")
Back to Journals » Clinical, Cosmetic and Investigational Dentistry » Volume 11
Halitosis And Its Associated Factors Among Kermanshah High School Students (2015)
Authors Ziaei N, Hosseinpour S, Nazari H, Rezaei M , Rezaei K
Received 15 May 2019
Accepted for publication 3 October 2019
Published 22 October 2019 Volume 2019:11 Pages 327—338
DOI https://doi.org/10.2147/CCIDE.S215869
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Christopher E. Okunseri
Narges Ziaei,1 Sajjad Hosseinpour,1 Hesamedin Nazari,2 Mansour Rezaei,3 Khansa Rezaei4
1Department of Periodontology, School of Dentistry, Kermanshah University of Medical Sciences, Kermanshah, Iran; 2Department of Oral and Maxillofacial Surgery, School of Dentistry, Kermanshah University of Medical Sciences, Kermanshah, Iran; 3Social Development and Health Promotion Research Center, Kermanshah University of Medical Sciences, Kermanshah, Iran; 4Educational Development Center, Kermanshah University of Medical Sciences, Kermanshah, Iran
Correspondence: Khansa Rezaei
Educational Development Center, Taleghani Hospital, Shahid Beheshti Blvd, Kermanshah 67146-73159, Iran
Tel +989189333405
Email [email protected]
Introduction: Halitosis as a common dental problem results in psychological social problems and relates to many factors. The aim of this study was to evaluate the prevalence of halitosis and its associated factors among students aged from 14 to 18 years in Kermanshah in 2015.
Materials and methods: The study was conducted in high school students of Kermanshah city in 2015. The questionnaire including questions about bad breath and other associated factors (demographic information, background diseases, oral and dental problems, decay-missing-filled (DMF) index, etc.) was completed by students or determined by the examiner. Organoleptic evaluation was conducted. Prevalence of organoleptic and self-reported halitosis and related factors was reported. The relationship between malodor and variables was evaluated and the most important factor was determined by multiple logistic regression analysis. The diagnostic agreement between self-perception and organoleptic halitosis was assessed using Kappa coefficient as well.
Results: The prevalence of halitosis in the organoleptic evaluation was 29.75% and higher in boys (32.6% male vs. 25.2% female) and 27.47% in self-perception (32.9% male vs. 19% female). The diagnostic agreement between organoleptic and self-perception halitosis was moderate or poor. Among the studied factors, the most important factor related to the organoleptic evaluation of halitosis was DMF≥4 (P<0.001 and OR=2.253).
Conclusion: The DMF index was the factor most strongly associated with organoleptic halitosis in this sample of high school students. Other factors with significant association included parent’s lower education level, not brushing, not flossing, bleeding gums, tongue coating, pericoronitis, and plaque index. Also, older age, male gender, and gastrointestinal disease increased the possibility for halitosis.
Keywords: halitosis, organoleptic, self-perception
Introduction
Halitosis is an unpleasant smell from the mouth of people that is recognizable to others. This medical-social problem exists in different ages and races. It is the third common cause of oral problems after decay and periodontal diseases.1 Halitosis not only can cause concern in various aspects of health but also can lead to psychological changes causing social and personal isolation.2 More than 50% of the general population is suffering from this symptom.3
The origin of malodor in 90% of patients is related to oral cavity, in 9% it is non-oral ones such as respiratory system, digestive system or urinary system, and in 1% it is diet or medication.3 Halitosis oral causes include tongue coating, periodontal diseases, deep caries lesions associated with exposure of palpation, pericoronitis, mucosal ulcers, remaining food and debris, poor dental health, reduced salivation, and oral respiration.4 Among the mentioned oral causes, tongue coating especially the posterior part of the back of the tongue is the most common cause.5 Gingival inflammation and periodontitis are the main causes of bad breath.6 Reduced salivation can be caused by diseases like diabetes, Sjogren’s syndrome, stress, depression, drug use, oral respiration and alcohol consumption, which increase plaque volume in the teeth and tongue. Research has shown the association between oral dryness and increased halitosis.6 Extra-oral halitosis includes upper respiratory tract problems, sinusitis, polyps, digestive disorders and some metabolic diseases such as diabetes.7 The respiratory tract infection, nasal and sinus secretions that enter oropharynx, oral respiration, tonsil inflammation, foreign body in the nose, bronchiectasis, other respiratory infections, and lung cancer can be the causes of malodor.8 Also, bad breath is directly related to the consumption of some foods such as garlic and onions and is common in smokers. Also, reduced salivation could be the side effect of drugs such as antidepressants, antihistamines, antipsychotics, antihypertensives, decongestants and opiates, which cause halitosis.7
A non-pathologic form of halitosis occurs in the morning due to the low salivary secretion during the night. Women exhibit higher levels of sulfur compounds in morning breath.6 Diseases like diabetes, kidney diseases and hepatitis associated with bad breath are rare in adolescents. But their different lifestyles such as using more precooked and packaged foods can affect malodor.9 Clinical studies indicate that anxiety conditions may increase sulfide volatile compounds and consequently cause halitosis. Therefore, the treatment requires psychological support in addition to professional dental care.10
The main causative components of bad breath are volatile sulfur compounds (VSCs), especially hydrogen sulfide (H2S), methyl mercaptan (CH3SH), and dimethyl sulfide ((CH3)2S).5 The main bacteria involved in halitosis are Fusobacterium nucleatum, Prevotella intermedia and Tannerella forsythia.1 Microorganisms produce volatile compounds (VCs) in reaction with sulfur compounds in saliva and blood.5
There are two organoleptic and instrumental methods for evaluating halitosis.11 In the organoleptic method, the smell of bad breath is determined by the sense of smell of the examiner, and in the instrumental method, there are numerous devices including gas chromatographs, electronic noses, sulfide monitors, and fresh kiss. Advantages of the organoleptic method are low cost and ease of application; however, the measured results cannot be repeated.11 This method is a golden standard for the detection of halitosis.12
In some studies, a significant positive correlation was observed between using mouthwash and reduced salivation, tongue coating and bad breath. Chlorhexidine mouthwash is an antimicrobial agent that has been shown to be effective in halitosis. However, long-term use of chlorhexidine mouthwash has side effects, such as discoloration of the teeth and tongue, bad taste, and decreased taste sensation.13
If the oral cavity is the cause of bad breath, reducing bacterial load is essential. Periodontal examination is the first step. Necrotizing ulcerative, gingivitis, adult invasive periodontitis, and periodontal pocket can increase the bacterial burden. Therefore, periodontal health is very important in controlling bad breath. Sometimes, even if periodontal health is excellent, tongue coating can be the considerable source of halitosis. Tongue coating will be greater if the patient has a geographic or fissured tongue. Hence, brushing the back of the tongue is very effective in eliminating malodor. Existing and required dental restorations should be investigated. Inappropriate prostheses and restoration should be replaced or corrected. Also, available dental caries, nonvital teeth with a fistula or a pulp opening to mouth provide a reservoir for bacterial accumulation, which is very important to treat or restore these teeth. Other causes of halitosis such as dry mouth, pericoronitis (soft tissue infections and inflammatory conditions around the tooth crown at any time of tooth development),14 oral ulcers and malignant tumors should be well recognized and treated. The cause of dry mouth should be investigated in detail. If oral dryness is due to radiotherapy or salivary gland diseases, artificial saliva should be prescribed as a treatment. Medical history can determine the cause of halitosis. If the source of the bad breath is extra-oral causes, such as respiratory, digestive, liver, kidney, endocrine, or blood diseases, expert advice should be considered. Halitophobia management is much more complicated than real halitosis. People with halitophobia prevent themselves from social behaviors or even talking to others. Consultation with a psychologist is required if the patient has halitophobia.3
Many studies in different countries have been conducted on the prevalence of halitosis and on the relationship between demographic factors,5,9,15,16 psychosocial factors,9,10 dietary factors,4,9,16,17 health habits,10,18 oral and dental diseases, and other diseases4,15–20 with malodor. Considering that bad breath has a different outbreak in different societies with various races and ages, and so far no such study has been done in Iranian population, and halitosis causes medical-social problems in individuals, in this study we investigated the prevalence of malodor and its causes among high school students in Kermanshah city and the prevalence of various factors associated with it.
Materials And Methods
This cross-sectional study included 790 high school students aged 14 to 18 years who were selected through a two-stage cluster sampling, of which 484 (61.3%) were boys and 306 (38.7%) were girls. The variables studied included halitosis, age, sex, respiratory disease, sinusitis, gastrointestinal disease, bleeding gums, dry mouth, tongue coating, fissured tongue, father’s education, mother’s education, brushing, dental floss, cigarettes, mouthwash, oral hygiene education history, the decay-missing-filled (DMF) index, postnasal drip, pericoronitis, plaque index, organoleptic evaluation, caries-free status (CFS), and mouth breathing.
At first, high schools in Kermanshah were identified. Then, based on the sample size of the study, some of the high schools were selected by cluster sampling. After that, in each high school, a certain number of students were selected by cluster sampling. The written informed consent was delivered to the selected students before the study, completed by their parents and received on the day of the study. The data were anonymized and maintained with confidentiality. The Research Ethics Committee of Kermanshah University of Medical Sciences approved this study process on 17 Feb 2016 (number: IR.KUMS.REC.1394.391).
On the desired day, the designed questionnaire that included the study questions was distributed among the students for completion. Students’ self-evaluation of halitosis was also included in the questionnaire as a general question on a dichotomous scale. After completing the questionnaire by the students, the examiner examined each student. The evaluation was performed by a single investigator who was a well-trained dentist and was not aware of the outcome of self-perception halitosis. The examination was done in the morning after students’ first break time while they had eaten their snack (almost 3 hrs after morning brush and 1 hr after eating). During the examination, bad breath, history of respiratory diseases, sinusitis and gastrointestinal disease, DMF, dry mouth, fissured tongue, postnasal drip, pericoronitis, plaque index, CFS, periodontal condition, mouth breathing, and tongue coating were investigated. A dry mouth was determined by the tongue depressor test, in which tongue depressor was placed on the surface of the buccal mucosa, and when removing it, oral dryness was seen in case of adhesion of the mucus to tongue depressor. The diagnosis of tongue coating and fissured tongue was visually determined by the examiner. For division of tongue coating, if there was no tongue coating, it was expressed as “no”, if only one third of the posterior part of the tongue had coating “first grade”, two thirds of the posterior had coating “second grade”, and if the whole tongue had coating “third grade”. The postnasal drip, according to the patient’s own words and also the examiner’s monitoring with a flashlight behind the throat, to find pharyngeal secretions, was determined. Also, determination of plaque index was done by the probe and visual observation. For plaque index, the absence of plaque was “zero rank”, revealing the plaque after the periodontal probe moved along the gingival margin “first rank”, visible plaque “second rank”, and large plaque “third rank”. For organoleptic evaluation, the patient was asked to count the numbers from 1 to 10, and while counting the numbers, the patient’s halitosis was examined by the examiner’s sense of smell at 10 cm from the student’s oral cavity. He determined if the produced odors smell bad or not. In addition, CFS was determined visually and based on catheter examination and diagnosis of caries. Students’ examination was performed on a chair with artificial light, a dental mirror, and so on.
To analyze the data, chi-square test was done to investigate the relationship between halitosis and qualitative variables and single-variable logistic regression was used to calculate the odds ratio for each variable. To calculate the adjusted odds ratio and the final model, backward multiple logistic regression model was used. Also, Kolmogorov–Smirnov test was used to test the normalization of the quantitative data. The Mann–Whitney U-test was used to compare the quantitative variables among those who had bad breath and those who did not have it. Kappa coefficient was used to evaluate the diagnostic agreement between self-perception and organoleptic halitosis evaluation. Data were analyzed using SPSS.16 software. The significance level in this study was considered 0.05.
Results
Mean and standard deviation of students’ age in this study were 16.11 and 1.03, respectively. The prevalence of halitosis was 29.75% based on organoleptic evaluation.
None of the quantitative variables follow the normal distribution. The descriptive statistics of the quantitative variables D, M, F and DMF were reported in terms of mean and standard deviation in halitosis variable as well as in general (Table 1). Also, Mann–Whitney U-test showed that D, M, and DMF were significantly lower in those without halitosis than in those with halitosis. F had no significant difference between those with halitosis and those without it.
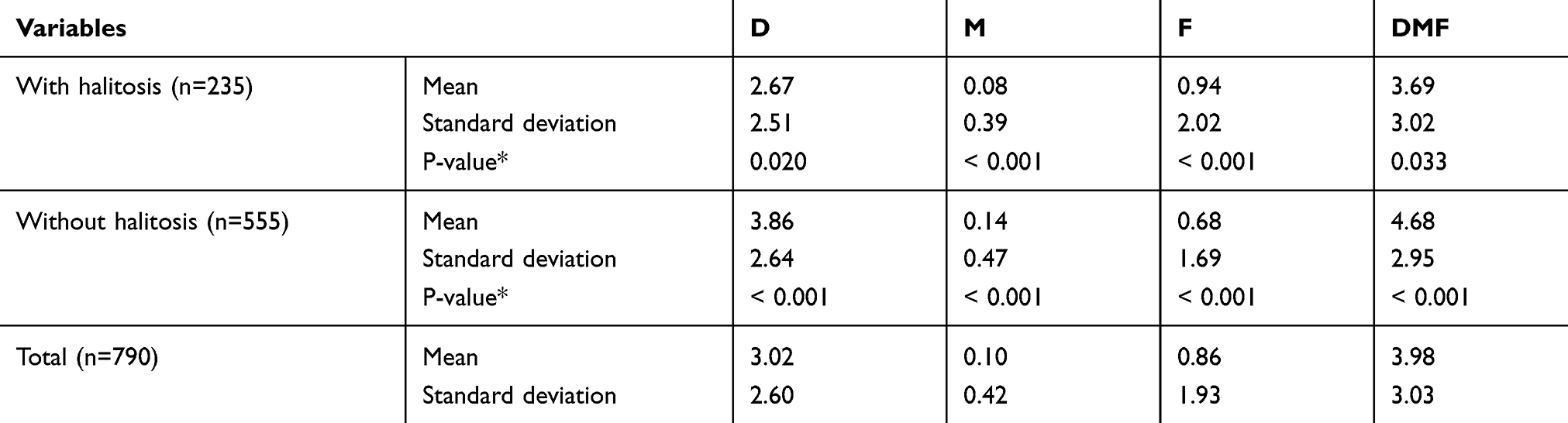 |
Table 1 Normality Test Results For DMF Index In Two Groups |
Chi-square test showed that there was a significant relationship between halitosis and parents’ education, brushing, dental floss, bleeding gums, tongue coating, pericoronitis, plaque index, and CFS. But there was no significant relationship between halitosis and gender, using mouthwash, oral hygiene education history, specific disease, specific drug use, respiratory disease, sinusitis, gastrointestinal disease, dry mouth, fissured tongue, mouth breathing, and postnasal drip (Table 2).
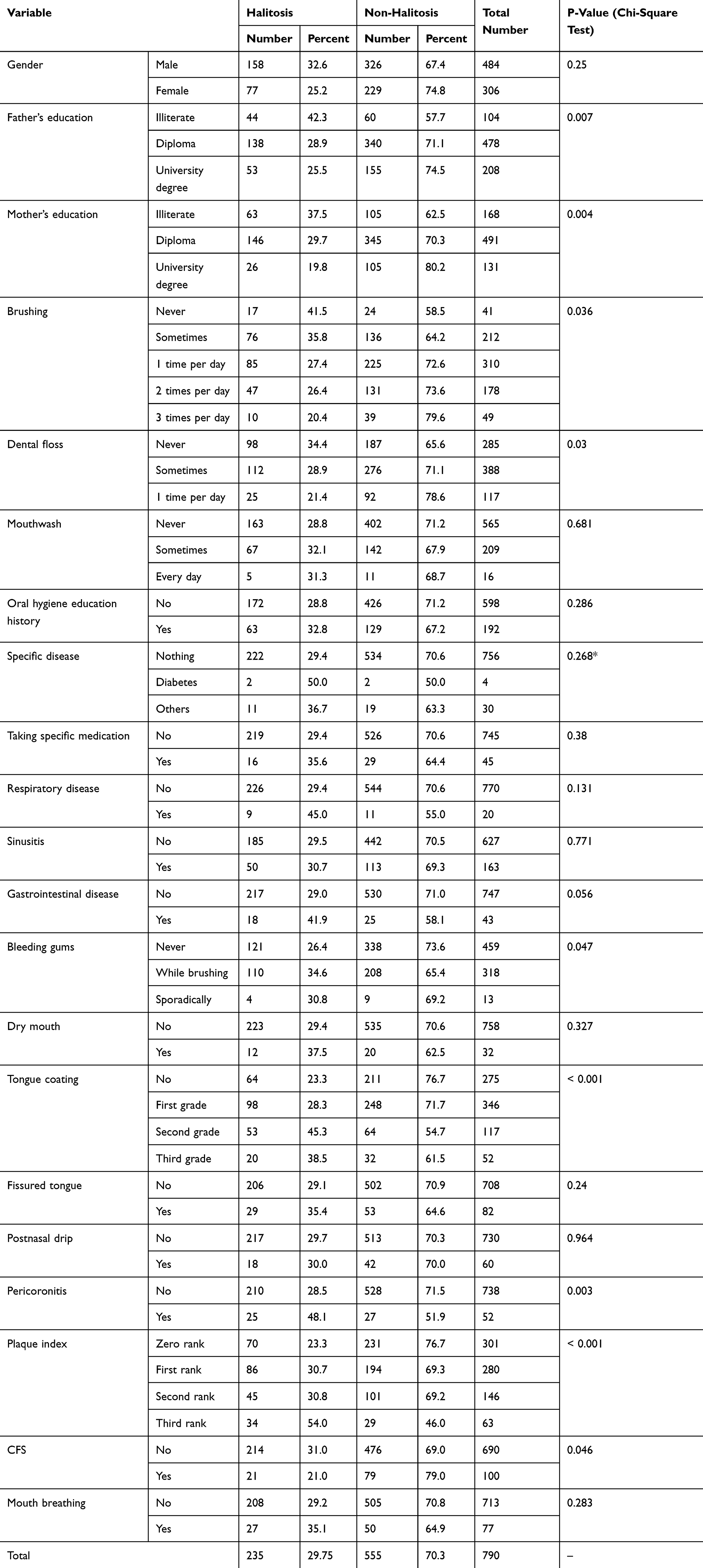 |
Table 2 Frequency Distribution Of Halitosis In The Studied Subjects According To Organoleptic Method |
Single-variable logistic regression showed that the chance of organoleptic evaluation halitosis in girls was 0.694 times more than boys, and this relationship was significant. The chance of organoleptic evaluation halitosis in those with a DMF of more than four was 2.253 times more than those with a DMF less than four, and this was a significant relationship, and this was the most influential variable on the chance of organoleptic evaluation halitosis in this model. Also, in this single-variable model, the variables including bleeding gums, tongue coating, father’s education, mother’s education, brushing, dental floss, pericoronitis, plaque index, and CFS had a significant relationship with the chance of organoleptic evaluation halitosis.
In the backward multiple logistic regression model, some variables (independent variables) had a significant relationship with the chance of halitosis (dependent variable) such as sex (boys two times more than girls), age (each year older, 1.17 times more), D (each unit increase in D, 1.211 times more), gastrointestinal disease (those with gastrointestinal disease, 2.359 times more), second grade tongue coating (second grade tongue coating, 2.903 times more), pericoronitis (pericoronitis, 2.063 times more), and third rank plaque index (third rank plaque index, 3.414 times more). Also, some variables did not have a significant relationship with the chance of halitosis such as M (each unit increase in M, 1.407 times more), use of dental floss (those who brush once a day, 0.461 times more than those who never brush), mouthwash, bleeding gums (bleeding gums, 1.333 times more), third grade tongue coating (third grade tongue coating, 1.915 times more than without tongue coating), and first rank plaque index (first rank plaque index, 1.377 times more).
Chi-square test showed that there are statistical significant relationship between tongue coating and brushing (P=0.01), no significant relationship between mouth breathing and bleeding gums (P=0.503), a statistical significant relationship between bleeding gums and plaque index (P<0.001), brushing (P<0.001), and mouthwash (P=0.008), and no statistical significant relationship between bleeding gums and dental floss (P<0.001).
The prevalence of self-perception halitosis in this study was 27.47%. The diagnostic agreement (Kappa coefficient) between the two methods used in this study, namely self-perception and organoleptic methods, was significant (P<0.001) and its value was 0.309 which is medium downward (Table 3).
 |
Table 3 Frequency Distribution Of Individuals By Organoleptic Evaluation And Self-Perception Halitosis |
There was a significant relationship between self-perception halitosis and gender (boys higher than girls), father’s education (illiterate fathers higher than fathers with a diploma or a university degree), mother’s education (illiterate mothers higher than mothers with a diploma or a university degree), brushing (the highest in never brushing, the lowest in brushing three times per day), dental floss (the highest in never using dental floss, the lowest in using dental floss once a day), mouthwash (never using mouthwash higher than in using mouthwash every day), bleeding gums (the lowest in no bleeding gums, the highest in bleeding gums sporadically), and tongue coating (22.5% in no tongue coating and 41% in second-grade tongue coating). In addition, there was no significant relationship between self-perception halitosis and oral hygiene education history, presence of specific disease, taking specific medication, respiratory disease, sinusitis, gastrointestinal disease, dry mouth, fissured tongue, postnasal drip, and mouth breathing (Table 4).
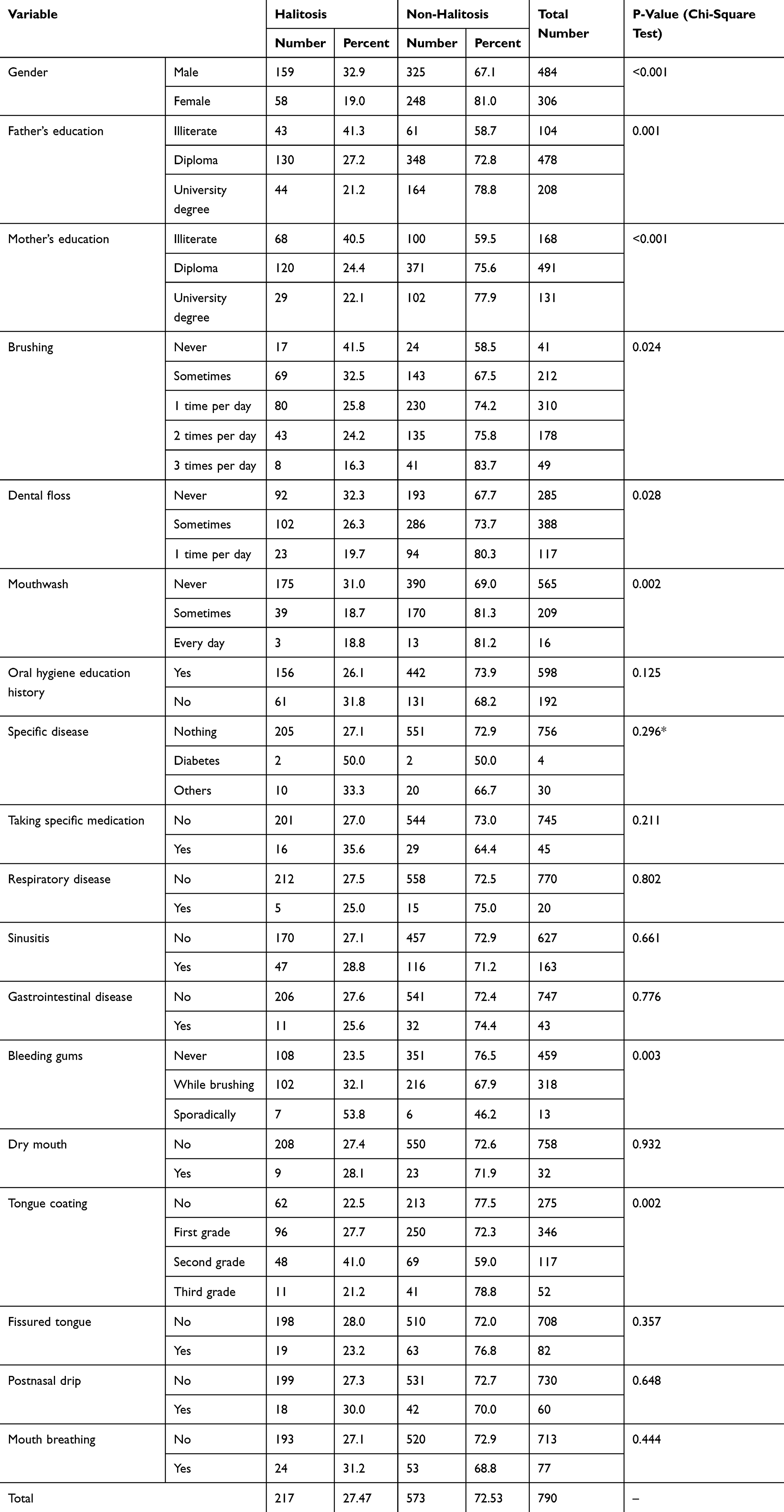 |
Table 4 Frequency Distribution Of Halitosis In The Studied Subjects According To Self-Perception Method |
In multiple logistic regression model, there was a significant relationship between the chance of self-perception halitosis and gender (girls 0.504 times higher than boys), mother’s education (illiterate mothers 1.856 times higher than literate mothers), mouthwash (not using mouthwash 1.903 times more than using it), oral hygiene education history (oral hygiene education history 1.748 times more than without it), bleeding gums (bleeding gums 1.416 times more than without it), and tongue coating (tongue coating 1.44 times more than without it). It is worth noting that mouthwash was the most effective variable on the chance of self-perception halitosis in this model. Also, there was no significant relationship between the chance of self-perception halitosis and DMF. In addition, the constant coefficient in this model was 0.125. Low constant coefficient indicates that most of the variables affecting malodor were studied in this study (Table 5).
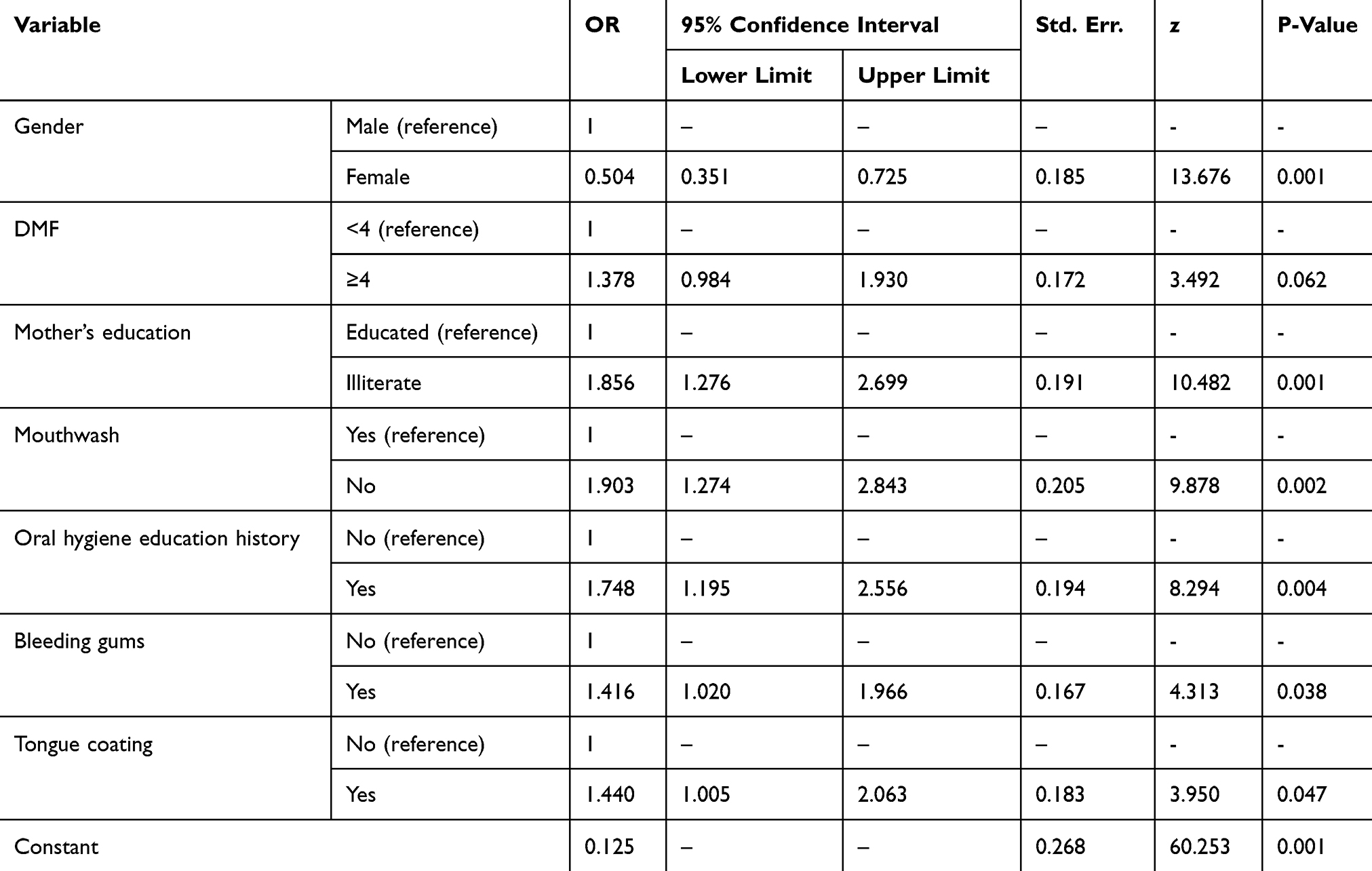 |
Table 5 Multiple Logistic Regression Analysis Of Related Factors With Self-Perception Sensory Evaluation Of Halitosis (n=790) |
Discussion
The present study was found that a significant number of students, about 29.75% in the organoleptic evaluation and 27.47% in the self-perception evaluation, have bad breath, an important problem of this age. However, the prevalence of bad breath has been expressed differently in different studies. For example, in 2015, a study was conducted in Korea in 359,263 young people and the prevalence of halitosis was 23.6%.9 In 2014, another study was conducted in India, which included 285 dental students. In this study, the prevalence of halitosis was 44.1% for men and 45.32% for women.5 Another study in Jordan in 2014 was conducted in 205 people, with a halitosis prevalence of 78%.19 A further study of 839 cases in 2010 showed a 61.1% prevalence of halitosis.15
In the present study, the prevalence of halitosis was higher in boys (organoleptic: 32.6% male and 25.2% female, self-perception: 32.9% male and 19% female). However, in most previous studies, halitosis was higher in girls than in boys.7,9,10 Considering the higher frequency of teeth brushing and the use of dental floss among girls, it seems that the difference is due to the higher level of health in girls compared to boys.
In general, various factors are associated with bad breath, which we examined some of these factors. One of the factors was the level of parents’ education that there was a significant relationship between the prevalence of halitosis and the low level of parents’ education, which could be due to parents’ low awareness of oral health and inadequate family status. Previous studies have shown that socioeconomic inequality affects oral health.9 Also, Youngnak-Piboonratanakit and Vachirarojpisan (2010) showed that there is a significant relationship between halitosis and the education level of people, and bad breath has a higher prevalence among those with lower literacy levels.15
There was a relationship between halitosis and brushing, and dental floss. In the present study, it was found that there is a relationship between brushing and reducing tongue coating and bleeding gums. Tongue coating and periodontal diseases are also the main causes of halitosis.9 Previous studies have also shown that brushing and dental floss can significantly reduce bad breath.5 Therefore, it can be concluded that brushing can reduce bad breath by increasing oral hygiene and reducing plaque index, bleeding gums, periodontal diseases, tongue coating, and decay, all of which are related to malodor.
In the organoleptic evaluation, there was no significant relationship between halitosis and using mouthwash, and oral hygiene education history. However, in self-perception halitosis, there was a significant relationship between using mouthwash and reduction of halitosis. Also, in the multiple model, it was found that this variable was the most effective variable on the chance of self-perception halitosis. In previous studies, this contradiction exists with respect to mouthwash, for example, a study by Shinada et al (2010) showed that there was a positive relationship between the use of mouthwash and bad breath reduction.13 Nevertheless, the study of Youngnak-Piboonratanakit and Vachirarojpisan (2010) showed that the prevalence of halitosis is higher in those who use mouthwash, as in the present study.15 Of course, due to the fact that in the current study, the number of people who continuously use mouthwash is low, and it is not possible to judge accurately in this regard. It should also be considered that people who are more likely to use mouthwashes usually have a particular oral problem that may be associated with their bad breath than those who have been able to get rid of it after using mouthwash. Even those who suffer from bad breath for any reason may have used mouthwashes to treat their problem, and after taking mouthwash, they have concluded that their problem has been resolved. These reasons have led to using mouthwash to be the most effective factor associated with halitosis in self-perception.
In the present study, no statistically significant relationship was found between specific diseases such as diabetes, sinusitis, gastrointestinal disease, respiratory disease, mouth breathing, dry mouth, and taking a specific medication. Also, in a study by Aylıkcı and Çolak in 2013, it was expressed that only 9% of the causes of bad breath is due to non-oral agents such as respiratory disease, gastrointestinal disease, diabetes, sinusitis, mouth breathing, and dry mouth, and only 1% of the causes of halitosis is associated with the consumption of some medications and diet.3
There was a relationship between halitosis and tongue coating. In various studies, tongue coating is one of the main causes of bad breath.5,19 Dorsal surface of the tongue is an irregular environment for the accumulation of dead epithelial cells and food droplets, which provides a suitable environment for the accumulation of bacteria.6
There was a significant statistical relationship between halitosis and bleeding gums. Studies have shown that periodontal disease is one of the main causes of malodor.4 In another study by Youngnak-Piboonratanakit and Vachirarojpisan (2010), bleeding gums during brushing was the most important factor associated with halitosis after tongue coating.15 Gingival inflammation and periodontitis are introduced as the main causes of bad breath, and there is a positive relationship between the depth of the pocket and the sulfur compounds.6 It should also be noted that gingival bleeding usually occurs in those who have a very poor oral hygiene level and who have multiple dental problems such as caries, abundant dental plaque and tongue coating, which are also associated with halitosis.
There was no statistically significant relationship between organoleptic evaluation of halitosis and fissured tongue, but the prevalence of halitosis was higher in those who had fissured tongue than those who did not have fissured tongue. These grooves provide a good place for food to be stuck and to accumulate bacteria.21
In the present study, there was no relationship between halitosis and postnasal drip, while in previous studies, this relationship was reported.22
There was a significant statistical relationship between bad breath and pericoronitis. In many studies, pericoronitis has been identified as one of the causes of halitosis.3,7 Regarding the fact that pericoronitis is more related to the wisdom teeth14 and the studied subjects are at the age of the wisdom teeth growth and the prevalence of pericoronitis, the relationship between halitosis and pericoronitis seems logical.
There was a significant statistical relationship between halitosis and plaque index. By reducing oral hygiene and increasing oral plaque, raw materials are provided for the activity of halitosis-related bacteria. In most studies, poor oral health and increased plaque have been mentioned as one of the causes of bad breath.3,23
There was a significant statistical relationship between halitosis and CFS. The presence of dental caries provides favorable conditions for the activity of bacteria associated with bad breath. It should also be borne in mind that dental caries shows poor oral health, which is one of the causes associated with bad breath. In most studies, dental caries has been reported as one of the main causes of halitosis.3,5,23
There was a relationship between halitosis and DMF increase in organoleptic evaluation. An increase in DMF indicates an increase in caries and a low oral hygiene level, and it seems logical that this may increase the chance of halitosis. Previous studies have shown that this is true.24
The diagnostic agreement between the two methods used in this study, namely self-perception and organoleptic methods, was significant. Perhaps because in the organoleptic evaluation, halitosis occurs only at a specific time of the day, and halitosis depends on different variables such as nutrition and stress, and the control of these factors is almost impossible, as well as considering that the patient’s perception of the presence of bad breath may be beyond the time of study or certain conditions beyond the time of the study; the weak correlation between self-perception and organoleptic evaluation is not too far-fetched. Of course, in a study conducted by Bornstein et al in 2009, the correlation between different methods of halitosis assessment was also studied, and there was also a weak correlation between the different methods of study.4
One of the limitations of this study is that it was done only in a specific age group of people. Also, considering that the study is done at the age of puberty of people and hormonal changes in this age affect halitosis, and the sensitivity of the youth to bad breath is more than the rest of the population, it cannot be generalized to the whole society. One of the other drawbacks in this study was the lack of confidence of the participants in the study about the confidentiality of their information, which caused everyone to have a negative answer to the question about smoking, which led to the removal of this question from the study.
It is recommended to use halimeter in future studies and calculate the agreement rate of the three methods of self-perception, organoleptic and halimeter.
Conclusion
The DMF index was the strongest factor associated with bad breath in organoleptic evaluation in this sample of high school students. Other factors that had a significant relationship with halitosis in organoleptic evaluation included parent’s lower education level, not brushing, not flossing, bleeding gums, tongue coating, pericoronitis, plaque index, and lack of CFS. Also, older age, male gender, and gastrointestinal disease increased the chance of having halitosis. The degree of diagnostic agreement between the two self-perception and organoleptic methods was assessed as moderate to weak.
Acknowledgments
This study was adopted from the doctoral dissertation of Sajjad Hosseinpour, who was a dentistry student at the School of Dentistry, Kermanshah University of Medical Sciences, Kermanshah, Iran (Thesis number: 94569, June 21, 2016). The authors thank the Research and Education Deputy of the university and School of Dentistry, all patients and colleagues who participated in this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Joda A, Olukoju O. Halitosis amongst students in tertiary institutions in Lagos state. Afr Health Sci. 2013;12(4):473–478.
2. Elias MS, Ferriani MGC. Historical and social aspects of halitosis. Outubro. 2006;14(5):821–823.
3. Aylıkcı BU, Çolak H. Halitosis: from diagnosis to management. J Nat Sci Biol Med. 2013;4(1):14. doi:10.4103/0976-9668.107255
4. Bornstein MM, Kislig K, Hoti BB, Seemann R, Lussi A. Prevalence of halitosis in the population of the city of Bern, Switzerland. Eur J Oral Sci. 2009;117(3):261–267. doi:10.1111/j.1600-0722.2009.00630.x
5. Ashwath B, Vijayalakshmi R, Malini S. Self-perceived halitosis and oral hygiene habits among undergraduate dental students. J Indian Soc Periodontol. 2014;18(3):357. doi:10.4103/0972-124X.134575
6. Bollen CM, Beikler T. Halitosis: the multidisciplinary approach. Int J Oral Sci. 2012;4(2):55–63. doi:10.1038/ijos.2012.39
7. Eldarrat A, Alkhabuli J, Malik A. The prevalence of self-reported halitosis and oral hygiene practices among Libyan students and office workers. Libyan J Med. 2008;3(4):170. doi:10.4176/080527
8. Porter S, Scully C. Oral malodour (halitosis). BMJ. 2006;333(7569):632. doi:10.1136/bmj.38954.631968.AE
9. Kim SY, Sim S, Kim S-G, Park B, Choi HG. Prevalence and associated factors of subjective halitosis in Korean adolescents. Public Lib Sci. 2015;10(10):e0140214.
10. Settineri S, Mento C, Gugliotta SC, et al. Self-reported halitosis and emotional state: impact on oral conditions and treatments. Health Qual Life Outcomes. 2010;8:34. doi:10.1186/1477-7525-8-34
11. Brunner F, Kurmann M, Filippi A. The correlation of organoleptic and instrumental halitosis measurements. Schweiz Monatsschr Zahnmed. 2010;120(5):402–405.
12. Alzoubi FQ, Karasneh JA, Daamseh NM. Relationship of psychological and oral health statuses with self-perceived halitosis in a Jordanian population: a cross-sectional study. BMC Oral Health. 2015;15(1):89. doi:10.1186/s12903-015-0078-7
13. Shinada K, Ueno M, Konishi C, et al. Effects of a mouthwash with chlorine dioxide on oral malodor and salivary bacteria: a randomized placebo-controlled 7-day trial. J Trials. 2010;11(1):14. doi:10.1186/1745-6215-11-14
14. Sixou J-L, Magaud C, Jolivet-Gougeon A, Cormier M, Bonnaure-Mallet M. Evaluation of the mandibular third molar pericoronitis flora and its susceptibility to different antibiotics prescribed in France. J Clin Microbiol. 2003;41(12):5794–5797. doi:10.1128/jcm.41.12.5794-5797.2003
15. Youngnak-Piboonratanakit P, Vachirarojpisan T. Prevalence of self-perceived oral malodor in a group of Thai dental patients. J Dent (Tehran). 2010;7(4):196.
16. Ueno M, Yanagisawa T, Shinada K, Ohara S, Kawaguchi Y. Prevalence of oral malodor and related factors among adults in Akita Prefecture. J Med Dent Sci. 2007;54:159–165.
17. Yokoyama S, Ohnuki M, Shinada K, et al. Oral malodor and related factors in Japanese senior high school students. J School Health. 2010;80(7):346–352. doi:10.1111/j.1746-1561.2010.00512.x
18. Al-Ansari JM, Boodai H, Al-Sumait N, Al-Khabbaz AK, Al-Shammari KF, Salako N. Factors associated with self-reported halitosis in Kuwaiti patients. J Dent. 2006;34(7):444–449. doi:10.1016/j.jdent.2005.10.002
19. Hammad MM, Darwazeh AM, Al-Waeli H, Tarakji B, Alhadithy TT. Prevalence and awareness of halitosis in a sample of Jordanian population. J Int Soc Prev Community Dent. 2014;4(Suppl 3):S178. doi:10.4103/2231-0762.149033
20. Liu XN, Shinada K, Chen XC, Zhang BX, Yaegaki K, Kawaguchi Y. Oral malodor‐related parameters in the Chinese general population. J Clin Periodontol. 2006;33(1):31–36. doi:10.1111/j.1600-051X.2005.00862.x
21. Sudarshan R, Sree Vijayabala G, Samata Y, Ravikiran A. Newer classification system for fissured tongue: an epidemiological approach. J Trop Med. 2015;2015:5. doi:10.1155/2015/262079
22. Struch F, Schwahn C, Wallaschofski H, et al. Self-reported halitosis and gastro-esophageal reflux disease in the general population. J Gen Intern Med. 2008;23(3):260–266. doi:10.1007/s11606-007-0486-8
23. Rösing CK, Loesche W. Halitosis: an overview of epidemiology, etiology and clinical management. Braz Oral Res. 2011;25(5):466–471.
24. Cortelli JR, Barbosa MDS, Westphal MA. Halitosis: a review of associated factors and therapeutic approach. Braz Oral Res. 2008;22:44–54.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.