")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 15
Guselkumab, Risankizumab, and Tildrakizumab in the Management of Psoriasis: A Review of the Real-World Evidence
Authors Ruggiero A , Picone V, Martora F , Fabbrocini G, Megna M
Received 26 May 2022
Accepted for publication 7 August 2022
Published 16 August 2022 Volume 2022:15 Pages 1649—1658
DOI https://doi.org/10.2147/CCID.S364640
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Angelo Ruggiero, Vincenzo Picone, Fabrizio Martora, Gabriella Fabbrocini, Matteo Megna
Department of Clinical Medicine and Surgery, Section of Dermatology, University of Naples Federico II, Naples, Italy
Correspondence: Angelo Ruggiero, Section of Dermatology - Department of Clinical Medicine and Surgery, University of Naples Federico II, Via Pansini 5, Napoli, 80131, Italy, Tel +39 081 7462457, Fax +39 081 7462442, Email [email protected]
Abstract: Interleukin (IL)-23 inhibitors, guselkumab, risankizumab, and tildrakizumab, represent the latest class of biologics approved for the treatment of moderate-to-severe psoriasis. Since their approval numerous real-life studies were published on anti-IL-23 use in routine clinical practice. Indeed, real-life data are important to improve the dermatological decision-making process, including patients who are typically excluded from clinical trials, such as subjects suffering from several comorbidities, subjects on polypharmacy, as well as multifailure patients. Herein, we performed a comprehensive literature review about real-life data available on guselkumab, risankizumab, and tildrakizumab. Real-life data of anti-IL-23 seem to confirm the promising results of IL-23 shown by clinical trials, highlighting the efficacy and safety profiles of this new class of biologics also in clinical practice.
Keywords: guselkumab, tildrakizumab, risankizumab, psoriasis, review, real life, real-world practice, real-world evidence
Introduction
Psoriasis is a chronic inflammatory skin disease highly affecting patients’ quality of life, especially in moderate to severe disease.1,2 Although the pathophysiology of psoriasis is still not fully clarified, recent research advances lead to better understanding of the complex pathways behind psoriasis lesions, resulting in the development of highly efficacy and safety targeted therapies.3 Particularly, the relatively recent findings of effects of interleukin (IL)-17/23 axis in psoriasis burden and development, resulted in the development of biological drugs specifically binding IL-17 and IL-23 cytokines and/or their receptors.4,5 IL-23 inhibitors, guselkumab, risankizumab, and tildrakizumab, represent the latest class of biologics approved for the treatment of moderate-to-severe psoriasis.6 Guselkumab is a fully human monoclonal antibody specifically targeting the p19 subunit of IL-23.7 Its efficacy and safety were assessed by 4 phase-III trials (VOYAGE-1, VOYAGE-2, ECLIPSE, and NAVIGATE), evaluating guselkumab efficacy and safety profiles compared to placebo, adalimumab, secukinumab, and ustekinumab.8–11 Risankizumab is a fully human immunoglobulin (Ig)G monoclonal antibody that binds with high affinity to the p19 sub-unit of IL-23, which showed promising results in two phase-III studies (UltIMMa-1 and UltIMMa-2) comparing risankizumab to placebo and ustekinumab, in the IMMerge study, comparing risankizumab to secukinumab, and in the IMMvent study, comparing risankizumab with adalimumab.12 Tildrakizumab is another high-affinity, humanised, IgG1-κ antibody targeting p19 subunit of IL-23, which was evaluated by two phase-III trials (reSURFACE 1 and reSURFACE 2) showing its efficacy and safety compared to placebo and etanercept.13,14 The IL-23 inhibitors, guselkumab, risankizumab, and tildrakizumab, received the EMA and FDA approval for the treatment of moderate-to-severe psoriasis, in patients who are candidates for phototherapy or systemic therapy with guselkumab and risankizumab being also approved for psoriatic arthritis.6 Since their approval numerous real-life studies were published on anti-IL-23 use in routine clinical practice. Indeed, real-life data are mandatory to improve the dermatological decision-making process, because these studies also include patients who are typically excluded from clinical trials, such as subjects suffering from several comorbidities, subjects on polypharmacy, as well as multifailure patients.15–17 Herein, we performed a comprehensive literature review about real-life data on guselkumab, risankizumab, and tildrakizumab.
Materials and Methods
A comprehensive review of the English-language medical literature was performed using PubMed, Ovid, Scopus, Embase, and Cochrane Library databases from their inception to 1 April 2022, using Medical Subject Headings (mesh) terms (if applicable) and medical terms for the concepts of the use of guselkumab, risankizumab, and tildrakizumab in a real-life setting. Search strategy to identify articles was performed using the following research terms: “IL-23 inhibitors”, “guselkumab”, “risankizumab”, “tildrakizumab”, AND “real life”, AND “real world evidence”, AND “psoriasis”, and combinations thereof. Search involved all fields including title, abstract, keywords, and full text. Clinical and epidemiological studies, review, and systematic review regarding the use of guselkumab, risankizumab, and tildrakizumab in a real-life setting were included. Papers published from the start of time through April 2022 and from all origins were considered. Non-English literature had been excluded. The article is based on previously conducted studies.
Guselkumab
Guselkumab is a human monoclonal immunoglobulin G1 (IgG1) lambda antibody directed against IL-23 that has been recently approved for the treatment of moderate-to-severe plaque psoriasis and psoriatic arthritis.18 Numerous clinical trials have demonstrated the safety and efficacy of guselkumab, with the randomized double-blind phase III-controlled trials VOYAGE 1 and VOYAGE 2 assessing the guselkumab superiority vs adalimumab.19 Moreover, the ECLIPSE study assessed Guselkumab superiority vs secukinumab in long-term efficacy based on PASI 90 and the NAVIGATE study demonstrated guselkumab superiority against ustekinumab, showing that patients treated with ustekinumab who did not achieve an IGA of 0/1 by week 16 derived significant benefit from switching to guselkumab.20,21 Even if real studies on its efficacy and safety are growing in literature, long-term data as well as focus on anti-IL-17 or other anti-IL-23 failure subjects are still limited.22 A retrospective real-life study assessed the tolerability and efficacy of guselkumab in 180 patients in an observation period of 16 weeks.23 PASI 100 was achieved by 38.3% of patients, while PASI 90 and PASI 75 were achieved by 50.6% and 72.2% of patients, respectively.23 Only 15 patients (8.3%) had side effects and of these 5 (2.8%) discontinued therapy (1 due to arthromyalgia, 1 due to injection site reaction, 1 due to chronic lymphoid leukemia, 1 due to eczema and heart palpitation, and 1 due to panic attack).23 Similarly, Benhadou et al evaluated guselkumab in 112 patients in a retrospective 16-week real-life study.24 PASI 100 was achieved by 32.1%, PASI 90 by 55.4%, and PASI 75 by 82.1%. No patients discontinued therapy during the observation period.24 A similar study was carried out on the Chinese population, evaluating the clinical effectiveness using PASI 75, PASI 90, and PASI 100 responses at week 4, 12, and 16 separately on 45 patients.25 At week 16, PASI 75 was achieved by 95.5% of patients, PASI 90 by 88.6%, and PASI 100 by 45.5%. None of the 45 patients enrolled discontinued therapy because of ineffectiveness or intolerance due to side effects.25 The latter 3 studies evaluated the short-term (16 weeks) efficacy and safety of guselkumab therapy, giving important insights into its use but leaving unknowns about long-term therapies, given the chronic-recurrent nature of psoriasis.
Data from guselkumab short-term-real-life studies are summarized in Table 1.
 |
Table 1 Data from Guselkumab Short-Term (16-Week) Real-Life Studies |
However, real-life surveys with longer observation period exist. A prospective, observational, cohort study in a series of 44 patients to assess the effectiveness and safety of guselkumab was conducted in the Reggio Calabria and Messina dermatology wards.26 At week 24 PASI 75, PASI 90, and PASI 100 were achieved by 95.5%, 59.1%, and 16% of patients, respectively. Surprisingly, no AE were reported throughout the follow-up period.26 A retrospective cohort study by Snast et al evaluated the efficacy and safety of guselkumab in a cohort of 33 psoriasis patients who previously failed biologic agents.27 Only 29 patients (87.9%) completed at least 24 weeks of therapy. At week 24, 22 patients (76%) reached a PASI 75 or higher, 18 (62%) achieved PASI 90 or higher, 5 (17%) PASI 100. Moreover, none of the patients analyzed discontinued therapy due to AE or drug inefficacy.27 This study demonstrated that guselkumab represents a viable alternative even in patients who are poorly responsive to other biologic drugs, such as anti-TNF-alpha and anti-IL-17, with a good safety profile.27 The real-life non interventional, prospective, German multicenter PERSIST trial evaluated the efficacy and safety of guselkumab in 303 patients with moderate-to-severe psoriasis in a real-world setting.28 By week 28, 76.7%, 55.3%, and 28.9% of patients achieved a PASI 75, PASI 90, and PASI 100 response, respectively. Moreover, the mean Dermatology life quality index (DLQI) score decreased to 2.8, and 56.8% of patients achieved DLQI ≤ 1.28 The most common treatment-related AEs were viral upper respiratory tract infection (2.6%), diarrhea (1.3%), and pruritus (1.3%), leading to therapy discontinuation only for six patients (2%). A single-center retrospective cohort study in a population consisting of 46 patients, followed from December 2018 to April 2021, PASI 75, 90, and 100 were achieved on average on weeks 14, 19, and 21 respectively.29 In a subgroup of this population, consisting of 35 patients, PASI 75, PASI 90, and PASI 100 were reached at week 28 by 85.7%, 74.3%, and 57.1%, respectively.29 No patients dropped out of the study due to AE nor to inefficacy of the biologic agent.29 A multicentric study retrospectively evaluated 135 patients with psoriasis treated with guselkumab from June 2018 until November 2020, assessing efficacy using the degree of improvement in the PASI scores at baseline and after 4, 12, 20, 28, and 36 weeks.30 At week 36, the proportion of patients achieving PASI 75 and PASI 90 was 67% and 37%, respectively. Delayed onset of therapeutic response was noted in heavier patients and in patients with a previous exposure to biologic drugs, like IL-17 inhibitors: these were identified as the principal clinical predictors of a reduced response to guselkumab.30 For these reasons, the sample of patients analyzed in this study probably showed a lower clinical response to therapy. A real-world cohort retrospective study analyzed data on 181 Finnish patients who initiated guselkumab in 15 different study centers. Median treatment duration was 11 months; during follow-up 21 patients (12%) discontinued treatment.31 The most frequently reported reason for discontinuation was primary non-response (9 patients), followed by loss of response, lack of compliance or other causes. Eighty-five patients had a follow-up duration of at least 1 year and among them 73 (86%) were still on guselkumab at 1 year.31 High improvements were seen in the absolute PASI scores with 32 patients having absolute PASI ≤ 2 after a 9–14-month treatment.31 A prospective, observational, single-center, real-life study on 23 patients conducted by Megna et al demonstrated the efficacy and efficiency of guselkumab, showing that, at week 12, 95.6% of patients achieved PASI 75, while 43.5% PASI 90 whereas PASI 100 was reached by 26%.32 Moreover, at week 44, PASI 75, PASI 90, and PASI 100 were reached by 95.6%, 73.9%, and 43.5% respectively. Treatment was interrupted only for one patient, already suffering from Hepatitis C, because of altered liver enzymes.32 A retrospective real-life study was conducted evaluating all patients with moderate-to-severe psoriasis who started treatment with guselkumab at Hospital de la Santa Creu i Sant Pau, Barcelona (Spain), between February 2019 and October 2020.33 A total of 35 patients were included in the study. All patients had previously received at least one biologic treatment, such as anti-TNF-alpha, anti-IL-17, and anti-IL-12/23 agents, with a median of 2 biologic drugs per patient.33 At the first follow-up visit (25.6 ± 11.5 weeks), 19 patients (55.9%) reached PASI 100, 24 (70.6%) reached PASI 90, and 32 (94.1%) reached PASI 75.33 As for safety, 3 (8.6%) patients developed AE due to guselkumab. One patient showed paradoxical psoriasis attributable to guselkumab after the first dose and treatment was interrupted (2.9%). Two further patients developed AE: one developed a rash, diarrhea and arthromyalgia, and the other had an upper respiratory tract infection. None of the other patients reported side effects during the follow-up period.33 In a 52-week real-life retrospective longitudinal study 52 patients with moderate-to-severe plaque psoriasis were treated with guselkumab and followed for 12 months, demonstrating at 12 weeks a PASI 75, 90, and 100 response of 68%, 36%, and 18% of patients, respectively.34 After 1 year, PASI 75, 90, and 100 response was reached in 84.2%, 78.9%, and 63.2% of patients, respectively.34 During this period, no patients dropped out of the study due to adverse events nor to primary or secondary inefficacy.34 A 52-week real-life single-center retrospective study was conducted to evaluate the long-term efficacy and safety of guselkumab in patients who previously failed therapy with anti-IL-17 agents.35 Forty-four patients were enrolled and clinical efficacy was evaluated at each follow-up measuring PASI and BSA. PASI decreased from 13.9 ± 8.1 to 0.9 ± 0.7 at week 52 while BSA from 24.3 ± 19.6 to 1.3 ± 1.4. Only 3 (6.8%) patients discontinued guselkumab due to secondary inefficacy and no cases of serious AE were assessed.35 Another 52-week single-center retrospective study was performed enrolling psoriasis patients from October 2018 to May 2020.36 Thirteen patients were enrolled; about them, 46.1% have been previously treated with ustekinumab, while 69.2% with an anti-IL-17 biologic agent (38.5% secukinumab, 30.8% ixekizumab, and 38.5% both) (20). At baseline, mean PASI was 13.2 ± 6.8, reducing to 0.5 ± 0.7 at week 52. Moreover, BSA reduced from 22.3 ± 10.5 at baseline to 0.8 ± 1.1 at week 52. In addition, no statistically significant differences have been found between patients previously treated with anti-IL-12/23 compared to anti-IL-17 or both. Only one patient (7.7%) discontinued treatment with guselkumab at week 36 due to secondary inefficacy.36 A 60-week, real-life, multicenter, retrospective study investigated the effectiveness, safety, and tolerability of guselkumab in psoriatic patients.37 The mean baseline PASI reduced from 14.2 to 3.1 at week 12 and decreased to around 0 at weeks 36, 48, and 60. PASI 75, PASI 90, and PASI 100 have been achieved by 100%, 96.8%, and 83.9% of patients at week 60, respectively.37 Another real-life study on guselkumab was represented by a retrospective chart review conducted in 79 patients with psoriasis who were prescribed guselkumab from November 2017 to June 2019 in Ontario, Canada.38 Efficacy was assessed primarily through the body surface area (BSA) score, showing the complete clearance (BSA = 0%) for 35 patients (44.2%), an almost complete resolution (BSA < 1%) for 23 patients (29.1%), mild residual disease (BSA 2–3%) for 11 patients (13.9%), and low efficacy (BSA ≥3) for 10 patients (12.2%). The median duration of administration was 1.2 years with the shortest duration of administration being 10 weeks and the longest duration of administration being 2.7 years at the time of analysis.38 A total of 16.9% of patients reported at least 1 adverse event (AE), such as nasopharyngitis (6.3%) and headache (5.1%), and globally 9.0% discontinued guselkumab.38 Moreover, real-life data on a cohort of 24 early psoriatic arthritis patients demonstrated the efficacy and safety of guselkumab on peripheral and axial manifestations, reducing inflammation and joint pain.39
All the considered studies reported significant clinical improvements during guselkumab treatment in real-life settings. Data from real-world experiences are variable among different studies, showing results in line with clinical trials at week 28–48, in terms of PASI 90 response (achieved by 37–95.24% in real-life studies vs 84–90% reported by VOYAGE 219 and ECLIPSE trials).20 These results confirm guselkumab as an excellent choice in terms of both security, long-term efficacy, and overall tolerance.
Data from guselkumab long-term real-life studies are summarized in Table 2.
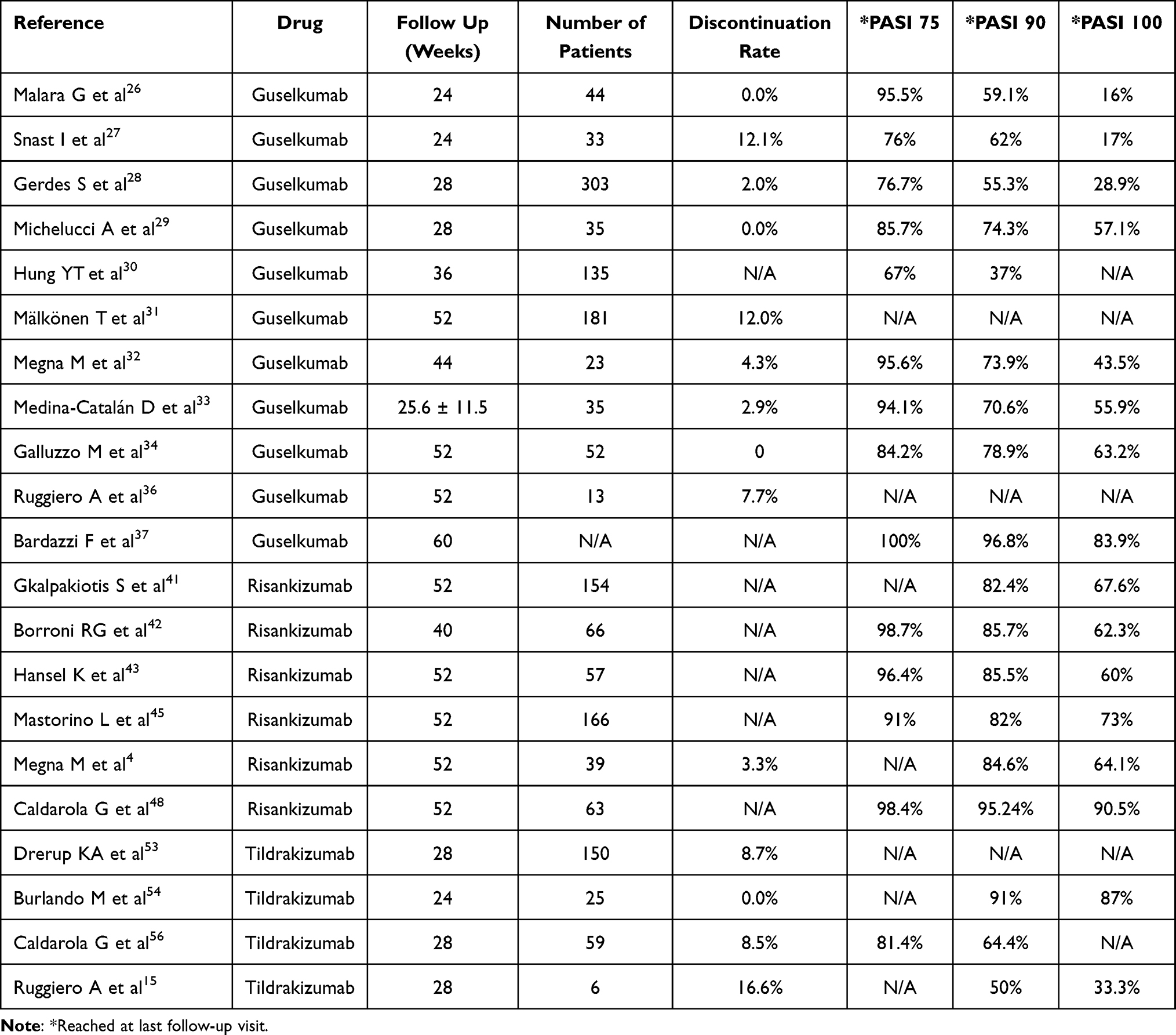 |
Table 2 Data from Guselkumab (Long-Term Follow Up), Risankizumab, and Tildrakizumab Real-Life Studies |
Risankizumab
Risankizumab, a fully human IgG monoclonal antibody against IL-23, is a biologic agent recently approved for moderate-to-severe psoriasis and psoriatic arthritis treatment.40
Hansel et al43 first reported a real-life experience of risankizumab at 16 weeks and published the same work taking the data to 52 weeks in 57 adults.43,44 In this study, the efficacy and safety of risankizumab at week 52 compared with week 16 were evaluated. The response in terms of PASI-75, PASI-90, and PASI-100 was excellent. Specifically, PASI-75 was achieved by 96.4% of patients, PASI-90 response was 85.5%. PASI-100 was achieved by 60.0%. Results at 52 weeks were achieved as early as week 36. Notably, PASI-100 was achieved by 65.5% of patients, showing a significant improvement over the PASI-100 achievement of the 16-week real-world experience (49.1%). This result underscores the increasing efficacy of risankizumab in the long-term.43,44
Megna et al47 conducted a 16-week prospective study to evaluate the efficacy and safety of risankizumab. Mean PASI decreased from 12.3 ± 5.2 (baseline) to 4.4 ± 2.7 at week 4 (p < 0.01) and to 2.7 ± 1.7 at week 16 (p < 0.001). No AEs were reported up to week 16 and few and mild grade laboratory tests were reported.
Borroni et al42 conducted a retrospective study that included 66 consecutive adults with moderate to severe psoriasis vulgaris treated with risankizumab as monotherapy until week 40 in a real-life setting. At week 40, 98.7%, 85.7%, and 62.3% of patients achieved a reduction in Area Psoriasis and Severity Index (PASI) ≥ 75% (PASI 75), PASI 90, and PASI 100, respectively, they also noted that patients who had not responded to 2 or more prior biologic treatments were significantly less likely to achieve PASI 75/90 at week 16 and PASI 90/100 at week 40 compared with those who had been previously treated with a single biologic, and compared with those treated with risankizumab as a first-line biologic.42
Real-life data are less numerous than guselkumab. Gkalpakiotis et al41 have retrospectively analyzed 154 patients from 18 centers in the Czech Republic who had undergone biologic therapy with risankizumab for moderate to severe plaque psoriasis, in this real life the proportion of patients achieving a 90% improvement in their PASI score from baseline (PASI 90) and complete resolution (PASI 100) after 16, 28, and 52 weeks was analyzed.
After 16 weeks, 63.8 and 44.7% of patients achieved PASI 90 and PASI 100 responses, respectively. The improvement continued over time, and the proportion of patients with PASI 90 and PASI 100 responses increased to 82.4 and 67.6%, respectively, at week 52.42
Mastorino et al45 have retrospectively analyzed 166 patients from two centers in Italy undergoing risankizumab for psoriasis. The percentage of patients achieving 100%, 90%, 75% improvement in PASI and PASI <3 was collected at weeks 16, 28, 40, and 52. At the time of analysis, 165, 103, 30, and 11 patients had completed 16, 28, 40, and 52 weeks of treatment, respectively.45 The mean PASI score decreased from 12.5 ± 5.1 at baseline to 1.9 ± 2.4 at week 16. Similar reductions were observed when considering PASI <3, PASI 75, PASI 90, and PASI 100. The authors concluded that previous failure of biologics, different smoking habits, obesity, and joint involvement led to a lower response to risankizumab whereas no difference in risankizumab response occurred with involvement of hard-to-treat areas.45
A 52-week retrospective real-life study was performed to evaluate the long-term efficacy and safety of risankizumab in patients who had previously failed anti-IL-17 by Megna et al.4 A total of 39 patients (26 males, 66.7%; mean age 50.5 ± 13.7 years) were enrolled. A statistically significant reduction in Psoriasis Area Severity Index (PASI) and Body Surface Area (BSA) was assessed at each follow-up (PASI at baseline vs week 52: 13.7 ± 5.8 vs 0.9 ± 0.8, p < 0.0001; BSA 21.9 ± 14.6 vs 1.9 ± 1.7, p < 0.0001). No cases of serious adverse events were evaluated.4,46 The authors concluded that the efficacy and safety of risankizumab has also been demonstrated in patients with psoriasis who have previously failed anti-IL-17 treatments.4,46
Also, by the same authors, Megna et al47 evaluated the efficacy and safety of risankizumab in patients who had previously failed anti-IL-17, anti-IL-12/23, or anti-IL-23 inhibitors. A retrospective single-center study was conducted with a total of eight patients (four men and four women, mean age 45.4747 ± 14.3 years). Five of them (62.5%) had received ustekinumab, seven (87.5%) at least one anti-IL-17, and only one patient (12.5%) guselkumab. Secukinumab had been used in five (62.5%) cases, and ixekizumab in four (50.0%). Mean PASI and BSA at baseline were 11.9 ± 5.5 and 22.9 ± 13.1, respectively, and 3.3 ± 1.7 and 7.5 ± 5 (P < 0.001 and P < 0.01) at week 16.47 Mean NAPSI at baseline (18.0 ± 8.5) decreased to 7 ± 1.4 at week 16. No adverse events were reported. The authors conclude that these preliminary real-world data show risankizumab as a promising treatment option in patients who have failed anti-IL-17, anti-IL-12/23, and even the other anti-IL-23 counterpart, guselkumab.47
Also, Caldarola et al48 have analyzed the efficacy and safety of risankizumab in patients with moderate to severe psoriasis over a 52-week period in 112 patients. A multicenter retrospective study was conducted in patients who started risankizumab between July 2019 and December 2020. The Area Psoriasis and Severity Index (PASI) was measured at baseline and after 4, 16, 28, and 52 weeks. At week 52, data were available for 63 of 112 (56.25%) patients, with 98.41% (61 out of 63) of these patients achieving PASI 75, 95.24% (60 out of 63) achieving PASI 90 and 90.48% (57 out of 63) achieving PASI 100.48 No serious safety issues or discontinuations related to adverse events were reported.
There are no other real-life experiences in the literature up to 52 weeks beyond what we have already analyzed on the use of risankizumab, but there are some case series or preliminary studies at 16 weeks or even comparison studies between biologicals such as risankizumab and guselkumab.49–51
Tildrakizumab
Tildrakizumab is fully humanized IgG1-κ antibody specifically targeting and binding with high affinity the p19 subunit of IL-23.52 Tildrakizumab efficacy and safety profiles have been showed by two randomized clinical trials (reSURFACE 1 and reSURFACE 2), which evaluated tildrakizumab superiority to both placebo and etanercept.13 Due to its more recent availability in clinical practice than the other IL-23 inhibitors, data from tildrakizumab real-life studies are still poor.
The largest available real-life study was published by Drerup et al53 who evaluated tildrakizumab efficacy and safety in a cohort of 150 patients until week 28.53 The enrolled patients highly differed from patients included in clinical trials by both demographic data, and psoriasis severity.53 Particularly, the mean PASI at baseline was significantly lower than reSURFACE studies (8.6 ± 4.2 vs 20.5 ± 7.63) Interestingly, the authors reported tildrakizumab as an high and rapid effective treatment, being able to reach a rapid decrease of mean PASI, as well as a significant and rapid improvement of DLQI.53 However, the authors did not report the rate of patients achieving PASI 75, PASI 90, and PASI 100 responses.53
Burlando et al54 reported tildrakizumab efficacy and safety in 25 patients up to 24 weeks of follow-up.54 Results were in line with data reported by reSURFACE studies, showing even higher rates of both PASI 90 and PASI 100 responses, at both week 12 (PASI 90: 71%, PASI 100: 67%), and week 28 (PASI 90: 91%, PASI 100: 87%).54 Furthermore, no patients discontinued the treatment.54
Caldarola et al55 reported the results of a multicentric retrospective study enrolling patients who initiated tildrakizumab, up to 28 weeks of follow-up.56 The authors reported huge improvements in PASI during follow-ups. Particularly, PASI 75 response was achieved by 11.90% at week 4, 57.60% at week 16, and up to 81.40% at week 28, while PASI 90 was reported in 5.11% at week 4, 33.91% at week 16, and up to 64.40% at week 28.56 Treatment discontinuation was reported in 8.47% of patients.55
Galluzzo et al56 evaluated the efficacy of tildrakizumab for the treatment of difficult-to-treat areas (Scalp, Nail, Palmoplantar and Genital Psoriasis), in a retrospective 28-week study including 18 patients.56 In all treated patients, tildrakizumab decreased a range of disease activity, showing a significant reduction of the mean PASI, which decreased from 11.5 at baseline up to 2.4 at week 28.56 Huge improvements were also reported in the PSSI score for scalp involvement (which decreased from 36.2 to 2.7), the NAPSI score for nail involvement (which decreased by 67.6% at week 28), and the ppPASI score for palmoplantar involvement (with complete clearance achieved at week 28).56
Data from real-world experiences are variable among different studies, reporting results also higher than clinical trials at weeks 24–28, in terms of both PASI 90 (achieved by 50–91% in real-life studies vs 56–58% reported by reSURFACE studies), and PASI 100 responses (achieved by 33.3–87% in real-life studies vs 23–27% reported by reSURFACE studies).
Hence, from real-life data available for tildrakizumab, it seems to confirm the promising efficacy and safety profiles showed by clinical trials, highlighting the potential use of tildrakizumab with high-efficacy rates even in patients with less favorable characteristics, such as elderly and more fragile patients.
Miscellaneous
Further data from real-world experience comes from studies evaluating the whole anti-IL-23 class and/or comparing risankizumab, guselkumab, and/or tildrakizumab with other biological therapies. Ruggiero et al49 reported the results of a retrospective study evaluating and comparing the efficacy and safety of guselkumab and risankizumab.49 Interestingly, the authors reported high and comparable rates of PASI 90 (75% vs 68.7%) and PASI 100 (47.2% vs 46.8%) responses among the two anti-IL-23, with also comparable rates of reported AEs and discontinuations until last follow-up visit (weeks 40–44).49,57 Bonifati et al58 reported their experience in treating 12 multifailure psoriatic patients (including 9 patients treated with guselkumab and 3 treated with risankizumab), switching from an anti-IL-17 to an anti-il-23 treatment, who showed a significant improvements. The efficacy of anti-IL-23s, particularly for guselkumab, and risankizumab, in multifailure patients had also been shown by several real-life studies evaluating their efficacy and safety in patients previously treated with IL-17 and/or anti-IL-12/23, showing their efficacy even in this subgroup of patients which represent a frequent situation to face in daily dermatologic practice.4,35,36,46,58
With regard to tildrakizumab, in a recent published retrospective study, Narcisi et al59 evaluated and compared the efficacy of anti-IL-23 drugs and IL-17 or IL-17RA inhibitors in a real-life population suffering from scalp psoriasis.59 Iinteresting data reported by the authors showed that the rate of patients showing a significant improvement of scalp psoriasis was slightly higher at week 24 and at week 48 in patients treated with anti-IL-17, no statistically significant differences were reported between the two treatment groups.59 Data about anti-IL-23 were grouped, so no specific data for the tildrakizumab treatment group were available. However, the authors reported that patients treated with tildrakizumab seemed to respond later than risankizumab and guselkumab.59 Further data of tildrakizumab from real-life studies were published by Ruggiero et al15 who reported the results of a retrospective study evaluating and comparing guselkumab, risankizumab, and tildrakizumab safety and efficacy in real-world-practice in elderly patients.15 Among the study population, 6 patients received tildrakizumab treatment, showing high rates of PASI 90 and PASI 100 at week 28 (PASI 90: 50%; PASI 100: 33.3%), with no adverse events reported even in this older study population (mean age).15
Conclusions
IL-23 inhibitors represent the latest class of biologic therapy available for the management of psoriasis. Clinical trials previously showed promising results for all the members of this class, including guselkumab, risankizumab, and tildrakizumab. Although the already available results from trials, real-life studies are important due to the different cohort of patients to which these studies refer to, such as subjects suffering from multiple comorbidities, the elderly, as well as subjects suffering from other forms than plaque psoriasis. Indeed, these patients are usually excluded by the rigid inclusion and exclusion criteria characterizing the clinical trials. Furthermore, data from real-life settings are important also in patients affected by infections, such as patients affected by latent tuberculosis, as well as patients affected by COVID-19.60–68 Indeed, these conditions may raise several safety concerns during the treatment decision progress. Hence, real-life studies may represent an important source of data to improve the decision-making progress, leading physicians to choose the best treatment for the best patient. In this context, real-life data about anti-IL-23 seem to confirm the promising results of IL-23 showed by clinical trials, highlighting the efficacy and safety profiles of this new class of biologics also in clinical practice. Hence, guselkumab, risankizumab, and tildrakizumab are confirmed to be effective and safe treatment option in routine dermatological practice, showing excellent outcomes even in more fragile patients, such as the elderly, suffering from multiple comorbidities, with no serious adverse events reported. However, more studies are needed to confirm the actually available data, with further studies evaluating these relatively recent class of biologics also in long-term follow ups, to better evaluate the long-term efficacy, safety, and drug survival.
Data Sharing Statement
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Boehncke WH, Schön MP. Psoriasis. Lancet. 2015;386(9997):983–994. doi:10.1016/S0140-6736(14)61909-7
2. Ruggiero A, Fabbrocini G, Cacciapuoti S, Cinelli E, Gallo L, Megna M. Ocular Manifestations in Psoriasis Screening (OcMaPS) questionnaire: a useful tool to reveal misdiagnosed ocular involvement in psoriasis. J Clin Med. 2021;10(5):1031. doi:10.3390/jcm10051031
3. Rendon A, Schäkel K. Psoriasis pathogenesis and treatment. Int J Mol Sci. 2019;20(6):1475. doi:10.3390/ijms20061475
4. Megna M, Potestio L, Ruggiero A, Camela E, Fabbrocini G. Risankizumab treatment in psoriasis patients who failed anti-IL17: a 52-week real-life study. Dermatol Ther. 2022;e15524. doi:10.1111/dth.15524
5. Bugaut H, Aractingi S. Major role of the IL17/23 axis in psoriasis supports the development of new targeted therapies. Front Immunol. 2021;12:621956. doi:10.3389/fimmu.2021.621956
6. Yang K, Oak ASW, Elewski BE. Use of IL-23 inhibitors for the treatment of plaque psoriasis and psoriatic arthritis: a comprehensive review. Am J Clin Dermatol. 2021;22(2):173–192. doi:10.1007/s40257-020-00578-0
7. Megna M, Ruggiero A, Camela E, Fabbrocini G, Marasca C. A case of erythrodermic psoriasis successfully treated with guselkumab. Dermatol Ther. 2020;33(2):e13238. doi:10.1111/dth.13238
8. Megna M, Tommasino N, Potestio L, et al. Real-world practice indirect comparison between guselkumab, risankizumab and tildrakizumab: results from an Italian 28-week retrospective study. J Dermatolog Treat. 2022;1–13. doi:10.1080/09546634.2022.2081655
9. Megna M, Ruggiero A, Di Guida A, Patrì A, Fabbrocini G, Marasca C. Ixekizumab: an efficacious treatment for both psoriasis and hidradenitis suppurativa. Dermatol Ther. 2020;33(4):e13756. doi:10.1111/dth.13756
10. Blauvelt A, Papp KA, Griffiths CE, et al. Efficacy and safety of guselkumab, an antiinterleukin-23 monoclonal antibody, compared with Adalimumab for the continuous treatment of patients with moderate to severe psoriasis: results from the Phase III, double blinded, placebo- and active comparator-controlled VOYAGE 1 trial. J Am Acad Dermatol. 2017;76(3):405–417. doi:10.1016/j.jaad.2016.11.041
11. Reich K, Armstrong AW, Foley P, et al. Efficacy and safety of guselkumab, an antiinterleukin 23 monoclonal antibody, compared with Adalimumab for the treatment of patients with moderate to severe psoriasis with randomized withdrawal and retreatment: results from the phase III, double-blind, placebo- and active comparator-controlled VOYAGE 2 trial. J Am Acad Dermatol. 2017;76(3):418–431. doi:10.1016/j.jaad.2016.11.042
12. Gordon KB, Strober B, Lebwohl M, et al. Efficacy and safety of risankizumab in moderate-to-severe plaque psoriasis (UltIMMa-1 and UltIMMa-2): results from two double-blind, randomised, placebo-controlled and ustekinumab-controlled Phase 3 trials. Lancet. 2018;392(10148):650–661. doi:10.1016/S0140-6736(18)31713-6
13. Reich K, Papp KA, Blauvelt A, et al. Tildrakizumab versus placebo or etanercept for chronic plaque psoriasis (reSURFACE 1 and reSURFACE 2): results from two randomised controlled, phase 3 trials. Lancet. 2017;390:276–288. doi:10.1016/S0140-6736(17)31279-5
14. Griffiths CEM, Thaci D, Iversen L, et al. Tildrakizumab results in significant and sustained improvements in health-related quality of life in patients with moderate to severe psoriasis in a phase 3 trial (reSURFACE 1) [e-poster 8047]. In:
15. Ruggiero A, Fabbrocini G, Cinelli E, Ocampo Garza SS, Camela E, Megna M. Anti-interleukin-23 for psoriasis in elderly patients: guselkumab, risankizumab and tildrakizumab in real-world practice. Clin Exp Dermatol. 2022;47(3):561–567. doi:10.1111/ced.14979
16. Ruggiero A, Megna M, Marino V, et al. A case of esophageal candidiasis in a psoriatic patient treated with ixekizumab: should treatment be discontinued? Dermatol Ther. 2022;35(4):e15361. doi:10.1111/dth.15361
17. Garcia-Doval I, Dávila-Seijo P. How real are ‘real-life studies’ in psoriasis, and the uncertain meaning of drug persistence. Br J Dermatol. 2019;180(1):15–16. doi:10.1111/bjd.17104
18. Blauvelt A, Burge R, Gallo G, et al. A retrospective cohort analysis of treatment patterns over 1 year in patients with psoriasis treated with ixekizumab or guselkumab. DermatolTher. 2022;12(3):701–714.
19. Reich K, Armstrong AW, Foley P, et al. Efficacy and safety of guselkumab, an anti-interleukin-23 monoclonal antibody, compared with Adalimumab for the treatment of patients with moderate to severe psoriasis with randomized withdrawal and retreatment: results from the phase III, double-blind, placebo- and active comparator-controlled VOYAGE 2 trial. J Am Acad Dermatol. 2017;76(3):418–431.
20. Reich K, Armstrong AW, Langley RG, et al. Guselkumab versus secukinumab for the treatment of moderate-to-severe psoriasis (ECLIPSE): results from a phase 3, randomised controlled trial. Lancet. 2019;394(10201):831–839. doi:10.1016/S0140-6736(19)31773-8
21. Langley RG, Tsai TF, Flavin S, et al. Efficacy and safety of guselkumab in patients with psoriasis who have an inadequate response to ustekinumab: results of the randomized, double-blind, Phase III NAVIGATE trial. Br J Dermatol. 2018;178(1):114–123. doi:10.1111/bjd.15750
22. Singh S, Singh S, Thangaswamy A, Thangaraju P, Varthya SB. Efficacy and safety of Risankizumab in moderate to severe psoriasis: a systematic review and meta-analysis. Dermatol Ther. 2021;34(1):e14487. doi:10.1111/dth.14487
23. Fougerousse AC, Ghislain PD, Reguiai Z, et al. Effectiveness and short-term (16-week) tolerance of guselkumab for psoriasis under real-life conditions: a retrospective multicenter study. J Eur Acad Dermatol Venereol. 2020;34(10):e644–e646.
24. Benhadou F, Ghislain PD, Guiot F, et al. Real-life effectiveness and short-term (16-week) tolerance of guselkumab for psoriasis: a Belgian retrospective multicentre study. J Eur Acad Dermatol Venereol. 2020;34(12):e837–e839. doi:10.1111/jdv.16715
25. Zhuang JY, Li JS, Zhong YQ, et al. Evaluation of short-term (16-week) effectiveness and safety of guselkumab in patients with psoriasis: a prospective real-life study on the Chinese population. DermatolTher. 2021;34(5):e15054.
26. Malara G, Trifirò C, Bartolotta A, et al. Real-world effectiveness and safety of Guselkumab for the treatment of psoriasis: a 6-month prospective study in a series of psoriatic patients. Eur Rev Med Pharmacol Sci. 2021;25(1):406–412. doi:10.26355/eurrev_202101_24408
27. Snast I, Sherman S, Holzman R, Hodak E, Pavlovsky L. Real-life experience of guselkumab in patients with psoriasis. Dermatol Ther. 2020;33(6):e13964. doi:10.1111/dth.13964
28. Gerdes S, Bräu B, Hoffmann M, et al. Real-world effectiveness of guselkumab in patients with psoriasis: health-related quality of life and efficacy data from the noninterventional, prospective, German multicenter PERSIST trial. J Dermatol. 2021;48(12):1854–1862. doi:10.1111/1346-8138.16128
29. Michelucci A, Manzo Margiotta F, Panduri S, et al. A real-life experience as a proof of Guselkumab effectiveness and safety in patients with moderate to severe psoriasis. Dermatol Ther. 2022;35(4):e15339. doi:10.1111/dth.15339
30. Hung YT, Lin YJ, Chiu HY, Huang YH. Impact of previous biologic use and body weight on the effectiveness of guselkumab in moderate-to-severe plaque psoriasis: a real-world practice. Ther Adv Chronic Dis. 2021;12:20406223211046685. doi:10.1177/20406223211046685
31. Mälkönen T, Nuutinen P, Hallinen T, et al. Guselkumab treatment outcomes and persistence in a nationwide real-world cohort of patients with plaque psoriasis. Acta Derm Venereol. 2022;102:adv00631. doi:10.2340/actadv.v101.910
32. Megna M, Fabbrocini G, Cinelli E, Camela E, Ruggiero A. Guselkumab in moderate to severe psoriasis in routine clinical care: an Italian 44-week real-life experience. J Dermatolog Treat. 2020;1–5. doi:10.1080/09546634.2020.1800577
33. Medina-Catalán D, Riera P, Pagès-Puigdemont N, et al. A cohort study of guselkumab in the treatment of psoriasis refractory to previous biologic therapies: effectiveness, safety and adherence. Int J Clin Pharm. 2022;44:725–730. doi:10.1007/s11096-022-01400-z
34. Galluzzo M, Tofani L, Lombardo P, et al. Use of guselkumab for the treatment of moderate-to-severe plaque psoriasis: a 1 year real-life study. J Clin Med. 2020;9(7):2170. doi:10.3390/jcm9072170
35. Megna M, Potestio L, Ruggiero A, Camela E, Fabbrocini G. Guselkumab is efficacious and safe in psoriasis patients who failed anti-IL17: a 52-week real-life study. J Dermatolog Treat. 2022;1–5. doi:10.1080/09546634.2022.2036674
36. Ruggiero A, Fabbrocini G, Cinelli E, Megna M. Efficacy and safety of guselkumab in psoriasis patients who failed ustekinumab and/or anti-interleukin-17 treatment: a real-life 52-week retrospective study. Dermatol Ther. 2021;34(1):e14673. doi:10.1111/dth.14673
37. Bardazzi F, Viviani F, Merli Y, et al. Guselkumab for the treatment of psoriasis: a 60-week real-life multicenter retrospective experience. Expert Opin Biol Ther. 2022;1–6. doi:10.1080/14712598.2022.2064216
38. Maliyar K, O’Toole A, Gooderham MJ. Long-term single center experience in treating plaque psoriasis with guselkumab. J Cutan Med Surg. 2020;24(6):588–595. doi:10.1177/1203475420932514
39. Pantano I, Mauro D, Romano F, et al. Real-life efficacy of guselkumab in patients with early psoriatic arthritis. Rheumatology. 2022;61(3):1217–1221. doi:10.1093/rheumatology/keab509
40. Martora F, Villani A, Ocampo-Garza SS, Fabbrocini G, Megna M. Alopecia universalis improvement following risankizumab in a psoriasis patient. J Eur Acad Dermatol Venereol. 2022;36. doi:10.1111/jdv.18017
41. Gkalpakiotis S, Cetkovska P, Arenberger P, et al. Risankizumab for the treatment of moderate-to-severe psoriasis: real-life multicenter experience from the Czech Republic. DermatolTher. 2021;11(4):1345–1355.
42. Borroni RG, Malagoli P, Gargiulo L, et al. Real-life effectiveness and safety of risankizumab in moderate-to-severe plaque psoriasis: a 40-week multicentric retrospective study. Acta Derm Venereol. 2021;101(11):adv00605. doi:10.2340/actadv.v101.283
43. Hansel K, Zangrilli A, Bianchi L, et al. A multicenter study on effectiveness and safety of risankizumab in psoriasis: an Italian 16-week real-life experience during the COVID-19 pandemic. J Eur Acad Dermatol Venereol. 2021;35(3):e169–e170. doi:10.1111/jdv.17003
44. Hansel K, Zangrilli A, Bianchi L, et al. A 52-week update of a multicentre real-life experience on effectiveness and safety of risankizumab in psoriasis. J Eur Acad Dermatol Venereol. 2022;36(2):e111–e113. doi:10.1111/jdv.17656
45. Mastorino L, Susca S, Megna M, et al. Risankizumab shows high efficacy and maintenance in improvement of response until week 52. DermatolTher. 2022;35(5):e15378.
46. Megna M, Fabbrocini G, Ruggiero A, Cinelli E. Efficacy and safety of risankizumab in psoriasis patients who failed anti-IL-17, anti-12/23 and/or anti IL-23: preliminary data of a real-life 16-week retrospective study. Dermatol Ther. 2020;33(6):e14144. doi:10.1111/dth.14144
47. Megna M, Cinelli E, Gallo L, Camela E, Ruggiero A, Fabbrocini G. Risankizumab in real life: preliminary results of efficacy and safety in psoriasis during a 16-week period. Arch Dermatol Res. 2021;314:619–623. doi:10.1007/s00403-021-02200-7
48. Caldarola G, Zangrilli A, Bernardini N, et al. Risankizumab for the treatment of moderate-to-severe psoriasis: a multicenter, retrospective, 1 year real-life study [published online ahead of print, 2022 Apr 6]. DermatolTher. 2022;35:e15489.
49. Ruggiero A, Fabbrocini G, Cinelli E, Megna M. Real world practice indirect comparison between guselkumab and risankizumab: results from an Italian retrospective study. DermatolTher. 2022;35(1):e15214.
50. Dawoud NM, El Badawy MB, Al Eid HS, Abdel Fattah MM. Risankizumab effectiveness and safety in psoriasis patients who failed other biologics: real-life case series. Indian J Dermatol Venereol Leprol. 2022;88(2):235–240. doi:10.25259/IJDVL_510_2021
51. Sotiriou E, Bakirtzi K, Papadimitriou I, et al. A head-to-head comparison of risankizumab and ixekizumab for genital psoriasis: a real-life, 24-week, prospective study. J Eur Acad Dermatol Venereol. 2022;36(5):e359–e361. doi:10.1111/jdv.17880
52. Sinclair R, ThirtharPalanivelu V. Tildrakizumab for the treatment of psoriasis. Expert Rev Clin Immunol. 2019;15(1):5–12. doi:10.1080/1744666X.2019.1544493
53. Drerup KA, Seemann C, Gerdes S, Mrowietz U. Effective and safe treatment of psoriatic disease with the anti-IL-23p19 biologic tildrakizumab: results of a real-world prospective cohort study in nonselected patients. Dermatology. 2021;238:1–5.
54. Burlando M, Castelli R, Cozzani E, Parodi A. Treatment of moderate-to-severe plaque psoriasis with tildrakizumab in the real-life setting. Drugs Context. 2021;10:2021. doi:10.7573/dic.2021-2-6
55. Caldarola G, Galluzzo M, Bernardini N, et al. Tildrakizumab in moderate-to-severe plaque psoriasis: a multicenter, retrospective, real-life study. Dermatol Ther. 2022;35:e15488. doi:10.1111/dth.15488
56. Galluzzo M, Talamonti M, Cioni A, et al. Efficacy of tildrakizumab for the treatment of difficult-to-treat areas: scalp, nail, palmoplantar and genital psoriasis. J Clin Med. 2022;11(9):2631. doi:10.3390/jcm11092631
57. Ruggiero A, Fabbrocini G, Cinelli E, Megna M. Guselkumab and risankizumab for psoriasis: a 44-week indirect real-life comparison. J Am Acad Dermatol. 2021;85(4):1028–1030. doi:10.1016/j.jaad.2021.01.025
58. Rivera-Díaz R, LLamas-Velasco M, Hospital M, et al. Risankizumab in psoriasis: prior biologics failure does not impact on short-term effectiveness. Expert Opin Biol Ther. 2022;22(1):105–107. doi:10.1080/14712598.2022.2012567
59. Narcisi A, Valenti M, Cortese A, et al. Anti-IL17 and anti-IL23 biologic drugs for scalp psoriasis: a single-center retrospective comparative study. Dermatol Ther. 2022;35(2):e15228. doi:10.1111/dth.15228
60. Villani A, Megna M, Scalvenzi M, Fabbrocini G, Ruggiero A. Teledermatology and chronic skin diseases: real life experience in a Southern Italian Dermatologic Centre. Dermatol Ther. 2020;33(6):e13839. doi:10.1111/dth.13839
61. Napolitano M, Patruno C, Ruggiero A, Nocerino M, Fabbrocini G. Safety of dupilumab in atopic patients during COVID-19 outbreak. J Dermatolog Treat. 2022;33(1):600–601. doi:10.1080/09546634.2020.1771257
62. Marasca C, Ruggiero A, Megna M, Annunziata MC, Fabbrocini G. Biologics for patients affected by hidradenitis suppurativa in the COVID-19 era: data from a referral center of Southern Italy. J Dermatolog Treat. 2022;33(1):592. doi:10.1080/09546634.2020.1769828
63. Megna M, Potestio L, Gallo L, Caiazzo G, Ruggiero A, Fabbrocini G. Reply to “Psoriasis exacerbation after COVID-19 vaccination: report of 14 cases from a single centre” by Sotiriou E et al. J Eur Acad Dermatol Venereol. 2022;36(1):e11–e13.
64. Megna M, Potestio L, Camela E, Fabbrocini G, Ruggiero A. Ixekizumab and brodalumab indirect comparison in the treatment of moderate to severe psoriasis: results from an Italian single-center retrospective study in a real-life setting. Dermatol Ther. 2022;e15667. doi:10.1111/dth.15667
65. Marasca C, Ruggiero A, Napolitano M, Fabbrocini G, Megna M. May COVID-19 outbreaks lead to a worsening of skin chronic inflammatory conditions? Med Hypotheses. 2020;143:109853. doi:10.1016/j.mehy.2020.109853
66. Ruggiero A, Martora F, Picone V, et al. The impact of COVID-19 infection on psoriatic patients treated with biologics: an Italian experience. Clin Exp Dermatol. 2022. doi:10.1111/ced.15336
67. Potestio L, Genco L, Villani A, et al. Reply to ‘Cutaneous adverse effects of the available COVID-19 vaccines in India: a questionnaire-based study’. by Bawane J et al. J Eur Acad Dermatol Venereol. 2022. doi:10.1111/jdv.18341
68. Annunziata MC, Patrì A, Ruggiero A, et al. Cutaneous involvement during COVID-19 pandemic: an emerging sign of infection. J Eur Acad Dermatol Venereol. 2020;34(11):e680–e682. doi:10.1111/jdv.16769
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.