")
Back to Journals » Patient Preference and Adherence » Volume 14
Haemo-Adhaesione: A New Measure of Adherence for Adolescent and Adult Patients with Haemophilia
Authors Torres-Ortuño A , Cuesta-Barriuso R , Nieto-Munuera J, Castiello-Munuera Á, Moreno-Moreno M, López-Pina JA
Received 6 October 2019
Accepted for publication 11 January 2020
Published 3 March 2020 Volume 2020:14 Pages 455—465
DOI https://doi.org/10.2147/PPA.S233601
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Ana Torres-Ortuño,1,2 Rubén Cuesta-Barriuso,3,4 Joaquín Nieto-Munuera,1 Álvaro Castiello-Munuera,1 Manuel Moreno-Moreno,2,4,5 José Antonio López-Pina6
1Department of Psychiatry and Social Psychology, Faculty of Medicine, University of Murcia, Murcia, Spain; 2Association of Hemophilia, Murcia, Spain; 3Department of Physiotherapy, School of Biomedical and Health Sciences, European University of Madrid, Madrid, Spain; 4Royal Foundation Victoria Eugenia, Madrid, Spain; 5Hematology and Hemotherapy Service, University Clinical Hospital Virgen de la Arrixaca, Murcia, Spain; 6Department of Basic Psychology and Methodology, Faculty of Psychology, University of Murcia, Murcia, Spain
Correspondence: Ana Torres-Ortuño
Department of Psychiatry and Social Psychology, Faculty of Medicine, University of Murcia, Campus de Espinardo s/n, 30100, Spain
Tel +34 868887170
Fax +34 913508
Email [email protected]
Purpose: To build a multidimensional questionnaire of adherence for a patient with hemophilia that includes not only clinical but also psychosocial aspects.
Patients and Methods: One hundred and forty-six patients with haemophilia (A and B) were recruited from several Hemophilia Treatment Centers for this study. The recruitment was performed through a personal interview (20– 25 mins for each patient). A literature review was carried out (different databases). In the first version (136 items), all items were subjected to an external judgment (experts in hemophilia) and also presented and discussed with a group of patients. It was made a study of content validity and homogeneity index and reliability coefficients of score were calculated with an alpha coefficient. Empirical validation was made with Pearson correlation.
Results: The Haemo-Adhaesione scale was composed of 5 dimensions and 10 questions about basic haemophilia concepts. It was shown to be valid and reliable to assess adherence in the Spanish population. Its internal consistency was good in all dimensions. The Rasch model was used to confirm the multidimensional structure of the scale. Significant and negative correlations were observed with the VERITAS-Pro and VERITAS-PRN scale in all dimensions, and in the total score.
Conclusions: The Haemo-Adhaesione scale is a good measure of adherence for PWH. Its multidimensional structure favors the inclusion of the objective and subjective aspects implicit in its definition, as well as its dynamic nature. Patients with greater adherence are those who have more awareness of their disease, and as a result, they are more compliant with prescription and their self-care. It also discriminates between patients who follow one treatment or another.
Keywords: hemophilia, adherence, young, adults, scale
Introduction
Haemophilia, a hereditary congenital chronic coagulopathy, entails deficits in the coagulation factors and presents spontaneous or trauma-related muscle or joint bleeding. Its treatment consists of the intravenous administration of the deficit factor in two ways: on-demand or in prophylaxis.1,2 Prophylactic treatment is currently considered as the “gold standard” because it reduces or prevents the presence of bleeding and delays the onset of joint diseases.3–5 The following of treatment is essential to maintain adequate control of the disease and lead a normal life. However, patients do not always follow this recommendation, generating adherence problems and treatment non-efficacy.
Adherence involves a dynamic and multidimensional process.6 That is, it varies over time and depends on multiple factors. The World Health Organization (WHO) defines it as “extent to which a patient’s behaviour coincides with the prescribed health care regimen as agreed through a shared decision-making process between the patient and the health care provider, both from the point view of habits or lifestyles recommended, as well as, prescribed pharmacological treatment”7 It is a problem for not only the patient (ie, treatment ineffectiveness affects their quality of life) but also the entire population, as well as for current and upcoming biomedical advances.
The adherence rates associated with haemophilia vary from 44% to 87% depending on the studies and methods used.8–12 The first studies8,13-15 showed adherence levels between 45% and 60% but with a great variety of methods that were impossible to replicate. Duncan et al.16,17 developed two standardised self-evaluation questionnaires that sought to measure the different components of adherence and the degree of total adherence among patients with haemophilia following a prophylactic treatment or on-demand treatment. Its purpose was to measure the adherence to the instructions given by the professional based on the treatment prescribed (pharmacological).
Recent studies refer to the importance of the assessment of adherence regarding patients’ perceptions or beliefs about their need for treatment, attitudes and motivation, relationships with professionals, and active participation in decision-making.18–22 Thus, the aim of this study was to build a multidimensional questionnaire that included aspects regarding compliance (ie, following the prescribed guidelines, only administer the deficit coagulation factor) and adherence (ie, patient awareness of the disease or the mental representation of their situation, therapeutic alliance, knowledge about the management of relevant clinical processes and consequences of the disease). Both concepts imply that the patients understand the most appropriate behaviour to control their illness and prevent risks, in addition, it is necessary to maintain a positive and regular relationship with their doctor because all of that will encourage them to take care of themselves. Knowledge of conflicts or difficulties in these areas will facilitate interventions to resolve adherence problems and provide treatment continuity and effectiveness.
Materials and Methods
Study Design
A cross-sectional study was conducted with a group of patients with haemophilia (PWH) aged between 15 and 64 years.
Patients
A total of 146 patients with haemophilia (A and B) were recruited for this study of several Haemophilia Treatment Centers (HTC) in Spain. The patients had different degrees of haemophilia (mild, moderate, and severe) and were participating in prophylactic or on-demand treatment. The recruitment was performed through a personal interview. The time spent on it was between 20 and 25 mins for each patient.
Ethics and Consent to Participate
The Ethics Committee of the University of Murcia (School of Medicine) approved this study and the Spanish Agency of Medicines and Medical Devices (Agencia Española de Medicamentos y Productos Sanitarios; AEMPS. Study No-EPA) approved and classified this study as No-EPA (Non-post-authorization observational study). The participants signed an informed consent document (following the Declaration of Helsinki, 1975). The parent or legal guardian of any patient under the age of 18 years provided a written informed consent.
Procedure
The literature was reviewed using the PUBMED, PsycINFO, MEDLINE, and SCOPUS databases. The keywords used were “adherence questionnaires”, “psychometric properties”, “haemophilia”, and “validation”; all keywords were combined with the Boolean operators AND and OR. Given the purpose of our study, our article analysis led us to the most representative dimensions: disease awareness (DA), sequelae knowledge (SK), difficulties with treatment (DT), doctor–patient relationship (DPR), and haemorrhagic processes treatment (HPT). See Appendix 1 for detailed definitions.
In addition, 10 questions addressed basic haemophilia concepts such as disease characteristics, treatment types, complications, and preventive measures to follow its evolution to assess patients’ disease knowledge.
In the first version of the Haemo-Adhaesione questionnaire, 136 items were developed and sent to five expert evaluators in the field of haemophilia with 20 years of experience working in HTCs for an external trial. Each expert individually reported their agreement with the items via qualitative and quantitative judgements using a Likert scale ranging from 0 to 4. In addition, these items were presented and discussed with a group of patients (n = 12). The opinion of the patients was recorded with regard to the difficulty associated with understanding the concepts presented in the items, how patients interpreted each item, and their degree of agreement with the items representing the behaviours to be measured. Item comprehension was also evaluated based on the educational level of the patients (minimal or secondary school level [15 or 16 years]).
A congruency analysis was performed, and the items with the highest level of agreement were selected. The inter-rater agreement ranged between 0.90 and 1.00. Based on the analysis of both experts and patients, 65 items were eliminated. The pilot scale that was administered consisted of 61 items: 16 DA items, 6 SK items, 20 DT items, 7 DPR items, and 11 HPT items, as well as 10 items on knowledge of the disease.
The questions were posed to patients receiving prophylaxis and those receiving on-demand treatments because both should follow specific and scheduled instructions according to their doctor’s prescriptions but in different ways.
Measurements
Other adherence measures were used to validate the Haemo-Adhaesione as follows:
VERITAS-Pro16,32 is a validated adherence measure for prophylactic treatment. This scale consists of 24 items and six subscales: time, dose, plan, remember, skip, and communicate. The potential scores range from 24 to 120, where a low score indicates greater adherence. The estimated cut-off is 38 points, considering the scale’s total score.
VERITAS-PRN17 is a validated adherence measure for on-demand treatment. This scale consists of 24 items and six subscales: time, treatment, dose, plan, remember, and communicate. The potential scores range from 24 to 120, and a low score indicates greater adherence. The estimated cut-off is 38 points, considering the scale’s total score.
Statistical and Psychometric Analyses
Descriptive statistics and item discrimination indices were calculated. To determine metric quality, an interval (0.3–0.7) was used, where a value of 0.30 was used to eliminate the item.
To maintain a balanced number of items for each dimension, the items were classified by the discrimination index. The least discriminative items and those whose wording represented slightly different aspects of the dimension than those intended were eliminated completely.
The internal consistency of the scores for each dimension was assessed with Cronbach’s alpha coefficient.
The scale structure was tested with a multidimensional version of the rating scale model.23 The items followed the specified model if their infit and outfit statistics fell within the interval [0.6–1.4].
A convergent validity study was performed to assess the correlations between the dimensions of the constructed scale and the VERITAS-Pro and VERITAS-PRN scales. In addition, empirical validity was determined via Student’s t-test and an ANOVA. The effect size (ES) was assessed using Cohen’s d standardised mean difference (where small, medium, and large ESs are 0.20, 0.50, and 0.80, respectively) or ω2 (where small, medium, and large values are 0.01, 0.06, and 0.14, respectively). All analyses were performed using SPSS v. 19.0 and ConQuest v. 4.0.24
Results
The age of the patients ranged from 15 to 64 years old (Mean = 40.0; SD = 11.5). A total of 120 (82.2%) patients had type A haemophilia, and 26 (17.8%) had type B haemophilia; 10 cases (6.8%) were mild, 46 cases (31.5%) were moderate, and 90 cases (61.6%) were severe. A total of 62 patients (42.5%) were receiving on-demand treatment, and 84 (57.5%) were receiving prophylaxis. In addition, 11 (7.5%) patients developed an inhibitor, 93 (63.7%) had a family history of haemophilia, 92 (63%) had hemarthrosis, 123 (84.2%) developed a joint disease, 19 (13%) needed an orthotic, and 89 (61%) had co-infections with HCV, HIV, or both. See Table 1.
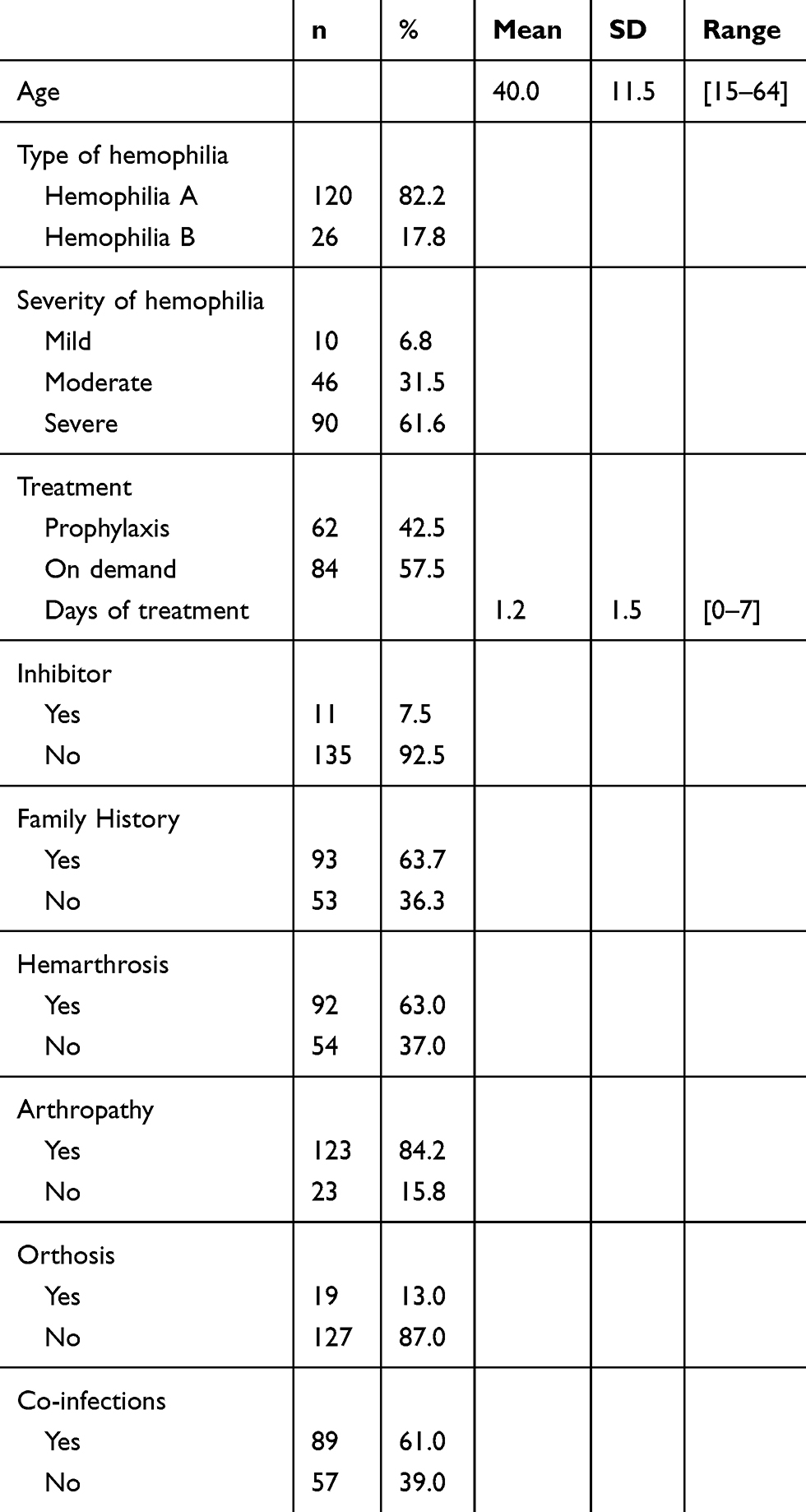 |
Table 1 Sociodemographic and Clinical Characteristics of the Patients |
Item Analysis
Table 2 shows the means, standard deviations, and homogeneity indices of the dimensions of the proposed adherence scale. The items that were selected for the final scale based on the statistics applied and the expert judgement of the research team appear in bold. We attempted to maintain a balance between the five dimensions of the scale so that the DA dimension was composed of six items, the SK dimension was composed of four items, the DT dimension was composed of five items, the DPR dimension was composed of five items, and the HPT dimension was composed of five items. The final scale appears in Appendix 2. The knowledge of the disease dimension was not a part of the final scale because between 99% and 100% of patients answered all items correctly.
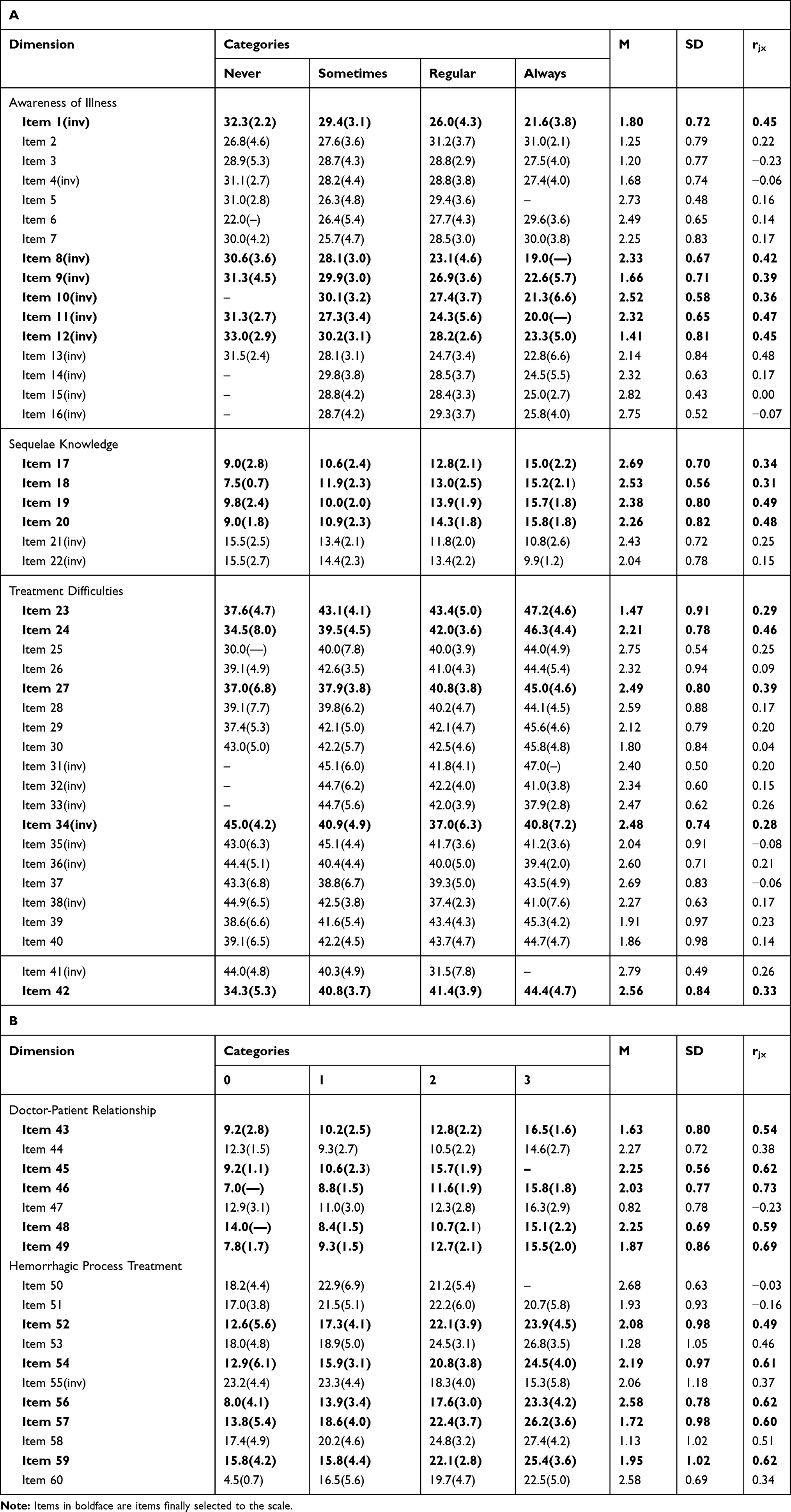 |
Table 2 Mean (SD) in Each Category of Total Scores, Mean (M), Standard Deviation (SD) and Homogeneity Index of the Items |
Haemo-Adhaesione scores
Table 3 presents the descriptive statistics and the alpha coefficients of the five dimensions. No floor effect was observed with regard to any dimension, although ceiling effects were found for DT (28.1%) and DPR (17.1%), which might have partially reduced the reliability of the scores. All dimensions obtained reliability coefficients above 0.70, except for the DT dimension, which had a relatively low value (0.56); however, this value was noticeable depending on the number of items used to obtain it.
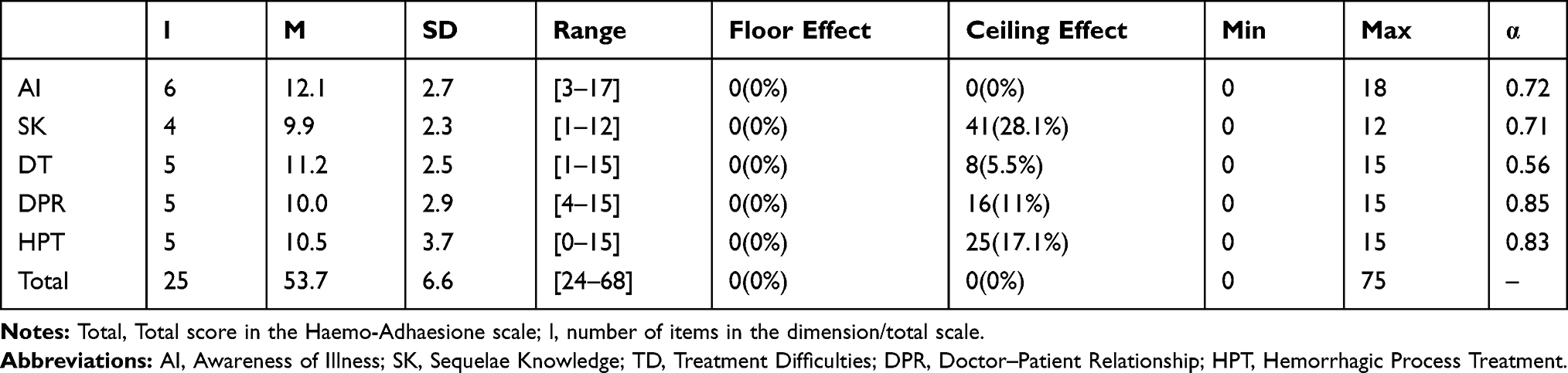 |
Table 3 Descriptive Statistics and Reliability Coefficients of the Five Dimensions of the Haemo-Adhaesione |
The correlations between all dimensions were significant, except for DA, which was not correlated with the other scale dimensions. The correlations of the dimensions of the Haemo-Adhaesione scale with the VERITAS-Pro scale were significant and negative, given that the latter scale assesses adherence in the opposite direction. In this sense, DA was significantly correlated with dose (p < 0.05), plan (p < 0.001), and the total score (p < 0.05). SK was significantly correlated with plan (p < 0.05). DT was significantly correlated with plan (p < 0.05), remember (p < 0.01), skip (p < 0.01), communicate (p < 0.01), and the total score (p < 0.001). DPR was significantly correlated with remember (p < 0.01), skip (p < 0.05), communicate (p < 0.001) and the total score (p < 0.05), and the total score was significantly correlated with time (p < 0.05), plan (p < 0.001), skip (p < 0.01), communicate (p < 0.05), and the total VERITAS-Pro score (p < 0.01).See Tables 4 and 5.
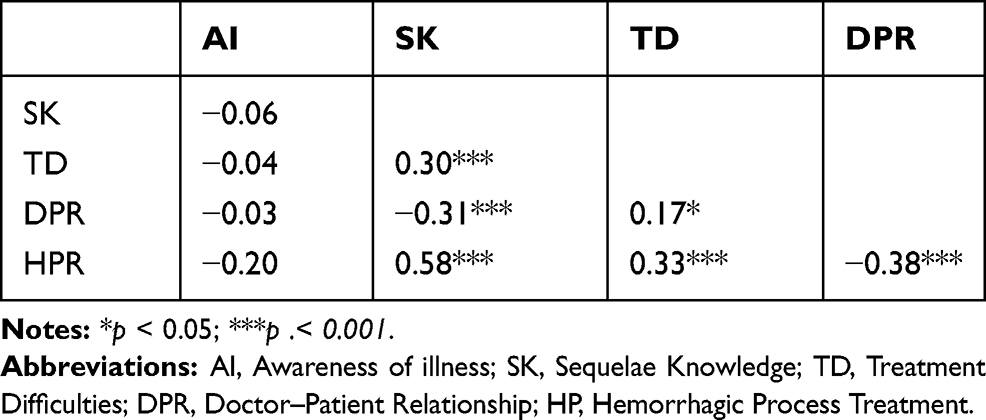 |
Table 4 Pearson Correlation Between Dimensions of Adherence Scale |
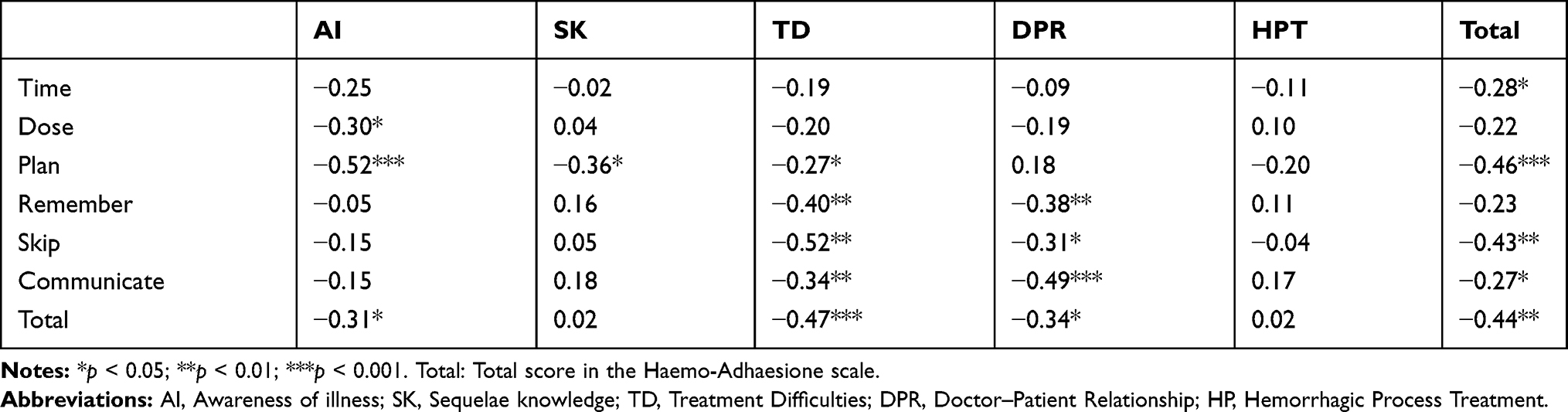 |
Table 5 Pearson Correlation Between Adherence Dimensions and VERITAS-Pro Scale |
The Haemo-Adhaesione scale was also negatively and significantly correlated with the VERITAS-PRN scale (see Table 6), except with regard to the DA dimension. The SK dimension was significantly correlated with treatment (p < 0.05), time (p < 0.001), plan (p < 0.001), remember (p < 0.01), and the total score (p < 0.001). The DT dimension was significantly correlated with treatment (p < 0.05), time (p < 0.001), plan (p < 0.001), and the total score (p < 0.001). The DPR dimensions were significantly correlated with time (p < 0.001) and remember (p < 0.01). The HPT dimension was significantly correlated with treatment (p < 0.001), time (p < 0.001), plan (p < 0.001), remember (p < 0.001), and the total score (p < 0.001). Finally, the total score was significantly correlated with treatment (p < 0.001), time (p < 0.001), plan (p < 0.001), remember (p < 0.05), and the total VERITAS-PRN score (p < 0.001).
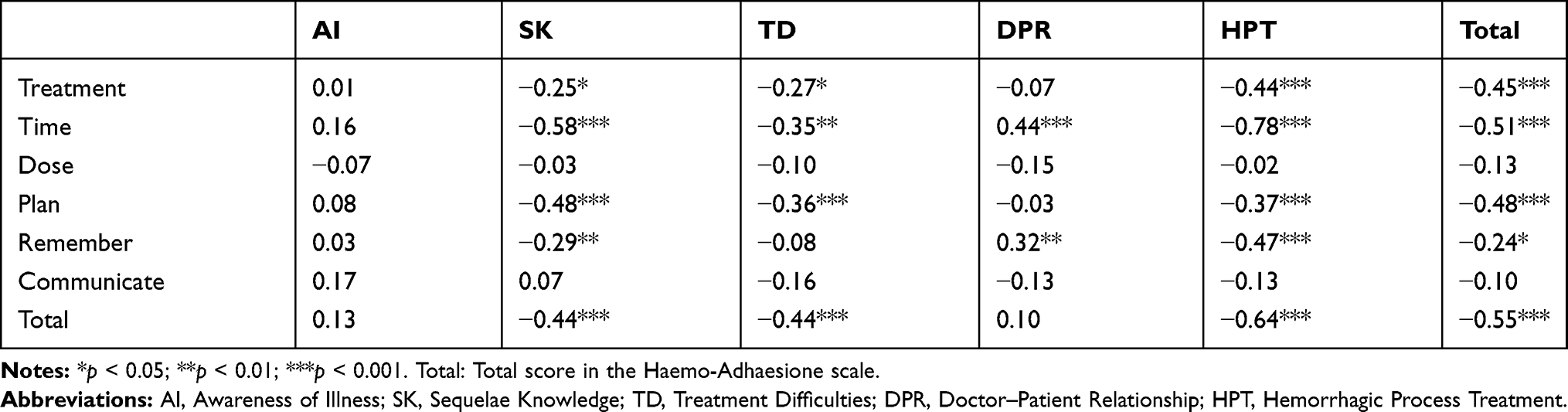 |
Table 6 Pearson Correlation Between Adherence Dimensions and Veritas-PRN Scale |
Structural Validity
To confirm the multidimensional structure of the Haemo-Adhaesione scale, a multidimensional Rating Scale Model was applied. The parameter estimations and fit statistics appear in Table 7. All but items 14 and 15 on the DT dimension were associated with fit statistics within the range expected by the model. The parameter separation index (0.99) was sufficiently high, indicating an adequate separation of the items used to assess treatment adherence across the five specified dimensions. In addition, the categories were in order and sufficiently separated (δ1= −1.701, δ2= 0.071, δ3= 1.629), showing that the number of categories used in this scale worked properly.
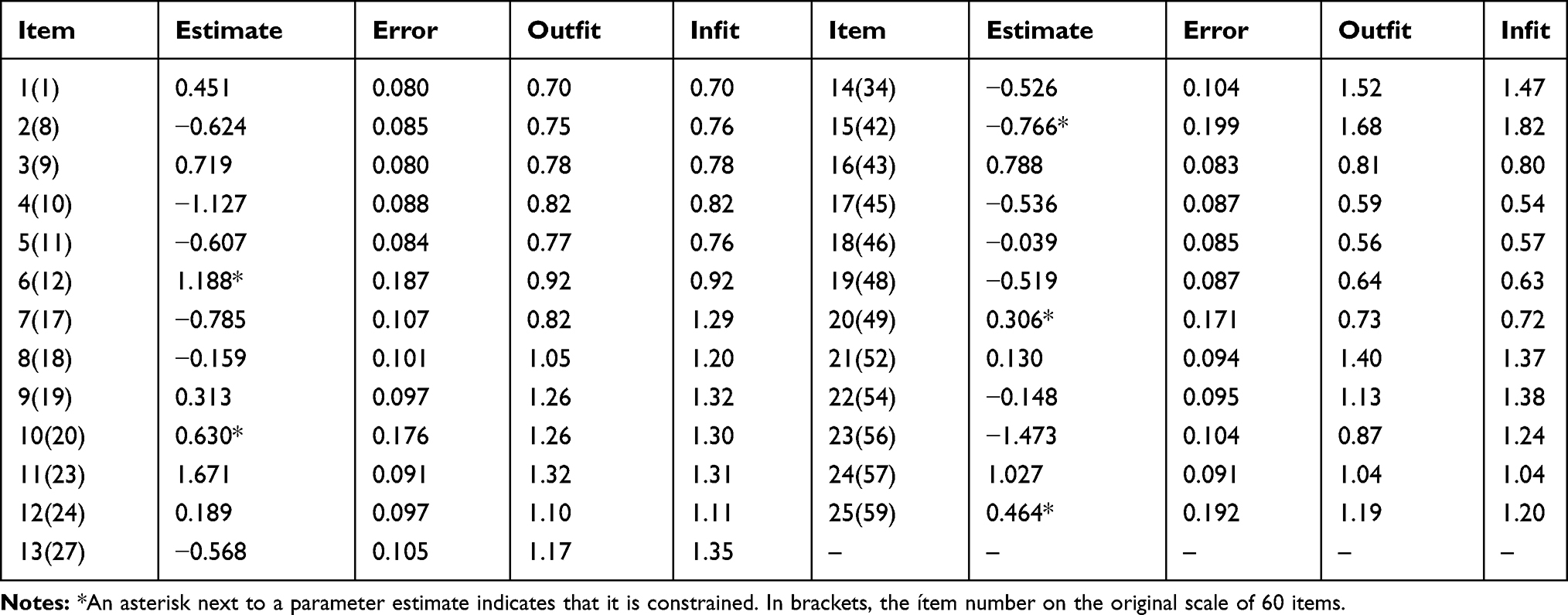 |
Table 7 Parameter Estimation and Goodness-of-Fit Statistics of Haemo-Adhaesione Scale |
Empirical Validity
No significant differences were found with regard to any of the dimensions or the total score based on the type of haemophilia.
The patients receiving prophylaxis showed higher DT (ES = 0.37) scores than those receiving on-demand treatment. The latter showed better management with regard to HPT than patients on prophylaxis (ES = −0.51). Patients with moderate haemophilia showed better SK (ES = 0.13) scores than patients with mild or severe haemophilia. In addition, patients with severe or moderate haemophilia showed higher DT (ES = 0.25) scores than those with mild haemophilia, whereas patients with moderate haemophilia showed better HPT management (ES = 0.15).
In general, patients with inhibitors show better DPR (ES = 1.04) scores than those who did not. However, patients with a family history of haemophilia showed more DT (ES = −0.38) than those without. Patients with hemarthrosis showed lower DA (ES = −0.35) scores than those without. Patients with joint disease showed higher SK (ES = 0.98) scores, a worse PMR ratio (ES = −0.59), and better HPT (ES = 1.21) scores. However, patients with co-infections showed better SK (ES = 0.50) and HPT (ES = 0.95) scores. Finally, patients with orthosis showed better PMR (ES = 0.81) scores than those without orthosis. See Table 8.
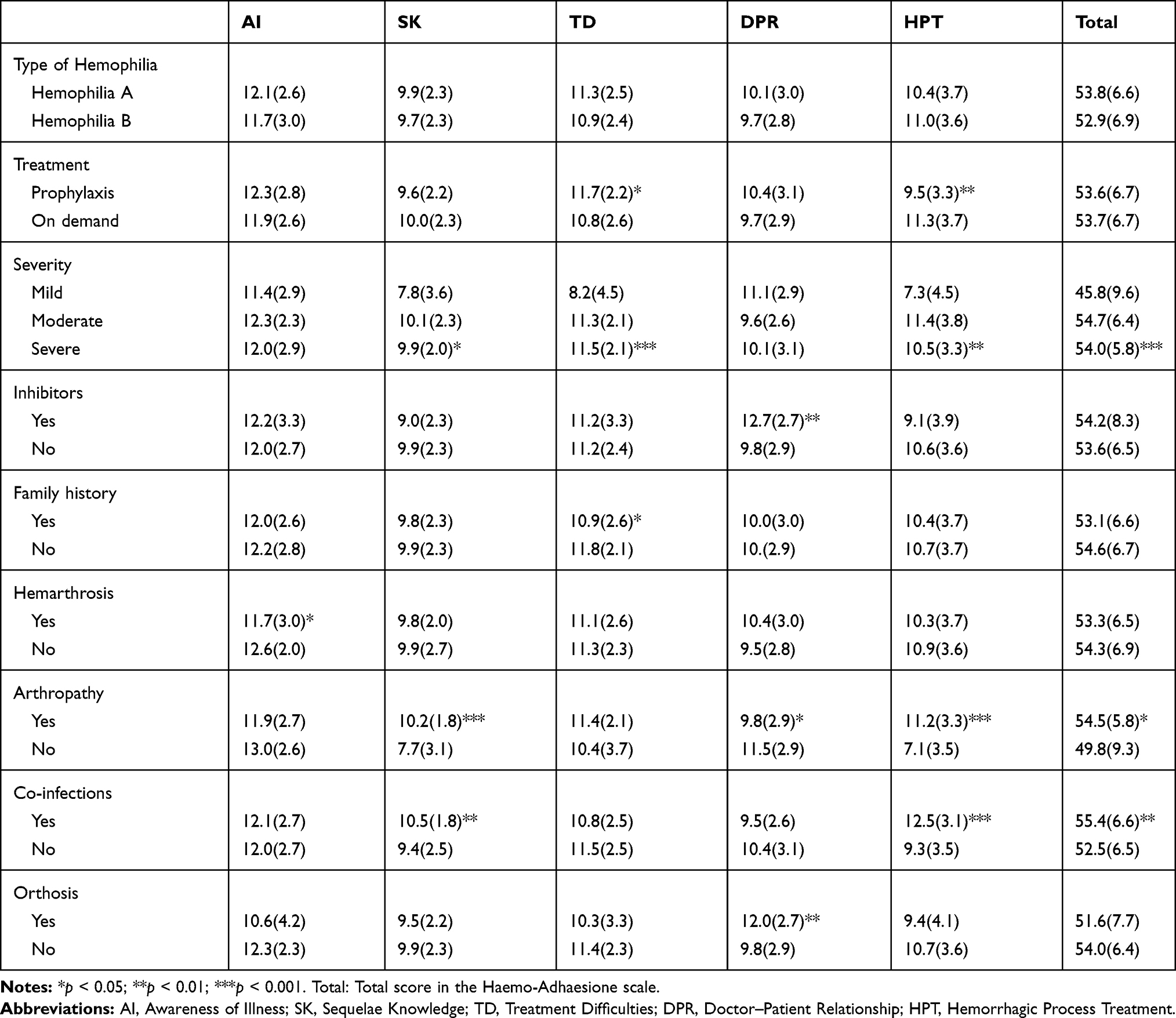 |
Table 8 Mean (SD) of the Dimensions of Veritas-PRN |
Discussion
The results obtained showed a high degree of adherence and between 99% and 100% of patients showed adequate knowledge of their haemophilia and its treatment. The degree of adherence found was similar to that in recent studies.11,12,21,22
The Haemo-Adhaesione scale was valid and reliable for assessing adherence among the Spanish population. Its internal consistency was acceptable for all dimensions, except DT, which might have been because of the number of items used. In addition, a ceiling effect was observed with regard to the dimensions DT and DPR, which indicates that difficulties can be experienced when discriminating between patients.
The Rasch model showed that all items except items 14 and 15 of the DT dimension had a satisfactory fit to the model.
Negative significant correlations were observed with regard to all dimensions and the total scores of the VERITAS-Pro and VERITAS-PRN scales. Adherence among patients with haemophilia is based on not only compliance with the professional’s prescriptions but also psychological aspects such as awareness of the disease and the relationship with the professional (the patient shows an agreement and commitment with to his health).18–22
All of the Haemo-Adhaesione dimensions were correlated with those of the VERITAS-Pro, except for HPT. Patients receiving prophylaxis showed satisfactory adherence, planned their treatment without omissions, and followed the indications of the professional, with whom they had a positive relationship. They also expressed adequate awareness of their disease due to their behaviours correlated with the advice that professional pointed out in order to manage his disease. Their lack of attention to haemorrhagic processes might be understood based on the finding that their treatment reduces the appearance of these symptoms, thereby decreasing worry. This aspect is important to consider with regard to adherence.28
All of the dimensions of the VERITAS-PRN were correlated, except for DA. Patients receiving on-demand treatment showed satisfactory treatment adherence. Their lower disease awareness might be conditioned by the low (mild) symptomatology which they typically present. Therefore, some authors25–27 have warned of the importance of raising awareness and educating these patients to prevent future difficulties because of their lack of attention to their disease.
Significant differences were found with regard to the dimension HPT. Patients receiving on-demand treatment were more likely to adhere than those receiving prophylaxis. This result might be because they felt less secure or protected from the disease and therefore paid more attention to their treatment when symptoms appeared.18
Patients with moderate haemophilia were more adherent with regard to the dimensions SK and HPT; however, patients with severe symptoms were more adherent with regard to the total score. Patients with severe haemophilia had the highest total score (most adherent). In addition, both cases coincide with a diagnosis of joint disease and the presence of co-infections. Given the mean age of the sample, it is unlikely that many patients with arthropathy and co-infections had not received prophylaxis with their first treatments which have had an impact on adulthood. Although they now receive more effective treatments, joint damage is already established.14,18,19,21,28
Patients with inhibitors showed greater adherence with regard to the DPR dimension. Additionally, these patients used orthopaedic devices for proper functionality in their daily lives, unsurprisingly because they presented with more difficulties associated with the disease. This finding might be a reason to abandon treatment. However, these patients visit their doctor, they believe that professionals help them to solve their problems, and this promotes adherence. Therefore, a positive therapeutic alliance is relevant for patients to follow treatments. In chronic care, it is difficult to implement treatment without considering the patient’s interpretations, preferences, feelings, concerns, needs, values, and social context.29,30
Patients with a family history of haemophilia showed greater difficulties with treatment. Inheritance is not a guarantee of better control. According to how the past experience has been lived, it may be conditioned for or against the future view of the new generations. In addition, the first effective factor concentrates did not appear until the 1970s and the subsequent emergence of the HIV and HCV infections in the 1980s (especially the latter) caused rejection and distrust among the patients. Patients should follow recommended treatments if they want to be well and have a life of quality. But we cannot forget that adverse circumstances experienced personally or by others may influence patient response. Thus, improving and adapting communication to patients’ demands and needs might help to enable a successful cohabitation with the disease and motivate them to change wrong behaviours. Thereby, every day, it is more evident that treatments (prophylaxis or on-demand) should be personalised.31
Strengths and Limitations
One limitation of our study might be the ceiling effect regarding the dimensions DT and DPR, which could be improved (specifically, items 14 and 15). Another limitation might be the small sample size. However, the recruitment via personal interview, which facilitated the correct and complete data collection, must be considered. Furthermore, the PWH census of all of Spain via random selection suggests that the data are representative.
Conclusions
The Haemo-Adhaesione scale is a satisfactory measure of patient adherence to haemophilia. Its multidimensional structure favours the inclusion of the objective and subjective aspects implicit in its definition. We believe that the inclusion of the additional measure on the scale regarding patient knowledge about treatment and disease is adequate. Patients with greater adherence are more aware of their symptoms, which favours their involvement in following the guidelines indicated on a regular basis. This scale also discriminates among patients who follow different treatments. Most importantly, it helps professionals consider what action to take for dealing with non-adherence, emphasising that psychosocial aspects condition patient responses to maintain treatment success. The clinical signs of haemophilia are relevant, but new treatments that reduce the number of treatment days and symptoms can lead patients to “forget” the disease and show consequently inadequate adherence. Therefore, these psychosocial aspects play a determining role in adherence.
Acknowledgment
The authors are grateful to the Hemophilia Associations´ patients in Spain for their help in recruiting the sample and to the professional of Haemophilia Treatment Centers who have collaborated as external judges.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work. The authors state that this work has received Investigator-Initiated Research grant from Baxalta US Inc., now part of Takeda group of companies, Bannockburn, IL.
References
1. Colvin BT, Astermark J, Fischer K, et al. European principles of haemophilia care. Haemophilia. 2008;14(2):361–374. doi:10.1111/hae.2008.14.issue-2
2. Srivastava A, Brewer AK, Mauser-Bunschoten EP, et al. Guidelines for the management of hemophilia. Haemophilia. 2013;19:e1–e47.
3. Berntorp E, Astermark J, Björkman S, et al. Consensus perspectives on prophylactic therapy for haemophilia: summary statement. Haemophilia. 2003;9(Suppl 1):1–4. doi:10.1046/j.1365-2516.9.s1.17.x
4. MJ M-J, TC A, AD S, et al. Prophylaxis versus episodic treatment to prevent joint disease in boys with severe hemophilia. N Engl J Med. 2007;357(6):535–544. doi:10.1056/NEJMoa067659
5. Valentino LA, Mamonov V, Hellmann A, et al. A randomized comparison of two prophylaxis regimens and a paired comparison of on-demand and prophylaxis treatments in hemophilia A management. J Thromb Haemost. 2012;10(3):359–367. doi:10.1111/j.1538-7836.2011.04611.x
6. Haynes RB. Compliance in health care. In: Haynes RB, Taylor DW, Sackett DL, editors. . Introduction. Baltimore: Johns Hopkins University Press; 1979.
7. World Health Organization. Adherence to Long-Term Therapies: Evidence for Action. World Health Organization; 2009.
8. De Moerloose P, Urbancik W, Van den Berg HM, Richards M. A survey of adherence to haemophilia therapy in six countries: results and recommendations. Haemophilia. 2008;14:931–938. doi:10.1111/j.1365-2516.2008.01843.x
9. Duncan N, Shapiro A, Ye X, Epstein J, Luo MP. Treatment patterns, health-related quality of life and adherence to prophylaxis among haemophilia A patients in the United States. Haemophilia. 2012;18(5):760–765. doi:10.1111/hae.2012.18.issue-5
10. Lock J, Raat H, Duncan N, et al. Adherence to treatment in a Western European paediatric population with haemophilia: reliability and validity of the VERITAS-Pro scale. Haemophilia. 2014;20:616–623. doi:10.1111/hae.2014.20.issue-5
11. Miesbach W, Kalnins W. Adherence to prophylaxis treatment in patients with haemophilia in Germany. Haemophilia. 2016;22(5):e367–e374. doi:10.1111/hae.13003
12. Schrijvers LH, Beijlevelt‐van der Zande M, Peters M, et al. Adherence to prophylaxis and bleeding outcome in haemophilia: a multicenter study. Br J Haematol. 2016;174:454–460. doi:10.1111/bjh.14072
13. Hacker MR, Geraghty S, Manco-Johnson M. Barriers to compliance with prophylaxis therapy in haemophilia. Haemophilia. 2001;7:392–396. doi:10.1046/j.1365-2516.2001.00534.x
14. Llewellyn CD, Miners CD, Lee CA, Harrington C, Weinman J. The illness perceptions and treatment beliefs of individuals with severe haemophilia and their role in adherence to home treatment. Psychol Health. 2003;18:185–200. doi:10.1080/0887044031000098198
15. du Treil S, Rice J, Leissinger CA. Quantifying adherence to treatment and its relationship to quality of life in a well-characterized haemophilia population. Haemophilia. 2007;13:493–501. doi:10.1111/j.1365-2516.2007.01526.x
16. Duncan N, Kronenberger W, Roberson C, et al. VERITAS-Pro: a new measure of adherence to prophylactic regimens in haemophilia. Haemophilia. 2010;16:247–255. doi:10.1111/j.1365-2516.2009.02129.x
17. Duncan N, Kronenberger W, Roberson C, Shapiro A. VERITAS-PRN: a new measure of adherence to episodic treatment regimens in haemophilia. Haemophilia. 2010;16(1):47–53. doi:10.1111/hae.2009.16.issue-1
18. Lamiani G, Strada I, Mancusa ME, Coppola A, Vegni E, Moja EA; Pro-adherence study group. Factors influencing illness representations and perceived adherence in haemophilic patients: a pilot study. Haemophilia. 2015;21::598–604. doi:10.1111/hae.12654
19. Schrijvers LH, Schuurmans MJ, Fischer K. Promoting self-management and adherence during prophylaxis: evidence-based recommendations for haemophilia professionals. Haemophilia. 2016;22:499–506. doi:10.1111/hae.2016.22.issue-4
20. Thornburg CD, Duncan NA. Treatment adherence in hemophilia. Patient Prefer Adherence. 2017;11:1677–1686. doi:10.2147/PPA
21. van Os SB, Troop NA, Sullivan KR, Hart DP. Adherence to prophylaxis in adolescent and young adults with severe haemophilia: a quantitative study with patients. PLoS One. 2017;12(1):e0169880. doi:10.1371/journal.pone.0169880
22. Lamiani G, Bigi S, Mancuso ME, Coppola A, Vegni E. Applying a deliberation model to the analysis of consultations in haemophilia: implications for doctor-patient communication. Patient Educ Couns. 2017;100(4):690–695. doi:10.1016/j.pec.2016.11.021
23. Andrich D. A rating formulation for ordered response categories. Psychometrika. 1978;43:561–573. doi:10.1007/BF02293814
24. Wu ML, Adams RJ, Wilson MR, Haldane SA. AcerConquest v 2.0. ACER; 2007.
25. Lindvall K, Colstrup L, Loogna K, Wollter IM, Grönhaug S. Knowledge of disease and adherence in adult patients with haemophilia. Haemophilia. 2010;16:592–596. doi:10.1111/j.1365-2516.2009.02189.x
26. Nilson J, Schachter C, Mulder K, et al. A qualitative study identifying the knowledge, attitudes and behaviours of young men with mild haemophilia. Haemophilia. 2012;18:e120–e125. doi:10.1111/hae.2012.18.issue-3
27. Arnold E, Lane S, Weber KE, et al. What should men living with haemophilia need to know? The perspectives of Canadian men with haemophilia. Haemophilia. 2014;20:219–225. doi:10.1111/hae.2014.20.issue-2
28. Schrijvers LH, Uitslager N, Schuurmans MJ, Fischer K. Barriers and motivators of adherence to prophylactic treatment in haemophilia: a systematic review. Haemophilia. 2013;19(1):35–43. doi:10.1111/hae.12079
29. Zolnierek KB, Dimatteo MR. Physician communication and patient adherence to treatment: a meta-analysis. Med Care. 2009;47:826–834. doi:10.1097/MLR.0b013e31819a5acc
30. Bigi S. Key components of effective collaborative goal setting in the chronic care encounter. Commun Med. 2014;11(2):103–115. doi:10.1558/cam.v11i2.21600
31. Recht M, Konkle BA, Jackson S, Neufeld EJ, Rockwood K, Pipe S. Recognizing the need for personalization of haemophilia patient-reported outcomes in the prophylaxis era. Haemophilia. 2016;22:825–832. doi:10.1111/hae.2016.22.issue-6
32. Cuesta-Barriuso R, Torres-Ortuño A, Galindo-Piñana P, Nieto-Munuera J, Duncan N, López-Pina JA. Validation of the VERITAS-Pro treatment adherence scale in a Spanish sample population with hemophilia. Patient Prefer Adherence. 2017;11:653–660. doi:10.2147/PPA.S126828
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.