable development, full participation of couples is required in health care decision making.
Even though every woman has the right to participate in making decisions about her own health care, more than two fifths of study participants have no role in making health care decisions about their own health. Husbands/partners play a major role in making health care decisions about their wives. The majority of women with the highest health care decision making autonomy in Wolaita and Dawro zones also have significantly higher odds of having literate husbands, lower wealth index, older age, small family size, and employment.
Even if a household has adequate resources, a woman’s limited participation in household decision making can lead to low uptake of maternal health services. This study revealed that a woman’s health care decision making autonomy is broadly influenced by her age, husband’s literacy, household economy, family size, and her involvement in income generating activities.
A comprehensive strategy needs to be implemented in order to empower women to access and utilize health care services, as well as to challenge the traditional male dominance in household decision making. Reducing women’s dependency on their husbands/partners and family through education and employment will have a positive impact on improving women’s autonomy in health care decision making. One effective way to do so is to provide non-formal and formal education to both women and their husbands/partners. Even though the Ethiopian policy and school curricula are supportive of gender equality and female empowerment, due attention needs to be given to women living in remote and rural areas whose dependency is higher than their counterparts. Involving women in income generating activities is another aspect of female empowerment. Family planning utilization can also have a positive impact on decision making autonomy of women, since it helps to limit the family size, which in turn allows freedom and independency of women with regard to health care decision making.
Funding
This research was funded by Wolaita Sodo University.
Acknowledgments
Wolaita Sodo University, respective zonal and district administrative offices, data clerks, collectors, and study participants deserve our special thanks.
Author contributions
MA conceived the study, participated in the design of the study, and performed statistical analysis; MA and MM obtained ethical clearance and permission to conduct the study, supervised data collection, interpreted the data, and wrote the article. Both authors read and approved the final manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
Dyson T, Moore M. On kinship structure, female autonomy, and demographic behavior in India. Population and Development Review. 1983;9(1):35–60. | ||
Woldemicael G, Tenkorang EY. Women’s autonomy and maternal health-seeking behavior in Ethiopia. Matern Child Health J. 2010;14(6):988–998. | ||
International Conference on Population and Development 1994. Available from: http://www.unfpa.org/events/international-conference-population-and-development-icpd. Accessed April 10, 2017. | ||
un.org [homepage on the Internet]. United Nations International Conference on Population and Development Programme of Action; 1994. Available from: http://www.un.org/popin/icpd/conference/offeng/poa.html. Accessed April 4, 2017. | ||
Bloom SS, Wypij D, Das Gupta M. Dimensions of women’s autonomy and its influence on maternal health care utilization in north Indian city. Demography. 2001;38(1):67–78. | ||
Hindin M. Women’s autonomy, status, and nutrition in Zimbabwe, Zambia, and Malawi. In: Kishor S, editor. A Focus on Gender: Collected Papers on Gender using DHS Data. Calverton, MD: ORC Macro; 2005; 93–116. | ||
Kishor S. Empowerment of women in Egypt and links to the survival and health of their infants. In: Presser H, Sen G, editors. Women’s empowerment and demographic processes: Moving beyond Cairo. New York: Oxford University Press; 2000;118–158. | ||
Anderson S, Eswaran M. What determines female autonomy? Evidence from Bangladesh. J Dev Econ. 2009;90(2):179–191. | ||
Power in sexual relationships: an opening dialogue among reproductive health professionals; 2001. Available from: http://www.eldis.org/go/home&id=16288&type=Document#.WOsll_lTLcd. Accessed April 10, 2017. | ||
Asian development bank to promote greater empowerment for Nepal’s most disadvantaged women 2004. Available from: https://nrb.org.np/red/publications/special_publication/Special_Publications--ADB%20%20Nepal_(2004).pdf. Accessed April 10, 2017. | ||
Morgan SP, Niraula BB. Gender inequality and fertility in two Nepali villages. Popul Dev Rev. 1995;21(3):541–561. | ||
Sathar ZA, Kazi S. Women’s autonomy in the context of rural Pakistan. The Pakistan Development Review. 2000;39:89–110. | ||
Jin H. A study of rural women’s decision-making power on reproduction and fertility. Chin J Popul Sci. 1995;7(3):241–257. | ||
Fever and its treatment among the more and less poor in Sub-Saharan Africa 2002. Available from: http://dx.doi.org/10.1596/1813-9450-2798. Accessed April 10, 2017. | ||
Becker S, Fonseca-Becker F, Schenck-Yglesias C. Husbands’ and wives’ reports of women’s decision-making power in Western Guatemala and their effects on preventive health behaviours. Soc Sci Med. 2006;62(9):2313–2326. | ||
Makinwa P, Jensen A, editors. Women’s position and Demographic Change in sub-Saharan Africa. Liege, Belgique: IUSSP; 1995. | ||
Central Statistical Agency [Ethiopia] and ICF International. Ethiopia Demographic and Health Survey 2011. Addis Ababa EaC, Maryland, USA: Central Statistical Agency and ICF International; 2012. Available from: https://dhsprogram.com/pubs/pdf/FR255/FR255.pdf. Accessed June 15, 2016. | ||
Summary and statistical report of the 2007 population and housing census, Federal democratic republic of Ethiopia, 2008. Available from: https://www.google.com/url?sa=t&rct=j&q=&esrc=s&source=web&cd=1&cad=rja&uact=8&ved=0ahUKEwiQzfb4o5nTAhWHuhoKHRWGCnUQFggeMAA&url=http%3A%2F%2Funstats.un.org%2Funsd%2Fcensuskb20%2FAttachment489.aspx%3FAttachmentType%3D1&usg=AFQjCNHp0T0P5np7cnArJhEHOovwk50JQQ&sig2=CQM5nNcIgsvDSce4tvhQfw. Accessed June 15, 2016. | ||
Mekonnen A, Asrese K. Household decision making status of women in dabat district, north west Ethiopia, 2009 Gc. Science Journal of Public Health. 2014;2(2):111–118. | ||
Agarwal B. Gender and command over property: a critical gap in economic analysis and policy in South Asia. World Development. 1994;22(10):1455–1478. | ||
Acharya DR, Bell JS, Simkhada P, van Teijlingen ER, Regmi PR. Women’s autonomy in household decision-making: a demographic study in Nepal. Reprod Health. 2010;7:15. | ||
Bernasek A, Bajtelsmit V. Predictors of women’s involvement in household financial decision-making. Journal of Financial Counseling and Planning. 2002;13(2):39–48. | ||
Measuring women’s empowerment and women’s autonomy in the Philippines. Available from: https://unstats.un.org/unsd/gender/Mexico_Nov2014/HighLevelPanel%20Philippines.pdf. Accessed April 10, 2017. | ||
Delbiso TD. Gender power relations in reproductive decision-making: The case of migrant weavers of Addis Ababa, Ethiopia. Journal of Science & Development. 2014;2(1):59–71. | ||
Irwanto PH, Sunarno N, Poerwandari EK, Hardee K, Eggleston E, Hull T. In the shadow of men: reproductive decision making and women’s psychological well-being in Indonesia. 1997. Available from: http://pdf.usaid.gov/pdf_docs/Pnacc567.pdf. Accessed April 10, 2017. | ||
Chapagain M. Conjugal power relations and couples’ participation in reproductive health decision-making: Exploring the link in Nepal. Gender, Technology and Development. 2006;10(2):159–189. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.