")
Back to Journals » International Journal of Women's Health » Volume 12
Glycosylated Hemoglobin A1c Is Associated with Anthropometric Measurements and Tumor Characteristics in Breast Cancer Patients
Authors Ayoub NM , Jaradat SK , Alhusban A, Tahaineh L
Received 12 October 2019
Accepted for publication 20 February 2020
Published 6 March 2020 Volume 2020:12 Pages 139—149
DOI https://doi.org/10.2147/IJWH.S234408
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Nehad M Ayoub, Sara K Jaradat, Ahmed Alhusban, Linda Tahaineh
Department of Clinical Pharmacy, Faculty of Pharmacy, Jordan University of Science and Technology (JUST), Irbid, Jordan
Correspondence: Nehad M Ayoub
Department of Clinical Pharmacy, Faculty of Pharmacy, Jordan University of Science and Technology (JUST), P.O. Box 3030, Irbid 22110, Jordan
Tel +962 27201000 Ext 23809
Fax +962 27095123
Email [email protected]
Purpose: To investigate the association between glycosylated hemoglobin A1c (HbA1c) with anthropometric measurements and clinicopathologic characteristics of breast cancer patients. Such data are lacking in Arabian countries.
Patients and Methods: A cross-sectional study was conducted at the Outpatient Oncology Unit at King Hussein Medical Center at the Royal Medical Services (RMS) and 223 breast cancer patients were included. Blood levels of HbA1c were measured and patients were classified into normal/non-diabetic (HbA1c < 5.7%), prediabetic (HbA1c 5.7– 6.4%), and diabetic (HbA1c ≥ 6.5%).
Results: The average age of patients was 49.9± 10.3 years. Most patients had waist circumference equal to or more than 80 cm (91.9%) and more than half (55.2%) had waist-hip ratio equal to or more than 0.85. Mean body mass index (BMI) was 29.9± 5.7 kg/m2. The mean level of HbA1c was 6.2± 1.4% (range 4.7% to 12.6%). HbA1c levels revealed that most patients in this study classified as prediabetics (44.4%). There was a significant positive correlation between HbA1c levels and each of patient’s age (r=0.267, p< 0.001), waist circumference (r=0.180, p=0.008), and waist-hip ratio (r=0.278, p< 0.001). Compared with premenopausal breast cancer patients, postmenopausal patients had significantly higher HbA1c blood levels (t=– 3.542, p=0.003). HbA1c was significantly associated with stage (p=0.044) and grade (p=0.016) of carcinoma in premenopausal breast cancer patients. Among postmenopausal cases, HbA1c was significantly associated with molecular subtype of the disease (p=0.039).
Conclusion: The majority of Jordanian breast cancer patients in this study are prediabetic, obese, and had visceral obesity. HbA1c levels are increased among older patients and those who have greater waist circumference and waist-hip ratio. HbA1c is associated with advanced stage and grade of breast carcinoma in premenopausal patients and with molecular subtype in postmenopausal cases. These findings urge the need to screen breast cancer patients for glycemic status upon disease presentation and to further consider treatments to control hyperglycemia in order to reduce the impact of metabolic derangements on disease prognosis and outcomes.
Keywords: breast cancer, glycosylated hemoglobin, clinicopathologic, prediabetes
Introduction
The exact causes of breast cancer remain largely unknown.1 Greater emphasis is being given to modifiable risk factors to reduce the incidence of the disease. Of interest, anthropometrics and metabolic profile have captured recent attention in breast cancer research. In recent years, growing evidence suggested a complex association between breast cancer and diabetes. Breast cancer and diabetes are commonly occurring comorbidities. It has been reported that up to 16% of postmenopausal breast cancer patients have diabetes.2 Furthermore, diabetes shares many risk factors with breast cancer such as obesity, advanced age, physical inactivity, and smoking.3 Diabetic women have an increased risk for breast cancer compared to the non-diabetic.4,5 According to a meta-analysis, the risk of breast cancer among women with type II diabetes is increased by 27%.6 In addition, overall mortality among diabetic breast cancer patients is higher compared to those without diabetes.7–9 Hyperglycemia is linked to breast cancer mainly by three mechanisms which include activation of the insulin-like growth factor (IGF) signaling pathway, activation of insulin signaling, and altered endogenous sex-hormone regulation.10,11 In line with this, obesity is known to induce insulin resistance leading to hyperglycemia which in turn increases the risk of breast cancer patients to develop aggressive phenotypes of cancer and to present with advanced disease.12
Most studies on the association between glycemic status and breast cancer were conducted in Western countries. Data regarding the association in the Arab countries are still deficient despite the high prevalence of breast cancer in this region of the world. In addition, limited number of studies investigated the relationship between glycemic status and each of anthropometric measurements and clinicopathologic characteristics of breast cancer patients in the Arab world. In this study, the goal was to investigate the association between glycemic status, as determined by glycosylated hemoglobin A1c (HbA1c) levels, and measures of general and central obesity along with clinicopathologic characteristics of breast cancer among Jordanian patients.
Methods
A cross-sectional study was conducted at the Outpatient Oncology Unit at King Hussein Medical Center at the Jordanian Royal Medical Services (RMS), Amman, Jordan. RMS has a wide network of hospitals distributed in different provinces across the Kingdom of Jordan. King Hussein Medical Center is a major medical compound affiliated to RMS with an annual admission rate of 25,000 patients.13 RMS serve multiple directorates in Amman and other areas in Jordan.
The study was approved by Research Ethics Committee of RMS and by the Institutional Review Board (IRB) committee of Jordan University of Science and Technology (JUST) and King Abdullah University Hospital (KAUH) (Research number 13/94/2016). The study was conducted in accordance with the standards and regulations of the declaration of Helsinki. The goals, procedure, and protocol of the study were discussed to all patients before interviewing. All participants provided written informed consent prior to data collection.
Study Population
The study enrolled adult females who were ≥18 years of age with histologically confirmed diagnosis of breast cancer. The diagnosis of breast carcinoma was performed using histopathologic analysis of resected tumor, biopsy or cytology specimens at the Pathology Department of King Hussein Medical Center. Breast cancer patients were interviewed by a trained-graduate student (SKJ) in the Chemotherapy Unit waiting room at the Outpatient Oncology Unit.
Data Collection
The data collection form was developed and modified by researchers based on previously published studies.8,10,14–16 Collected data included demographic and lifestyle information. Regarding menopausal status, patients were determined to be postmenopausal if they indicated to have physiological menopause for at least 12 months.17 Patients were considered diabetic if their laboratory results are suggestive of diabetic state or if they present with a well-established diagnosis of diabetes for at least 48 hrs prior to interview based on a known history of diagnosis and treatment with insulin and/or oral hypoglycemic agents. In addition, the diagnosis of diabetes was confirmed by reviewing medical records of patients.
Anthropometric measurements for body weight (kg), height (cm), waist (cm), and hip (cm) circumferences were obtained for all patients according to recommendations by World Health Organization (WHO).18 The measurements were carried out by a trained graduate student (SKJ) using the same scale and balance for all patients. Visceral obesity was evaluated using measurements of waist circumference and the waist-hip ratio, which was calculated by dividing the waist circumference by the hip circumference.18 Central obesity was indicated if the waist circumference measurement was 80 cm or more. Body mass index (BMI) was calculated using the standard method, in which weight in kilograms is divided by the square of the height in meters.19 Patients were divided into groups based on WHO classification of BMI as follows: underweight (<18.5 kg/m2), normal (18.5–24.99 kg/m2), overweight (25.00–29.99 kg/m2) and obese (≥30.00 kg/m2).19 Only two patients classified as underweight, therefore, the “underweight” and “normal” BMI groups were categorized together as one unit for the purpose of the current analysis.20 Patients were interviewed on daily basis through workdays from 9:00 am to 3:00 pm. Average time for interviewing patients was 10–15 mins.
Tumor characteristics for patients were extracted from relevant pathology reports issued by Pathology Department. Reports included details of tumor grade, stage, ipsilateral axillary lymph node status, lymphovascular invasion (LVI), and detailed histological criteria. Expression status of estrogen receptor (ER) and progesterone receptor (PR) was determined using immunohistochemical methods. Activity greater than 1% was considered positive for each hormone receptor. Expression of human epidermal growth factor receptor 2 (HER2) was evaluated by immunohistochemical analysis in which scores of 0 or +1 were considered negative, while scores of +3 were considered positive for HER2 overexpression. For equivocal results of immunohistochemical analysis (+2), fluorescence in situ hybridization (FISH) analysis positive for gene amplification implied overexpression of HER2. Stage of disease was classified according to the tumor–node–metastasis (TNM) cancer staging system of the American Joint Committee on Cancer (AJCC).21 Grade of carcinoma was determined based on the Nottingham Combined Histologic Grade system.22 Accordingly, tumors were classified into grade I (well-differentiated/low grade), grade II (moderately-differentiated/intermediate grade), and grade III (poorly-differentiated/high grade) carcinomas. Breast cancer was classified into molecular subtypes based on expression of receptors into: luminal A (ER+ and/or PR+, HER2–); luminal B (ER+ and/or PR+, HER2+); HER2-positive (ER–, PR–, HER2+); and triple-negative (ER–, PR–, HER2–).23
Blood Samples and HbA1c Measurements
Venous blood samples were drawn from patients before starting their scheduled treatment. Blood samples were obtained by venipuncture of an antecubital vein of the forearm and were collected in EDTA tubes (Greiner Bio‑One GmbH, Kremsmünster, Austria). Blood levels of HbA1c were measured at JUST Health Center Laboratories. During blood sample analysis, laboratory technicians were blind to patient data as the tubes were given serial numbers to allow retrieval by researchers. Based on the American Diabetes Association (ADA) criteria for HbA1c% blood levels, patients were classified into normal/non-diabetic (HbA1c <5.7%), prediabetic (HbA1c 5.7–6.4%), and diabetic (HbA1c ≥6.5%).24
Statistical Analysis
Data analysis was performed using the IBM SPSS version 21 statistical package (IBM Corp. Version 21.0. Armonk, NY, USA). Continuous variables presented as mean ± standard deviation while categorical variables presented as frequency and percentage (n, %). To compare categorical variables between groups, Pearson’s chi-square test of independence was used. Independent samples t-test was applied to compare two independent groups. One-way Analysis of Variance (ANOVA) test was used for multiple comparisons between independent groups when indicated. To assess correlations between continuous variables, Pearson’s correlation test was applied. All p values were two-sided at α value of 0.05. Differences were statistically significant at p-value of less than 0.05.
Dichotomization of some categorical variables was considered for correlation analysis of some study variables. This dichotomization was based on sample size and was performed in advance of conducting statistical analysis in order to avoid small sample size upon further stratification of data.23 Therefore, the TNM stage of breast cancer was dichotomized as early stages (I/II) and advanced stages (III/IV). Histologic grade was categorized into grades (I/II) and grade III tumors. Tumor size was classified into two groups, less than 2 cm (T1) and greater than 2 cm (T2 and T3). Categories of these tumor variables were selected based on cut points previously published by other researchers.25
Results
The study was conducted over an 8-month period from July 2016 to February 2017. Of 248 interviewed patients, 223 patients agreed to participate in the study, yielding a response rate of 88.8%.
Demographic and Anthropometric Characteristics of Breast Cancer Patients
Demographic characteristics of breast cancer patients are shown in Table 1. The average age of patients was 49.9±10.3 years (range 27 to 80). Among participants, 72 (32.3%) were premenopausal and 151 (67.7%) were postmenopausal. Most patients have no family history of breast cancer among first-degree relatives (n=166, 74.4%), never smoked (80.7%), or consumed alcoholic beverages (99.1%) (Table 1). Mean waist circumference of patients was 98.8±12.4 cm (range 70.0–132.0). Average waist-hip ratio was 0.86±0.75 (range 0.65–1.10). Majority of patients had waist circumference equal to or more than 80 cm (91.9%). In addition, more than half of patients (55.2%) had waist-hip ratio equal to or more than 0.85. Average BMI for patients was 29.9±5.7 kg/m2 and ranging from 17.7 to 51.1. One hundred and eight patients (48.4%) were obese at time of interview (Table 1).
 |
Table 1 Demographic and Anthropometric Characteristics of Breast Cancer Patients (N=223) |
Glycemic Status and HbA1c% Levels of Breast Cancer Patients
Forty-eight patients (21.5%) are known cases of diabetes mellitus. Almost all diabetics have type II disease and were diagnosed after the age of 40 years (Table 2). Most diabetics received treatment regimens composed of oral hypoglycemic agents (74.5%). The mean level of HbA1c% for patients was 6.2±1.4 (range 4.7% to 12.6%). HbA1c% levels revealed that most patients classified as prediabetics (44.4%) (Table 2). Among non-diabetic cases (n=175), more than half (n=92, 52.6%) were prediabetic and nine patients had HbA1c% levels suggestive of diabetes (n=9, 5.1%).
 |
Table 2 Description of Glycemic Status and HbA1c% Levels Among Breast Cancer Patients (N=223) |
Clinicopathologic Characteristics of Breast Cancer Patients
Pathology reports were retrieved for 189 patients. Most patients had breast cancer for less than one-year duration (61.4%) and were diagnosed with left-sided disease (51.9%) (Table 3). Most patients had stage II (38.1%) or stage III (30.7%) disease at diagnosis. Almost half of patients (49.7%) presented with high tumor grade (III). Invasive ductal carcinoma (IDC) was the main histopathologic type identified (79.9%). Most patients had positive expression for both hormone receptors and luminal A was the most reported molecular subtype (40.2%). Many patients underwent surgical tumor resection (79.9%). Other tumor characteristics of patients are shown in Table 3.
 |
Table 3 Clinicopathologic Characteristics of Breast Cancer Patients (N=189) |
Correlation Between HbA1c Levels and Anthropometric Measurements of Breast Cancer Patients
Bivariate correlation analysis of continuous variables showed a significant positive correlation between HbA1c levels and patients' age (r=0.267, p<0.001, Table 4). HbA1c levels were positively and significantly correlated with waist circumference and waist-hip ratio (r=0.180, p=0.008 and r=0.278, p<0.001, respectively). However, HbA1c levels were not significantly correlated with BMI, tumor size, and number of lymph nodes among breast cancer patients (Table 4).
 |
Table 4 Correlation Analysis of HbA1c Levels with Selected Anthropometric and Clinicopathologic Characteristics of Breast Cancer Patients (N=223) (Continuous Variables) |
In agreement, mean HbA1c levels were significantly higher among elderly patients compared to other age groups (F=5.225; p=0.006) (Figure 1A). Similarly, breast cancer patients with greater waist circumference and waist-hip ratio had significantly higher HbA1c levels (Figure 1B and C). Though obese and overweight patients had higher mean levels of HbA1c, these differences did not reach the level of statistical significance (p=0.204) (Figure 1D). Mean HbA1c blood levels were significantly higher among postmenopausal compared to premenopausal patients (t=–3.542, p=0.003) (Figure 1E).
 |
Figure 1 HbA1c levels in relation to anthropometric measurements and menopausal status of breast cancer patients. Average blood levels of HbA1c were compared according to (A) age, (B) waist circumference, (C) waist-hip ratio, (D) BMI, and (E) menopausal status of breast cancer patients. *Statistically significant at p<0.05. Abbreviations: BMI, body mass index; HbA1c, glycosylated hemoglobin A1c. |
Association of HbA1c with Clinicopathologic Characteristics in Breast Cancer Patients Based on Menopausal Status
Associations between HbA1c with clinicopathologic characteristics of breast cancer patients was stratified according to menopausal status as indicated in Table 5. HbA1c was significantly associated with stage (p=0.044) and grade (p=0.016) of carcinoma in premenopausal cases. Among prediabetic breast cancer patients, a greater proportion of cases presented with advanced stage and higher grade of the disease compared to patients with normal HbA1c status (Table 5). Among postmenopausal patients, HbA1c was significantly associated with molecular subtype of breast cancer (p=0.039). However, HbA1c lacked significant associations with tumor stage and grade in postmenopausal cases. Other associations between HbA1c and tumor characteristics based on menopausal status are shown in Table 5.
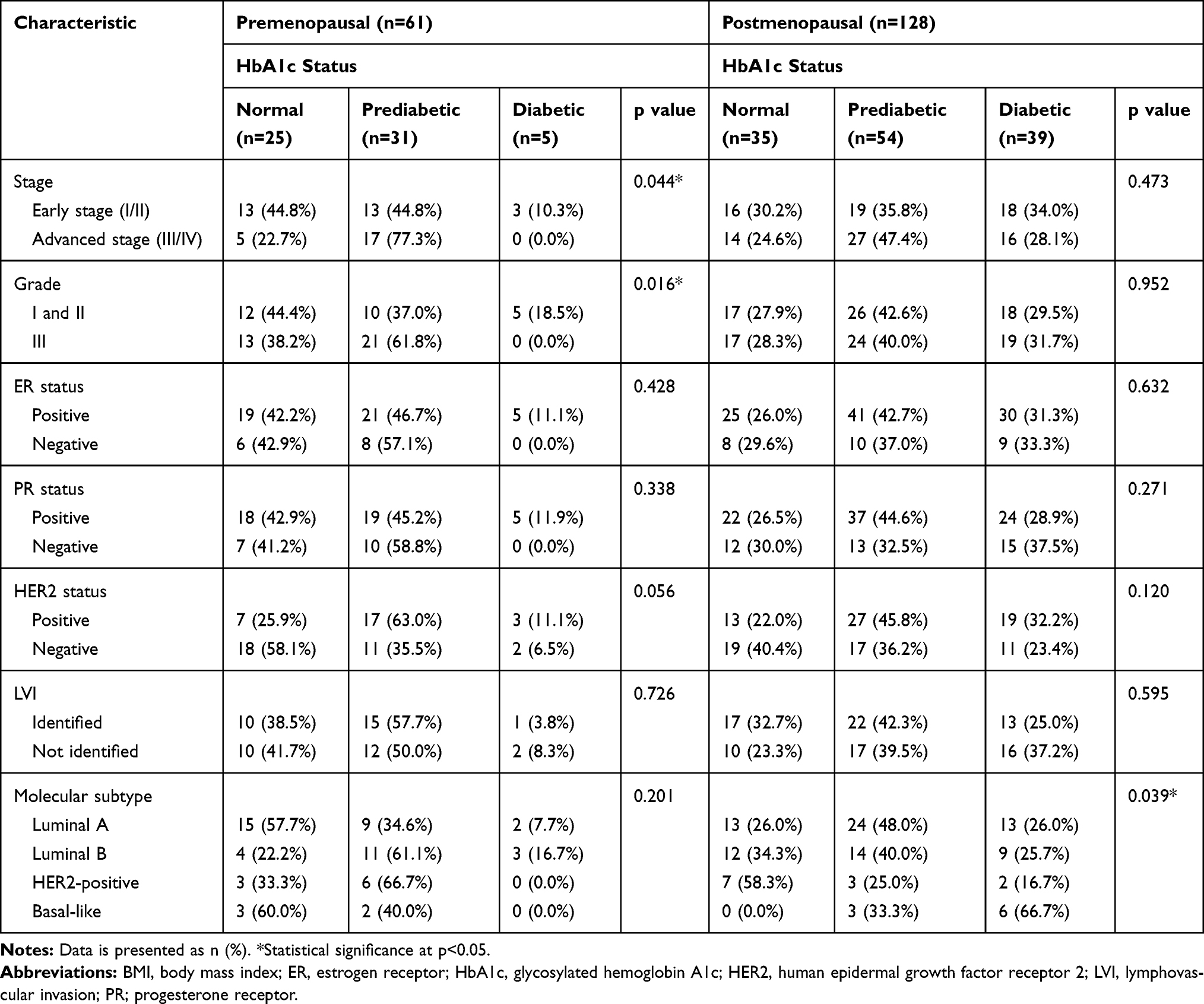 |
Table 5 Association Between HbA1c with Clinicopathologic Characteristics in Breast Cancer Patients Based on Menopausal Status (N=189) |
Discussion
American Diabetes Association (ADA) had adopted the use of Glycosylated Hemoglobin A1c (HbA1c) measurements as a diagnostic test for diabetes.24 HbA1c is a marker for chronic glycemic exposure which identifies average levels of blood glucose over a duration of 2 to 3 months.24,26 Measurements of HbA1c levels retain multiple advantages compared to fasting plasma glucose determination.27 These advantages include the feasibility and convenience of the analysis since fasting is not required along with reduced sensitivity to acute changes in dietary habits or lifestyle factors.24,26 In addition, HbA1c levels are not affected by diurnal variations in blood glucose levels and are less sensitive to acute glycemic fluctuations which may result from certain drug treatments that cancer patients could be receiving and known to adversely affect fasting glucose levels.27 Findings from our study revealed that most breast cancer patients in this series were prediabetic with no previous diagnosis of diabetes. This is of particular interest as earlier studies showed that many diabetes cases may remain undiagnosed until a diagnosis of breast cancer is made.28 In agreement to this finding, Erickson et al indicated that among breast cancer patients who were screened for HbA1c and had levels of ≥7.0%, less than half reported diabetes.8 These findings are alarming taking into consideration the negative impact of hyperglycemia on presentation and prognosis of breast cancer patients. Prediabetes is associated with high risk of developing diabetes.29 Earlier evidence indicated that microvascular and macrovascular changes commonly associated with diabetes actually begin during prediabetic stage.29 Prediabetes is associated with increased risk of various types of tumors including breast, gastric, colorectal, pancreatic, liver, and endometrial cancers.30,31 In addition, breast cancer patients who were prediabetic are more vulnerable for early detection of breast cancer as the risk of the disease is increased during prediabetes phase.16,32
In Jordan, breast cancer is the most commonly diagnosed carcinoma among women.33,34 In addition, the prevalence of diabetes is high and increasing in the Jordanian community.35 This is due, in part, to a rise in the number of individuals with metabolic syndrome and obesity; since these conditions are related.36 It is estimated that 38.8% of Jordanian women aged between 15 and 49 years are obese.34 In our study, 80.7% of breast cancer patients were overweight or obese based on BMI. In addition, majority of patients in this study had waist circumference and waist-hip ratio measurements supportive of visceral/central obesity.18 Visceral obesity is a substantial risk factor for insulin resistance, diabetes, and metabolic syndrome. Recent evidence also indicated that visceral obesity is associated with increased risk of multiple types of solid tumors and reduced overall treatment outcomes in cancer patients.37,38 Our findings revealed that HbA1c levels were positively correlated with age and measures of central obesity among breast cancer patients, but not BMI. HbA1c levels are increased among older patients and those who have greater waist circumference and waist-hip ratio. These findings are consistent with multiple other studies.8,39,40 Among patients with solid cancers, prediabetic patients were found to be older in age and had a higher BMI compared to non-diabetic patients.41 It is well-known that obesity affects survival and mortality of breast cancer patients.42,43 Obesity is associated with advanced clinicopathologic presentation of breast cancer and higher rates of disease recurrence and reduced overall survival.39,44,45 The impact of obesity on risk for breast cancer has been shown to be affected by menopausal status in which obese postmenopausal women showed consistent increase of breast cancer risk compared to premenopausal patients.46,47 The relationship between premenopausal obesity and breast cancer risk remains inconclusive. While some studies report that premenopausal obesity could be protective and is inversely related to breast cancer risk,48–50 others report no association between obesity and breast cancer among premenopausal women.51 Nevertheless, obesity has been associated with poor prognosis in both premenopausal and postmenopausal breast cancer patients.52 Our data indicated a significant association between HbA1c and menopausal status. Postmenopausal women presented with higher mean levels of HbA1c compared to premenopausal patients. This could be explained by the fact that postmenopausal women are older in age and tend to be more obese than younger premenopausal patients.53
The impact of HbA1c on breast cancer presentation and clinicopathologic characteristics is inconsistent. In this study, HbA1c status lacked significant associations with tumor clinicopathologic characteristics among the entire cohort of breast cancer patients (data not shown). However, when patients were stratified based on menopausal status, HbA1c levels were significantly associated with tumor stage and grade in premenopausal patients and associated with molecular subtype among postmenopausal cases. Several studies demonstrated a lack of association between HbA1c levels and presentation of breast cancer patients.39,54,55 Bronsveld et al revealed a lack of association between HbA1c levels and tumor clinicopathologic characteristics including molecular subtypes among diabetic postmenopausal breast cancer patients compared to the non-diabetic.54 Similarly, Karlin et al reported no significant differences in breast cancer grade, stage, and receptor positivity between diabetic and non-diabetic patients.55 Alternatively, multiple studies in literature showed correlations between glycemic status and breast cancer characteristics.8,14,56–58 In agreement to our findings, Erickson et al indicated that patients with HbA1c ≥6.5% are more likely to be obese and present with more advanced breast cancer at diagnosis.8 Liao et al found significant differences in tumor stage and lymph node metastasis after adjustment for age between diabetic and non-diabetic breast cancer patients.58 In addition, data from meta-analysis reported that diabetic patients presenting with breast cancer had advanced stage, larger tumor size, and negative status of hormone receptors.56
The main limitation to this study was the inability to retrieve all pathology reports of enrolled patients which resulted in missed clinicopathologic data for some patients. This could have hindered potential significant correlations and/or associations to be revealed. The main strengths of our study included its homogenous patient population and its diagnostic data that were generated by practitioners and protocols applied in a single medical institution. In addition, anthropometric data were measured by a single-trained person and were not self-reported by patients.
Conclusions
To the best of our knowledge, this is the first study to describe the association between HbA1c levels with anthropometric measurements and clinicopathologic characteristics among Jordanian breast cancer patients. Findings from this study showed that a considerable proportion of breast cancer patients in this series were prediabetic. Glycemic status was clearly associated with measures of visceral obesity in breast cancer patients. Postmenopausal patients have higher levels of HbA1c compared to premenopausal cases. HbA1c was significantly associated with clinicopathologic characteristics of breast cancer in premenopausal and postmenopausal cases. Collectively, findings from this study call for appropriate assessment for glycemic status in breast cancer patients up on disease presentation, particularly emphasizing the need to control hyperglycemia and identify vulnerable groups of cancer patients who might benefit from interventions to improve glycemic control.
Data Sharing Statement
Data supporting the findings of this study are available upon reasonable request from the corresponding author. The data are not available to public in order not to compromise the privacy of research participants.
Acknowledgments
The authors would like to extend their sincere appreciation and gratitude to all who contributed to this study. Many thanks to the medical and nursing staff at King Hussein Medical Center for their cooperativeness and valuable assistance. Importantly, thanks should go to breast cancer patients who agreed to participate in this study.
Funding
This work was supported by a grant from the Deanship of Research at Jordan University of Science and Technology (JUST) [grant number 20160123].
Disclosure
The authors report no conflicts of interest in this work.
References
1. Taira N, Akiyama I, Ishihara S, et al. Impact of modifiable lifestyle factors on outcomes after breast cancer diagnosis: the Setouchi Breast Cancer Cohort Study. Jpn J Clin Oncol. 2015;45(6):600–602. doi:10.1093/jjco/hyv033
2. Yancik R, Wesley MN, Ries LA, Havlik RJ, Edwards BK, Yates JW. Effect of age and comorbidity in postmenopausal breast cancer patients aged 55 years and older. JAMA. 2001;285(7):885–892. doi:10.1001/jama.285.7.885
3. Giovannucci E, Harlan DM, Archer MC, et al. Diabetes and cancer: a consensus report. Diabetes Care. 2010;33(7):1674–1685. doi:10.2337/dc10-0666
4. Liao S, Li J, Wei W, et al. Association between diabetes mellitus and breast cancer risk: a meta-analysis of the literature. Asian Pac J Cancer Prev. 2011;12(4):1061–1065.
5. Starup-Linde J, Karlstad O, Eriksen SA, et al. CARING (CAncer Risk and INsulin analoGues): the association of diabetes mellitus and cancer risk with focus on possible determinants - a systematic review and a meta-analysis. Curr Drug Saf. 2013;8(5):296–332. doi:10.2174/15748863113086660071
6. Boyle P, Boniol M, Koechlin A, et al. Diabetes and breast cancer risk: a meta-analysis. Br J Cancer. 2012;107(9):1608–1617. doi:10.1038/bjc.2012.414
7. Cleveland RJ, North KE, Stevens J, Teitelbaum SL, Neugut AI, Gammon MD. The association of diabetes with breast cancer incidence and mortality in the Long Island Breast Cancer Study Project. Cancer Causes Control. 2012;23(7):1193–1203. doi:10.1007/s10552-012-9989-7
8. Erickson K, Patterson RE, Flatt SW, et al. Clinically defined type 2 diabetes mellitus and prognosis in early-stage breast cancer. J Clin Oncol. 2011;29(1):54–60. doi:10.1200/JCO.2010.29.3183
9. Luo J, Virnig B, Hendryx M, et al. Diabetes, diabetes treatment and breast cancer prognosis. Breast Cancer Res Treat. 2014;148(1):153–162. doi:10.1007/s10549-014-3146-9
10. Wolf I, Sadetzki S, Catane R, Karasik A, Kaufman B. Diabetes mellitus and breast cancer. Lancet Oncol. 2005;6(2):103–111. doi:10.1016/S1470-2045(05)01736-5
11. Belfiore A, Frasca F. IGF and insulin receptor signaling in breast cancer. J Mammary Gland Biol Neoplasia. 2008;13(4):381–406.
12. Gallagher EJ, LeRoith D. Obesity and diabetes: the increased risk of cancer and cancer-related mortality. Physiol Rev. 2015;95(3):727–748. doi:10.1152/physrev.00030.2014
13. Royal Medical Services (RMS). Available from: http://www.jrms.mil.jo/Contents/About_JRMSar.aspx#.
14. Hou G, Zhang S, Zhang X, Wang P, Hao X, Zhang J. Clinical pathological characteristics and prognostic analysis of 1013 breast cancer patients with diabetes. Breast Cancer Res Treat. 2013;137(3):807–816. doi:10.1007/s10549-012-2404-y
15. Wang XL, Jia CX, Liu LY, Zhang Q, Li YY, Li L. Obesity, diabetes mellitus, and the risk of female breast cancer in Eastern China. World J Surg Oncol. 2013;11:71. doi:10.1186/1477-7819-11-71
16. Salinas-Martinez AM, Flores-Cortes LI, Cardona-Chavarria JM, et al. Prediabetes, diabetes, and risk of breast cancer: a case-control study. Arch Med Res. 2014;45(5):432–438. doi:10.1016/j.arcmed.2014.06.004
17. Sherman S. Defining the menopausal transition. Am J Med. 2005;118(Suppl 12B):3–7. doi:10.1016/j.amjmed.2005.11.002
18. World Health Organization (WHO). Waist Circumference and Waist-Hip Ratio: Report of a WHO Expert Consultation. Geneva. 8–11 December 2008; 2011.
19. World Health Organization (WHO). Obesity: Preventing and Managing the Global Epidemic, WHO Technical Report Series 894, Geneva, Switzerland; 2000.
20. Stark A, Stahl MS, Kirchner HL, Krum S, Prichard J, Evans J. Body mass index at the time of diagnosis and the risk of advanced stages and poorly differentiated cancers of the breast: findings from a case-series study. Int J Obes. 2010;34(9):1381–1386. doi:10.1038/ijo.2010.69
21. Edge S,Byrd DR, Compton CC, Fritz AG, Greene FL, Trotti A. AJCC Cancer Staging Handbook from the AJCC Cancer Staging Manual.
22. Rakha EA, Reis-Filho JS, Baehner F, et al. Breast cancer prognostic classification in the molecular era: the role of histological grade. Breast Cancer Res. 2010;12(4):207. doi:10.1186/bcr2607
23. Stark A, Schultz D, Kapke A, et al. Obesity and risk of the less commonly diagnosed subtypes of breast cancer. Eur J Surg Oncol. 2009;35(9):928–935. doi:10.1016/j.ejso.2008.11.009
24. American Diabetes Association. Diabetes overview, diagnosis. 2019. Available from: https://www.diabetes.org/a1c/diagnosis.
25. Abdel-Maksoud MF, Risendal BC, Slattery ML, Giuliano AR, Baumgartner KB, Byers TE. Behavioral risk factors and their relationship to tumor characteristics in Hispanic and non-Hispanic white long-term breast cancer survivors. Breast Cancer Res Treat. 2012;131(1):169–176. doi:10.1007/s10549-011-1705-x
26. International Expert Committee. International expert committee report on the role of the A1C assay in the diagnosis of diabetes. Diabetes Care. 2009;32(7):1327–1334. doi:10.2337/dc09-9033
27. Bonora E, Tuomilehto J. The pros and cons of diagnosing diabetes with A1C. Diabetes Care. 2011;34(Suppl 2):S184–S190. doi:10.2337/dc11-s216
28. Danese MD, O’Malley C, Lindquist K, Gleeson M, Griffiths RI. An observational study of the prevalence and incidence of comorbid conditions in older women with breast cancer. Ann Oncol. 2012;23(7):1756–1765. doi:10.1093/annonc/mdr486
29. Tabak AG, Herder C, Rathmann W, Brunner EJ, Kivimaki M. Prediabetes: a high-risk state for diabetes development. Lancet. 2012;379(9833):2279–2290. doi:10.1016/S0140-6736(12)60283-9
30. Lambe M, Wigertz A, Garmo H, Walldius G, Jungner I, Hammar N. Impaired glucose metabolism and diabetes and the risk of breast, endometrial, and ovarian cancer. Cancer Causes Control. 2011;22(8):1163–1171. doi:10.1007/s10552-011-9794-8
31. Huang Y, Cai X, Qiu M, et al. Prediabetes and the risk of cancer: a meta-analysis. Diabetologia. 2014;57(11):2261–2269. doi:10.1007/s00125-014-3361-2
32. Onitilo AA, Stankowski RV, Berg RL, et al. Breast cancer incidence before and after diagnosis of type 2 diabetes mellitus in women: increased risk in the prediabetes phase. Eur J Cancer Prev. 2014;23(2):76–83. doi:10.1097/CEJ.0b013e32836162aa
33. Jordan Cancer Registry. Cancer incidence in Jordan. Available from: https://www.moh.gov.jo/Echobusv3.0/SystemAssets/245e1e7a-a9ab-4fab-b876-832c2af5f340.pdf.
34. Al Nsour M, Al Kayyali G, Naffa S. Overweight and obesity among Jordanian women and their social determinants. East Mediterr Health J. 2013;19(12):1014–1019.
35. Ajlouni K, Khader YS, Batieha A, Ajlouni H, El-Khateeb M. An increase in prevalence of diabetes mellitus in Jordan over 10 years. J Diabetes Complications. 2008;22(5):317–324. doi:10.1016/j.jdiacomp.2007.01.004
36. Genser L, Casella Mariolo JR, Castagneto-Gissey L, Panagiotopoulos S, Rubino F. Obesity, type 2 diabetes, and the metabolic syndrome: pathophysiologic relationships and guidelines for surgical intervention. Surg Clin North Am. 2016;96(4):681–701. doi:10.1016/j.suc.2016.03.013
37. Park SW, Lee HL, Doo EY, et al. Visceral obesity predicts fewer lymph node metastases and better overall survival in colon cancer. J Gastrointest Surg. 2015;19(8):1513–1521. doi:10.1007/s11605-015-2834-z
38. Wierup I, Carlsson AC, Wandell P, Riserus U, Arnlov J, Borne Y. Low anthropometric measures and mortality–results from the Malmo Diet and Cancer Study. Ann Med. 2015;47(4):325–331. doi:10.3109/07853890.2015.1042029
39. Jousheghany F, Phelps J, Crook T, Hakkak R. Relationship between level of HbA1C and breast cancer. BBA Clin. 2016;6:45–48. doi:10.1016/j.bbacli.2016.04.005
40. Sheth J, Shah A, Sheth F, et al. The association of dyslipidemia and obesity with glycated hemoglobin. Clin Diabetes Endocrinol. 2015;1:6. doi:10.1186/s40842-015-0004-6
41. Hammer MJ, Aouizerat BE, Schmidt BL, Cartwright F, Wright F, Miaskowski C. Glycosylated hemoglobin A1c and lack of association with symptom severity in patients undergoing chemotherapy for solid tumors. Oncol Nurs Forum. 2015;42(6):581–590. doi:10.1188/15.ONF.581-590
42. Abrahamson PE, Gammon MD, Lund MJ, et al. General and abdominal obesity and survival among young women with breast cancer. Cancer Epidemiol Biomarkers Prev. 2006;15(10):1871–1877. doi:10.1158/1055-9965.EPI-06-0356
43. Healy LA, Ryan AM, Carroll P, et al. Metabolic syndrome, central obesity and insulin resistance are associated with adverse pathological features in postmenopausal breast cancer. Clin Oncol. 2010;22(4):281–288. doi:10.1016/j.clon.2010.02.001
44. Chan DS, Vieira AR, Aune D, et al. Body mass index and survival in women with breast cancer-systematic literature review and meta-analysis of 82 follow-up studies. Ann Oncol. 2014;25(10):1901–1914. doi:10.1093/annonc/mdu042
45. Ayoub NM, Yaghan RJ, Abdo NM, Matalka II, Akhu-Zaheya LM, Al-Mohtaseb AH. Impact of obesity on clinicopathologic characteristics and disease prognosis in pre- and postmenopausal breast cancer patients: a Retrospective Institutional Study. J Obes. 2019;2019:3820759. doi:10.1155/2019/3820759
46. van den Brandt PA, Spiegelman D, Yaun SS, et al. Pooled analysis of prospective cohort studies on height, weight, and breast cancer risk. Am J Epidemiol. 2000;152(6):514–527. doi:10.1093/aje/152.6.514
47. Reeves GK, Pirie K, Beral V, et al. Cancer incidence and mortality in relation to body mass index in the Million Women Study: cohort study. BMJ. 2007;335(7630):1134. doi:10.1136/bmj.39367.495995.AE
48. Carmichael AR, Bates T. Obesity and breast cancer: a review of the literature. Breast. 2004;13(2):85–92. doi:10.1016/j.breast.2003.03.001
49. Bhaskaran K, Douglas I, Forbes H, dos-Santos-Silva I, Leon DA, Smeeth L. Body-mass index and risk of 22 specific cancers: a population-based cohort study of 5.24 million UK adults. Lancet. 2014;384(9945):755–765. doi:10.1016/S0140-6736(14)60892-8
50. Palmer JR, Adams-campbell LL, Boggs DA, Wise LA, Rosenberg L. A prospective study of body size and breast cancer in black women. Cancer Epidemiol Biomarkers Prev. 2007;16(9):1795–1802. doi:10.1158/1055-9965.EPI-07-0336
51. Gravena AAF, Romeiro Lopes TC, Demitto MO, et al. The obesity and the risk of breast cancer among pre and postmenopausal women. Asian Pac J Cancer Prev. 2018;19(9):2429–2436. doi:10.22034/APJCP.2018.19.9.2429
52. Vona-Davis L, Rose DP, Hazard H, et al. Triple-negative breast cancer and obesity in a rural Appalachian population. Cancer Epidemiol Biomarkers Prev. 2008;17(12):3319–3324. doi:10.1158/1055-9965.EPI-08-0544
53. Haslam DW, James WP. Obesity. Lancet. 2005;366(9492):1197–1209. doi:10.1016/S0140-6736(05)67483-1
54. Bronsveld HK, Jensen V, Vahl P, et al. Diabetes and breast cancer subtypes. PLoS One. 2017;12(1):e0170084. doi:10.1371/journal.pone.0170084
55. Karlin N, Dueck A, Nagi Reddy S, Verona P, Cook C. Implications of breast cancer with diabetes mellitus on patient outcomes and care. Diabetes Manage. 2014;4(5):411–419. doi:10.2217/dmt.14.39
56. Peairs KS, Barone BB, Snyder CF, et al. Diabetes mellitus and breast cancer outcomes: a systematic review and meta-analysis. J Clin Oncol. 2011;29(1):40–46. doi:10.1200/JCO.2009.27.3011
57. Griffiths RI, Danese MD, Gleeson ML, Valderas JM. Epidemiology and outcomes of previously undiagnosed diabetes in older women with breast cancer: an observational cohort study based on SEER-medicare. BMC Cancer. 2012;12:613. doi:10.1186/1471-2407-12-613
58. Liao S, Li J, Wang L, et al. Type 2 diabetes mellitus and characteristics of breast cancer in China. Asian Pac J Cancer Prev. 2010;11(4):933–937.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.