")
Back to Journals » Clinical Interventions in Aging » Volume 11
Habitual cocoa intake reduces arterial stiffness in postmenopausal women regardless of intake frequency: a randomized parallel-group study
Authors Okamoto T, Kobayashi R, Natsume M, Nakazato K
Received 26 July 2016
Accepted for publication 15 October 2016
Published 14 November 2016 Volume 2016:11 Pages 1645—1652
DOI https://doi.org/10.2147/CIA.S118152
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Richard Walker
Takanobu Okamoto,1 Ryota Kobayashi,1 Midori Natsume,2 Koichi Nakazato1
1Department of Exercise Physiology, Nippon Sport Science University, Tokyo, Japan; 2Food Sciences Research Laboratories, Meiji Co Ltd, Kanagawa, Japan
Abstract: Arterial stiffness is substantially higher in postmenopausal than in premenopausal women. Daily cocoa intake has been shown to reduce central arterial stiffness in health adults, regardless of age; however, the effect of cocoa-intake frequency on arterial stiffness in postmenopausal women remains unclear. Therefore, the purpose of this study was to investigate the effects of cocoa-intake frequency on arterial stiffness in postmenopausal women. A total of 26 postmenopausal women (mean age ± standard deviation 64±12 years) were randomly assigned to two groups with different cocoa-intake frequencies: one group ingested 17 g of cocoa once daily except on Sundays (every-day group, n=13), and the other ingested 17 g of cocoa twice daily every other day (every-other-day group, n=13). These intake regimens were maintained in both groups for 12 weeks. Carotid–femoral pulse-wave velocity and femoral–ankle pulse-wave velocity were measured in both groups at baseline and again at the end of the 12-week study period. Compared to baseline, both pulse-wave velocities had significantly decreased after the 12-week study period in both groups (P<0.05). However, no significant difference in degree of change was observed between the two groups. Although this study did not include a sedentary control group, these results suggest that regardless of frequency, habitual cocoa intake reduces central and peripheral arterial stiffness in postmenopausal women.
Keywords: flavanol-enriched cocoa, pulse-wave velocity, intake frequency, endothelin 1
Introduction
Increased arterial stiffness, as assessed by pulse-wave velocity (PWV), has been shown to be associated with increased risk for initial and subsequent cardiovascular events, as well as mortality,1,2 and aortic stiffness, as assessed by aortic PWV, has been shown to be a powerful predictor of future cardiovascular events and all-cause mortality.3 Increased aortic stiffness impairs arterial buffering function and coronary perfusion, and contributes to an increase in systolic blood pressure (SBP) and the development of left ventricular hypertrophy.4–6 Menopause has been shown to be a risk factor for increased arterial stiffness, and is thus associated with an increased risk of cardiovascular disease (CVD) in postmenopausal women.7 Compared with their postmenopausal normotensive counterparts, postmenopausal prehypertensive women are more likely to develop myocardial infarction, stroke, and heart failure and experience cardiovascular death.8 Therefore, it is important to seek strategies that prevent or limit increased arterial stiffness among postmenopausal women.
Acute and habitual intake of flavanol-enriched cocoa and/or dark chocolate was reported to increase flow-mediated vasodilator response, thereby effectively lowering blood pressure (BP).9,10 In addition, associations have been reported between habitual cocoa and/or dark-chocolate intake and reduced BP, antioxidant effects, improved blood-lipid profiles, and reduced endothelin (ET)-1 vasoconstrictor activity.10–12 These findings indicate that habitual intake of flavanol-enriched cocoa and/or dark chocolate may have a number of beneficial effects on cardiovascular health. Furthermore, habitual cocoa intake has been shown to reduce central arterial stiffness in healthy young, middle-aged,13 and older adults,10,14 and an association has been found between habitual intake of flavanol-enriched cocoa and improved vascular endothelial function in hypercholesterolemic postmenopausal women.15 Although participants in many previous studies ingested cocoa on a daily basis, daily cocoa intake may be unnecessary to achieve the associated cardiovascular benefits, which range in duration from a few hours to a few days.16–20 Unfortunately, to our knowledge, no previous studies have investigated the effects of various cocoa-intake frequencies on arterial stiffness.
This study investigated the effects of differences in cocoa-intake frequency on arterial stiffness in a randomized, uncontrolled, parallel-group study in postmenopausal women. We hypothesized that habitual cocoa intake would reduce arterial stiffness in postmenopausal women if intake dose per week was the same, regardless of intake frequency.
Subjects and methods
Study participants
The study participants were 26 healthy postmenopausal women (aged 64±2 years) who did not actively engage in regular physical exercise, were normotensive (BP <140/90 mmHg), nonsmokers, and had no signs, symptoms, or history of any overt chronic diseases. Those who were currently taking antihyperlipidemic, antihypertensive, or antihyperglycemic medications or undergoing hormone-replacement therapy were excluded. Postmenopausal status was defined as more than 1 year since the last menstrual period. The study protocol was approved by the ethics committee of Nippon Sport Science University (013–H56). Written informed consent was obtained from all participants after providing explanations of the potential risks of the study in detail.
Study design
Measurements were obtained at baseline and again at the end of the 12-week study period. After the baseline measurements, participants were randomly assigned to groups that ingested cocoa either every day (every-day group, n=13) or every other day (every-other-day group, n=13). All participants were asked to maintain their regular activity levels, dietary habits, and sleep routines, and to avoid supplements and all other cocoa products throughout the 12-week study period. They were also instructed to abstain from caffeine and alcohol for at least 24 hours and to fast for at least 10–14 hours overnight for vascular measurements and blood collections. All measurements were recorded in a quiet room at a constant temperature (23°C–25°C) after the participants had been resting in a supine position for at least 20 minutes. To avoid the effects of diurnal variation, all measurements were recorded at the same time of day throughout the study period. All participants completed the experiment.
Cocoa intake
Partially fermented and dried cocoa beans were roasted, cracked, and compressed to prepare cocoa powder. The total flavan-3–ol (ie, flavanol) content of the cocoa was determined by the Prussian blue method using epicatechin as the standard.21 To remove most of the fats, the cocoa (10 g) was triturated for 30 minutes with a fivefold volume of room-temperature n-hexane three times. Next, the defatted cocoa (0.5 g) was extracted twice at 80°C with a 100-fold volume of 50% aqueous methanol (v/v). The resulting solution, containing nearly all of the extracted flavanols (catechins and procyanidins), was then diluted to 100 mL with 50% methanol (v/v). This final solution was used in the subsequent high-performance liquid chromatography (HPLC) analysis. Next, a partially modified HPLC method was used to quantify the catechin, epicatechin, procyanidin B2, and procyanidin C1 content in the powder as epicatechin equivalents.22 All reagents used in the study were of analytical and HPLC grade and commercially available (Meiji Co Ltd, Tokyo, Japan). To prepare the experimental cocoa drink used as the cocoa intake in the study, the subject transferred the cocoa from the bulk cocoa powder into a cup using a measuring spoon. Prior to consumption, the cocoa powder was mixed with 120 mL of hot water. The subjects were directed to take the cocoa only after mixing with water. Adding milk or sugar was not allowed. The composition of the cocoa beverage is shown in Table 1. The every-day group ingested 17 g of cocoa, excluding Sundays, for 12 weeks, while the every-other-day group ingested 17 g of cocoa twice daily (once before and once after noon), 3 days (Monday, Wednesday, and Friday) a week for 12 weeks. We prohibited the intake of such beverages as green tea and/or dietary supplements that included polyphenols during the 12 weeks of the study. Compliance with cocoa intake was confirmed by regular email or telephone contact. No restrictions were placed on food intake, but all participants were given clear instructions to maintain their normal diets throughout the study period. Furthermore, all participants were asked to keep food diaries throughout the duration of the study, which were subsequently verified by food-frequency questionnaires, to ensure that they had maintained their regular diets. Cocoa intake took place from September to December 2014.
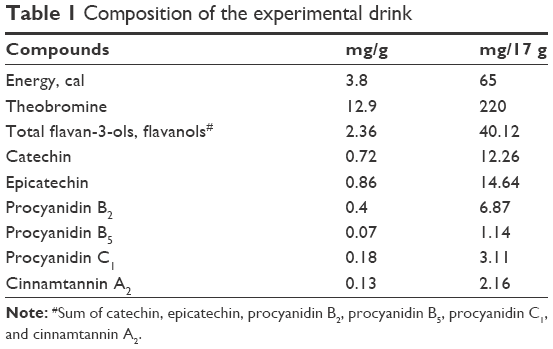 | Table 1 Composition of the experimental drink |
Body composition
The body composition of the participants was determined by bioelectric impedance using a body-composition analyzer (InBody770; Biospace Co Ltd, Seoul, South Korea).
Pulse-wave velocity
Carotid–femoral PWV (cfPWV) and femoral–ankle PWV (faPWV), which reflect aortic and leg arterial stiffness, respectively, were measured as previously described.23 Carotid and femoral artery-pressure waveforms were obtained for 30 seconds using arterial applanation tonometry incorporating form PWV/ABI micropiezoresistive transducers (Omron-Colin Co Ltd, Tokyo, Japan), which comprise 15 aligned pressure-sensitive elements that can identify carotid and femoral pulse traces, arranged side by side and attached to the left common carotid and femoral arteries, respectively. A vascular testing device (form PWV/ABI; Omron-Colin) was then used to measure simultaneously electrocardiograms, bilateral brachial and ankle BP, and carotid and femoral arterial pulse waves (PWs) . cfPWV and faPWV were calculated by dividing the distance between the two arterial recording sites by the transit time, which was determined based on the time delay between the proximal and distal “foot” waveforms. faPWV was calculated based on the transit time between the femoral artery site and the ankle site. Next, time delays were obtained from between the right brachial and posttibial arteries, the carotid and femoral arteries (Tcf), and the femoral and posttibial arteries. A nonelastic tape measure was then used to make duplicate random zero-length measurements over the body surface in order to determine the path length from the carotid to the femoral artery (Dcf). cfPWV was then calculated using the following equation:
cfPWV = Dcf/Tcf | (1) |
The investigator who performed the PWV measurements was blinded to the group assignment of the participants.
Cardiovascular indices
During waveform recording, normal resting levels of heart rate and brachial and ankle SBP and diastolic BP (DBP) were simultaneously measured using electrocardiography and an automatic oscillometric device (form PWV/ABI), respectively. Data were recorded in triplicate with participants in the supine position. The pressure signal obtained using plethysmography was calibrated by equating SBP and DBP values, and then used to calculate mean arterial pressure (MAP).
Plasma ET1 concentration
Blood samples were collected from the ulnar vein of the nondominant arm (nonactive limb) of each participant using a Vacutainer with ethylenediaminetetraacetic acid–2Na and Trasylol. After 1 mL of distilled water had been added, all samples were centrifuged at 4,000 RCF for 15 minutes. The counts of each sample were plotted against a standard curve with known concentrations of ET1 to determine plasma ET1 concentrations. Plasma ET1 was concentrated by extraction through a preparative C18 cartridge (Waters, Milford, MA, USA), and pretreated with 60% acetonitrile–0.1% trifluoroacetic acid. Supernatants were then acidified with 3 mL of 4% glacial acetic acid and loaded on the columns, after which each column was eluted with a mixture of 4% glacial acetic acid and 40% ethanol. Eluates were then evaporated to dryness in a 37°C water bath, reconstituted with 0.5 mL of assay buffer, and subjected to sandwich enzyme-linked immunosorbent assay. Next, 0.2 mL of each sample was incubated with 0.1 mL of 123I-ET1 and 0.1 mL of rabbit anti-ET serum for 18 hours at 2°C–8°C. Finally, 0.1 mL of donkey antirabbit Ig-coated cellulose was added, and incubation was carried out for another 20–30 minutes at room temperature. Plasma ET1 concentrations were quantified using an ET1 enzyme-linked immunosorbent assay (R&D Systems, Minneapolis, MN, USA).
Metabolic risk factors
Blood samples were collected as previously described and then mixed with 1 mL of distilled water and centrifuged at 4,000 RCF for 15 minutes. Next, serum concentrations of fasting glucose (FG), total cholesterol (TC), high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), and triglycerides (TG) were determined using standard enzymatic techniques with intra- and interassay coefficients of variance of <5%.
Statistics
All data are expressed as mean ± standard deviation. Statistical analysis was performed using Statistica software (Dell, Round Rock, TX, USA). Data were analyzed using two-way analysis of variance (group × period) with repeated measures. Differences between groups were assessed using the Wilcoxon test. Statistical significance was set at P<0.05.
Results
Table 2 shows changes in physical characteristics of the participants. No significant differences were observed in baseline physical characteristics between the two groups. In addition, no significant differences were found in body weight, body fat, or body mass index before and after cocoa intake.
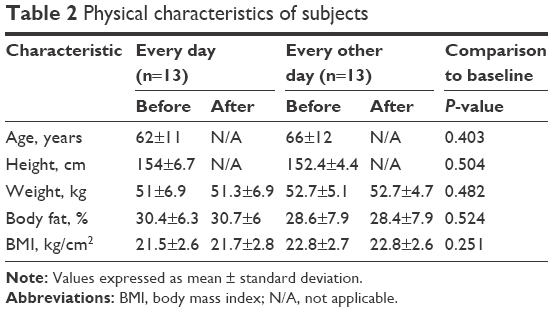 | Table 2 Physical characteristics of subjects |
Figure 1 shows changes in cfPWV and faPWV before and after cocoa intake in both groups. No significant differences in cfPWV or faPWV were observed between the two groups at baseline. cfPWV and faPWV decreased significantly in both groups after cocoa intake compared with baseline values (P<0.05). No significant differences were found between the two groups in the rate of change of cfPWV and faPWV after cocoa intake.
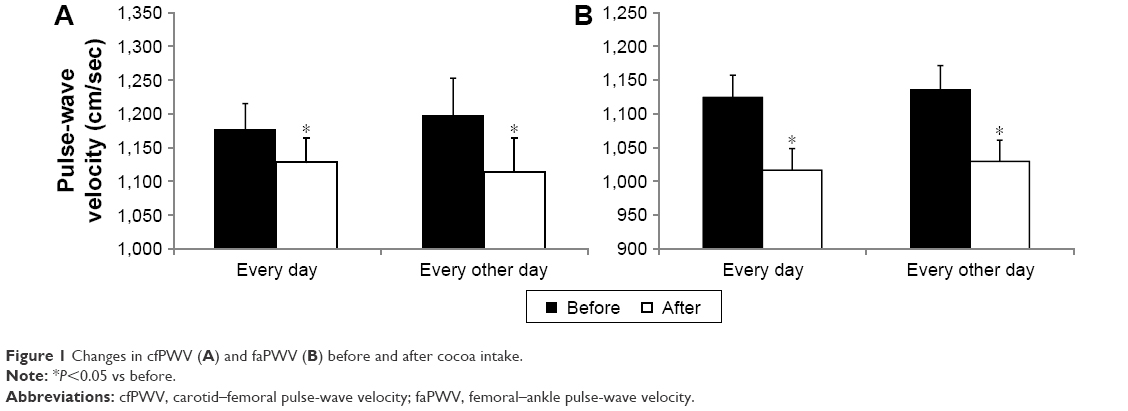 | Figure 1 Changes in cfPWV (A) and faPWV (B) before and after cocoa intake. |
Table 3 shows changes in heart rate, brachial BP, and ankle BP before and after cocoa intake in both groups. No significant differences were observed between the two groups in baseline heart rate, brachial and ankle SBP, DBP, MAP, or pulse pressure (PP). However, significant decreases were observed among both groups in brachial SBP, DBP, MAP, and PP after cocoa intake. In the every-day group, significant decreases were seen in ankle SBP, DBP, MAP, and PP after cocoa intake (P<0.05). In contrast, in the every-other-day group, significant decreases were seen in ankle PP after cocoa intake (P<0.05), but not in ankle SBP, DBP, or MAP. No significant differences were found between the two groups in the rate of change of brachial and ankle SBP, DBP, MAP, or PP.
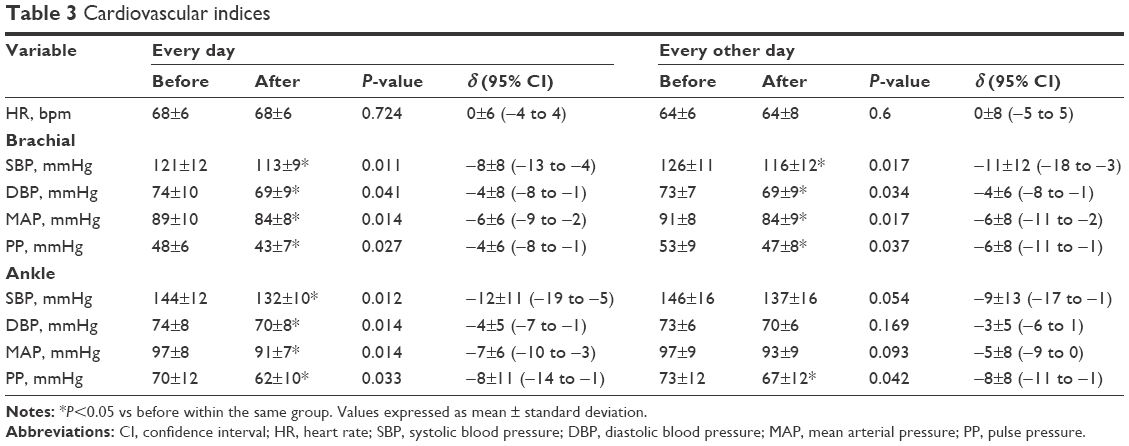 | Table 3 Cardiovascular indices |
Figure 2 shows changes in plasma ET1 concentration before and after cocoa intake in both groups. No significant differences were observed between the two groups in plasma ET1 concentration at baseline. Significant decreases were seen among both groups after cocoa intake (P<0.05). No significant differences were found between the two groups in the rate of change of plasma ET1 concentration after cocoa intake.
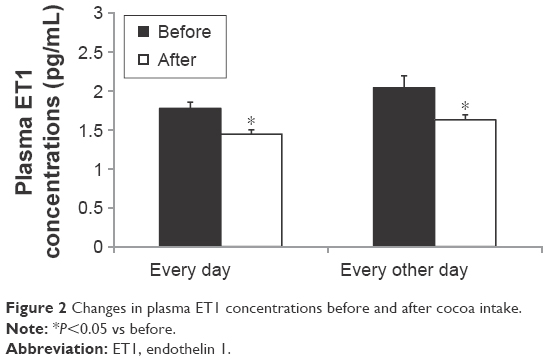 | Figure 2 Changes in plasma ET1 concentrations before and after cocoa intake. |
Table 4 shows changes in metabolic risk factors before and after cocoa intake in both groups. Regarding metabolic risk factors, no significant differences were seen between the two groups in serum concentrations of FG, TC, HDL-C, LDL-C, or TG at baseline. Significant decreases were observed among both groups in FG and TG after cocoa intake (P<0.05). No significant differences were found between the two groups in the rate of change of serum concentrations of FG, TC, HDL-C, LDL-C, or TG after cocoa intake.
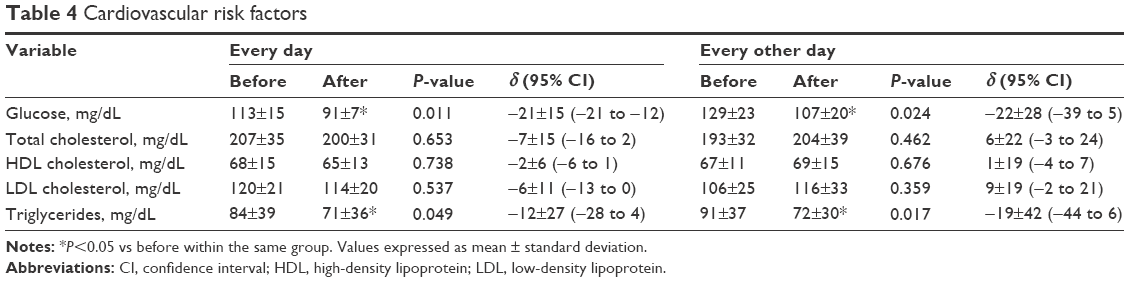 | Table 4 Cardiovascular risk factors |
Discussion
To our knowledge, this is the first study to investigate the effects of various cocoa-intake frequencies on arterial stiffness among postmenopausal women. The key finding of this study was that central and peripheral arterial stiffness decreased significantly in both groups after cocoa intake. Since the same dose of cocoa was ingested by each group, although at a different frequency, this indicates that intake frequency does not affect the cocoa-induced changes in arterial stiffness.
Daily consumption of cocoa and/or dark chocolate has a beneficial effect in the prevention of cardiovascular events.24,25 In a previous study, daily consumption of cocoa and dark chocolate over a 4-week period improved vascular function and reduced cardiovascular risk in both healthy and overweight adults.26 In a similar study, cocoa intake for 4 weeks was shown to reduce cardiovascular risk in healthy middle-aged adults, regardless of sex.13 These findings provide evidence that habitual cocoa intake has a beneficial effect on CVD risk factors24 and an inverse association with all-cause mortality and cardiovascular death.12 However, although the beneficial effects of cocoa intake have been reported, the effect of intake frequency on arterial stiffness has remained unclear. In this study, a significant decrease in arterial stiffness among postmenopausal women was observed after 12 weeks of cocoa intake, regardless of intake frequency. This finding suggests that intake frequency has no effect on the cardiovascular-protective actions exerted by cocoa.
Arterial stiffness increases with age, as evidenced by increases in PWV, and arterial stiffness is dramatically increased in postmenopausal compared with premenopausal women.7 Therefore, suppressing increases in arterial stiffness among this population is crucial for health promotion. Daily consumption of cocoa has been shown to be associated with decreases in central arterial stiffness in healthy adults, regardless of age.10,14 However, the findings in the present study among postmenopausal women indicate that consuming cocoa every other day also reduces central and peripheral arterial stiffness. Therefore, cocoa intake exerts beneficial effects regardless of frequency. This finding suggests that regardless of intake frequency, decreases in arterial stiffness may be associated with the dose of cocoa ingested weekly. Higher quantities of regularly ingested cocoa have been reported to be an independent determinant of reduced arterial stiffness,27 which is an effect dependent upon the dose of cocoa flavonoids.10 The participants in the present study consumed cocoa powder that included flavanols, a dose that has been shown to exert antiatherosclerotic effects. Both groups in the present study ingested an equivalent total weekly dose of cocoa flavanols, which suggests that habitual intake of flavanol-rich cocoa exerts positive effects on cardiovascular health in postmenopausal women, regardless of intake frequency. This finding expands upon previous research regarding the effects of habitual cocoa intake on arterial stiffness among postmenopausal women.
Several mechanisms may explain why the frequency of intake does not appear to alter the effects of cocoa on arterial stiffness. Some meta-analyses have proposed that flavanol-enriched cocoa reduces BP,28–30 which is a key determinant of arterial stiffness.31 In addition, ingestion of cocoa flavanols induces vasodilation, which also reduces BP.30 In the present study, BP was effectively reduced in both groups. Furthermore, ingestion of flavanol-enriched cocoa has been shown to be associated with reduced BP and significant improvements in vascular endothelial function.24,29,32 Vascular endothelial cells produce vasoactive substances, such as nitric oxide (NO), which help to regulate arterial stiffness and thus play a key role in the control of vascular tone.33–35 Vascular endothelial function affects large elastic and muscular arterial stiffness.36 Cocoa flavanols have been shown to stimulate NO production in endothelial cells.17,37 Acute intake of dark chocolate improved vascular endothelial function in healthy smokers 2–8 hours after ingestion, and this improvement was higher than baseline at even 24 hours after ingestion, although the difference was not significant.38 Moreover, daily consumption of cocoa and/or dark chocolate is associated with significant increases in basal and peak arterial diameter, as well as improved arterial blood flow through the brachial artery, which helps to reduce peripheral arterial stiffness.26 Increased arterial diameter with greater arterial blood flow has been shown to persist for several hours after the ingestion of flavanol-enriched cocoa.20 Therefore, it is reasonable to assume that acute unfavorable responses, such as increased arterial stiffness in the central and peripheral arterial vascular walls, might be reduced via peripheral artery vasodilation. In fact, consequential changes in vasodilator function may persist for several weeks,39 which can reduce baseline levels of arterial stiffness. This mechanism might help explain reductions in arterial stiffness in the absence of daily cocoa intake, and thereby supports the findings in the present study that cocoa intake twice daily every other day is also beneficial for arterial function. However, it should be noted vascular endothelial function was not measured in this study, which is an important limitation.
Endothelium-derived NO and ET1 play important roles in the regulation of arterial stiffness.40,41 Oral administration of (−)-epicatechin can increase NO production and reduce ET1 concentrations, thereby improving endothelial function.42 In addition, epicatechin can lead to acute improvements in endothelial function by modulating the circulating concentrations of vasoactive NO products and ET1.42 The endothelium regulates vascular tone by balancing the production of vasodilators, such as NO,43 and vasoconstrictors, such as ET1.44 Flavanols help to prevent reactive oxygen species-mediated degradation of NO, as well as blunt vasoconstrictor and proinflammatory responses.11 In the present study, plasma ET1 concentrations decreased in both groups. Decreases in plasma ET1 concentrations caused by flavanol occurred not only with daily cocoa intake but also with twice-daily cocoa intake ingested on an every-other-day basis, which may contribute to reductions in arterial stiffness. However, additional studies are needed to determine the precise mechanisms underlying the effects of intake frequency on arterial stiffness.
The findings in the present study demonstrated significant decreases in FG and TG, and these were consistent with previous observations that consumption of flavanol-enriched cocoa improves FG and TG levels in healthy adults.45,46 However, no effects were observed in regard to TC, HDL-C, or LDL-C. Increases in LDL-C and decreases in HDL-C can lead to the development of CVD.47 Flavanol-rich cocoa has been reported to reduce plasma levels of LDL-C and increase HDL-C serum concentrations in hypercholesterolemic patients.48,49 In this respect, our results differ from previous findings. One possible reason for this difference may be differences in the subjects of the studies. However, as TC, HDL-C, and LDL-C values in this study were within the standard ranges, these values might not have differed from baseline.
Study limitations
This study had several limitations. First, it did not include a sedentary control group who did not actively engage in regular physical exercise. Second, structural changes in the arterial wall that could impact arterial stiffness, such as changes in intima-media thickness, were not assessed.31 Third, the participants in the present study were all healthy postmenopausal women. Therefore, our findings might not be generalizable to older males or patients with CVD. Nevertheless, we believe that the present findings provide some potentially important clinical implications for postmenopausal women.
Conclusion
In conclusion, the results of the present study suggest that decreases in arterial stiffness are dependent upon the total amount, but not the frequency, of cocoa intake. These findings provide additional evidence that regular ingestion of cocoa helps to improve cardiovascular health among postmenopausal women.
Disclosure
The authors report no conflicts of interest in this work.
References
Mitchell GF, Hwang SJ, Vasan RS, et al. Arterial stiffness and cardiovascular events: the Framingham Heart Study. Circulation. 2010;121(4):505–511. | ||
van Sloten TT, Sedaghat S, Laurent S, et al. Carotid stiffness is associated with incident stroke: a systematic review and individual participant data meta-analysis. J Am Coll Cardiol. 2015;66(19):2116–2125. | ||
Vlachopoulos C, Aznaouridis K, Stefanadis C. Prediction of cardiovascular events and all-cause mortality with arterial stiffness: a systematic review and meta-analysis. J Am Coll Cardiol. 2010;55(13):1318–1327. | ||
Abhayaratna WP, Barnes ME, O’Rourke MF, et al. Relation of arterial stiffness to left ventricular diastolic function and cardiovascular risk prediction in patients ≥65 years of age. Am J Cardiol. 2006;98(10):1387–1392. | ||
Ikonomidis I, Lekakis J, Papadopoulos C, et al. Incremental value of pulse wave velocity in the determination of coronary microcirculatory dysfunction in never-treated patients with essential hypertension. Am J Hypertens. 2008;21(7):806–813. | ||
Kingwell BA, Gatzka CD. Arterial stiffness and prediction of cardiovascular risk. J Hypertens. 2002;20(12):2337–2340. | ||
Zaydun G, Tomiyama H, Hashimoto H, et al. Menopause is an independent factor augmenting the age-related increase in arterial stiffness in the early postmenopausal phase. Atherosclerosis. 2006;184(1):137–142. | ||
Hsia J, Margolis KL, Eaton CB, et al. Prehypertension and cardiovascular disease risk in the Women’s Health Initiative. Circulation. 2007;115(7):855–860. | ||
Hooper L, Kay C, Abdelhamid A, et al. Effects of chocolate, cocoa, and flavan-3-ols on cardiovascular health: a systematic review and meta-analysis of randomized trials. Am J Clin Nutr. 2012;95(3):740–751. | ||
Grassi D, Desideri G, Necozione S, et al. Cocoa consumption dose-dependently improves flow-mediated dilation and arterial stiffness decreasing blood pressure in healthy individuals. J Hypertens. 2015;33(2):294–303. | ||
Andriantsitohaina R, Auger C, Chataigneau T, et al. Molecular mechanisms of the cardiovascular protective effects of polyphenols. Br J Nutr. 2012;108(9):1532–1549. | ||
Buijsse B, Feskens EJ, Kok FJ, Kromhout D. Cocoa intake, blood pressure, and cardiovascular mortality: the Zutphen Elderly Study. Arch Intern Med. 2006;166(4):411–417. | ||
Sansone R, Rodriguez-Mateos A, Heuel J, et al. Cocoa flavanol intake improves endothelial function and Framingham risk score in healthy men and women: a randomised, controlled, double-masked trial: the Flaviola Health Study. Br J Nutr. 2015;114(8):1246–1255. | ||
Heiss C, Sansone R, Karimi H, et al. Impact of cocoa flavanol intake on age-dependent vascular stiffness in healthy men: a randomized, controlled, double-masked trial. Age (Dordr). 2015;37(3):9794. | ||
Wang-Polagruto JF, Villablanca AC, Polagruto JA, et al. Chronic consumption of flavanol-rich cocoa improves endothelial function and decreases vascular cell adhesion molecule in hypercholesterolemic postmenopausal women. J Cardiovasc Pharmacol. 2006;47(Suppl 2):S177–S186. | ||
Faridi Z, Njike VY, Dutta S, Ali A, Katz DL. Acute dark chocolate and cocoa ingestion and endothelial function: a randomized controlled crossover trial. Am J Clin Nutr. 2008;88(1):58–63. | ||
Heiss C, Dejam A, Kleinbongard P, Schewe T, Sies H, Kelm M. Vascular effects of cocoa rich in flavan-3-ols. JAMA. 2003;290(8):1030–1031. | ||
Monahan KD, Feehan RP, Kunselman AR, Preston AG, Miller DL, Lott ME. Dose-dependent increases in flow-mediated dilation following acute cocoa ingestion in healthy older adults. J Appl Physiol (1985). 2011;111(6):1568–1574. | ||
Vlachopoulos C, Alexopoulos N, Stefanadis C. Effect of dark chocolate on arterial function in healthy individuals: cocoa instead of ambrosia? Curr Hypertens Rep. 2006;8(3):205–211. | ||
Vlachopoulos C, Aznaouridis K, Alexopoulos N, Economou E, Andreadou I, Stefanadis C. Effect of dark chocolate on arterial function in healthy individuals. Am J Hypertens. 2005;18(6):785–791. | ||
Price L, Butler G. Rapid visual estimation and spectrophotometric determination of tannin content of sorghum grain. J Agric Food Chem. 1977;25(6):1268–1273. | ||
Natsume M, Osakabe N, Yamagishi M, et al. Analyses of polyphenols in cacao liquor, cocoa, and chocolate by normal-phase and reversed-phase HPLC. Biosci Biotechnol Biochem. 2000;64(12):2581–2587. | ||
Okamoto T, Sakamaki MS, Min SK, Yoshida S, Watanabe Y, Ogasawara R. Repeated cessation and resumption of resistance training attenuates increases in arterial stiffness. Int J Sports Med. 2015;36(6):440–445. | ||
Hooper L, Kroon PA, Rimm EB, et al. Flavonoids, flavonoid-rich foods, and cardiovascular risk: a meta-analysis of randomized controlled trials. Am J Clin Nutr. 2008;88(1):38–50. | ||
Zomer E, Owen A, Magliano DJ, Liew D, Reid CM. The effectiveness and cost effectiveness of dark chocolate consumption as prevention therapy in people at high risk of cardiovascular disease: best case scenario analysis using a Markov model. BMJ. 2012;344:e3657. | ||
West SG, McIntyre MD, Piotrowski MJ, et al. Effects of dark chocolate and cocoa consumption on endothelial function and arterial stiffness in overweight adults. Br J Nutr. 2014;111(4):653–661. | ||
Vlachopoulos CV, Alexopoulos NA, Aznaouridis KA, et al. Relation of habitual cocoa consumption to aortic stiffness and wave reflections, and to central hemodynamics in healthy individuals. Am J Cardiol. 2007;99(10):1473–1475. | ||
Desch S, Schmidt J, Kobler D, et al. Effect of cocoa products on blood pressure: systematic review and meta-analysis. Am J Hypertens. 2010;23(1):97–103. | ||
Shrime MG, Bauer SR, McDonald AC, Chowdhury NH, Coltart CE, Ding EL. Flavonoid-rich cocoa consumption affects multiple cardiovascular risk factors in a meta-analysis of short-term studies. J Nutr. 2011;141(11):1982–1988. | ||
Taubert D, Roesen R, Schömig E. Effect of cocoa and tea intake on blood pressure: a meta-analysis. Arch Intern Med. 2007;167(7):626–634. | ||
Laurent S, Boutouyrie P, Lacolley P. Structural and genetic bases of arterial stiffness. Hypertension. 2005;45(6):1050–1055. | ||
Taubert D, Roesen R, Lehmann C, Jung N, Schömig E. Effects of low habitual cocoa intake on blood pressure and bioactive nitric oxide: a randomized controlled trial. JAMA. 2007;298(1):49–60. | ||
Kinlay S, Creager MA, Fukumoto M, et al. Endothelium-derived nitric oxide regulates arterial elasticity in human arteries in vivo. Hypertension. 2001;38(5):1049–1053. | ||
Sugawara J, Maeda S, Otsuki T, Tanabe T, Ajisaka R, Matsuda M. Effects of nitric oxide synthase inhibitor on decrease in peripheral arterial stiffness with acute low-intensity aerobic exercise. Am J Physiol Heart Circ Physiol. 2004;287(6):H2666–H2669. | ||
Wilkinson IB, Qasem A, McEniery CM, Webb DJ, Avolio AP, Cockcroft JR. Nitric oxide regulates local arterial distensibility in vivo. Circulation. 2002;105(2):213–217. | ||
Wilkinson IB, Franklin SS, Cockcroft JR. Nitric oxide and the regulation of large artery stiffness: from physiology to pharmacology. Hypertension. 2004;44(2):112–116. | ||
Balzer J, Rassaf T, Heiss C, et al. Sustained benefits in vascular function through flavanol-containing cocoa in medicated diabetic patients a double-masked, randomized, controlled trial. J Am Coll Cardiol. 2008;51(22):2141–2149. | ||
Hermann F, Spieker LE, Ruschitzka F, et al. Dark chocolate improves endothelial and platelet function. Heart. 2006;92(1):119–120. | ||
Maiorana A, O’Driscoll G, Taylor R, Green D. Exercise and the nitric oxide vasodilator system. Sports Med. 2003;33(14):1013–1035. | ||
Bonetti PO, Lerman LO, Lerman A. Endothelial dysfunction: a marker of atherosclerotic risk. Arterioscler Thromb Vasc Biol. 2003;23(2):168–175. | ||
McVeigh GE, Allen PB, Morgan DR, Hanratty CG, Silke B. Nitric oxide modulation of blood vessel tone identified by arterial waveform analysis. Clin Sci (Lond). 2001;100(4):387–393. | ||
Loke WM, Hodgson JM, Proudfoot JM, McKinley AJ, Puddey IB, Croft KD. Pure dietary flavonoids quercetin and (-)-epicatechin augment nitric oxide products and reduce endothelin-1 acutely in healthy men. Am J Clin Nutr. 2008;88(4):1018–1025. | ||
Rassaf T, Preik M, Kleinbongard P, et al. Evidence for in vivo transport of bioactive nitric oxide in human plasma. J Clin Invest. 2002;109(9):1241–1248. | ||
Strachan FE, Newby DE, Sciberras DG, McCrea JB, Goldberg MR, Webb DJ. Repeatability of local forearm vasoconstriction to endothelin-1 measured by venous occlusion plethysmography. Br J Clin Pharmacol. 2002;54(4):386–394. | ||
Engler MB, Engler MM, Chen CY, et al. Flavonoid-rich dark chocolate improves endothelial function and increases plasma epicatechin concentrations in healthy adults. J Am Coll Nutr. 2004;23(3):197–204. | ||
Grassi D, Lippi C, Necozione S, Desideri G, Ferri C. Short-term administration of dark chocolate is followed by a significant increase in insulin sensitivity and a decrease in blood pressure in healthy persons. Am J Clin Nutr. 2005;81(3):611–614. | ||
Wilson PW. Changing cholesterol levels and coronary heart disease risk. Circulation. 2016;133(3):239–241. | ||
Baba S, Natsume M, Yasuda A, et al. Plasma LDL and HDL cholesterol and oxidized LDL concentrations are altered in normo- and hypercholesterolemic humans after intake of different levels of cocoa powder. J Nutr. 2007;137(6):1436–1441. | ||
Baba S, Osakabe N, Kato Y, et al. Continuous intake of polyphenolic compounds containing cocoa powder reduces LDL oxidative susceptibility and has beneficial effects on plasma HDL-cholesterol concentrations in humans. Am J Clin Nutr. 2007;85(3):709–717. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.