")
Back to Journals » Clinical Interventions in Aging » Volume 17
Handgrip Strength as a Predictor of Successful Rehabilitation After Hip Fracture in Patients 65 Years of Age and Above
Authors Milman R, Zikrin E, Shacham D, Freud T, Press Y
Received 12 May 2022
Accepted for publication 28 July 2022
Published 31 August 2022 Volume 2022:17 Pages 1307—1317
DOI https://doi.org/10.2147/CIA.S374366
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Nandu Goswami
Rivka Milman,1 Evgeniya Zikrin,2,3 David Shacham,2,3 Tamar Freud,4 Yan Press2– 6
1Department of Family Medicine, Faculty of Health Sciences, Ben-Gurion University of the Negev, Beer- Sheva, Israel; 2Faculty of Health Sciences, Ben-Gurion University of the Negev, Beer- Sheva, Israel; 3Department of Geriatrics, Soroka Medical Center, Beer-Sheva, Israel; 4Siaal Research Center for Family Medicine and Primary Care, Faculty of Health Sciences, Ben-Gurion University of the Negev, Beer- Sheva, Israel; 5Unit for Community Geriatrics, Division of Health in the Community, Ben-Gurion University of the Negev, Beer-Sheva, Israel; 6Center for Multidisciplinary Research in Aging, Ben-Gurion University of the Negev, Beer-Sheva, Israel
Correspondence: Yan Press, Unit for Community Geriatrics, Division of Health in the Community, Ben-Gurion University of the Negev, Beer-Sheva, Israel, Tel +972-8-6477433 ; +972-50-6263903, Fax +972-8-6407795, Email [email protected]
Purpose: It is important to identify factors associated with the outcome of rehabilitation after hip fracture as an aid to planning the rehabilitation framework and the future discharge of patients. Previous studies have shown that handgrip strength (HGS) is one of the factors associated with the success of rehabilitation.
Materials and Methods: A retrospective study among patients 65 years of age and above who underwent surgical repair of a hip fracture followed by rehabilitation in the Geriatrics ward between September 2019 and December 2021. Successful rehabilitation was determined as Montebello Rehabilitation Factor Score Revised (MRFS-R) ≥ 50%. Associations were assessed between various sociodemographic and clinical variables, including HGS, and rehabilitation success. HGS was tested as a continuous and dichotomous variable, in accordance with various definitions of low muscle strength.
Results: Data were collected for 173 patients. The mean age was 81.2 ± 7.2 years and 68.2% were women. In a logistic regression model only HGS, as a continuous variable, was independently associated with rehabilitation success, with each increase of 1 kg increasing the chance for successful rehabilitation by 6.8%.
Conclusion: HGS is a simple tool for the planning of the rehabilitation process among patients with hip fracture.
Keywords: hip fracture, rehabilitation, handgrip strength, a Montebello Rehabilitation Factor Score Revised, geriatric
Introduction
Hip fracture is a very common medical problem around the world1 and has numerous negative consequences including prolonged functional impairment,2 impaired quality of life,3 increased risk of transfer to long-term care (LTC),4 high cost,5 and increased mortality.6 The early identification of patients at high risk for negative outcomes is very important for the planning of treatment strategies, the selection of an appropriate rehabilitation setting, and the timing of discharge from the hospital.7 Lim et al8 identified 107 pre-discharge prognostic factors for functional recovery after hip fracture, including handgrip strength (HGS). Xu et al9 also reported, in a systematic review, that HGS is a significant prognostic factor for poor function and mortality.
It should be noted that in various studies of the association between HGS and functional recovery after hip fracture there is no consistent gold standard for defining “strong HGS” and “weak HGS”. Thus, for example, some studies measured HGS as a continuous variable10−12 and others as a categorical variable.13–15 The Revised European Working Group on Sarcopenia (EWGSOP2) defined probable sarcopenia with a cut-off of 27 kg for men and 16 kg for women.16 Perez-Rodriguez et al17 used somewhat different definitions with cut-offs of 23 kg for men and 13 kg for women. In their analysis Savino et al used HGS as a continuous variable and as sex-specific tertiles (highest tertile vs lowest).7
The aim of the present study was to identify an association between HGS and short-term functional recovery among patients who completed intensive rehabilitation after osteoporotic hip fracture repair.
Methods
Setting and Study Population
On September 1, 2019, the measurement of HGS was added to the routine of the Geriatrics department of the Soroka University Medical Center (SUMC), a tertiary center located in the south of Israel. On that date data collection was initiated for the present study.
This retrospective study was based on the medical records of patients 65 years of age and above who completed rehabilitation between September 1, 2019, and December 1, 2021, in the Geriatrics department. The department and the rehabilitation process have been described previously.18 In short, this is a 25-bed ward with a multidisciplinary staff composed of board-certified physicians, physicians training in geriatric medicine, nurses, physiotherapists, occupational therapists, a social worker, and dieticians. Patients were transferred from the Department of Orthopedic Surgery several days after undergoing surgical repair of a hip fracture.
Each patient underwent a comprehensive geriatric assessment and a multidisciplinary rehabilitation strategy was developed for them. The rehabilitation process included early mobilization facilitated by all staff members, physiotherapy five times per week, occupational therapy several times a week, and a psychosocial intervention by the social worker. The department staff held weekly meetings in which changes in the rehabilitation plan were discussed and the discharge date was determined. The patient was discharged when the rehabilitation goals, such as independence in transition, mobility and toileting were achieved, or when the patient reached a functional plateau.
Variables
- The data collected from the patient’s computerized record included:
- Socio-demographic data: age, gender, education level, marital status, information about the patient’s nursing caregiver.
- Medical status: type of hip fracture, the patient’s chronic diseases (the Charlson Comorbidity Index19 was calculated as Total and Total Combined scores), drug therapy and laboratory tests on admission to the rehabilitation setting, complications during rehabilitation (delirium, thromboembolism, pressure sores, and infections), length of stay (LoS) in the orthopedic and geriatric wards.
- HGS: The grip strength of the dominant hand was measured starting with the day of admission to the ward, using the Camry® Digital Hand Grip Dynamometer. Two consecutive measurements were taken on one of the first three days of hospitalization in the department. The patients were assessed while sitting with their shoulders next to their body, the elbow bent at 90 degrees, and the arm in a neutral position. The measuring posture was explained to the patient and then measurements were taken. The highest of the two measurement was used for the study. For data analyses we used HGS as a continuous variable and a binary variable with the patients divided into “strong” and “low muscle strength” groups using the following methods:
Cognitive function was assessed with the Mini Mental State Examination (MMSE).20 The MMSE score was adjusted for age and education level. Patients with MMSE below expected scores for their age and educational level21 and/or patients with a known diagnosis of dementia on admission, and/or patients who suffered from delirium over the course of their hospitalization were defined as suffering from “any cognitive impairment”.
Functional status was assessed by the Functional Independence Measure (FIM)22- anamnestic FIM (anFIM), FIM on admission (FIMa), and FIM on discharge (FIMd).
Mortality rate was measured three, six and 12 months after hip fracture.
Rehabilitation outcome was measured with the Montebello Rehabilitation Factor Score Revised (MRFS-R).23 The MRFS-R is calculated according to the following formula:
MRFS-R = ((FIMd – FIMa)/FIMd)/((an FIM – FIMa)/an FIM) × 100.
This index enables an appraisal of the degree that patients realize their rehabilitation potential. For example, a MRFSR score of 59 indicates that the patient achieved 59% of the rehabilitation potential. Successful rehabilitation was defined as MRFS-R≥50.
Statistical Analyses
Statistical analyses were conducted with the SPSS package (version 26). Continuous variables are presented as means ± standard deviation (SD) and categorical variables are presented as frequencies. Comparisons of variables, according to HGS and success of rehabilitation, were conducted by t-tests or Mann–Whitney tests for continuous variables, based on variable distribution, and chi-square tests for categorical variables. Logistic regression models were developed for success of rehabilitation (MRFS-R≥50). Statistical significance was defined as P<0.05 for all tests.
The study was approved by the Helsinki Committee of the Soroka Medical Center (SOR-466-20). This study was conducted in accordance with the declaration of Helsinki. This study was retrospective and did not require written informed consent. Patient data were kept confidential in this study.
Results
Over the course of the study period 177 patients underwent rehabilitation in the Geriatrics department and 173 completed the process. One of the four who did not complete the rehabilitation died a few days after admission to the ward, and the others were transferred to other wards for treatment (orthopedic surgery, general surgery, and intensive care).
Table 1 shows data on the 173 patients who completed the rehabilitation process and were discharged from the Geriatrics ward. Their mean age was 81.2 ± 7.2 years, and 118 (68.2%) were women.
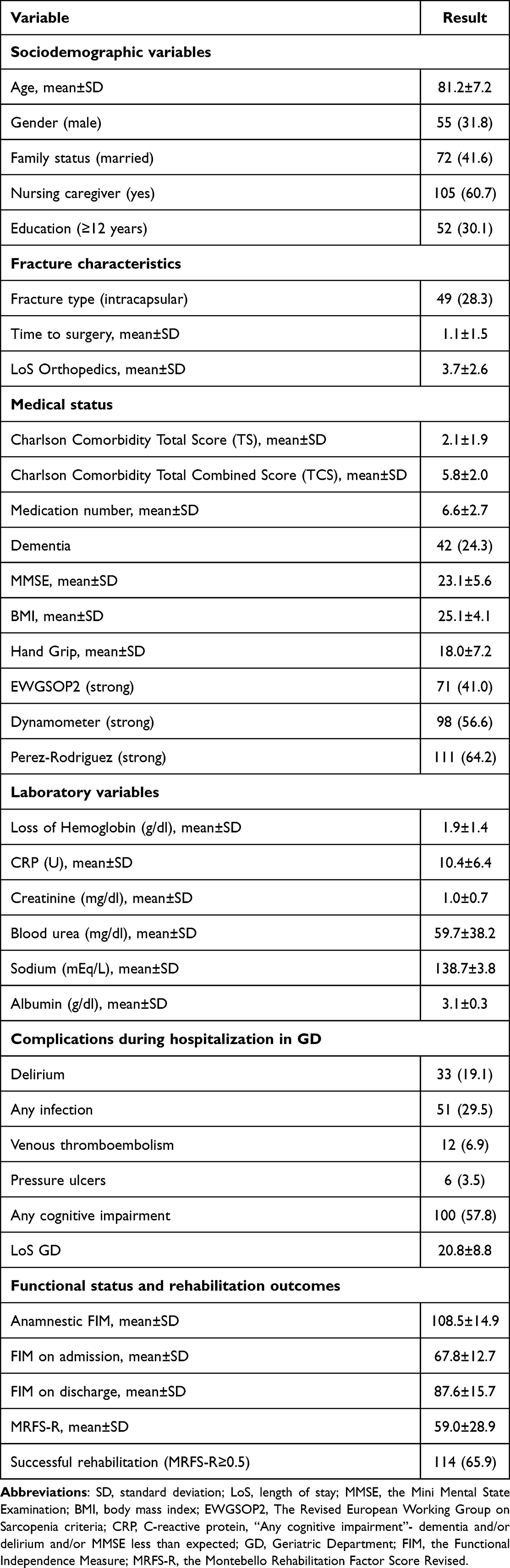 |
Table 1 Study Population Characteristics (N = 173) (Unless Otherwise Stated, Results are [N (%)]) |
The mean HGS was 18.0 ± 7.2 kg. Using the different methods of calculation between 62 patients (35.8%) to 102 patients (60.0%) were defined as “sarcopenic” according to HGS.
The Characteristics of Patients by the Different Definitions of Low Muscle Strength
Table 2 shows that regardless of the method used to define patients, sarcopenic patients had common socio-demographic and clinical characteristics. They were older, more assisted by a nursing caregiver, their MMSE score was lower, more were defined as suffering from “any cognitive impairment”, and their serum albumin level was lower.
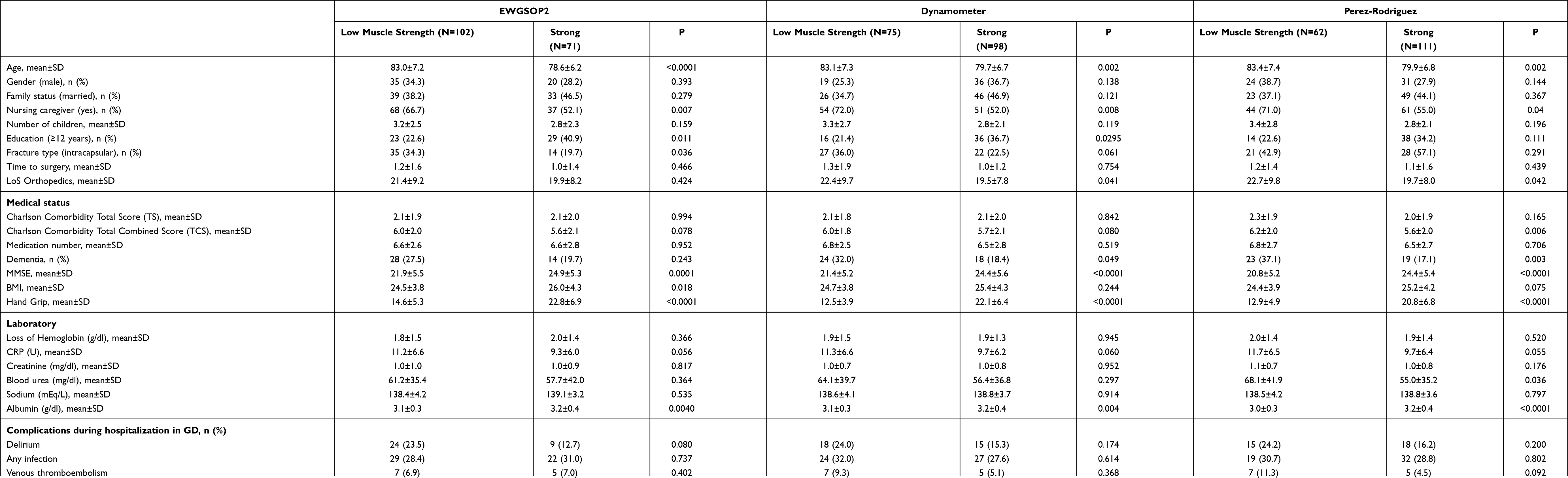 |
Table 2 Patients Characteristics by to Different Definitions of Low Muscle Strength |
In each of the three methods of categorization of low muscle strength the scores for an FIM, FIMa, and FIMd were lower in the sarcopenic group and in each of the three methods the “strong” patients had more success in realizing their rehabilitation potential as reflected in the higher MRFS-R in this group.
For the other variables, the calculation method had a substantial effect on the difference between “sarcopenic” and “strong”. For example, the only method of calculation that showed a difference between “sarcopenic” and “strong” for sub-capital fractures was EWGSOP2, and the only method that led to differences in blood urea and one-year mortality was that of Perez-Rodriquez et al.
Characteristics of Patients Who Underwent Successful Rehabilitation (MRFS-R ≥ 50)
A total of 114 patients (65.9%) had successful rehabilitation. Table 3 shows the results of univariate analyses for sociodemographic and medical variables and rehabilitation success. In comparison with those patients whose rehabilitation was less successful (MRFS-R<50) the group with successful rehabilitation had a higher mean MMSE score (24.3 ± 4.7 vs 20.8 ± 6.5, respectively, P < 0.001), had a lower rate of dementia (14.9% vs 42.4%, respectively, P < 0.0001), a lower rate of delirium (14.0% vs 28.8%, respectively, P = 0.025), and fewer patients with any cognitive impairment (46.5% vs 79.7%, respectively, P = 0.0002). HGS was higher in this group (18.9 ± 7.1 vs 16.2 ± 7.2, P = 0.022), with more patients categorized as “strong” based on EWGSOP2 (46.6% vs 30.5%, respectively, P = 0.044) and the categorization by Perez-Rodriguez et al (71.1% vs 50.9%, respectively, P = 0.001). Patients defined as “strong” also had lower levels of serum creatinine (0.9 ± 0.5 vs 1.2 ± 1.1, respectively, P = 0.004), and urea (55.9 ± 54.2 vs 70.4 ± 51.3, respectively, P = 0.008). There were no statistically significant differences for any of the other sociodemographic and medical variables.
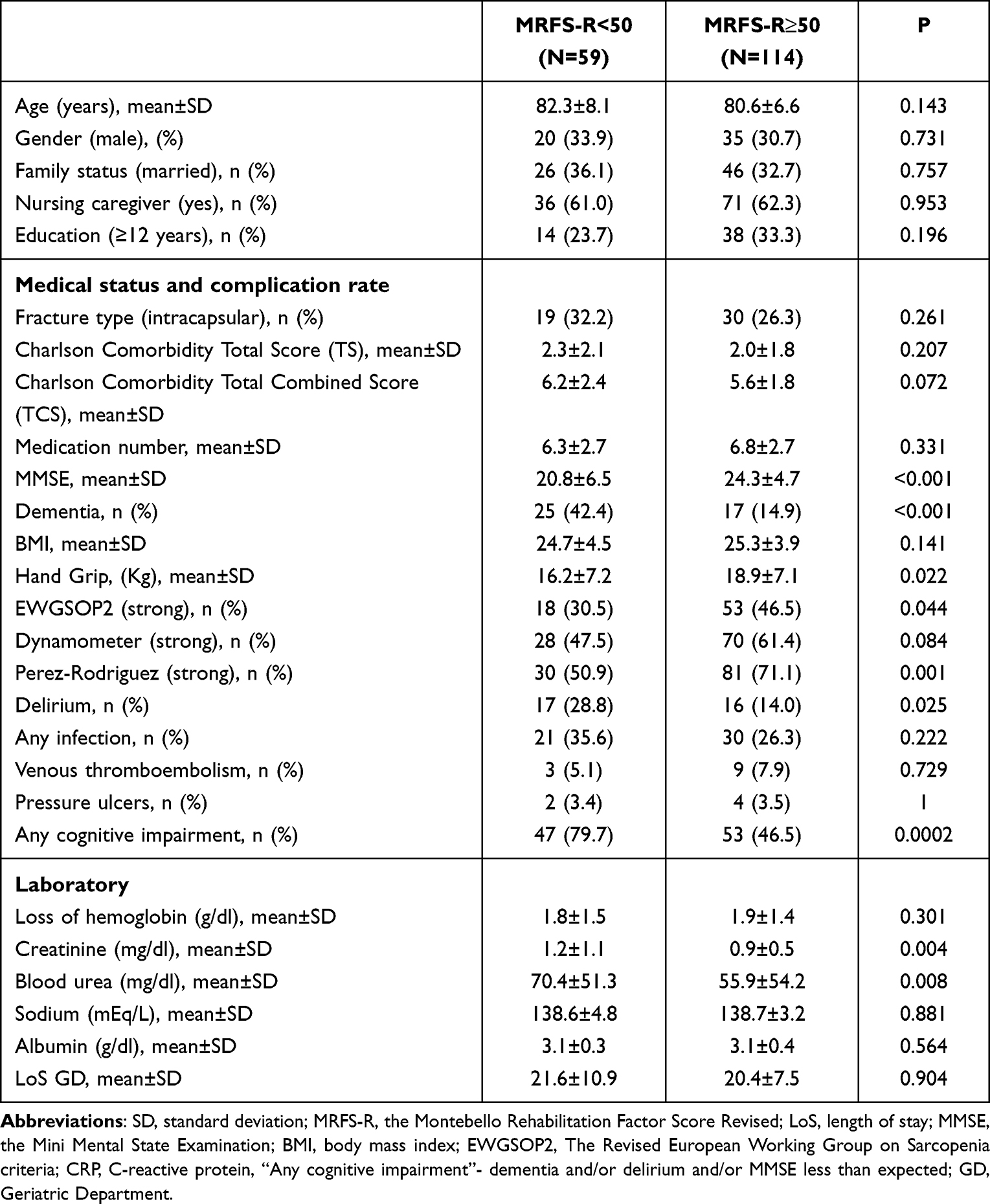 |
Table 3 Patients Characteristics by Rehabilitation Group |
Logistic Regression Analysis Predicting Successful Rehabilitation (MRFS-R≥50)
Several logistic regression models were developed for the prediction of successful rehabilitation. HGS was entered into each model in a different way: as a continuous variable in model 1, as a binary variable (sarcopenic and strong) based on Perez-Rodriguez et al in model 2, by dynamometer in model 3, and by EWGSOP2 in model 4. In addition, all variables with a P value <0.1 in univariate analyses were entered into the models (Table 3). For the cognition-related variables (MMSE, delirium rate, and rate of patients with any cognitive impairment) all of which showed significant associations in univariate analyses, we decided to use the variable “any cognitive impairment” since it includes MMSE and the rates of dementia and delirium. Since urea and creatinine were correlated, we decided to use creatinine in the analyses. TCS, which combines morbidity and age was entered into the model as was sex for purposes of adjustment.
In each of these models (Table 4), any cognitive impairment was an independent predictor of rehabilitation success. In the model where HGS was entered as a continuous variable each increase of 1 kg in HGS increased the chance of a successful rehabilitation by 6.8%.
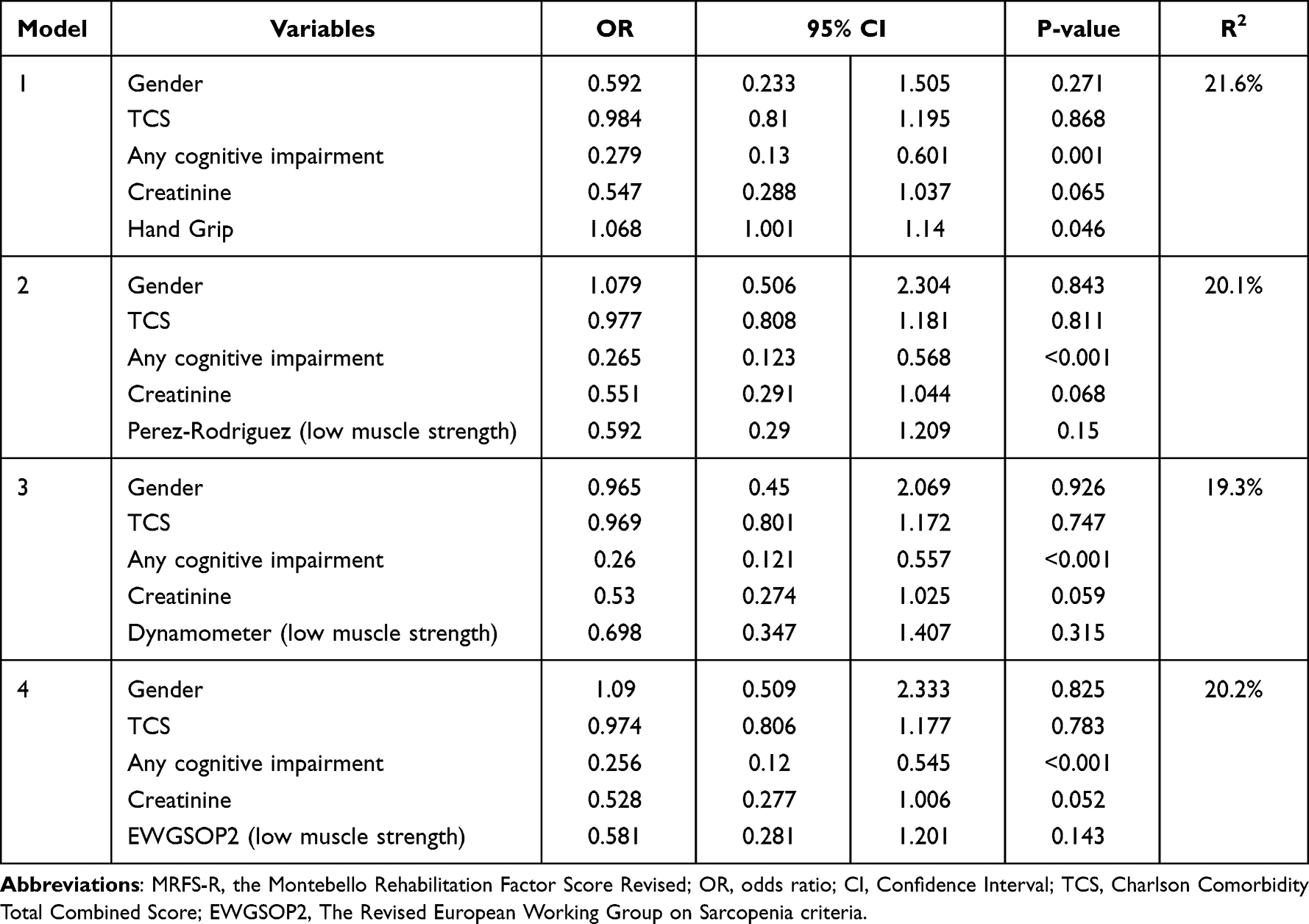 |
Table 4 Logistic Regression Analysis to Predict Rehabilitation Success (MRFS- R≥50) |
Discussion
In the present study we found that some characteristics that differentiate between sarcopenic and strong HGS groups are common to all methods of categorization. These include age, cognitive state, serum albumin level, and functional state prior to and following the fracture, and at the end of an intensive period of rehabilitation. Other differences between the HGS groups are unique to the specific methods of categorizationfor example, the high rate of sub-capital fractures using EWGSOP2, or the high mortality rate a year after the fracture by the method of Perez-Rodriguez et al.
Some previous papers reported differences between sarcopenic and strong HGS groups. The results of the study by Selacovic et al15 was like ours in that the patients with low muscle strength (defined by EWGSOP2) were older, they had a higher rate of sub-capital fractures, their cognitive level was lower, and their pre-fracture functional level was lower. In contrast to that study, in the present study we did not find differences between the groups in terms of sex, BMI, and co-morbidity.
In the study by Perez-Rodriguez et al,17 using their method for definition of low muscle strength, the sarcopenic group was older, their functional status prior to the fracture and on admission was lower, the percentage of patients with cognitive impairment was higher, and the serum albumin level was lower. We found similar results in the present study. We did not find reports in the literature of the categorization of weak HGS and strong HGS, adjusted for age and sex (according to the instructions of the dynamometer), nor were there reports of comparisons between the groups using the different methods of definition of low muscle strength.
We found that HGS as a continuous variable was an independent predictor of the success of rehabilitation with the chance of success increasing by 6.8% with each increase in HGS of 1 kg. Several previous reports identified the association between HGS as a continuous variable and the outcome of rehabilitation. Thus, in the study by Beloosesky et al10 where the association between HGS and FIM was assessed at several points over a half year period, the authors found a significant association between HGS measured at 7–10 days after admission to the ward for rehabilitation and FIM a half year later in their regression analysis.
Savino et al7 who investigated walking recovery over the course of a year following hip fracture found, in a logistic regression model that a 1 kg increase in HGS increased the chance for recovery of independent walking by 6%. Hershkovitz et al12 measured the success of rehabilitation using a method that was very close to the one used in the present study. They used the Montebello Rating Factor Score (MRFS)24 based on motor FIM, with a score above 50 considered a successful rehabilitation. In their logistic regression analysis cognitive score and HGS were independent predictors of rehabilitation success with each increase of 1 kg of HGS increasing the chance of successful rehabilitation by 6.6%.
The study has several strengths. To our knowledge it is the first study to compare different methods of categorization in “sarcopenic” and “strong HGS groups”. We used a comprehensive electronic medical record that enabled us to consider different, clinically important variables. We believe that the method that we developed in the past23 to measure success of rehabilitation (and have used in other studies) reflects optimally the patient’s rehabilitation potential.
However, the study also has several limitations. This is a retrospective study and even though we collected data from a comprehensive database there were important variables that we could not include in the studyfor example, we were not able to calculate co-morbidity by the Cumulative Illness Rating Scale for Geriatrics (CIRS-G),25 which is considered very effective in predictions related to patients after hip fracture.23 We also did not collect data on instrumental activity of daily living, mood status, and quality of life. Such data, without doubt, could have added to our understanding of the rehabilitation process. The study population was relatively small. We did not collect routine data on patients’ functional state after discharge from the department, so this study provides information on short-term functional recovery only.
In summary, in this retrospective study we found that HGS is an independent predictor of rehabilitation success. HGS, a simple and on-hand test, can provide important information during the planning stages of the rehabilitation process for patients following surgical repair of hip fracture.
Acknowledgment
We would like to thank the staff of nurses, physiotherapists, occupational therapists, nutritionists, social workers, and doctors from the Soroka University Medical Center. Without their great efforts on behalf of the patients this study would not have been possible.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Kanis JA, Odén A, McCloskey EV, Johansson H, Wahl DA, Cooper C. A systematic review of Hip fracture incidence and probability of fracture worldwide. Osteoporos Int. 2012;23(9):2239–2256. doi:10.1007/s00198-012-1964-3
2. Dyer SM, Crotty M, Fairhall N, et al. A critical review of the long-term disability outcomes following Hip fracture. BMC Geriatr. 2016;16(1):158. doi:10.1186/s12877-016-0332-0
3. Peeters CM, Visser E, Van de Ree CL, Gosens T, Den Oudsten BL, De Vries J. Quality of life after Hip fracture in the elderly: a systematic literature review. Injury. 2016;47(7):1369–1382. doi:10.1016/j.injury.2016.04.018
4. Rapp K, Rothenbacher D, Magaziner J, et al. Risk of nursing home admission after femoral fracture compared with stroke, myocardial infarction, and pneumonia. J Am Med Dir Assoc. 2015;16(8):
5. Johnell O. The socioeconomic burden of fractures: today and in the 21st century. Am J Med. 1997;103(2a):
6. Melton LJ, Achenbach SJ, Atkinson EJ, Therneau TM, Amin S. Long-term mortality following fractures at different skeletal sites: a population-based cohort study. Osteoporos Int. 2013;24(5):1689–1696. doi:10.1007/s00198-012-2225-1
7. Savino E, Martini E, Lauretani F, et al. Handgrip strength predicts persistent walking recovery after Hip fracture surgery. Am J Med. 2013;126(12):1068–1075.e1061. doi:10.1016/j.amjmed.2013.04.017
8. Lim KK, Matchar DB, Chong JL, Yeo W, Howe TS, Koh JSB. Pre-discharge prognostic factors of physical function among older adults with Hip fracture surgery: a systematic review. Osteoporos Int. 2019;30(5):929–938. doi:10.1007/s00198-018-04831-5
9. Xu BY, Yan S, Low LL, Vasanwala FF, Low SG. Predictors of poor functional outcomes and mortality in patients with Hip fracture: a systematic review. BMC Musculoskelet Disord. 2019;20(1):568. doi:10.1186/s12891-019-2950-0
10. Beloosesky Y, Weiss A, Manasian M, Salai M. Handgrip strength of the elderly after Hip fracture repair correlates with functional outcome. Disabil Rehabil. 2010;32(5):367–373. doi:10.3109/09638280903168499
11. Chang CM, Lee CH, Shih CM, Wang SP, Chiu YC, Hsu CE. Handgrip strength: a reliable predictor of postoperative early ambulation capacity for the elderly with Hip fracture. BMC Musculoskelet Disord. 2021;22(1):103. doi:10.1186/s12891-021-03964-9
12. Hershkovitz A, Yichayaou B, Ronen A, et al. The association between hand grip strength and rehabilitation outcome in post-acute Hip fractured patients. Aging Clin Exp Res. 2019;31(10):1509–1516. doi:10.1007/s40520-019-01200-y
13. Di Monaco M, Castiglioni C, Bardesono F, Milano E, Massazza G. The handgrip strength threshold of 16 kg discriminates successful rehabilitation: a prospective short-term study of 258 women with Hip fracture. Arch Gerontol Geriatr. 2020;91:104190. doi:10.1016/j.archger.2020.104190
14. Gleich J, Pfeufer D, Keppler AM, et al. Identification of Hip fracture patients at risk for postoperative mobilisation complications via handgrip strength assessment. Arch Orthop Trauma Surg. 2022;142(6):997–1002. doi:10.1007/s00402-021-03756-9
15. Selakovic I, Dubljanin-Raspopovic E, Markovic-Denic L, et al. Can early assessment of hand grip strength in older Hip fracture patients predict functional outcome? PLoS One. 2019;14(8):e0213223. doi:10.1371/journal.pone.0213223
16. Cruz-Jentoft AJ, Bahat G, Bauer J, et al. Sarcopenia: revised European consensus on definition and diagnosis. Age Ageing. 2019;48(1):16–31. doi:10.1093/ageing/afy169
17. Pérez-Rodríguez P, Rabes-Rodríguez L, Sáez-Nieto C, et al. Handgrip strength predicts 1-year functional recovery and mortality in Hip fracture patients. Maturitas. 2020;141:20–25. doi:10.1016/j.maturitas.2020.06.013
18. Levi Y, Punchik B, Zikrin E, et al. Intensive inpatient vs. home-based rehabilitation after Hip fracture in the elderly population. Front Med. 2020;7:592693. doi:10.3389/fmed.2020.592693
19. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373–383. doi:10.1016/0021-9681(87)90171-8
20. Folstein MF, Folstein SE, McHugh PR. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. 1975;12(3):189–198. doi:10.1016/0022-3956(75)90026-6
21. Crum RM, Anthony JC, Bassett SS, Folstein MF. Population-based norms for the Mini-Mental State Examination by age and educational level. JAMA. 1993;269(18):2386–2391. doi:10.1001/jama.1993.03500180078038
22. Keith RA, Granger CV, Hamilton BB, Sherwin FS. The functional Independence measure: a new tool for rehabilitation. Adv Clin Rehabil. 1987;1:6–18.
23. Press Y, Grinshpun Y, Berzak A, Friger M, Clarfield AM. The effect of co-morbidity on the rehabilitation process in elderly patients after Hip fracture. Arch Gerontol Geriatr. 2007;45(3):281–294. doi:10.1016/j.archger.2007.01.059
24. Drubach DA, Kelly MP, Taragano FE. The Montebello rehabilitation factor score. J Neural Rehabil. 1994;8:881–889.
25. Miller MD, Paradis CF, Houck PR, et al. Rating chronic medical illness burden in geropsychiatric practice and research: application of the Cumulative Illness Rating Scale. Psychiatry Res. 1992;41(3):237–248. doi:10.1016/0165-1781(92)90005-N
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.