")
Back to Journals » OncoTargets and Therapy » Volume 9
Haploidentical hematopoietic stem cell transplantation without total body irradiation for pediatric acute leukemia: a single-center experience
Authors Mu Y, Qin M, Wang B, Li S, Zhu G, Zhou X, Yang J, Wang K, Lin W, Zheng H
Received 11 December 2015
Accepted for publication 14 February 2016
Published 2 May 2016 Volume 2016:9 Pages 2557—2563
DOI https://doi.org/10.2147/OTT.S102286
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Min Li
Yanshun Mu,* Maoquan Qin,* Bin Wang, Sidan Li, Guanghua Zhu, Xuan Zhou, Jun Yang, Kai Wang, Wei Lin, Huyong Zheng
Beijing Key Laboratory of Pediatric Hematology Oncology, National Key Discipline of Pediatrics, Ministry of Education, Key Laboratory of Major Diseases in Children, Ministry of Education, Hematology Oncology Center, Beijing Children’s Hospital, Capital Medical University, Beijing, People’s Republic of China
*These authors contributed equally to this work
Abstract: Hematopoietic stem cell transplantation (HSCT) is a promising method for therapy of pediatric patients with acute leukemia. However, less availability of matched donors limited its wide application. Recently, haploidentical HSCT has become a great resource. Here, we have retrospectively reported our experience of 20 pediatric patients with acute leukemia who underwent haploidentical HSCT without total body irradiation (TBI) myeloablative regimen in our center from November 2007 to June 2014. All the patients attained successful HSCT engraftment in terms of myeloid and platelet recovery. Thirteen patients developed grade I–IV acute graft-versus-host disease (a-GVHD). The incidence of grade I–II a-GVHD, grade III–IV a-GVHD, and chronic GVHD (c-GVHD) was 45%, 20%, and 25%, respectively. The mean myeloid and platelet recovery time was 13.20±2.41 and 19.10±8.37 days. The median follow-up time was 43.95±29.26 months. During the follow-up, three patients died. The overall survival (OS) rate was 85%. The present study indicated that haploidentical HSCT without TBI myeloablative regimen significantly improved the OS rate of pediatric patients with acute leukemia.
Keywords: haploidentical, hematopoietic stem cell transplantation, myeloablative regimen, total body irradiation, acute leukemia, pediatric
Introduction
Acute leukemia (AL) is the most common malignancy in children. With the improvement in chemotherapy and risk stratification, children younger than 6 years show significantly better event-free survival – 83.7% in acute lymphoblastic leukemia1 and 54% in acute myeloid leukemia.2 The AL outcome has greatly improved in childhood in the past few decades. However, 15%–20% of the patients relapse, which is the most formidable challenge in leukemia treatment.3 Therefore, effective treatment strategies are imperative. Hematopoietic stem cell transplantation (HSCT) has been demonstrated to be safe and efficacious in children with AL.4 Transplantation from a human leukocyte antigen (HLA)-matched sibling is the ideal treatment for children with AL. However, the chance of availability of a matched donor is less than 25%.5 The availability of haploidentical donor has considerably widened the donor pool and many patients were assigned to haploidentical HSCT (haplo-HSCT).6,7 This method is now successfully utilized with myeloablative (MA) preparative regimen to achieve long-term survival compared to HLA-matched transplantation. Future directions will focus on optimizing conditioning regimens and enhancing graft-versus-leukemia effect. Limited data are available pertaining to haplo-HSCT without total body irradiation (TBI) regimens, particularly in the pediatric population. The aim of this single-center study was to review haplo-HSCT without TBI MA regimen for children with AL in our hospital.
Materials and methods
Patients
This retrospective study involved a total of 20 pediatric AL patients (13 males and seven females) who underwent haplo-HSCT between November 2007 and June 2014 in Beijing Children’s Hospital. The patients were selected for our study according to our Children’s Transplantation protocol, which was approved by the Health Department of Beijing City (Table 1). Patients with severe infection, organ failure, and sepsis were excluded. Twenty pediatric patients with a median age of 7.45±3.61 years (range: 1–14 years) and a median weight of 28.32±12.36 kg (range: 9.5–50 kg) were enrolled. This study was approved by the ethics and technological committees of the Beijing Children’s Hospital. The patients and donors provided written informed consent for the protocol. None of the patients found an HLA-matched sibling or unrelated donors. Acute graft-versus-host disease (a-GVHD) was graded from I to IV. Chronic GVHD (c-GVHD) was defined as present or absent.
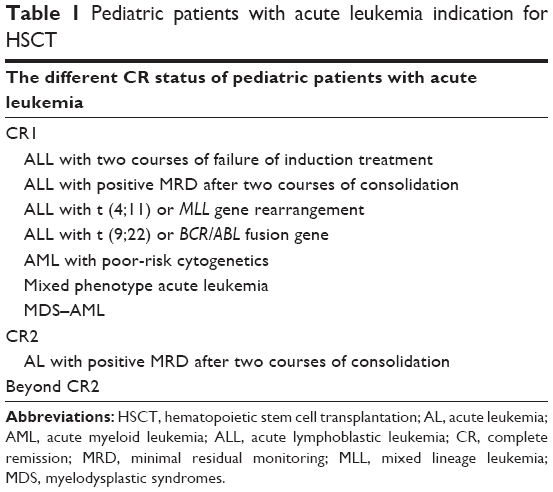 | Table 1 Pediatric patients with acute leukemia indication for HSCT |
HLA typing and donors
All family members were tested for the degree of HLA match. HLA-A and HLA-B typing were performed by intermediate resolution techniques, while HLA-C typing were performed using high-resolution techniques. HLA typing was strictly analyzed for the donor and recipient. The donors were searched on the basis of best HLA match, killer immunoglobulin-like receptors genotype, and health status.8–10 We adopted granulocyte-colony stimulating factor (G-CSF)-mobilized bone marrow (BM) and peripheral blood stem cells (PBSCs) in haploidentical transplantation from family donors without in vitro T-cell depletion. The procedure was well tolerated by all donors, without any severe side effects. The father served as the donor for six of the patients, the mother for seven, the brother for one, and the sister for six.
Conditioning regimens
In the haplo-HSCT, 14 patients underwent a preconditioning regimen intravenously with fludarabine (25 mg/m2/day, on days −14, −13, −12, −11, and −10), busulfan (Bu) (0.8–1 mg/kg four times per day, on days −9, −8, −7, and −6), and cyclophosphamide (Cy) (50 mg/kg/day on days −5, −4, −3, and −2). Five patients underwent intravenous preconditioning regimen with Bu (0.8–1 mg/kg four times per day, on days −8, −7, and −6), cytosine arabinoside (Ara-C) (4 g/m2/day, on days −10 and −9), Cy (50 mg/kg/day, on days −5 and −4), and oral semustine (MeCCNU) (250 mg/m2/day, on day −3). One patient underwent preconditioning regimen with intravenous Bu (0.8–1 mg/kg four times per day, on days −9, −8, −7, and −6) and intravenous Cy (50 mg/kg/day, on days −5, −4, −3, and −2). All patients were not treated by TBI before BM transplantation. The conditioning regimens of leukemia patients are summarized in Table 2.
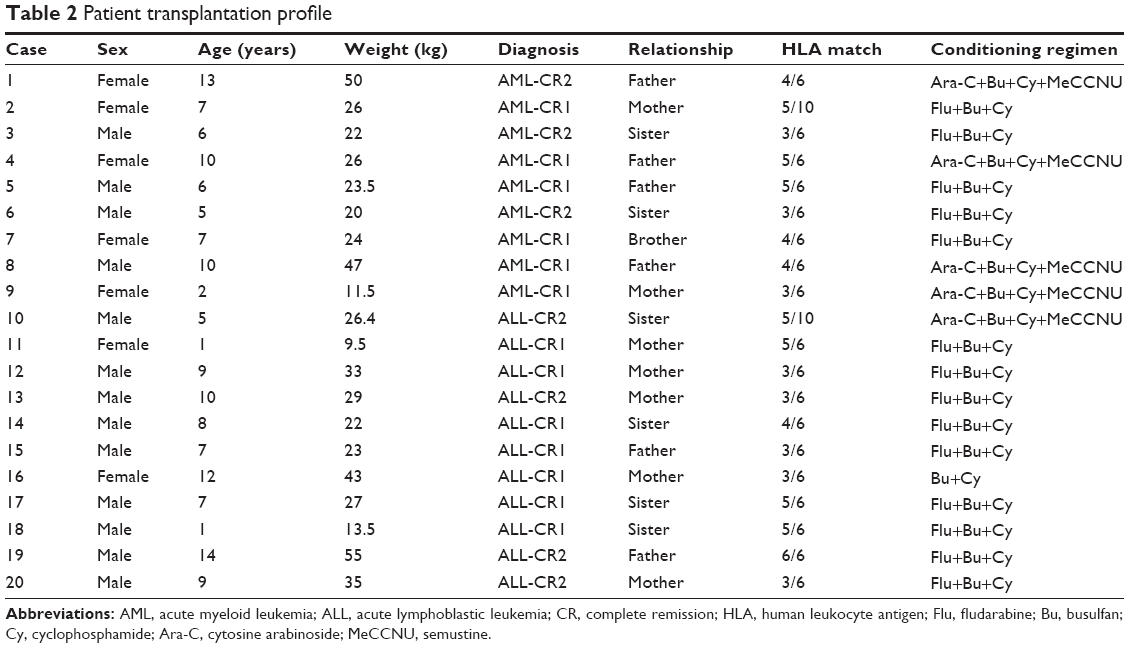 | Table 2 Patient transplantation profile |
Collection of hematopoietic stem cells
The donors were primed with G-CSF injected subcutaneously at a dose of 5 μg/kg/day for 5 consecutive days. On the sixth day, BM cells and PBSCs were harvested. The target mononuclear cell count was above 3×108 cells/kg of the recipient’s weight. PBSCs were collected using a blood cell separator (COBE Spectra LRS, Ceridian BCT, Inc., Lakewood, CO, USA) from a total blood volume of 150–200 mL/kg. In case of ABO major blood group compatibility, fresh and unmanipulated BM and PBSCs were immediately infused into the recipient after collection. However, in case of ABO major blood group incompatibility, the red cells were removed from the stem cells by density gradient sedimentation with Hespan according to the manufacturer’s instructions (B. Braun Medical Inc., Irvine, CA, USA). The surface markers of the graft cells were determined with monoclonal antibodies specific for CD34 using flow cytometry.
Graft-versus-host disease prophylaxis
Eleven patients were treated with cyclosporine A (CsA) plus methotrexate (MTX) together with anti-human thymocyte globulin (ATG; Lymphoglobuline; Genzyme Imtix-SangStat, Lyon, France) and mycophenolate mofetil (MMF) to prevent the occurrence of GVHD. Four patients were treated with CsA plus MTX and ATG. Three patients were treated with CsA plus MTX and anti-lymphocyte immunoglobulin (ALG). One patient was treated with CsA plus MTX and one with CsA plus ALG. CsA at a daily dose of 2.5 mg/kg was injected intravenously twice a day from day 10 before transplantation and administered orally until the recovery of digestion function. The whole blood CsA concentration level was monitored twice a week using fluorescence polarization immunoassay, and the dosage was maintained at 150–250 ng/mL. In the absence of the evidence of GVHD after 100 days, the CsA dosage was gradually reduced and discontinued at ~180 days. If GVHD was observed, then CsA was continued. MTX was injected intravenously at a dose of 15 mg/m2 on day 1 and at a dose of 10 mg/m2 on days 3, 6, and 11 after transplantation. ATG (Genzyme Imtix-SangStat) was injected intravenously at a daily dose of 3.5 mg/kg/day, from days −6, −5, −4, −3, and −2 before transplantation. ALG (Lymphoglobuline; Genzyme Imtix-SangStat) was injected intravenously at a daily dose of 30 mg/kg/day, from pre-transplantation days −6, −5, −4, −3, and −2. MMF was orally administered at a daily dose of 0.25 g twice a day, from day 0 before transplantation, and was subsequently reduced from day 30 after transplantation. If GVHD failed to occur, the administration of MMF was terminated 90 days post-transplantation. The onset and grades of a-GVHD and c-GVHD were assessed according to published consensus criteria.11,12 The characteristics of the pediatric leukemia patients after haplo-HSCT are shown in Table 3.
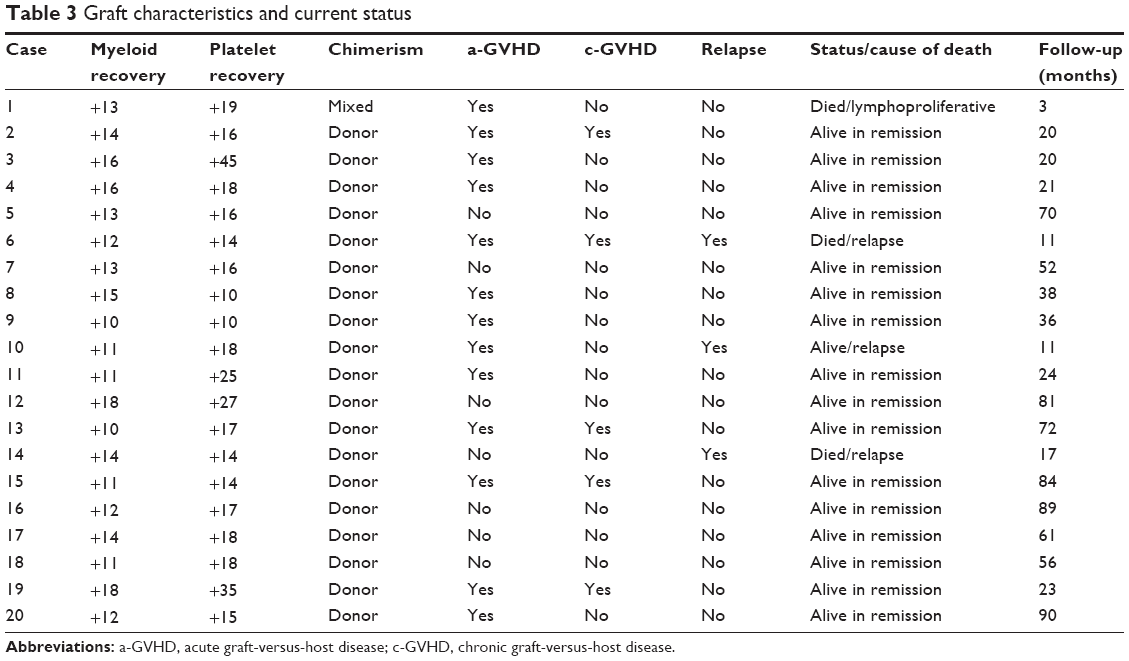 | Table 3 Graft characteristics and current status |
Evaluation of engraftment and chimeras
Hematopoietic stem cell engraftment was defined as an absolute peripheral myeloid count ≥0.5×109/L for 3 consecutive days. Platelet recovery was defined as a platelet count ≥20×109/L without transfusion support for 7 consecutive days.7 Hematopoietic chimeras were identified by HLA typing, blood type analysis, or sex chromosome determination. The chimeras were assessed by short tandem repeat polymerase chain reaction (STR-PCR). Immune reconstruction was evaluated by observation of the lymphocyte subsets at 3, 6, 12, and 18 months after transplantation.
Supportive care
All patients were nursed in separate rooms with laminar air flow until hematopoietic stem cell engraftment. Oral antibiotics including sulfamethoxazole and voriconazole were administered for infections with Pneumocystis and fungal infections. Intestinal prophylaxis drugs were orally administered along with systemic aseptic treatment. Acyclovir was administered as prophylaxis from day 0 for 10 days. Intravenous human immunoglobulin at a dosage of 400 mg/kg was infused once per week from transplantation +2 day until hematopoietic recovery. Hepatic veno-occlusive disease was prevented with low-molecular-weight heparin calcium. G-CSF at a dosage of 5 μg/kg/day was administered from post-transplantation day 5 until myeloid engraftment. Patients were monitored twice weekly for cytomegalovirus (CMV) antigenemia with real-time quantitative polymerase chain reaction. Patients with CMV viremia received therapy with foscarnet sodium at a daily dose of 100–160 mg/kg until CMV was eradicated. Epstein–Barr virus (EBV) pathogenesis was monitored twice weekly with real-time quantitative polymerase chain reaction. Ganciclovir was administered if EBV viremia was persistently positive with any of the symptoms, such as fever or enlargement of the lymph nodes. Minimal residual disease was evaluated by fluorescence in situ hybridization and flow cytometry. All the blood products were irradiated before infusion.
Statistical analysis
The day of the stem cell transfusion was counted as day 0, and all the intervals were calculated based on this date. Descriptive statistics were provided for baseline patient characteristics. Retrospective measures of the cumulative incidence, such as a-GVHD, c-GVHD, and transplantation-related mortality, were used to evaluate the outcome. The probabilities of overall survival (OS) were estimated by Kaplan–Meier method. All statistical analyses were performed using SPSS 20.0 (SPSS Inc., Chicago, IL, USA).
Results
GVHD and infection
The median follow-up time was 43.95±29.26 months (ranging from 3 to 90 months). Thirteen patients developed grade I–IV a-GVHD, including four cases of grade III–IV a-GVHD. The cumulative incidence of a-GVHD was 65%. The rate of occurrence of grade I–II a-GVHD was 45%, grade III–IV a-GVHD was 20%, and c-GVHD was 25%. The CMV infection rate on days +100 was 55% (11/20).
Hematologic reconstitution and engraftment
All pediatric patients achieved successful hematological recovery after transplantation. The median time to reach a myeloid count ≥0.50×109/L was 13.20±2.41 days and a platelet count ≥20×109/L was 19.10±8.37 days. The grafts contained a median of CD34+ cells of (11.72±8.65) ×106/kg body weight (range: 3.35–39.44×106). The grafts contained a median of total nucleated cells of (17.99±6.06) ×108/kg body weight (range: 7.42–30.1×108). The pediatric leukemia patients’ hematologic reconstitution and engraftment are shown in Table 3.
Relapse and survival
All pediatric patients achieved complete remission before transplantation. Evidence for engraftment 30 days post-transplantation revealed that the hematopoietic stem cells from donors survived well in recipients. Two acute lymphoblastic leukemia and one acute myeloid leukemia patients showed relapse. The relapsed patients were treated with donor lymphocyte infusion and immunosuppressant therapy simultaneously. The Kaplan–Meier curves depicting OS are shown in Figure 1. Three patients died during the follow-up time after transplantation. The OS rate was 85%.
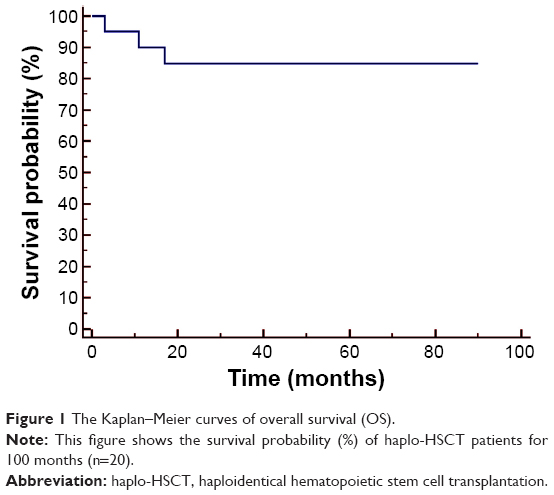 | Figure 1 The Kaplan–Meier curves of overall survival (OS). |
Discussion
Long-term survival is difficult to achieve with conventional chemotherapy for patients with high-risk leukemia.13 HSCT is regarded as the most effective curative therapy for such kinds of patients. An HLA-identical sibling donor, which has optimal 10/10 match (HLA-A, -B, -C, -DRB1, and -DQB1),5,6 is the first choice for HSCT treatment. However, sibling HLA-identical donor has become rare due to birth control in the Chinese population. Therefore, haplo-HSCT has become an option for AL patients without an appropriate HLA-identical or an immediate donor. However, haploidentical transplantation was associated with the high rate of GVHD and non-engraftment.14 A number of strategies have led to improved haplo-HSCT outcomes and decreased complications. The high number of CD34+ cell implants led to faster hematopoietic recovery and reduced incidence of GVHD.15,16 Transplantation of G-CSF-mobilized BM and peripheral blood for hematopoietic recovery and the occurrence of a-GVHD in haplo-HSCT are associated with great benefits.17 The outcome of haplo-HSCT with G-CSF-mobilized PBSCs grafts without T-cell depletion for hematologic diseases is similar to HLA-identical matched donor HSCT.18 Owing to these advantages, we decided to use haploidentical stem cells as a graft source for patients with no suitable HLA-identical sibling or unrelated donor in our center. To achieve great outcome, all donors were administrated with G-CSF and treated with CsA plus MTX, ATG, or ALG. Our results indicated that all the patients obtained successful myeloid and platelet recovery. The mean myeloid and platelet recovery time was 13.20±2.41 and 19.10±8.37 days, respectively. Thirteen patients developed grade I–IV a-GVHD, with a cumulative incidence of 65.0%. The incidence of grade I–II a-GVHD, grade III–IV a-GVHD, and c-GVHD was 45%, 20%, and 25%, respectively. The OS rate was 85%. Haplo-HSCT requires more intensive preparative regimen to overcome the HLA mismatch barrier. MA preparative regimen plays a critical role in facilitating engraftment of full haplotype-mismatched donor hematopoietic stem cell and in preventing relapse. TBI MA preparative regimen eliminates leukemic cells in residual sites such as the central nervous system. Therefore, TBI regimen reduces relapse and transplantation-related mortality. However, the TBI preparative regimen increases transplantation-related toxicity and mortality, which indirectly influences the long-term survival rate of patients undergoing transplantation.19 TBI preparative regimen also is associated with radiation-related adverse effects such as decreased fertility, asymptomatic alterations in pulmonary function, cataracts, diarrhea, and thyroid dysfunction.20–23 The use of TBI preparative regimen in young children is controversial, as children are expected to lead a long life of high quality. Therefore, MA preparative regimens without TBI are expected to minimize the toxicities of irradiation. All the patients who underwent MA preparative regimen without TBI before haplo-HSCT in our center were free from central nervous system complications. Fourteen patients were administered with fludarabine, Bu, and Cy; five patients were treated with TBI plus high-dose Ara-C, MeCCNU, Bu, and Cy as precondition regimen; only one patient was treated with Bu plus Cy; and five patients were treated with high-dose Ara-C, Semustine (MeCCNU), Bu, and Cy as precondition regimen. These protocols greatly reduced the incidence of GVHD with minimal complication. Only one patient had early toxicity and died from lymphoproliferative disease. The CMV infection rate on days +100 was 55% (11/20). Hemorrhagic cystitis was found in two cases and no veno-occlusive disease was observed, which frequently occurred after HSCT. GVHD was the common complication. The GVHD clinical manifestation was relatively low in our study, since MA regimen without TBI reduces the toxicities of irradiation. Further, steroid and other immune inhibitor usage for GVHD treatment also reduced its clinical morbidity. Two patients died of original disease relapse.
To prevent disease relapse, we utilized a few methods for detecting disease. First, we monitored minimal residual disease by PCR method. Second, we treated the Philadelphia chromosome-positive leukemia patients with imatinib to prevent molecular recurrence before and after transplantation. Third, we applied prophylactic donor lymphocyte infusion, which was helpful in decreasing the relapse rates in high-risk AL patients following transplantation.
Conclusion
The present study demonstrated that most pediatric patients with AL can tolerate haplo-HSCT without TBI MA regimen with long-term disease-free survival. This protocol provided a great benefit for leukemia patients without available identical-matched donors.
Acknowledgments
This work was supported by grants from the National Natural Science Foundation of China (No 81300433), Beijing Municipal Natural Science Foundation (No 7144211), Specialized Research Fund for the Doctoral Program of Higher Education (No 20131107120008), BCH Young Investigator Program (BCHYIPA-2013-06), and Beijing Municipal Administration of Hospitals Clinical Medicine Development of Special Funding Support (No ZY201404).
Author contributions
HY Zheng and MQ Qin designed and guided the study. MQ Qin, B Wang, GH Zhu, SD Li, K Wang, W Lin, and X Zhou enrolled patient and collected clinical data. YS Mu and J Yang collected and interpreted data. YS Mu wrote the paper. All authors contributed toward data analysis, drafting and critically revising the paper and agree to be accountable for aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
Gunes AM, Oren H, Baytan B, et al. The long-term results of childhood acute lymphoblastic leukemia at two centers from Turkey: 15 years of experience with the ALL-BFM 95 protocol. Ann Hematol. 2014;93(10):1677–1684. | ||
Creutzig U, Buchner T, Sauerland MC, Zimmermann M, Reinhardt D, Dohner H, Schlenk RF. Significance of age in acute myeloid leukemia patients younger than 30 years: a common analysis of the pediatric trials AML-BFM 93/98 and the adult trials AMLCG 92/99 and AMLSG HD93/98A. Cancer. 2008;112(3):562–571. | ||
Locatelli F, Schrappe M, Bernardo ME, Rutella S. How I treat relapsed childhood acute lymphoblastic leukemia. Blood. 2012;120(14):2807–2816. | ||
Locatelli F, Masetti R, Rondelli R, et al. Outcome of children with high-risk acute myeloid leukemia given autologous or allogeneic hematopoietic cell transplantation in the aieop AML-2002/01 study. Bone Marrow Transplant. 2015;50(2):181–188. | ||
Chen XH, Gao L, Zhang X, et al. HLA-haploidentical blood and bone marrow transplantation with anti-thymocyte globulin: long-term comparison with HLA-identical sibling transplantation. Blood Cells Mol Dis. 2009;43(1):98–104. | ||
Palma J, Salas L, Carrion F, et al. Haploidentical stem cell transplantation for children with high-risk leukemia. Pediatr Blood Cancer. 2012;59(5):895–901. | ||
Liu DH, Xu LP, Liu KY, et al. Long-term outcomes of unmanipulated haploidentical HSCT for paediatric patients with acute leukaemia. Bone Marrow Transplant. 2013;48(12):1519–1524. | ||
Scquizzato E, Zambello R, Teramo A, et al. KIR/HLA-I mismatching and risk of relapse in paediatric patients undergoing non-haploidentical allogeneic haematopoietic stem cell transplantation. Pediatr Transplant. 2011;15(2):198–204. | ||
Kekre N, Antin JH. Hematopoietic stem cell transplantation donor sources in the 21st century: choosing the ideal donor when a perfect match does not exist. Blood. 2014;124(3):334–343. | ||
Shaw BE, Madrigal JA, Potter M. Improving the outcome of unrelated donor stem cell transplantation by molecular matching. Blood Rev. 2001;15(4):167–174. | ||
Filipovich AH, Weisdorf D, Pavletic S, et al. National Institutes of Health consensus development project on criteria for clinical trials in chronic graft-versus-host disease: I. Diagnosis and staging working group report. Biol Blood Marrow Transplant. 2005;11(12):945–956. | ||
Rowlings PA, Przepiorka D, Klein JP, et al. IBMTR Severity Index for grading acute graft-versus-host disease: retrospective comparison with Glucksberg grade. Br J Haematol. 1997;97(4):855–864. | ||
Mrozek K, Marcucci G, Nicolet D, et al. Prognostic significance of the European LeukemiaNet standardized system for reporting cytogenetic and molecular alterations in adults with acute myeloid leukemia. J Clin Oncol. 2012;30(36):4515–4523. | ||
Nagafuji K, Matsuo K, Teshima T, et al. Peripheral blood stem cell versus bone marrow transplantation from HLA-identical sibling donors in patients with leukemia: a propensity score-based comparison from the Japan Society for Hematopoietic Stem Cell Transplantation registry. Int J Hematol. 2010;91(5):855–864. | ||
Chang YJ, Xu LP, Liu DH, et al. Platelet engraftment in patients with hematologic malignancies following unmanipulated haploidentical blood and marrow transplantation: effects of CD34+ cell dose and disease status. Biol Blood Marrow Transplant. 2009;15(5):632–638. | ||
Aversa F, Tabilio A, Velardi A, Martelli MF. Allogeneic transplantation across the HLA barriers. Rev Clin Exp Hematol. 2001;5(2):147–161. | ||
Wang HX, Yan HM, Wang ZD, Xue M, Liu J, Guo ZK. Haploidentical hematopoietic stem cell transplantation in hematologic malignancies with G-CSF mobilized bone marrow plus peripheral blood stem cells grafts without T cell depletion: a single center report of 29 cases. Leuk Lymphoma. 2012;53(4):654–659. | ||
Lu RN, Miao KR, Zhang R, et al. Haploidentical hematopoietic stem cell transplantation following myeloablative conditioning regimens in hematologic diseases with G-CSF-mobilized peripheral blood stem cells grafts without T cell depletion: a single center report of 38 cases. Med Oncol. 2014;31(8):81. | ||
Hamidieh A, Kargar M, Jahani M, et al. The outcome of allogeneic hematopoietic stem cell transplants without total body irradiation in pediatric patients with acute lymphoblastic leukemia: single centre experience. J Pediatr Hematol Oncol. 2012;34(2):101–107. | ||
Fu H, Xu L, Liu D, et al. Total body irradiation and cyclophosphamide plus antithymocyte globulin regimen is well tolerated and promotes stable engraftment as a preparative regimen before T cell-replete haploidentical transplantation for acute leukemia. Biol Blood Marrow Transplant. 2014;20(8):1176–1182. | ||
Bunin N, Aplenc R, Kamani N, Shaw K, Cnaan A, Simms S. Randomized trial of busulfan vs total body irradiation containing conditioning regimens for children with acute lymphoblastic leukemia: a Pediatric Blood and Marrow Transplant Consortium study. Bone Marrow Transplant. 2003;32(6):543–548. | ||
Ferry C, Socie G. Busulfan-cyclophosphamide versus total body irradiation – cyclophosphamide as preparative regimen before allogeneic hematopoietic stem cell transplantation for acute myeloid leukemia: what have we learned? Exp Hematol. 2003;31(12):1182–1186. | ||
Thomas O, Mahe M, Campion L, et al. Long-term complications of total body irradiation in adults. Int J Radiat Oncol Biol Phys. 2001;49(1):125–131. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.