")
Back to Journals » Clinical Ophthalmology » Volume 15
Granulomatous Features in Juvenile Idiopathic Arthritis-Associated Uveitis is Not a Rare Occurrence
Authors Papasavvas I , Herbort CP Jr
Received 6 January 2021
Accepted for publication 15 February 2021
Published 8 March 2021 Volume 2021:15 Pages 1055—1059
DOI https://doi.org/10.2147/OPTH.S299436
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Ioannis Papasavvas, Carl P Herbort Jr
Retinal and Inflammatory Eye Diseases, Centre for Ophthalmic Specialized Care (COS), Clinic Montchoisi Teaching Centre, Lausanne, Switzerland
Correspondence: Carl P Herbort Jr
Centre for Ophthalmic Specialised Care, Montchoisi Teaching Centre, Rue Charles-Monnard 6, Lausanne, Switzerland
Email [email protected]
Background: Juvenile idiopathic arthritis (JIA)-associated uveitis is the most common form of intraocular inflammation with systemic involvement in childhood. Textbooks tend to describe it as non-granulomatous anterior uveitis. Here, we report the percentage of granulomatous features in JIA-related uveitis among patients at a uveitis referral center.
Methods: We conducted a retrospective study of all patients with JIA-related uveitis who were seen at the Center for Ophthalmic Specialized Care in Lausanne between 2000 and 2020. The sample comprised pediatric patients with bilateral anterior uveitis diagnosed as JIA-related with positive antinuclear antibody (ANA) titers. Exclusion criteria were a positive Mantoux or Quantiferon® test or elevated serum lysozyme and/or angiotensin converting enzyme (ACE) levels. The presence of one of the following features qualified the uveitis as granulomatous: granulomatous keratic precipitates (KPs) of mutton-fat type, smaller granulomatous KPs, or Koeppe nodules. The amount of inflammation was measured using laser flare photometry.
Results: Thirty-eight patients were identified (mean age 13.34 ± 2.71 years; all female). In 12 patients (31.5%), the uveitis presented granulomatous features at presentation or during follow-up in at least one eye. Two of the 12 (16%) granulomatous patients had only light or no systemic involvement. The mean flare was 136.3± 149 ph/ms, which is much higher than granulomatous uveitis entities of other origin reported in the literature.
Conclusion: JIA related uveitis can have a granulomatous presentation in about one third of patients with the Oligoarticular type and ANA positive, seen in a uveitis referral center. The presence of granulomatous features in bilateral uveitis in ANA-positive pediatric patients should not exclude the diagnosis of JIA-related uveitis, even in the absence of systemic involvement, as this entity presents a much more severe uveitis than other granulomatous anterior uveitis entities.
Keywords: JIA-related uveitis, anterior uveitis, non-granulomatous anterior uveitis, granulomatous anterior uveitis, laser flare photometry
Introduction
Anterior uveitis is classically divided into non-granulomatous and granulomatous entities. This classification is very useful because it corresponds to different specific entities and helps in the work-up of uveitis cases. Non-granulomatous uveitis is principally characterized by fine and diffuse endothelial keratic precipitates (KPs) in the lower half of the cornea, which appear as dust on the endothelium but are not visible by slit-lamp photography. One of the characteristic features of granulomatous uveitis is the presence of KPs larger than dust that can be individually photographed.1 Granulomatous KPs can be small as in Fuchs’ uveitis, medium-sized as in herpetic kerato-uveitis, or large (mutton-fat KPs) as in tuberculous or sarcoidosis uveitis. Other features of granulomatous uveitis include Koeppe nodules, fluffy small outgrowths on the pupillary edge or on the surface of the iris, and Busacca nodules within the stroma of the iris. The term granulomatous uveitis is a misnomer, as it uses a histological term applied to a set of clinical signs. Conditions presenting with non-granulomatous uveitis typically comprise HLA-B27 uveitis and Behçet’s uveitis. Conditions presenting with a granulomatous uveitis typically include uveitis caused by herpes, sarcoidosis, or tuberculosis. Fuchs’ uveitis is often erroneously classified as non-granulomatous, but it is a genuine granulomatous uveitis with stellate KPs that are easily identifiable and, in many cases, with Koeppe nodules.2
Juvenile idiopathic arthritis-associated uveitis (JIA-uveitis) is the most common uveitis related to a systemic disease in childhood. JIA-uveitis has been classified as a non-granulomatous uveitis and is still currently in articles and textbooks, confusing clinicians and creating problems in differential diagnosis. We consulted chapters on JIA-uveitis in 11 textbooks published in the UK, USA, France, and Germany.3–13 In all but one of these chapters, JIA-uveitis was qualified as non-granulomatous. In the other chapter, JIA-uveitis was described as potentially granulomatous in the following terms: “In the vast majority, the intraocular inflammation is non-granulomatous, although Koeppe nodules and mutton-fat KPs may rarely be seen”.8 After having seen several cases of JIA-uveitis with clearly granulomatous signs, the purpose of this study was to identify the proportion of granulomatous JIA-uveitis cases among our collective cases.
Methods
We conducted a retrospective study of all uveitis patients seen at the Center of Specialized Care in Lausanne between 2000 and 2020, identifying granulomatous signs at presentation or during follow-up in patients with JIA-uveitis. All patients referred to or directly seen at our center with the diagnosis of JIA-uveitis who had positive and elevated ANA titers (> 1/160) were included in this study. Exclusion criteria were a positive Mantoux test or a positive Tuberculosis IGRA test (interferon gamma test), elevated serum lysozyme, and/or elevated serum ACE when these investigations were performed.
Medium and large KPs (Figure 1), Koeppe nodules, and/or Busacca nodules were the signs considered as granulomatous in patients with JIA-uveitis at presentation or during the follow-up.
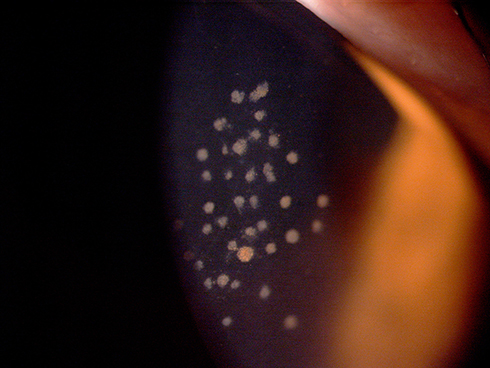 |
Figure 1 Presence of medium-sized keratic precipitates in a young girl with JIA-uveitis. |
Laser flare photometry (LFP) was performed the same day the granulomatous signs were detected. We used a Kowa FM-700 laser flare photometer following a previously described protocol.14
Results
Demographics
A total of 38 patients were diagnosed with JIA-related uveitis ANA positive. All patients were females. The patients’ ANA titers were between 1/160 and 1/1280. Mean age at presentation was 13.34 ± 2.71 years. Mean visual acuity at presentation was 0.72 ± 0.40 on a Snellen chart. Mean age of arthritis onset was 5.3 ± 1.7
Proportion of Granulomatous Uveitis
Twelve of the 38 patients (31.5%) had granulomatous signs at presentation or during follow up (Table 1). Eleven of these 12 (91%) patients had bilateral inflammation, whether granulomatous or not. One patient had unilateral granulomatous uveitis. Three patients presented with bilateral granulomatous uveitis, whereas nine had unilateral granulomatous signs (total number of eyes = 15). The KPs were distributed in the inferior cornea in nine eyes and the distribution diffuse in six eyes. Koeppe nodules (Figure 2A and B) were noted in three eyes. Two of the 12 patients had light or no systemic involvement, meaning that no systemic treatment was necessary.
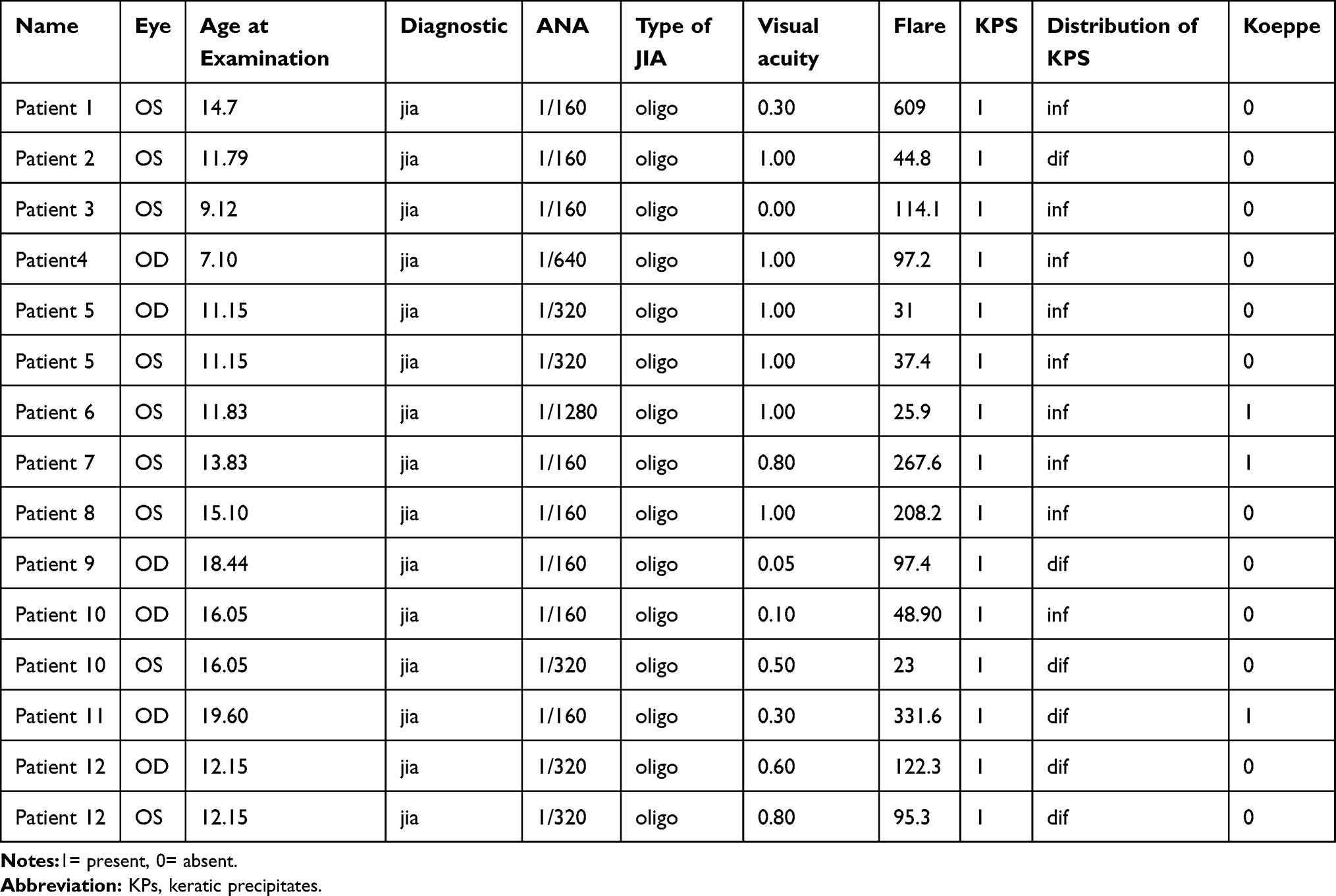 |
Table 1 Eyes That Presented Granulomatous Signs in Juvenile Idiopathic Arthritis (JIA)-RelatedUveitis |
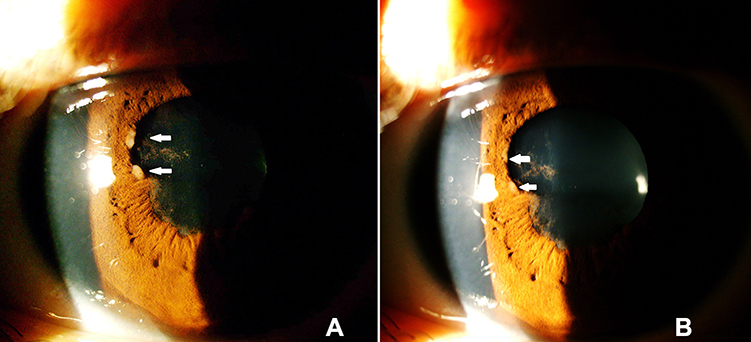 |
Figure 2 (A) Koeppe nodules (arrows) in a patient with exacerbation of JIA-related uveitis. (B) Same patient after treatment. The Koeppe nodules had disappeared (arrows points were the nodules were before treatment) but posterior synechiae persisted. |
Laser Flare Photometry
Mean flare values were 136.3±149 photons/milliseconds (ph/ms) in the 12 granulomatous JIA-uveitis patients (normal values 4–6 ph/ms). The mean flare values measured by LFP in JIA-uveitis were much higher than those reported for granulomatous uveitis of other origin (38.1±11 in sarcoidosis and 25.8±6.1 in zoster uveitis).15
Discussion
Our results show that a substantial proportion (ie one-third) of JIA related uveitis cases of oligoarticular type with ANA positive were granulomatous in at least one eye, which does not support JIA-uveitis being strictly qualified as non-granulomatous. In the literature, we found only one report that aimed to look at the clinical expression of JIA-uveitis and search for granulomatous signs.16 In the latter study, the proportion of granulomatous uveitis cases was 28% when all patients were considered, including White (62/71) and Black or Hispanic patients (9/71) but only 25% when only White patients were considered. The granulomatous signs were identified at presentation and/or during follow-up, as was the case in our study. Our percentage of patients with granulomatous signs was higher than that found by Keenan et al, even though all our patients were white Caucasians. We suspect that the percentage in our study was higher because the Keenan et al study included patients with oligo-articular, poly-articular, and enthesitis type JIA-related uveitis, regardless of the presence of ANA, in contrast to our study in which only oligo-articular JIA patients with elevated ANA titers were included.
In 1988, Kanski17 noted that 1 of 315 patients had mutton-fat KPs, and some patients with Koeppe nodules, but the vast majority of JIA-related uveitis was non-granulomatous. Dana et al found that 93% of 76 eyes were non-granulomatous, implying by inference that 7% were granulomatous without giving details on the signs found.18
As shown in our study, the non-granulomatous character of JIA-uveitis is far from overwhelming as described in the vast majority of textbooks. This can probably be explained by the fact that early reports stressed the non-granulomatous feature, reporting very rare, exceptional granulomatous signs.17 Thereafter, the formulation in Kanski’s article was taken up verbatim in subsequent textbooks.10,11 It is worth relativizing the importance of the non-granulomatous aspect in the definition of JIA-uveitis and considering a whole set of criteria, including epidemiological facts (young girls), the type of arthritis (oligo-articular), presence of elevated antinuclear antibodies, frequent bilaterality, and high severity of the uveitis. In this regard, LFP showed us that the amount of inflammation in our series was much higher than granulomatous uveitis entities of other origin.15
We could exclude other diagnoses occurring in children that present with arthritis and granulomatous uveitis, such as childhood sarcoidosis and/or Blau syndrome. Lysozyme and ACE were negative in all patients in our series, and after a prolonged follow-up, none of our patients presented clinical signs of sarcoidosis or signs compatible with Blau syndrome, which is characterized by arthritis, granulomatous panuveitis, and a rash in children younger than 5 years.19,20
Conclusion
The presence of granulomatous signs should not lead to excluding the diagnosis of JIA-uveitis, as 1 out of 3 patients with oligo-articular, ANA+ uveitis can present such signs. The whole set of criteria should be looked for to diagnose JIA-uveitis early, which is crucial for early treatment of an often silent uveitis that is potentially deleterious to the eye.
Ethics
The study was performed in accordance with the ethical standards laid down in the Declaration of Helsinki and in accordance with the IRB of our institution (Ethical Committee of the Centre of Ophthalmic Specialised care and Montchoisi Teaching Centre, protocol number: EC-COS-MTC-20-12-01) authorizing retrospective, anonymous and non-interventional studies. Parental informed consent statement was signed,authorizing review of medical records.
Disclosure
The authors report no conflicts on interest in this work.
References
1. Herbort CP. Appraisal, work-up and diagnosis of anterior uveitis: a practical approach. Middle East Afr J Ophthalmol. 2009;16:159–167. doi:10.4103/0974-9233.58416
2. Herbort CP, Bouchenaki N. Fuchs’ uveitis. In: Gupta A, Gupta V, Herbort CP, Khairallah M, editors. Uveitis, Text and Imaging. New Delhi: Jaypee Brothers Medical Publishers; 2009:323–332.
3. Read RW, Acharya N, Levinson RD, Kumar Rao P, Nida Sen H, Vasconelos-Santos WJ. 2018-2019 Basic and Clinical Science Course (BCSC), Section 9: Intraocular Inflammation and Uveitis.American Academy of Ophthalmology. 2015; 126–128. revised for currency September 2017.
4. Smith RE, Nozik RA, editors, Uveitis. A Clinical Approach to Diagnosis and Management. Williams & Wilkins: Baltimore; 1983:155–157.
5. Kanski JJ, editor, Uveitis. A Colour Manuel of Diagnosis and Treatment. Butterworths & Co: London; 1987:15–20.
6. Opremcak EM, editor, Uveitis, a Clinical Manual for Ocular Inflammation. New York: Springer-Verlag Inc; 1995:205–207.
7. Nussenblatt RB, Whitcup SM, Palestine AG, editors. Juvenile rhumatoid arthritis. Uveitis: Fundamentals and Clinical Practice
8. Kanski JJ, Petty RE. Chronic childhood arthritis and uveitis. In: Pepose JS, Holland GN, Wilhelmus KR, editors. Ocular Infection and Immunity. Saint Louis: Mosby-Year Book, Inc.; 1996:485–493.
9. Jones NP, editor, Uveitis, an Illustrated Manual. Oxford: Butterworth-Heinemann; 1998:129–135.
10. Kanski JJ, Pavésio CE, Tuft SJ, editors, Ocular Inflammatory Disease. Elsevier-Mosby: Philadelphia; 2006:165–167.
11. Heiligenhaus A, Heinz C, Hennig M, Niewerth M, Minden K. Juvenile Idiopathic arthritis; psoriatic arthritis and ankylosing spondylitis. In: Pleyer, editor. Entzündliche Augenerkrankungen. Berlin, Heidelberg: Springer-Verlag; 2014:319–330.
12. Heiligenhaus A, Tappeiner C, Heinz C, Foeldavri I. Juvenile Idiopathic arthritis. In: Zierhut M, Pavésio C, Shigeaki O, Orefice F, Rao NA, editors. Intraocular Inflammation. Berlin, Heidelberg: Springer-Verlag; 2016:733–735.
13. Terrada C, Prieur AM, Quartier P, Bodaghi B. Les atteintes oculaires au cours des maladies rhumatismales de l’enfant. In: Bahram B, LeHoang P, editors. Uvéite. Issy-les-Moulineaux: Elsevier Masson; 2017:215–217.
14. Herbort CP. Laser flare photometry. In: Gupta A, Gupta V, Herbort CP, Khairallah M, editors. Uveitis, Text and Imaging. New Delhi: Jaypee Brothers Medical Publishers; 2009:28–49.
15. Guex-Crosier Y, Pittet N, Herbort CP. Evaluation of laser flare-cell photometry in the appraisal and management of intraocular inflammation in uveitis. Ophthalmology. 1994;101(4):728–735. doi:10.1016/S0161-6420(13)31050-1
16. Keenan JD, Tessler HH, Goldstein DA. Granulomatous inflammation in juvenile idiopathic arthritis-associated uveitis. J AAPOS. 2008;12:546–550. doi:10.1016/j.jaapos.2008.05.012
17. Kanski JJ. Uveitis in Juvenile Chronic Arthritis: incidence, clinical features and prognosis. Eye. 1988;2(6):641–645. doi:10.1038/eye.1988.118
18. Dana M, Merayo-Lloves J, Schaumberg DA, Foster CS. Visual outcomes prognosticators in juvenile rheumatoid arthritis-associated uveitis. Ophthalmology. 1997;104(2):236–244. doi:10.1016/S0161-6420(97)30329-7
19. Shetty AK, Gedalia A. Childhood sarcoidosis: a rare but fascinating disorder. Pediatr Rheumatol Online J. 2008;6:16. doi:10.1186/1546-0096-6-16
20. Suresh S, Tsui E. Ocular manifestations of Blau syndrome. Curr Opin Ophthalmol. 2020;31(6):532–537. doi:10.1097/ICU.0000000000000705
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.