")
Back to Journals » International Journal of General Medicine » Volume 15
Group-Based Trajectory Modeling to Identify Factors Influencing the Development of Myopia in Patients Receiving Orthokeratology
Authors Duan C, Feng F, Liu L, Qu F, Yang Z, Zhang H, Jiang C
Received 21 December 2021
Accepted for publication 14 March 2022
Published 18 April 2022 Volume 2022:15 Pages 4151—4162
DOI https://doi.org/10.2147/IJGM.S355181
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Chunyu Duan,1 Fan Feng,1 Lijuan Liu,1 Fang Qu,1 Zhiye Yang,2 Hui Zhang,2 Chunguang Jiang1
1Pediatric Ophthalmology, Aier Eye Hospital Group, Kunming Air Eye Hospital, Kunming, Yunnan, 650200, People’s Republic of China; 2Physical Examination Center, Kunming Army Special Service Rehabilitation Center, Kunming, Yunnan, 650000, People’s Republic of China
Correspondence: Chunguang Jiang, Pediatric Ophthalmology, Kunming Aier Eye Hospital, No. 687 Huancheng South Road, Guandu District, Kunming City, Yunnan Province, 650200, People’s Republic of China, Tel + 86-15912177272, Email [email protected]
Purpose: To analyze the factors influencing the progression of myopia in adolescents receiving orthokeratology.
Methods: This prospective cohort study collected the data of 378 myopia patients receiving orthokeratology. The follow-up time was 12 months ranging from December 2015 to December 2019. The group-based trajectory modeling (GBTM) was used to identify similar developmental trajectories in the levels of uncorrected visual acuity and changes of axial length elongation. Univariate and multivariate logistic regression analyses were conducted to explore the influencing factors of myopia development in patients wearing orthokeratology.
Results: There was no factor having effect on visual acuity (left) and visual acuity (right) in different trajectories (all P> 0.05). The corneal curvature K1 (left) (OR=0.382, 95% CI: 0.188– 0.776), corneal curvature K2 (left) (OR=0.362, 95% CI: 0.187– 0.699), degree of spherical refraction (left) (OR=0.139, 95% CI: 0.082– 0.235) and spherical equivalent (left) (OR=7.276, 95% CI: 3.724– 14.215) were factors associated with the changes of axial length elongation (left). The corneal curvature K1 (right) (OR=0.260, 95% CI: 0.116– 0.585), corneal curvature K2 (left) (OR=0.272, 95% CI: 0.121– 0.610) and degree of spherical refraction (right) (OR=0.129, 95% CI: 0.068– 0.244) were correlated with the changes of axial length elongation (right). All P< 0.05.
Conclusion: Orthokeratology is a promising method for controlling the progression of myopia. The corneal curvature, degree of spherical refraction and spherical equivalent were factors influencing the changes of axial length elongation in myopia patients wearing orthokeratology. The findings might give a reference for the application of orthokeratology in clinic.
Keywords: group-based trajectory modeling, myopia, orthokeratology, factors
Introduction
Myopia has become a global public health problem. According to a previous study, about 30% of the global population is myopic, and the rate of it may increase to 50% by 2050.1 China has the second largest number of myopic teenagers with a prevalence of myopia as high as 59%.2 Myopia is one of the major causes of blindness, which seriously affects the health and quality of life in patients.3 It is imperative to find effective treatments to slow the progress of myopia. Currently, the treatments to slow the progression of myopia mainly include drugs, glasses, and laser surgery, and wearing orthokeratology is considered to be one of the most promising methods.4 Orthokeratology is a specially designed rigid contact lens with a flat center and steep sides worn on the cornea. Previous studies have confirmed that orthokeratology can effectively improve the naked visual acuity of patients and control the development of myopia in adolescents.5,6 Compared with surgery, orthokeratology is reversible and painless, which has become an important method for the control of myopia in teenagers and has been widely used in clinical treatment in recent years.7
Orthokeratology has achieved different efficacies in the treatment of adolescent myopia.6,8 Currently, the factors affecting the control of the progress of adolescent myopia by orthokeratology and the specific population suitable for orthokeratology have not been determined. According to previous studies, the axial length elongation change and initial orthokeratology wearing age were important factors affecting the efficacy of orthokeratology.9,10 Corneal curvature was also considered as an influencing factor for predicting the efficacy of orthokeratology.11 Another study was contradicted with this conclusion, showing that neither short-term nor long-term changes in corneal curvature were associated with the efficacy of orthokeratology in white European children.12 The factors influencing the efficacy of orthokeratology in adolescents were not consistent. This study collected the clinical data to analyze the factors influencing the progression of myopia in adolescents receiving orthokeratology treatments, which might provide a theoretical guidance for the use of orthokeratology in clinic.
Methods
Study Population
In this prospective cohort study, we enrolled 378 patients with myopia. The range of myopia in these patients was diopter ≤-6.00 D, corneal astigmatism≤-2.00 D, the best corrected visual acuity 0.5, and intraocular pressure within the normal range. Among them, we excluded 10 patients who were older than 18 years; 3 cases with contraindication for orthokeratology; 7 patients with amblyopia, strabismus, and abnormal visual function; and 358 patients were included and received orthokeratology, and the follow-up was performed. The follow-up time ranged from December 2015 to December 2019. The follow-up time was 12 months and the follow-up was conducted on 1 day, 3 months, 6 months and 12 months after wearing orthokeratology. The screen process is shown in Figure 1. The informed consents were obtained from the participants and this study was approved by the Ethics Committee of the Aier Eye Hospital Group, Kunming Air Eye Hospital. The current study complied with the Declaration of Helsinki.
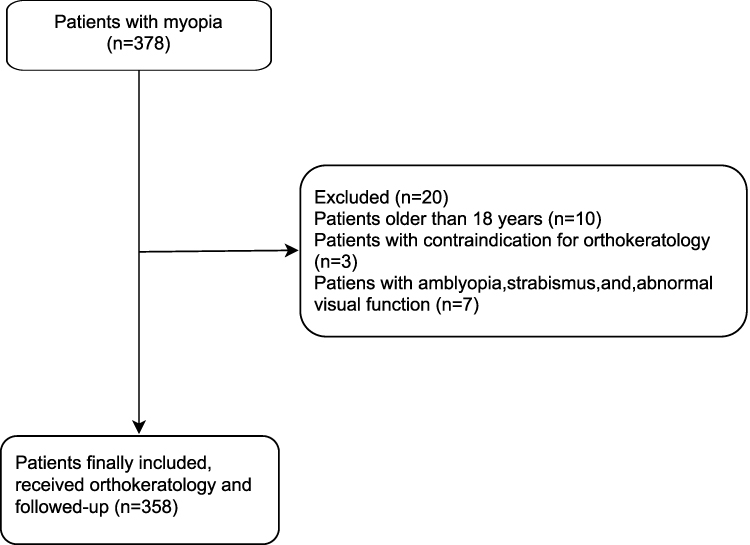 |
Figure 1 The screen process of the participants of the patients. |
Group-Based Trajectory Modeling
According to the purpose of the study, the group-based trajectory modeling (GBTM) was used to identify similar developmental trajectories in the levels of uncorrected visual acuity (diopter) and axial length elongation (mm). The survey wave was used as a timescale of trajectories to simulate the uncorrected visual acuity and axial length elongation trajectories in the sample in all waves. First, a base model without covariates was constructed to determine the number of groups and the order of the polynomial functions of the survey wave. The best-fitting model was considered as the trajectory group with the highest probability, which was based on goodness-of-fit statistics via the Bayesian information criterion (BIC) (the one whose absolute value of BIC is closest to zero is selected as the appropriate model). Second, each participant was assigned to the corresponding trajectory group according to the maximum likelihood estimation to estimate the probability of producing variance in uncorrected visual acuity and axial length elongation of each group. Third, univariate analysis and multivariate logistic regression analysis were applied to explore the influencing factors of the uncorrected visual acuity and axial length elongation at different points.
Data Collection
The clinical data of patients receiving orthokeratology were collected to evaluate the factors influencing the development of myopia. The data included wearing age (years), gender, allergic history, history of wearing glasses or orthokeratology, myopia time (month), origin of orthokeratology (China, America, Japanese or others), pupil diameter (left) (mm), pupil diameter (right) (mm), intraocular pressure (left) (mmHg), intraocular pressure (right) (mmHg), corneal curvature: K1 (left) (diopter), corneal curvature: K1 (right) (diopter), corneal curvature: K2 (left) (diopter), corneal curvature: K2 (right) (diopter), e value of corneal curvature (left), e value of corneal curvature (right), corneal thickness (left) (μm), corneal thickness (right) (μm), degree of spherical refraction (left), degree of spherical refraction (right), spherical equivalent (left) (diopter), spherical equivalent (right) (diopter), anterior chamber depth (left) (mm), anterior chamber depth (right) (mm).
Statistical Analysis
Statistical analyses were performed using SAS 9.4 and R 4.20 software. The measurement data of normal distribution were described as Mean ± standard deviation (Mean ± SD), and the independent sample t test and variance test were used for the comparisons between groups. The non-normal data were described as [M (Q1, Q3)], and the Mann–Whitney U rank sum test and Kruskal–Wallis H rank sum test were used for the comparisons between groups. The enumeration data were displayed as n (%). Chi-square test or Fisher’s exact probability method were applied for the comparisons between groups. Logistic regression was conducted to explore the influencing factors of myopia development in patients wearing orthokeratology. All statistical tests were conducted by two-sided tests, and P<0.05 was considered statistically significant.
Results
Trajectory Grouping of Visual Acuity and Axial Length Elongation
Based on GBTM, the visual acuity of left eye [visual acuity (left)] and visual acuity (right) respectively showed two different trajectories, while the axial length elongation (left) and axial length elongation (right) were respectively divided into three trajectories according to the baseline data of 1 day after wearing, 3 months after wearing, 6 months after wearing, and 12 months after wearing orthokeratology. As shown in Figure 2A, in terms of the visual acuity (left), in trajectory 1 (Group 1), the visual acuity (left) was at a low level, so it was defined as “low-initial level group” (n=240, 67.04%). In trajectory 2 (Group 2), the visual acuity (left) was at a high level, so it was defined as “high-initial level group” (n=118, 32.96%). Similarly, for visual acuity (right), trajectory 1 (Group 1) was defined as “low-initial level group” (n=229, 63.97%). Trajectory 2 (Group 2) was defined as “high-initial level group” (n=129, 36.03%) (Figure 2B). Regarding axial length elongation (left), the population of trajectory 1 (Group 1) had a low initial level, so it was defined as “low-initial level group” (n=124, 34.64%). In trajectory 2 (Group 2), the axial length elongation (left) had a medium initial level, and it was defined as “medium-initial level group” (n=195, 54.47%). In trajectory 3 (Group 3), the population had a relatively high level of axial length elongation initially, and it was defined as “high-initial level group” (n=39, 10.89%) (Figure 2C). Similarly, for the axial length elongation (right), trajectory 1 (Group 1) indicated “low-initial level group” (n=86, 24.02%); Trajectories type 2 (Group 2) was defined as “medium-initial level group” (n=181, 50.56%); Trajectory type 3 (Group 3) was defined as “high-initial level group” (n=91, 25.42%) (Figure 2D).
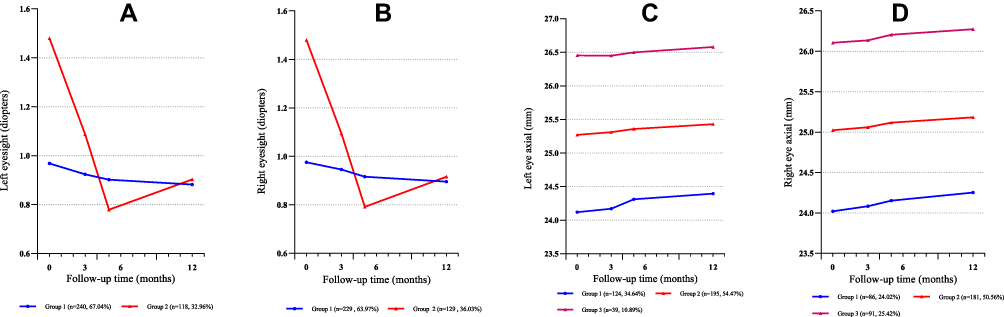 |
Figure 2 The trajectories of visual acuity (left) (A), visual acuity (right) (B), axial length elongation (left) (C) and axial length elongation (right) (D). |
The Baseline Characteristics of Participants
A total of 358 patients with myopia who wore orthokeratology were involved in this study. The average age of patients wearing orthokeratology was 12.08±2.40 years. Among them, 139 were males, which accounted for 38.83%. Seventy (19.55%) participants had a history of allergies. A total of 323 (90.22%) had a history of glasses or orthokeratology wearing. The median myopia time was 36 months. The origins of orthokeratology were from China, the United States, Japan or some other countries. There were 296 (82.68%) patients worn orthokeratology from China, 6 (1.68%) patients worn orthokeratology from the United States, and 36 (10.06%) patients worn orthokeratology from other countries (Table 1). As exhibited in Supplementary Table 1, the visual acuity (left) decreased −0.20 diopter, and the decrease of the visual acuity (left) was statistically different between Group 1 and Group 2 (0.00 diopter vs −0.50 diopter). The visual acuity (right) decreased −0.20 diopter, and the decrease was higher in Group 2 than Group 1 (−0.50 diopter vs 0.00 diopter) (Supplementary Table 2). In terms of the axial length elongation (left), the total elongation was 0.14 mm, and statistical difference was observed in the elongations of Group 1, Group 2 and Group 3 (Supplementary Table 3). The total elongation of the axial length elongation (right) was 0.16 mm, and no significant difference was found among the elongations in Group 1, Group 2 and Group 3 (Supplementary Table 4).
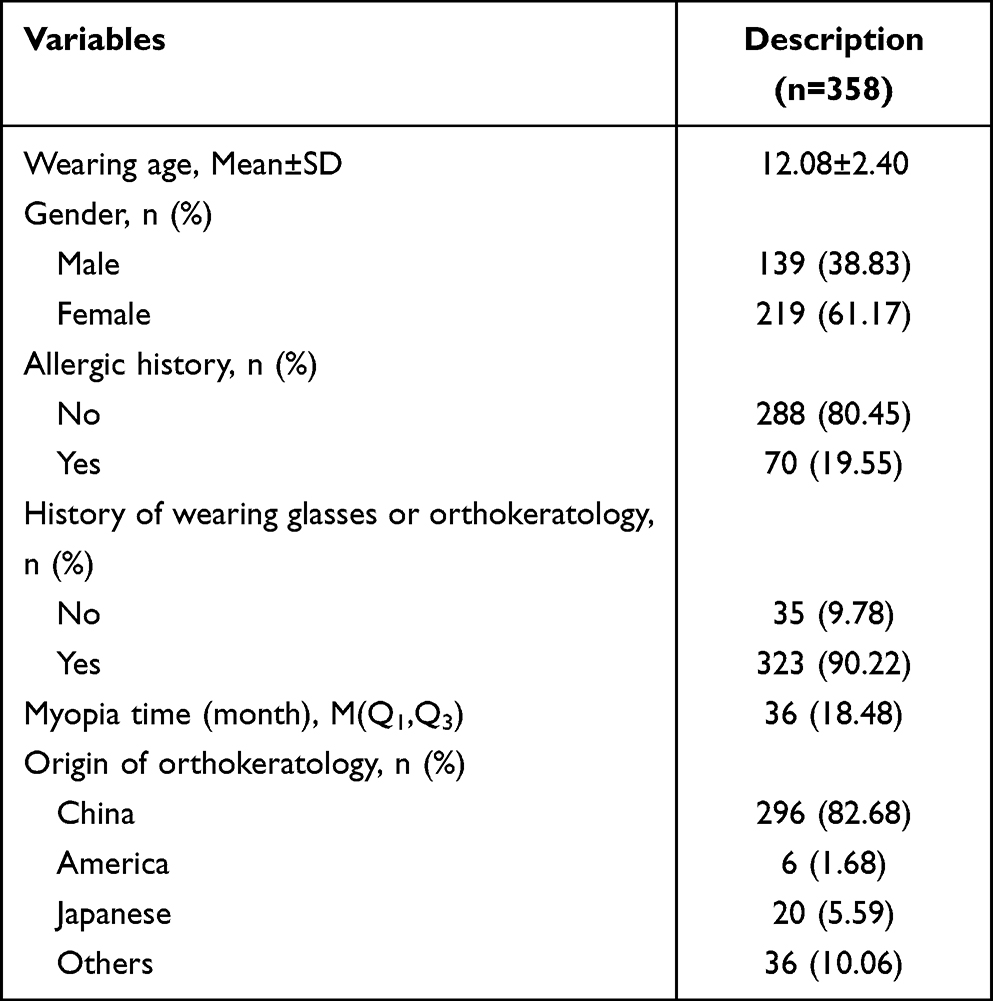 |
Table 1 The Baseline Characteristics of Participates |
Univariate Analysis of Factors Influencing Visual Acuity and Axial Length Elongation in Different Trajectories
As displayed in Tables 2 and 3, the data of univariate analysis delineated that there was no statistical difference in different trajectories in both visual acuity (right) and visual acuity (left). All P>0.05.
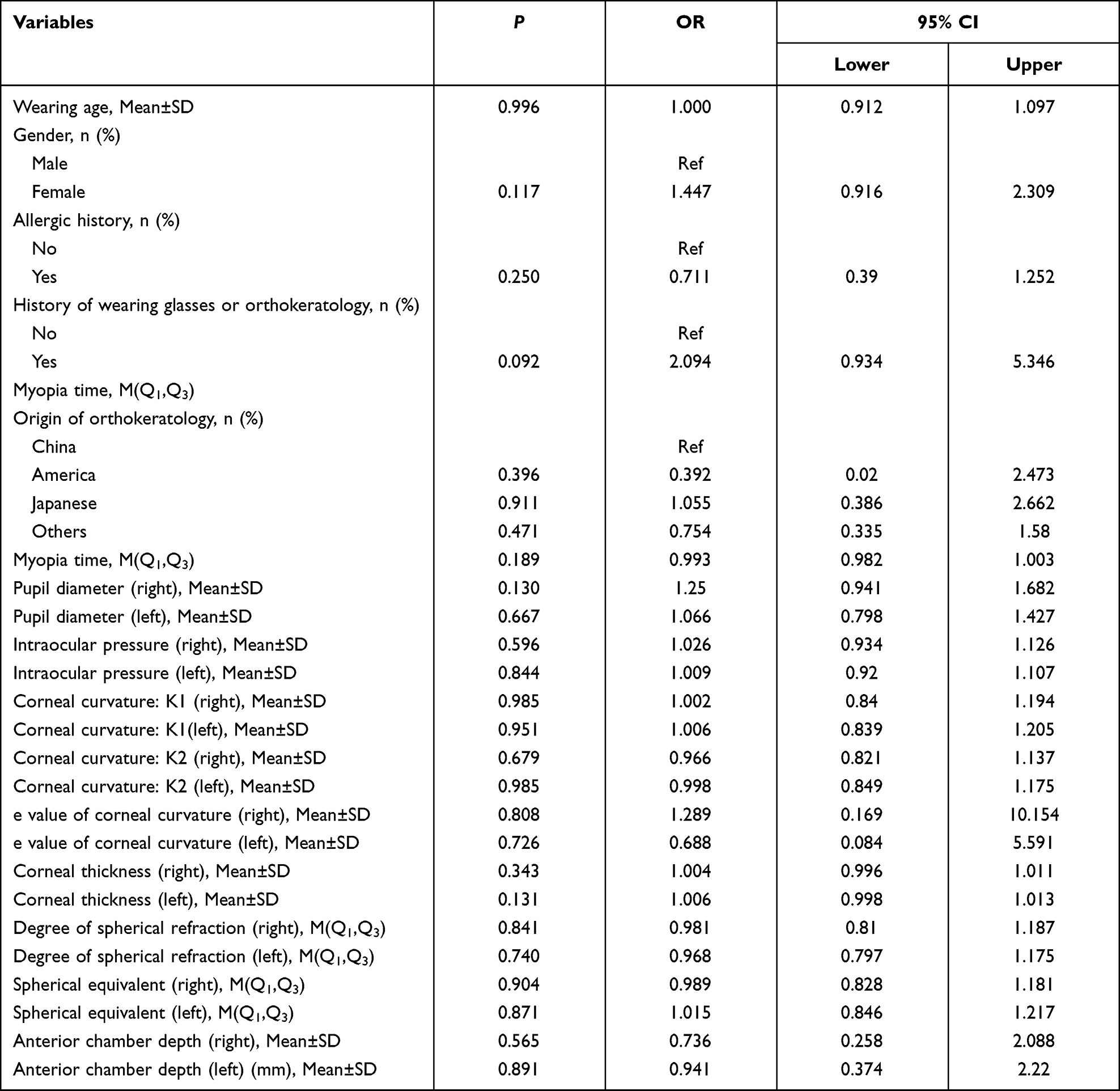 |
Table 2 Univariate Logistic Regression Results of Visual Acuity (Left) |
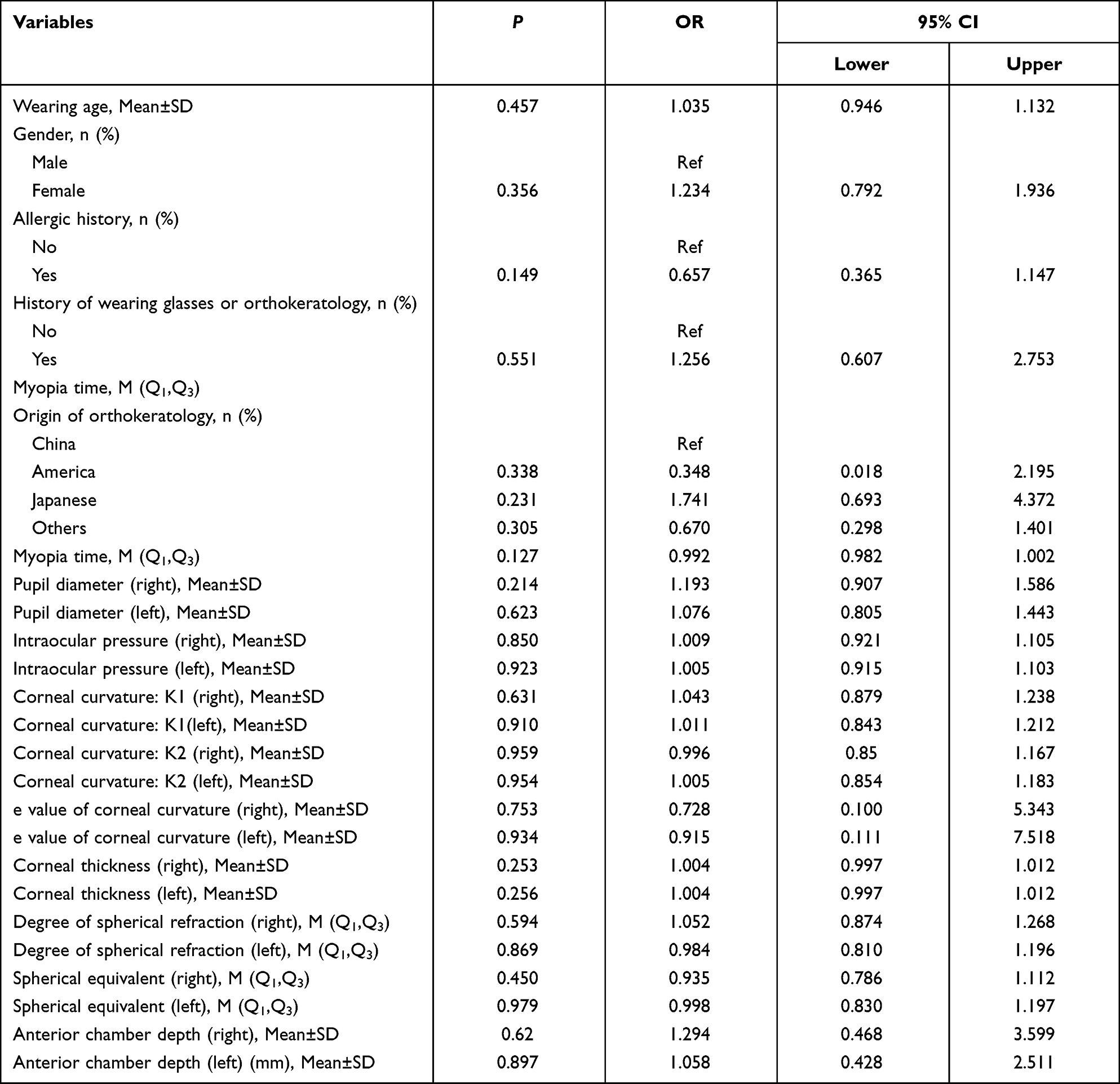 |
Table 3 Univariate Logistic Regression Results of Visual Acuity (Right) |
Regarding axial length elongation (left), the wearing age of orthokeratology (F=10.074, P<0.001), males (χ2=13.355, P=0.001), and myopia time (χ2=45.157, P<0.001), origin of orthokeratology (χ2=13.573, P=0.035), corneal curvature K1 (left) (F=67.522, P<0.001), corneal curvature K1 (right) (F=63.271, P<0.001), corneal curvature K2 (left) (F=57.621, P<0.001), corneal curvature K2 (right) (F=45.840, P<0.001), e value of corneal curvature (left) (F=3.308, P=0.038), e value of corneal curvature (right) (F=3.486, P=0.032), degree of spherical refraction (left) (χ2=86.682, P<0.001), degree of spherical refraction (right) (χ2=58.031, P<0.001), spherical equivalent (left) (χ2=80.901, P<0.001), spherical equivalent (right) (χ2=54.267, P<0.001), anterior chamber depth (left) (F=8.290, P<0.001) and anterior chamber depth (right) (F=12.054, P<0.001) levels were statistically different among three trajectories (Table 4).
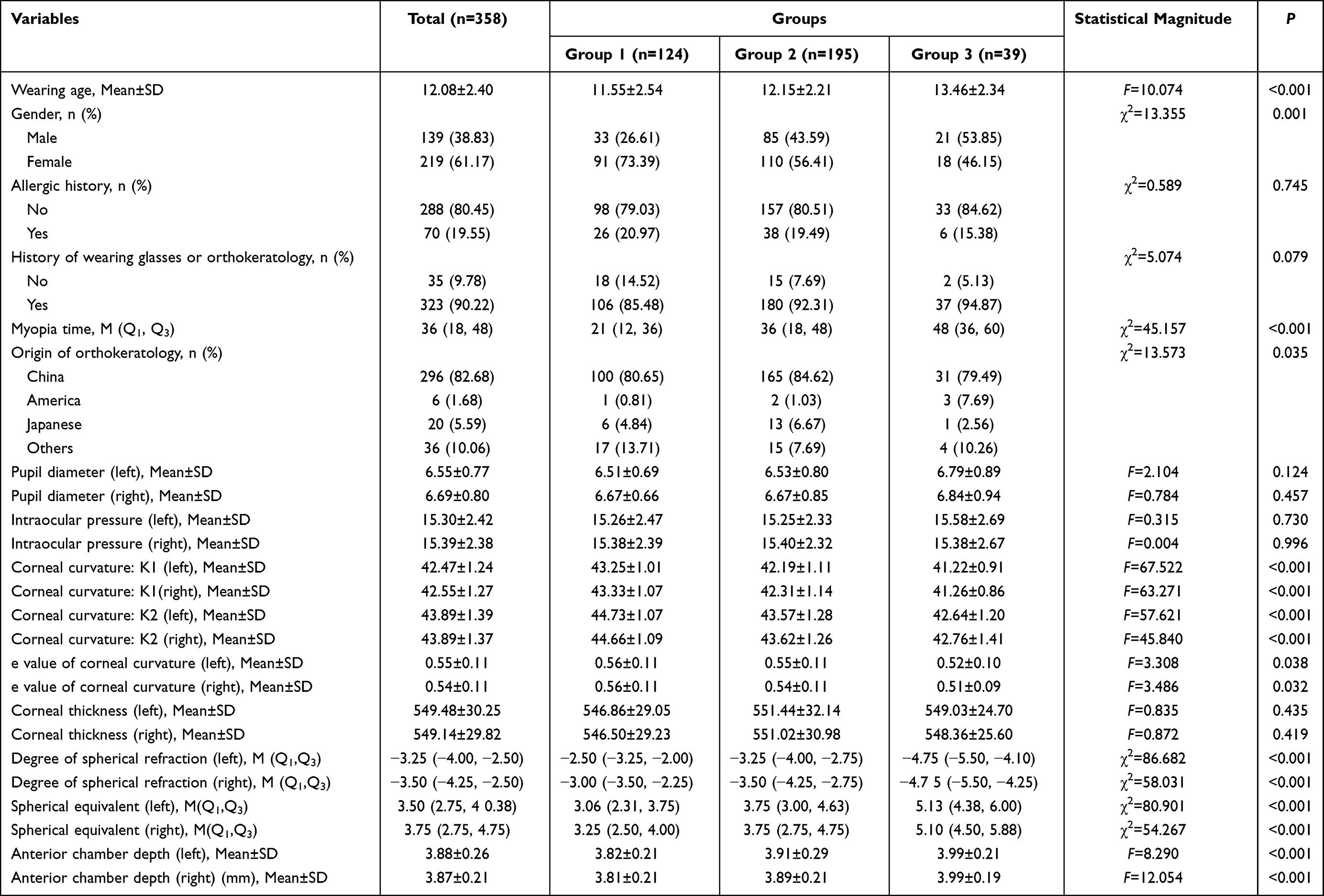 |
Table 4 Comparisons of Characters of Axial Length Elongation (Left) |
In different trajectories axial length elongation (right), the wearing age (F=8.774, P<0.001), males (χ2=19.853, P<0.001), history of wearing glasses or orthokeratology (χ2=7.218, P=0.027), myopia time (χ2=38.353, P<0.001), corneal curvature K1 (left) (F=82.776, P<0.001), corneal curvature K1 (right) (F=94.212, P<0.001), corneal curvature K2 (left) (F=65.051, P<0.001), corneal curvature K2 (right) (F=63.505, P<0.001), degree of spherical refraction (left) (χ2=40.912, P<0.001), degree of spherical refraction (right) (χ2=63.585, P<0.001), spherical equivalent (left) (χ2=39.820, P<0.001), spherical equivalent (right) (χ2=39.820, P<0.001), anterior chamber depth (left) (F=9.530, P<0.001) and anterior chamber depth (right) (F=15.406, P<0.001) (Table 5).
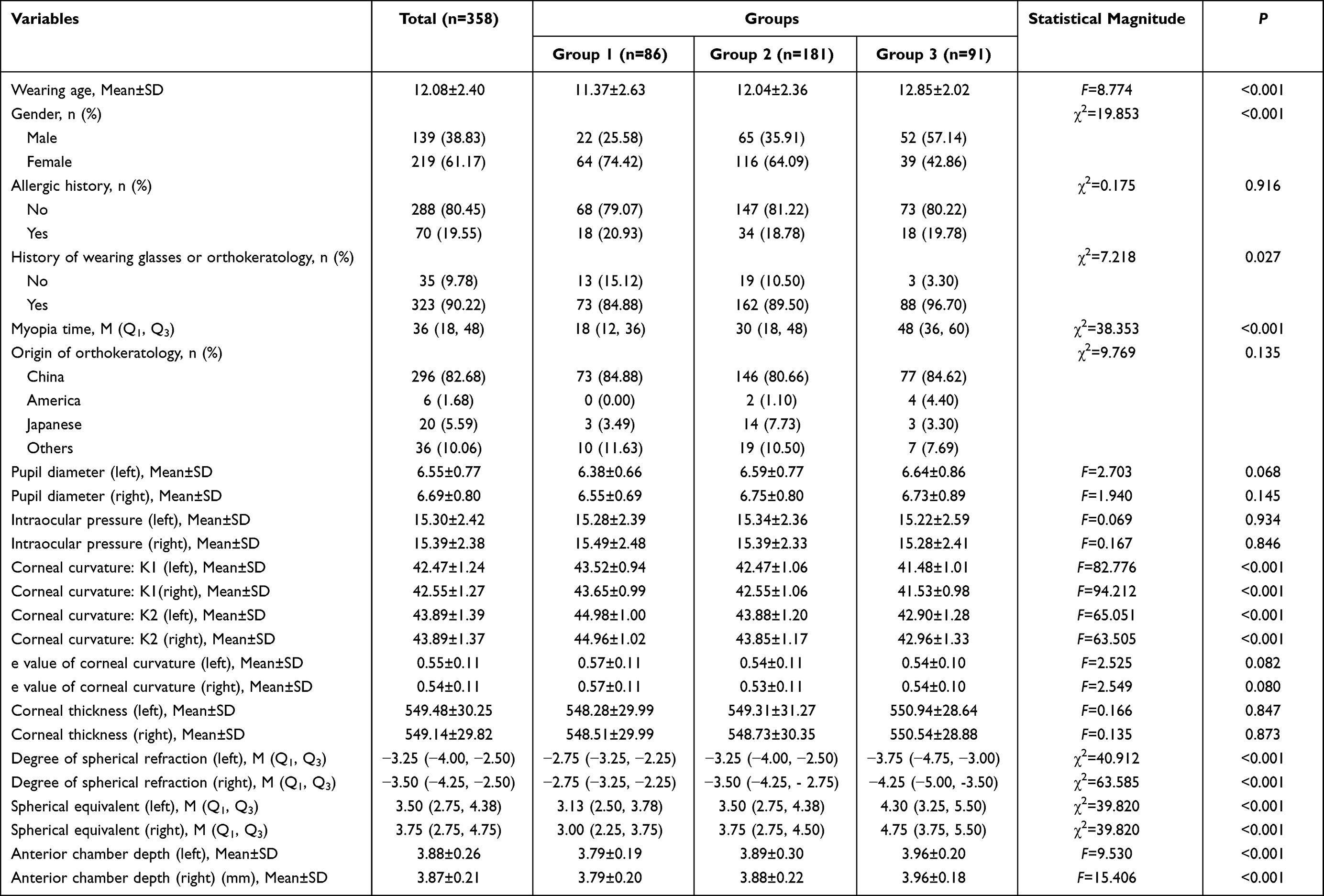 |
Table 5 Comparisons of Characters of Axial Length Elongation (Right) |
Multivariate Analysis of Factors Influencing Visual Acuity and Axial Length Elongation in Different Trajectories
According to results of the multivariate logistic regression analysis on the visual acuity (left) and visual acuity (right), no factor was found to have a statistical effect on visual acuity (left) and visual acuity (right). All P>0.05.
The data of multivariate logistic regression analysis on axial length elongation (left) showed that in Model 1, compared with Group 1, the corneal curvature K1 (left) (OR=0.382, 95% CI: 0.188–0.776, P=0.007), corneal curvature K2 (left) (OR=0.362, 95% CI: 0.187–0.699, P=0.003) and degree of spherical refraction (left) (OR=0.139, 95% CI: 0.082–0.235, P<0.001) were protective factors for the axial length elongation (left) in Group 2. In Model 2, compared with Group 1, spherical equivalent (left) (OR=7.276, 95% CI: 3.724–14.215, P<0.001) was a risk factor for the axial length elongation in Group 3 (Table 6).
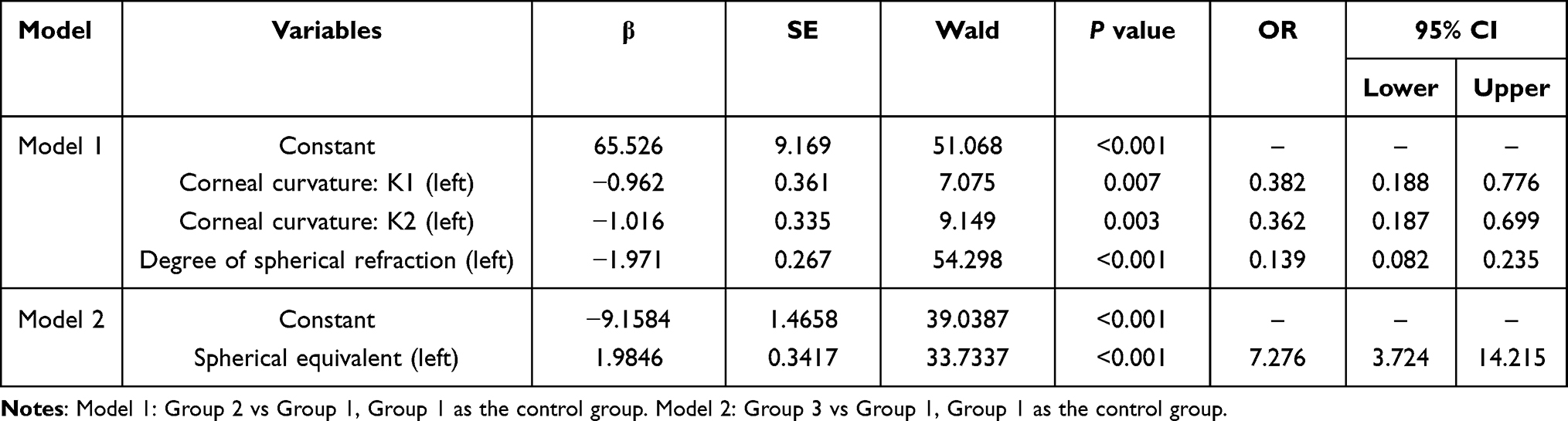 |
Table 6 Logistic Regression Analysis of Axial Length Elongation (Left) |
As shown in Table 7, the results of multivariate logistic regression analysis on axial length elongation (right) depicted that in Model 1, relative to Group 1, the corneal curvature K1 (right) (OR=0.260, 95% CI: 0.116–0.585, P=0.001), corneal curvature K2 (left) (OR=0.272, 95% CI: 0.121–0.610, P=0.002) and degree of spherical refraction (right) (OR=0.129, 95% CI: 0.068–0.244, P<0.001) were protective factors for the axial length elongation (right) in Group 2. In Model 2, compared with Group 1, the corneal curvature K1 (right) (OR=0.008, 95% CI: 0.001–0.123, P=0.001) and degree of spherical refraction (right) (OR=0.022, 95% CI: 0.002–0.233, P=0.002) were protective factors for axial length elongation (right) in Group 3.
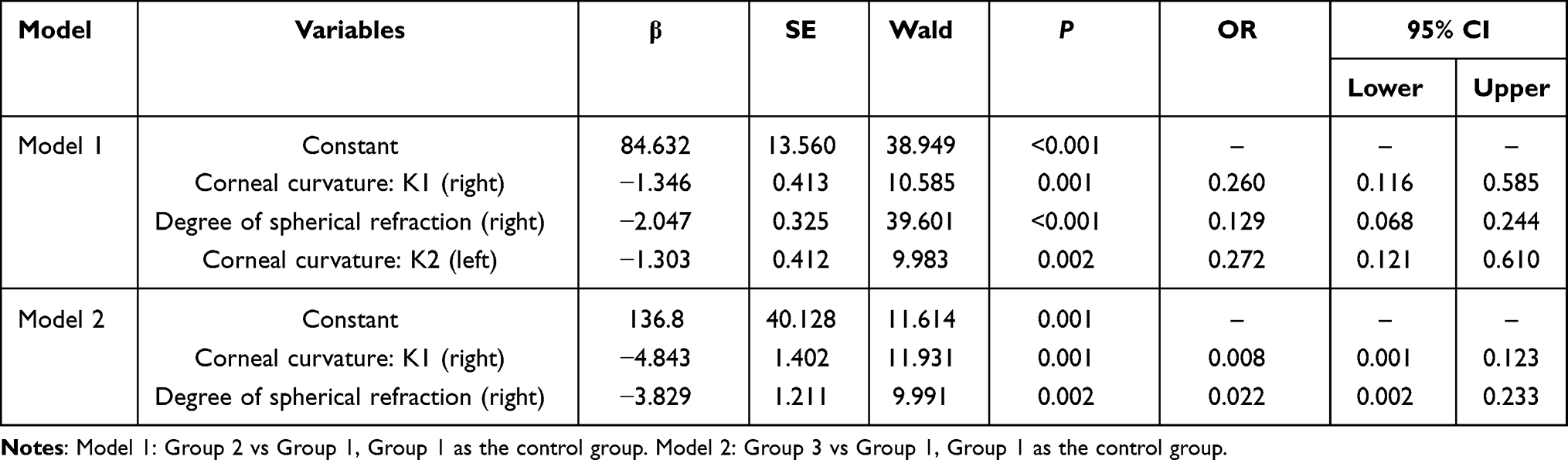 |
Table 7 Logistic Regression Analysis of Axial Length Elongation (Right) |
Discussion
This study analyzed the factors influencing the progression of myopia in 358 patients with orthokeratology. The results revealed that there was no factor having effects on visual acuity (left) and visual acuity (right) statistically in different trajectories. The corneal curvature K1 (left), corneal curvature K2 (left), degree of spherical refraction (left) and spherical equivalent (left) were factors associated with the changes of axial length elongation (left). The corneal curvature K1 (right), corneal curvature K2 (left) and degree of spherical refraction (right) levels were correlated with the changes of axial length elongation (right). The findings of our study might help identify patients suitable for using orthokeratology.
The axial length elongation of the eyeball is the main reason for the gradual deepening of myopia and is regarded as an index of myopic progression.13 Under normal circumstances, the axial length of the eyes is about 21 mm in children aged 5–6 years, 21.5 mm in children aged 7–8 years, 22 mm in children aged 9–10 years, 24 mm in children aged 17–18 years. In clinic, the axial length greater than 24 mm is considered myopia.14 Kong et al followed up 724 myopic children with orthokeratology for 6 months-65 months, and found that corneal curvature was an independent factor affecting the control effect of myopia.15 A previous study revealed that the corneal curvature might be a predictor for the changes of axial length elongation in myopic children with orthokeratology.16 Zhong et al analyzed the changes of corneal curvature before and after wearing orthokeratology in 32 myopic children and found that the changes of axial length elongation were 54–69% slower in those with higher levels of corneal curvature.17 According to the data in a study of Kang et al, orthokeratology can cause significant changes in the peripheral corneal refraction and corneal topography, especially on the first night of wearing, the peripheral corneal refraction and corneal refractive power in patients on the meridian level have the greatest changes, and the peripheral retina also produce myopic defocus.18 Corneal curvature includes the horizontal keratometry (K1) and vertical keratometry (K2).19 In our study, the results showed that the corneal curvature K1 (left) and corneal curvature K2 (left) were protective factors for the axial length elongation (left). Additionally, the corneal curvature K1 (right) and corneal curvature K2 (left) were protective factors for the axial length elongation (right) in Group 2, indicating a higher corneal curvature was negatively correlated with the changes of axial length elongation in patients with medium initial level of axial length. The degree of spherical refraction represents the degree of myopia or hypermetropia and minus indicates myopia in patients.20 A previous study demonstrated that a higher myopia degree could lead to a better effect on myopia controlling in patients wearing orthokeratology.21 The study of Kakita et al also confirmed that the effect of orthokeratology was better on patients with higher degrees of myopia.22 Herein, the degree of spherical refraction was identified as a protective factor in patients with medium initial levels compared with low initial levels, suggesting a higher initial degree of spherical refraction may have better effects on myopia control in patients with orthokeratology. This may be due to the myopic defocus around the retina can delay or prevent the increase of myopia. Patients with a higher degree of myopia can achieve better shaping degree and change in peripheral refractive light by orthokeratology. Previously, a study reported that the degree of spherical equivalent was negatively associated with the changes of diopter in adolescents wearing orthokeratology.23 In the current study, compared with Group 1, spherical equivalent was a risk factor for the axial length elongation in Group 3, suggesting a higher spherical equivalent degree might have a longer axial length elongation (left) in patients. This may be due to the small samples in Group 3 of left eyes. Although this was not consistent with the results in previous studies, orthokeratology had good overall effects in controlling axial length elongation in all three groups.
The present study evaluated the factors affecting the development of myopia in patients receiving orthokeratology based on GBTM. GBTMs are substantially being used in clinical research to map the developmental course of symptoms and assess heterogeneity in response to clinical interventions.24 GBTMs could clearly observe the development trajectories of development of myopia at different time points. The results delineated that the trajectories visual acuity in both groups achieved good controlling effects after 1 year. The trajectories of axial length elongation after wearing orthokeratology all developed slowly. These data suggested that orthokeratology could effectively control the development of myopia, which might be a promising method for myopia treatment in the clinic. There were some limitations in the present study. Firstly, the corneal curvature K2 of the left eye was identified as a factor influencing the axial length elongation of the right eye, but the deep regulatory mechanisms of it was not explored in this study and required to be investigated in further studies. Secondly, the small sample size was relatively small in Group 3 of left eyes, which might decrease the statistical power of our study. Thirdly, we did not explore whether the results may differ in patients of left-handed and right-handed and the influence of the dominant eye of the patients was not determined. In the future, more well-signed studies with large scale sample size were called for to confirm the findings of this study.
Conclusions
Our study analyzed the factors associated with the progression of myopia patients with orthokeratology via GBTM. The results depicted that the corneal curvature, degree of spherical refraction and spherical equivalent were factors associated with the changes of axial length elongation in myopia patients. Orthokeratology may be a promising method for controlling the progression of myopia. The findings might give a reference for the application of orthokeratology in clinic.
Ethics Approval and Informed Consent
The informed consents were obtained from the participants and this study was approved by the Ethics Committee of the Aier Eye Hospital Group, Kunming Air Eye Hospital ((2019) 0102). Written informed consents were obtained from the participants. All methods were performed in accordance with the relevant guidelines and regulations.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study received no funding.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Holden BA, Fricke TR, Wilson DA, et al. Global prevalence of myopia and high myopia and temporal trends from 2000 through 2050. Ophthalmology. 2016;123:1036–1042. doi:10.1016/j.ophtha.2016.01.006
2. Rudnicka AR, Kapetanakis VV, Wathern AK, et al. Global variations and time trends in the prevalence of childhood myopia, a systematic review and quantitative meta-analysis: implications for aetiology and early prevention. Br J Ophthalmol. 2016;100:882–890. doi:10.1136/bjophthalmol-2015-307724
3. Hosoda Y, Yoshikawa M, Miyake M, et al. CCDC102B confers risk of low vision and blindness in high myopia. Nat Commun. 2018;9:1782. doi:10.1038/s41467-018-03649-3
4. Santodomingo-Rubido J, Villa-Collar C, Gilmartin B, et al. Short- and long-term changes in corneal aberrations and axial length induced by orthokeratology in children are not correlated. Eye Contact Lens. 2017;43:358–363. doi:10.1097/ICL.0000000000000290
5. Tay SA, Farzavandi S, Tan D. Interventions to reduce myopia progression in children. Strabismus. 2017;25:23–32.
6. Cho P, Tan Q. Myopia and orthokeratology for myopia control. Clin Exp Optom. 2019;102:364–377. doi:10.1111/cxo.12839
7. Liu YM, Xie P. The safety of Orthokeratology–A systematic review. Eye Contact Lens. 2016;42:35–42. doi:10.1097/ICL.0000000000000219
8. Lee YC, Wang JH, Chiu CJ. Effect of Orthokeratology on myopia progression: twelve-year results of a retrospective cohort study. BMC Ophthalmol. 2017;17:243. doi:10.1186/s12886-017-0639-4
9. Swarbrick HA, Alharbi A, Watt K, et al. Myopia control during orthokeratology lens wear in children using a novel study design. Ophthalmology. 2015;122:620–630. doi:10.1016/j.ophtha.2014.09.028
10. Wang J, Yang D, Bi H, et al. A new method to analyze the relative corneal refractive power and its association to myopic progression control with orthokeratology. Transl Vis Sci Technol. 2018;7:17. doi:10.1167/tvst.7.6.17
11. Cheung SW, Boost MV, Cho P. Pre-treatment observation of axial elongation for evidence-based selection of children in Hong Kong for myopia control. Cont Lens Anterior Eye. 2019;42:392–398. doi:10.1016/j.clae.2018.10.006
12. Santodomingo-Rubido J, Villa-Collar C, Gilmartin B, et al. Short-term and long-term changes in corneal power are not correlated with axial elongation of the eye induced by orthokeratology in children. Eye Contact Lens. 2018;44:260–267. doi:10.1097/ICL.0000000000000313
13. Huang J, Wen D, Wang Q, et al. Efficacy comparison of 16 interventions for myopia control in children: a network meta-analysis. Ophthalmology. 2016;123:697–708. doi:10.1016/j.ophtha.2015.11.010
14. Wei S, Li SM, An W, et al. Safety and efficacy of low-dose atropine eyedrops for the treatment of myopia progression in Chinese children: a Randomized Clinical Trial. JAMA Ophthalmol. 2020;138:1178–1184. doi:10.1001/jamaophthalmol.2020.3820
15. Kong Q, Guo J, Zhou J, et al. Factors determining effective orthokeratology treatment for controlling juvenile myopia progression. Iran J Public Health. 2017;46:1217–1222.
16. Wan K, Cheung SW, Wolffsohn JS, et al. Role of corneal biomechanical properties in predicting of speed of myopic progression in children wearing orthokeratology lenses or single-vision spectacles. BMJ Open Ophthalmol. 2018;3:e000204. doi:10.1136/bmjophth-2018-000204
17. Zhong Y, Chen Z, Xue F, et al. Corneal power change is predictive of myopia progression in orthokeratology. Optom Vis Sci. 2014;91:404–411. doi:10.1097/OPX.0000000000000183
18. Kang P, Swarbrick H. Time course of the effects of orthokeratology on peripheral refraction and corneal topography. Ophthalmic Physiol Opt. 2013;33:277–282. doi:10.1111/opo.12027
19. Aksoy M, Asena L, Güngör SG, et al. Comparison of refractive outcomes using Scheimpflug Holladay equivalent keratometry or IOLMaster 700 keratometry for IOL power calculation. Int Ophthalmol. 2021;41:2205–2212. doi:10.1007/s10792-021-01781-6
20. Li Y, Li S, Zhou J, et al. Relationship between lipid layer thickness, incomplete blinking rate and tear film instability in patients with different myopia degrees after small-incision lenticule extraction. PLoS One. 2020;15:e0230119. doi:10.1371/journal.pone.0230119
21. Hiraoka T, Kakita T, Okamoto F, et al. Long-term effect of overnight orthokeratology on axial length elongation in childhood myopia: a 5-year follow-up study. Invest Ophthalmol Vis Sci. 2012;53:3913–3919. doi:10.1167/iovs.11-8453
22. Kakita T, Hiraoka T, Oshika T. Influence of overnight orthokeratology on axial elongation in childhood myopia. Invest Ophthalmol Vis Sci. 2011;52:2170–2174. doi:10.1167/iovs.10-5485
23. Cho P, Cheung SW. Retardation of myopia in Orthokeratology (ROMIO) study: a 2-year randomized clinical trial. Invest Ophthalmol Vis Sci. 2012;53:7077–7085. doi:10.1167/iovs.12-10565
24. Nagin DS, Odgers CL. Group-based trajectory modeling in clinical research. Annu Rev Clin Psychol. 2010;6:109–138. doi:10.1146/annurev.clinpsy.121208.131413
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.