")
Back to Journals » Clinical Interventions in Aging » Volume 15
Geriatric Interdisciplinary Home Rehabilitation After Hip Fracture in People with Dementia – A Subgroup Analysis of a Randomized Controlled Trial
Authors Karlsson Å , Berggren M, Olofsson B , Stenvall M , Gustafson Y, Nordström P, Lindelöf N
Received 21 February 2020
Accepted for publication 8 July 2020
Published 4 September 2020 Volume 2020:15 Pages 1575—1586
DOI https://doi.org/10.2147/CIA.S250809
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Richard Walker
Åsa Karlsson,1 Monica Berggren,2 Birgitta Olofsson,3 Michael Stenvall,2 Yngve Gustafson,2 Peter Nordström,2 Nina Lindelöf1
1Department of Community Medicine and Rehabilitation, Geriatric Medicine and Physiotherapy, Umeå University, Umeå, Sweden; 2Department of Community Medicine and Rehabilitation, Geriatric Medicine, Umeå University, Umeå, Sweden; 3Department of Nursing and Department of Surgical and Perioperative Science, Orthopedics, Umeå University, Umeå, Sweden
Correspondence: Åsa Karlsson
Department of Community Medicine and Rehabilitation, Geriatric Medicine, Umeå University, Umeå SE- 901 87, Sweden
Tel +46 90 785 87 66
Email [email protected]
Purpose: To investigate if the effects of geriatric interdisciplinary home rehabilitation after hip fracture were different among people with dementia compared to those without dementia and to describe the overall outcome after hip fracture in people with dementia.
Patients and Methods: A post hoc subgroup analysis of a randomized controlled trial was conducted including 205 people with hip fracture, aged ≥ 70, living in ordinary housing or residential care facilities. Early discharge followed by individually designed interdisciplinary home rehabilitation for a maximum of 10 weeks was compared to in-hospital geriatric care according to a multifactorial rehabilitation program. Outcomes were hospital length of stay (LOS), readmissions, falls, mortality, performance in activities of daily living (ADL), and walking ability.
Results: Interdisciplinary home rehabilitation vs in-hospital care had comparable effects on falls and mortality between discharge and 12 months and on ADL and walking ability at 3 and 12 months regardless of whether the participants had dementia or not (P≥ 0.05 for all). Among participants with dementia, postoperative LOS was a median of 18 days (interquartile range [IQR] 14– 30) in the home rehabilitation group vs 23 days (IQR 15– 30) in the control group (P=0.254) with comparable numbers of readmissions after discharge. Dementia was associated with increased risk of falling (odds ratio [OR] 3.86; 95% confidence interval [CI]: 2.05– 7.27; P< 0.001) and increased mortality (OR 4.20; 95% CI 1.79– 9.92, P=0.001) between discharge and 12 months and with greater dependence in ADL and walking at 3 and 12 months compared to participants without dementia (P< 0.001 for all).
Conclusion: The effects of geriatric interdisciplinary home rehabilitation vs in-hospital geriatric care did not differ in participants with and without dementia. However, the statistical power of this subgroup analysis was likely insufficient to detect differences between the groups. Dementia was associated with a substantial negative impact on the outcomes following the hip fracture. Our findings support offering interdisciplinary home rehabilitation after hip fracture to people with dementia.
Keywords: accidental falls, activities of daily living, cognitive impairment, length of stay, walking ability
Introduction
The number of people with dementia is growing worldwide, and according to the World Health Organization there is one new case of dementia every three seconds.1 An individual with Alzheimer´s disease is about three times more likely to sustain a hip fracture than an age- and sex-matched control who is cognitively intact,2 and the outcomes are worse when compared with people without dementia. Mortality is higher,2–5 postoperative complications are more common,3,6 and the negative impact on mobility and performance in activities of daily living (ADL) is greater in people with dementia than in people who are cognitively intact.5–7 In addition, dementia is an independent risk factor for postoperative admission to long-term residential care.3
Despite dementia being common among older people with hip fracture and that the population has complex care needs,6 the condition has often been an exclusion criterion for participation in previous clinical trials.8 There is, however, growing evidence that people with hip fracture and cognitive impairment (CI) or dementia benefit from enhanced interdisciplinary rehabilitation in hospital,9,10 combined in-hospital and in-home rehabilitation,11–14 and from rehabilitation in nursing homes,15 although the optimal rehabilitation strategies remain unclear.6
To our knowledge, no previous team-based home rehabilitation (HR) interventions after hip fracture have included people with severe CI or dementia. We have, however, in a randomized controlled trial (RCT) evaluated a Geriatric Interdisciplinary Home Rehabilitation (GIHR) intervention for older people with hip fracture, including those with dementia and those living in residential care facilities, compared with in-hospital geriatric care according to a multifactorial rehabilitation program. The results showed that functional recovery in ADL and walking ability, as well as complications and readmissions after discharge, were comparable between the GIHR and control groups,16–18 although the GIHR group had a significantly shorter initial postoperative length of stay (LOS) in hospital. Half of the participants in the RCT had dementia at baseline. Given this high proportion, the lack of HR studies including people with dementia, and the positive effects for people with dementia in a previous in-hospital RCT at our clinic with a multifactorial rehabilitation program,10 we considered it important to perform a subgroup analysis of the outcome in people with dementia.
The aim of the present study was to investigate if the effects of geriatric interdisciplinary home rehabilitation after hip fracture were different among people with dementia compared to those without dementia. A secondary aim was to describe the overall outcome after hip fracture in people with dementia.
Methods
Design and Participants
This post hoc subgroup analysis was part of a parallel-group RCT conducted between May 2008 and June 2011 at the Geriatric Department of the University Hospital of Umeå in Sweden. The method of the RCT has been described in detail previously,16–18 and the study is registered at Current Controlled Trials Ltd. (ISRCTN 15738119). People after hip fracture surgery (cervical or trochanteric fracture), aged 70 or older, and living in the municipality of Umeå in ordinary housing or in residential care facilities were eligible. People with pathological fractures and those who fractured their hips in the hospital were excluded.
Procedure
The participants were consecutively randomized using sequentially numbered lots in opaque, sealed envelopes drawn by a ward nurse who was not involved in the study. The randomization was stratified according to type of housing (ordinary or residential care facility) and to type of fracture (cervical or trochanteric). Participants were randomized to receive in-hospital care and rehabilitation in a geriatric ward plus GIHR after discharge, or to in-hospital geriatric care and rehabilitation. Study information was given both orally and in writing, and when CI was present the next of kin could provide written informed consent. The participants were assessed during their hospital stay, within 5 days after randomization, and at 3 and 12 months postoperatively in their homes by trained assessors, one physiotherapist, and one registered nurse who were blinded to group allocation.
Control Group
In-hospital care and rehabilitation in the geriatric ward were based on a multifactorial rehabilitation program, which was evaluated in an RCT19–21 and was implemented at the ward in 2000. In short, the program consists of interdisciplinary rehabilitation using comprehensive geriatric assessment followed by individual rehabilitation plans, participation of the whole staff in the patient’s everyday activities, and a thorough discharge plan. The in-hospital program had a special focus on detection, prevention, and treatment of postoperative complications and on specific retraining provided by the physiotherapist and the occupational therapist. Participants who needed additional rehabilitation after discharge were referred to primary health care, and at 3 months after the fracture they could also receive rehabilitation at a geriatric outpatient rehabilitation unit. For participants living in residential care, physiotherapists and occupational therapists in the facilities were contacted regarding the need for continued rehabilitation after discharge.
Intervention
Participants allocated to the GIHR intervention, as described in detail earlier,16–18 were also initially treated according to the in-hospital multifactorial rehabilitation program, but with the aim of early discharge and continuation of rehabilitation in their homes with the support of the GIHR team for a maximum of 10 weeks. Discharge was possible when the participants had no medical obstacles, could manage basic transfers, and had the care they required at home. The team was comprised of a nurse, an occupational therapist, and two physiotherapists who visited the participants regularly and a geriatrician who was medically responsible. A social worker and a dietician were available on consultation. The rehabilitation was individually tailored, ie, team actions, length of the rehabilitation period, and number of home visits varied for each participant according to their individual rehabilitation plan. The intervention included multifactorial fall prevention, modifications of the home environment, and specific training in ADL and in the use of assistive devices. In addition, walking exercises and progressive functional strength and balance training according to the High-Intensity Functional Exercise (HIFE) Program were included.22,23 The medical part of the intervention focused on prevention, detection, and treatment of complications after discharge, evaluation of pain, and assessment of the participants’ ability to handle their medicines safely. The participants’ nutrition was also evaluated, and all team members worked together to improve the participants’ nutritional status with the support of the dietician when necessary. The GIHR team worked closely with the next of kin and with the care providers in home social services or in the residential care facilities.
Outcome Measures
Data on initial postoperative LOS and readmissions, falls (numbers of participants who fell at least once and the total numbers of falls), and mortality between discharge and 12 months were registered when the study was completed using medical data from the participants´ digital charts along with the assessments at the 3- and 12-month follow-ups. An experienced geriatrician not blinded to group allocation collected the data according to a pre-set protocol. Medical data and assessments were analyzed by a geriatrician, who was blinded to group allocation, to determine if the participants fulfilled the criteria for dementia, delirium, and depressive disorders (DSM-IV).24 ADL performance (ie, what the participants actually did in their everyday life) before the fracture and at the 3- and 12-month follow-ups was assessed using the Barthel ADL Index25,26 along with the ADL Staircase including the Katz ADL Index.27,28 The Barthel Index (0–20; best score 20) and the Katz Index (A to G; A indicating independence) both measure personal ADL (PADL), namely feeding, continence, transfer, toilet use, bathing, and dressing, while the Barthel Index also measures mobility. In the ADL Staircase (0–10; 0 indicating independence in all activities), the Katz Index is extended with four items that measure instrumental ADL (IADL), namely cooking, cleaning, shopping, and using public transport. Walking ability indoors and outdoors before the fracture and at 3 and 12 months was assessed on a scale from 1 to 7, where 1 indicated no functional ability or the need for the assistance of two people and 7 indicated normal function.29 Data on ADL and walking ability were obtained by interviewing the participants, and, if CI was present, also the next of kin or the care staff in the facilities.
Baseline Descriptive Assessments
During the hospital stay, the participant and, when CI was present, the next of kin or a nurse in the residential care facility were interviewed about the participant’s pre-fracture social situation, medical history, and prescribed drugs. In addition, the participants were assessed with the Mini Mental State Examination,30 the Geriatric Depression Scale,31 and the Organic Brain Syndrome Scale.32
Statistical Analysis
LOS was used for sample size calculation and was based on the number of days patients with hip fracture spent in the hospital during one year in a previous study.19 Assuming a power of 80% and a 24% reduction in hospital days, the total sample size was estimated to be 206 participants. In agreement with the intention-to-treat principle, available data from all participants were analyzed according to their original allocation and regardless of level of attendance.
Descriptive statistics were used in comparisons between participants with and without dementia and between treatment groups (GIHR vs control) among the participants with and without dementia. Student´s t-test for independent samples was used for normally distributed continuous variables, and the Mann–Whitney U-test was used for ordinal data and for non-normally distributed continuous variables. Binary data were analyzed with Pearson´s chi-square test (with Yates’s continuity correction) or Fisher´s exact test.
Binary logistic regression was used to evaluate the associations (odds ratio [OR]) between dementia and the risk of falling and mortality after discharge and between dementia and performance in ADL and walking ability at 3 and 12 months. Analysis using Cox regression was considered for the outcomes related to falls and mortality, but this was considered inappropriate because the proportional hazard assumptions were not fulfilled. The regression models were unadjusted, except for the analysis of falling after discharge, which was adjusted for observation time. Observation time was registered as the time from discharge until the end of the study or until the participant died, declined participation, or for other reasons left the study. The total score on the Barthel ADL Index was dichotomized at the median value (<18, ≥18), and category A in the Katz ADL Index was considered as independent PADL performance. To investigate if the treatment effect on the outcomes was different among people with dementia, we also used binary logistic regression in separate models where an interaction term was added to each model between dementia (yes/no) and type of treatment (GIHR or control), and the P-value of the interaction was reported.
Analyses were performed using SPSS version 25.0 (IBM SPSS Statistics for Windows, Armonk, NY: IBM Corp.). All statistical tests were 2-tailed, and P < 0.05 was considered statistically significant.
Results
Of the 205 participants included in the study, 103 (50.2%) were diagnosed with dementia, 57 in the GIHR group and 46 in the control group (P=0.444) (Figure 1). The baseline characteristics of the participants included in the study are presented in Table 1. The most common dementia type was Alzheimer´s disease (n=49, 47.6%). Fourteen (13.6%) had vascular dementia, while 40 (38.8%) had other types of dementia such as mixed Alzheimer and vascular, frontotemporal, Parkinson, Lewy body, alcohol-related, or unspecified dementia. Among those with dementia, a larger proportion in the control group were prescribed analgesics compared with the GIHR group (P=0.048).
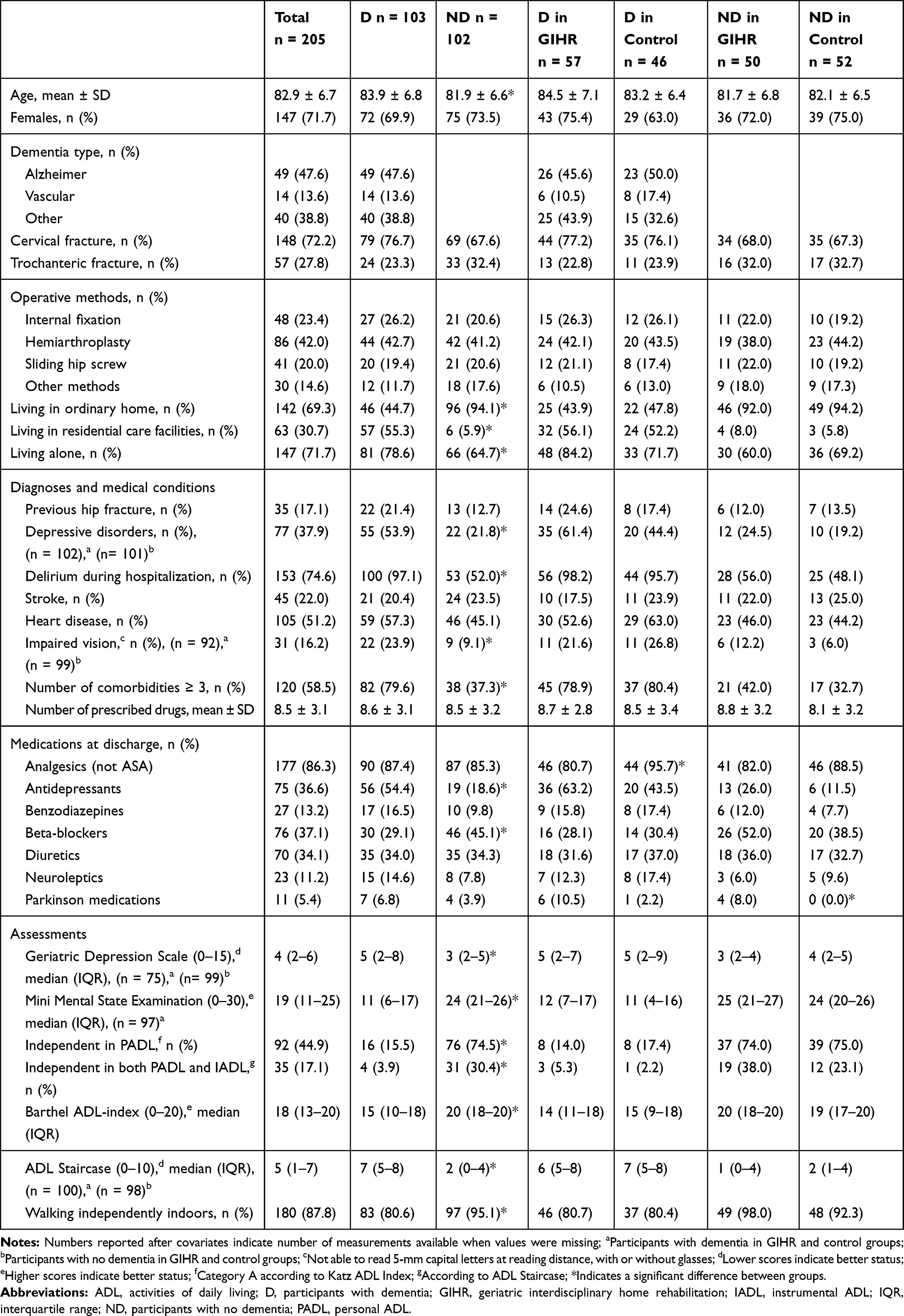 |
Table 1 Characteristics of the Study Population and Baseline Measures |
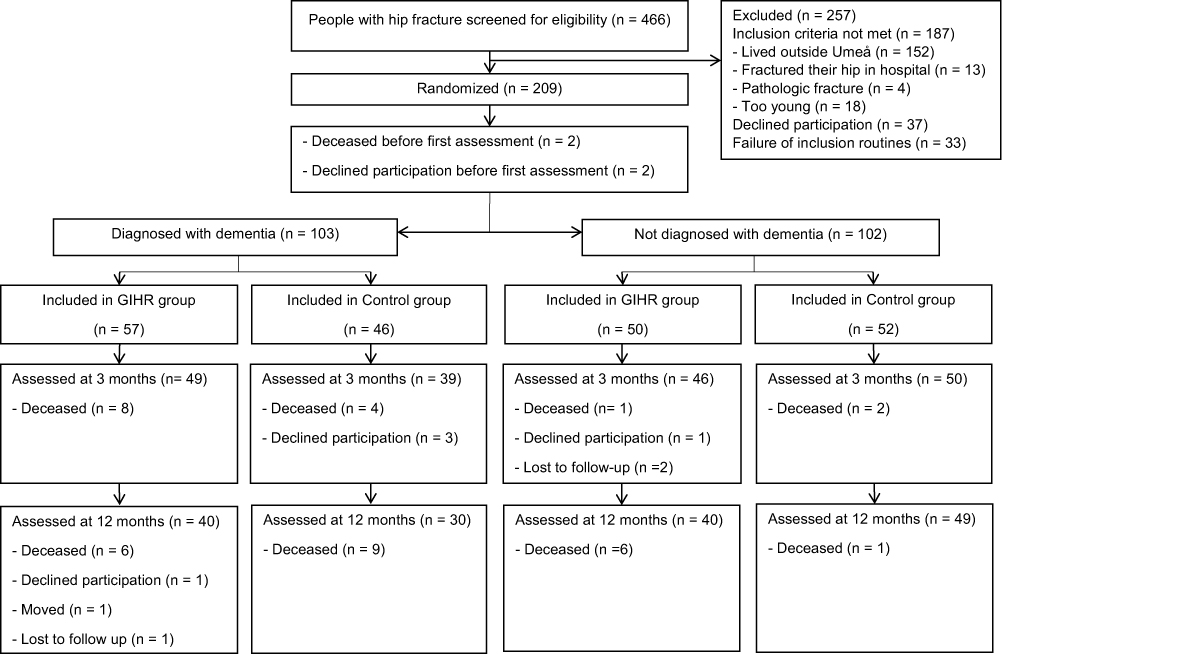 |
Figure 1 Flow of participants through the study. |
Effects of the GIHR Intervention
No statistically significant interaction was found between dementia (yes/no) at baseline and type of treatment (GIHR or control) on the risk of falling at least once during the year after discharge (P=0.100) or on measures of ADL or walking ability at 3 and 12 months (Table 2). In relation to mortality, however, a statistically significant interaction was found (P=0.035). Further analysis showed that for participants with dementia allocated to the GIHR group (compared with the control group) the OR for death after discharge was 0.67; 95% CI: 0.27–1.66 (P=0.392), whereas the OR for participants without dementia in the GIHR group was 8.14; 95% CI: 0.96–68.81 (P=0.054).
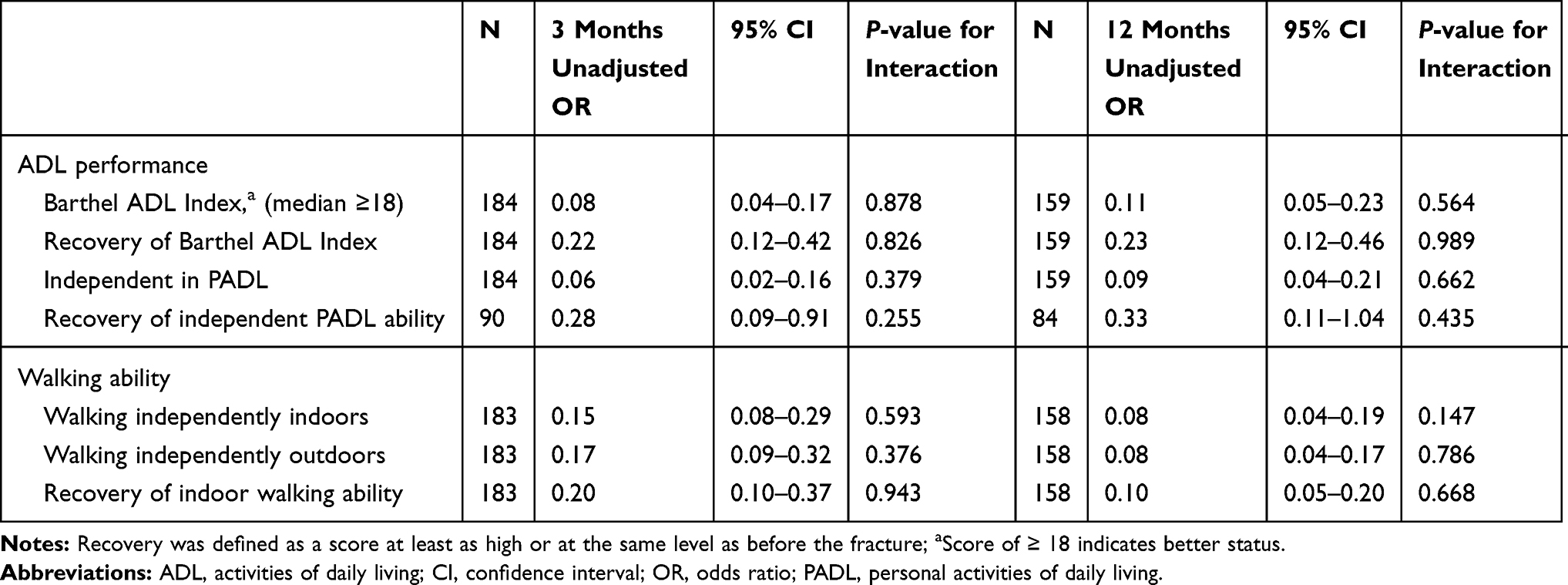 |
Table 2 Odds Ratios of Functional Performance at the 3- and 12-Month Follow-Ups for Participants with Dementia Compared to Those Without Dementia, and Interaction Effects Between Dementia (Yes/No) and Type of Treatment (GIHR or Control) |
When analyzing the effects of the GIHR intervention solely among the participants with dementia, we found no significant differences between the GIHR and control groups in postoperative LOS, readmissions, falls, or mortality between discharge and 12 months or in ADL or walking ability at 3 and 12 months (Tables 3 and 4).
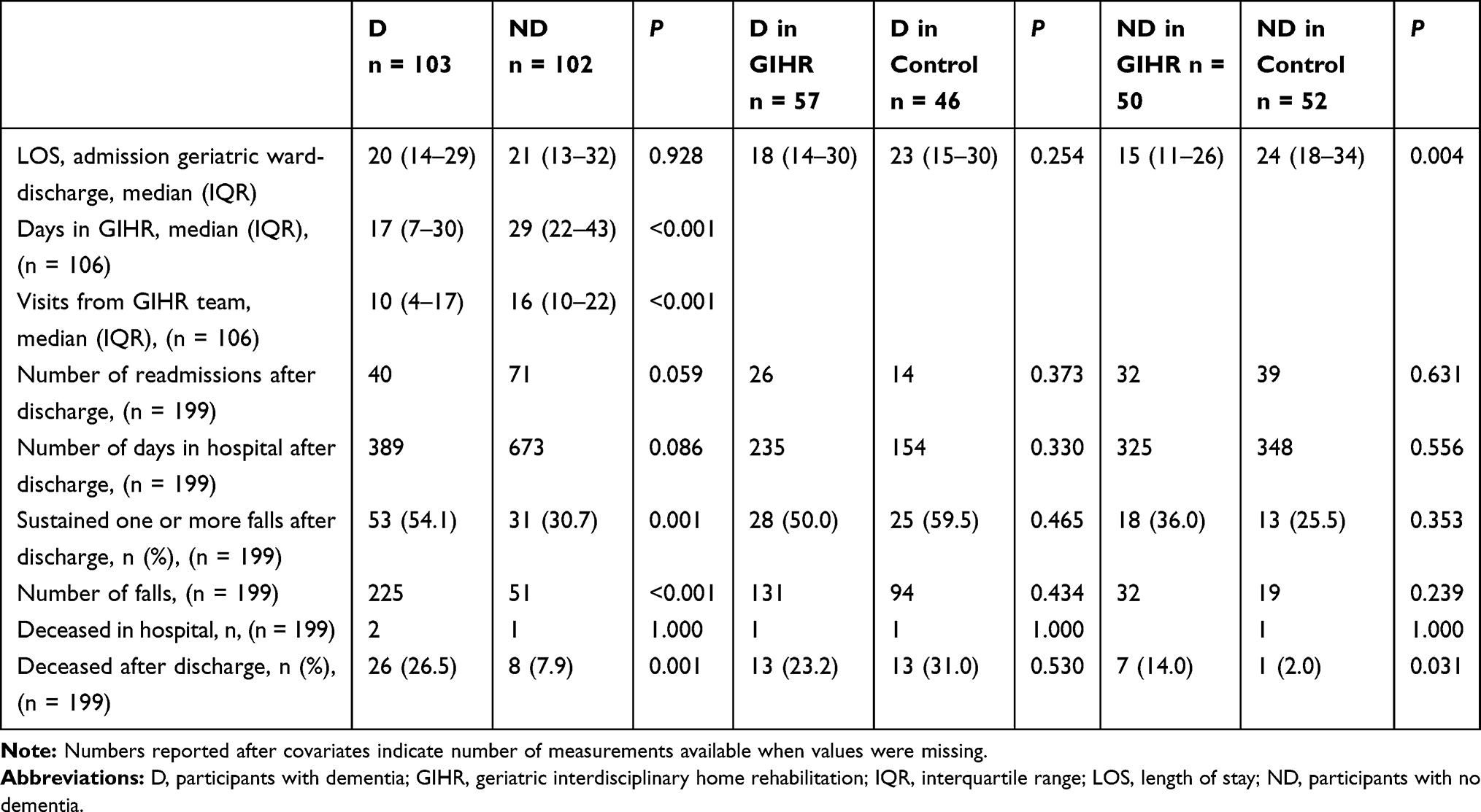 |
Table 3 Postoperative Use of Health Care and Falls and Mortality Between Discharge and 12 Months |
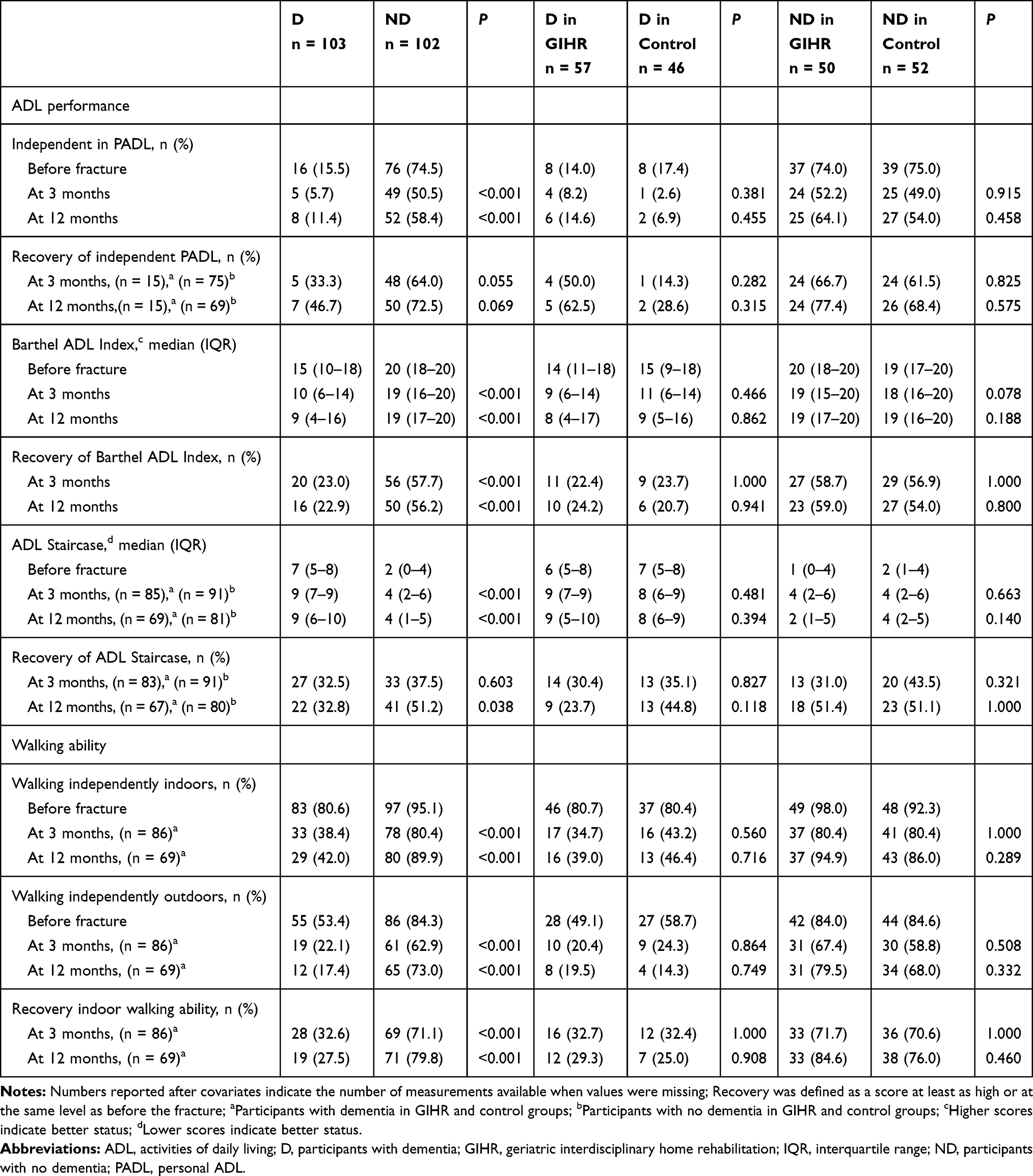 |
Table 4 ADL Performance and Walking Ability Before Fracture and at the 3- and 12-Month Follow-Ups |
Overall Outcome in People with Dementia
Between-group comparisons based on whether the participants had dementia or not, and irrespective of type of treatment, showed significantly worse results in most of the outcomes for the participants with dementia (Tables 3 and 4). The postoperative LOS was comparable between participants with and without dementia, but the GIHR intervention was significantly shorter and involved less frequent home visits for the participants with dementia than their counterparts without dementia (Table 3). No significant differences were seen for readmissions or total days in hospital during the year after discharge between participants with and without dementia (Table 3). Binary logistic regression analyses revealed a higher risk for falls after discharge (OR 3.86; 95% CI: 2.05–7.27, P<0.001) and increased mortality (OR 4.20; 95% CI 1.79–9.82, P=0.001) for participants with dementia compared to those without dementia. Additionally, dementia was associated with impaired performance in ADL (OR between 0.06 and 0.23, P<0.001 for all) and with impaired walking ability (OR between 0.08 and 0.20, P<0.001 for all) at the 3- and 12-month follow-ups compared with participants without dementia (Table 2). However, for recovery of independent PADL performance there was a significant difference between participants with and without dementia at 3 months (OR 0.28; 95% CI 0.09–0.91, P=0.034), but not at the 12-month follow-up (OR 0.33; 95% CI 0.11–1.04, P=0.059).
Discussion
This study showed that a GIHR intervention compared with in-hospital geriatric care according to a multifactorial rehabilitation program had comparable effects on falls and mortality between discharge and 12 months and on ADL and walking ability at 3 and 12 months regardless of whether the participants had dementia or not. Among the participants with dementia, the postoperative LOS was 5 days shorter in the GIHR group compared with controls, but this was not a significant reduction, and there were comparable numbers of readmissions. However, the study did show a substantial negative impact of dementia on the outcomes after hip fracture compared with participants without dementia.
The findings of the present study suggest that GIHR can be a complement to in-hospital rehabilitation after hip fracture for older people with dementia, which is an important clinical implication because severe CI or dementia and residing in residential care have been exclusion criteria in previous team-based HR interventions.33–37 Two previous subgroup analyses of RCTs have reported on the effects of an HR intervention after the postoperative hospital stay for people with CI.13,14 Shyu et al13 found that in people with mild to moderate CI, 3 months of interdisciplinary HR after the hip fracture resulted in better ADL performance and recovery of walking ability than controls who received routine care in hospital. The other study evaluated an intensive team-based in-hospital intervention that also included 10 home visits from a physiotherapist.14 This HR intervention showed that participants with mild to moderate CI, but not those with severe CI or normal scores, had shorter LOS and that fewer needed institutional care one year after the hip fracture compared with those who had rehabilitation in local hospitals. In contrast to the present study, CI in these studies was based on the Mini Mental State Examination scores and not on a physician-based dementia diagnosis. Furthermore, the samples in those studies were healthier because people were excluded if no consent to participate could be provided, eg, in the case of severe dementia, or if people had severe functional limitations before the fracture. The contents of the control interventions were also different from our study. In the present study the control group received rehabilitation according to a multifactorial rehabilitation program, which could be considered as best practice.
Falls post-discharge were more common in participants with dementia than in those without dementia, which highlights the importance of fall prevention in this population, although the evidence for the effectiveness of fall prevention interventions in people with dementia is limited.38–40 The GIHR intervention included multifactorial actions to prevent falls with exercise as one component as recommended.39,40 The exercise was individually adapted and included balance, strength, and functional exercises and was supervised in order to be safe to perform and to achieve as high intensity as possible. The results showed, however, that participants with dementia had a similar risk of falls as well as mortality after discharge, irrespective of the type of intervention. Surprisingly, among the participants without dementia, mortality was higher in the GIHR than in control groups because 7 participants in the GIHR group vs only 1 in the control group died between discharge and the 12-month follow-up. We believe, however, that this should be interpreted with caution and should be further evaluated in future research. Another unexpected finding was a trend for fewer readmissions and total days in hospital during the year after discharge among the participants with dementia compared with those without dementia. This might be explained by the fact that a large number of the participants with dementia lived in residential care where many medical conditions could be treated, and thus the number of hospital admissions was reduced. Additionally, this could also have contributed to the GIHR intervention being shorter with less frequent home visits for participants with dementia than for those without dementia. The facilities have established ways of working with their own rehabilitation staff. The GIHR team might have found it challenging to accomplish and maintain a continuous, successful team work with the care staff because of the different organizational routines. It is also possible that some of the participants in the facilities could receive a shorter home rehabilitation intervention because of dedicated staff contributing to their rehabilitation.
Because dementia is the leading cause of dependence in ADL41 and is a progressive disease, we expected to find poorer ADL performance and walking ability among the participants with dementia than those without, particularly from the long-term perspective. At 12 months, 23% of the participants with dementia had recovered their pre-fracture Barthel Index and 28% had recovered their pre-fracture indoor walking ability, and the corresponding numbers for those without dementia were 56% and 80%. According to the ADL Staircase, which measures both PADL and IADL, a significant difference in recovery between participants with and without dementia was found only at 12 months. This result may reflect that recovery of IADL activities tends to be slower than PADL with possible improvements during the first year following the fracture.42
Current recommendations regarding post hip fracture rehabilitation for people with dementia involve interdisciplinary person-centered approaches in settings that are adapted to the needs of this vulnerable population,43 where family and caregivers should also be involved.44 The interventions should address comorbidities and postoperative complications as well as behavioral problems connected to the dementia diagnosis.6,43 Education is also needed to change attitudes among care staff and health-care management.43 The present study was pragmatic and not tailored specifically for people with dementia, but towards old and vulnerable people with multi-comorbidity, including dementia. The clinical experience of the GIHR team is that the intervention is possible to carry out among people with dementia, although it is more challenging because complicating symptoms connected with the disease have to be considered. The feasibility of the intervention was, however, not systematically evaluated, and this should be further explored. Receiving rehabilitation in the home setting might be beneficial for common problems among people with dementia, such as an impaired ability to transfer skills,45 apathy, anxiety about upcoming events,46 and low motivation to participate in activities such as exercise programs.41 The familiar environment may increase the motivation for functional activities, and next of kin and caregivers may be able to participate more actively in the rehabilitation. Moreover, there is no need for transport, which could otherwise be a barrier.46
A strength of the study is that we included a representative sample of older people with hip fracture, including those with severe CI and dementia and people in residential care facilities, which increases the external validity of the study. These are groups in which the evidence of the optimal rehabilitation strategies is most insufficient.6 Moreover, dementia at baseline was diagnosed according to the DSM-IV criteria, and 3- and 12-month follow-ups were performed in the participants´ homes to make it easier for the participants and thereby reduce the number of drop-outs.
There are some limitations to consider. Subgroup analyses are known to have low statistical power to detect differences in subgroup effects, although we used interaction analyses, which is the recommended method.47 Moreover, the RCT was not designed to be a non-inferiority study, which means that it was likely underpowered to show equivalence. The lack of difference between the groups may therefore be a consequence of insufficient power. Additionally, the analysis of people with dementia was not pre-specified in the trial protocol. Despite this, we considered it to be of clinical importance to evaluate the GIHR intervention in this subpopulation because half of the study participants were diagnosed with dementia at baseline and they differed significantly from those without dementia in a number of baseline characteristics. Consequently, the randomization of the study was not stratified according to dementia, but to type of fracture and place of residence. Because a majority of the participants with dementia resided in residential care, which was one of the study stratifications, there were no baseline differences between the GIHR and control group among those with dementia, except for analgesics being more common in the control group. Lastly, we had no access to the written documentation in the residential care facilities, and therefore only had limited information about possible additional rehabilitative actions besides the GIHR intervention. This makes it more difficult to evaluate the effects of the intervention, although it is likely that any such actions would have influenced the study outcomes randomly.
Conclusions
The effects of a GIHR intervention after hip fracture compared with in-hospital geriatric care according to a multifactorial rehabilitation program did not differ in participants with and without dementia. However, the statistical power of this subgroup analysis was likely insufficient to detect differences between the groups. Dementia was associated with a substantial negative impact on the outcomes following the hip fracture. Our findings support that interdisciplinary HR after hip fracture should be offered to older people with dementia in clinical practice, but more research on the effectiveness of interdisciplinary HR after hip fracture in people with dementia is needed.
Abbreviations
ADL, activities of daily living; CI, cognitive impairment; 95% CI, confidence interval; GIHR, geriatric interdisciplinary home rehabilitation; HR, home rehabilitation; IADL, instrumental ADL; LOS, length of stay; OR, odds ratio; PADL, personal ADL; RCT, randomized controlled trial.
Data Sharing Statement
Participant data are not available in accordance with the General Data Protection Regulation (European Union Regulation).
Ethics Approval
The original study was conducted in accordance with the Declaration of Helsinki and approved by the Regional Ethical Review Board in Umeå, Sweden, in 2008 (DNR 08-053M).
Acknowledgments
We would like to express our sincere gratitude to the participants, the care staff at the geriatric ward, and the home rehabilitation team at the University Hospital in Umeå for participation in the study. We also want to thank Helen Abrahamsson, OT, Eva Elinge, OT, Med Lic, and Anita Persson, RN who contributed to the development and implementation of the study.
Disclosure
Mrs Åsa Karlsson reports grants from Umeå University and County Council of Västerbotten, grants from Strategic Research Area Health Care Sciences, Umeå University, grants from Swedish Dementia Association, during the conduct of the study. The authors report no other conflicts of interest in this work.
References
1. World Health Organization. Geneva: global action plan on the public health response to dementia 2017–2025. 2017. Available from: https://www.who.int/mental_health/neurology/dementia/action_plan_2017_2025/en/.
2. Baker NL, Cook MN, Arrighi HM, Bullock R. Hip fracture risk and subsequent mortality among Alzheimer’s disease patients in the United Kingdom, 1988–2007. Age Ageing. 2011;40(1):49–54. doi:10.1093/ageing/afq146
3. Seitz DP, Gill SS, Gruneir A, et al. Effects of dementia on postoperative outcomes of older adults with hip fractures: a population-based study. J Am Med Dir Assoc. 2014;15(5):334–341. doi:10.1016/j.jamda.2013.12.011
4. Bai J, Zhang P, Liang X, Wu Z, Wang J, Liang Y. Association between dementia and mortality in the elderly patients undergoing hip fracture surgery: a meta-analysis. J Orthop Surg Res. 2018;13(1):298. doi:10.1186/s13018-018-0988-6
5. Tarazona-Santabalbina FJ, Belenguer-Varea A, Rovira Daudi E, et al. Severity of cognitive impairment as a prognostic factor for mortality and functional recovery of geriatric patients with hip fracture. Geriatr Gerontol Int. 2015;15(3):289–295. doi:10.1111/ggi.12271
6. Smith TO, Gilbert AW, Sreekanta A, et al. Enhanced rehabilitation and care models for adults with dementia following hip fracture surgery. Cochrane Database Syst Rev. 2020;2:CD010569.
7. Ariza-Vega P, Lozano-Lozano M, Olmedo-Requena R, Martin-Martin L, Jimenez-Moleon JJ. Influence of cognitive impairment on mobility recovery of patients with hip fracture. Am J Phys Med Rehabil. 2017;96(2):109–115. doi:10.1097/PHM.0000000000000550
8. Sheehan KJ, Fitzgerald L, Hatherley S, et al. Inequity in rehabilitation interventions after hip fracture: a systematic review. Age Ageing. 2019;48(4):489–497. doi:10.1093/ageing/afz031
9. Al-Ani AN, Flodin L, Söderqvist A, et al. Does rehabilitation matter in patients with femoral neck fracture and cognitive impairment? A prospective study of 246 patients. Arch Phys Med Rehabil. 2010;91(1):51–57. doi:10.1016/j.apmr.2009.09.005
10. Stenvall M, Berggren M, Lundström M, Gustafson Y, Olofsson B. A multidisciplinary intervention program improved the outcome after hip fracture for people with dementia—Subgroup analyses of a randomized controlled trial. Arch Gerontol Geriatr. 2012;54(3):e284–289. doi:10.1016/j.archger.2011.08.013
11. Seitz DP, Gill SS, Austin PC, et al. Rehabilitation of older adults with dementia after hip fracture. J Am Geriatr Soc. 2016;64(1):47–54. doi:10.1111/jgs.13881
12. Resnick B, Beaupre L, McGilton KS, et al. Rehabilitation interventions for older individuals with cognitive impairment post-hip fracture: a systematic review. J Am Med Dir Assoc. 2016;17(3):200–205. doi:10.1016/j.jamda.2015.10.004
13. Shyu YI, Tsai WC, Chen MC, et al. Two-year effects of an interdisciplinary intervention on recovery following hip fracture in older Taiwanese with cognitive impairment. Int J Geriatr Psychiatry. 2012;27(5):529–538. doi:10.1002/gps.2750
14. Huusko TM, Karppi P, Avikainen V, Kautiainen H, Sulkava R. Randomised, clinically controlled trial of intensive geriatric rehabilitation in patients with hip fracture: subgroup analysis of patients with dementia. BMJ. 2000;321(7269):1107–1111. doi:10.1136/bmj.321.7269.1107
15. Crotty M, Killington M, Liu E, et al. Should we provide outreach rehabilitation to very old people living in Nursing Care Facilities after a hip fracture? A randomised controlled trial. Age Ageing. 2019;48(3):373–380. doi:10.1093/ageing/afz005
16. Karlsson Å, Lindelöf N, Olofsson B, et al. Effects of geriatric interdisciplinary home rehabilitation on independence in activities of daily living in older people with hip fracture: a randomized controlled trial. Arch Phys Med Rehabil. 2020;101(4):571–578. doi:10.1016/j.apmr.2019.12.007
17. Karlsson Å, Berggren M, Gustafson Y, Olofsson B, Lindelöf N, Stenvall M. Effects of geriatric interdisciplinary home rehabilitation on walking ability and length of hospital stay after hip fracture: a randomized controlled trial. J Am Med Dir Assoc. 2016;17(5):
18. Berggren M, Karlsson Å, Lindelöf N, et al. Effects of geriatric interdisciplinary home rehabilitation on complications and readmissions after hip fracture: a randomized controlled trial. Clin Rehabil. 2019;33:64–73. doi:10.1177/0269215518791003
19. Stenvall M, Olofsson B, Lundström M, et al. A multidisciplinary, multifactorial intervention program reduces postoperative falls and injuries after femoral neck fracture. Osteoporos Int. 2007;18(2):167–175. doi:10.1007/s00198-006-0226-7
20. Lundström M, Olofsson B, Stenvall M, et al. Postoperative delirium in old patients with femoral neck fracture: a randomized intervention study. Aging Clin Exp Res. 2007;19(3):178–186. doi:10.1007/BF03324687
21. Stenvall M, Olofsson B, Nyberg L, Lundström M, Gustafson Y. Improved performance in activities of daily living and mobility after a multidisciplinary postoperative rehabilitation in older people with femoral neck fracture: a randomized controlled trial with 1-year follow-up. J Rehabil Med. 2007;39(3):232–238. doi:10.2340/16501977-0045
22. Littbrand H, Rosendahl E, Lindelöf N, Lundin-Olsson L, Gustafson Y, Nyberg L. A high-intensity functional weight-bearing exercise program for older people dependent in activities of daily living and living in residential care facilities: evaluation of the applicability with focus on cognitive function. Phys Ther. 2006;86(4):489–498. doi:10.1093/ptj/86.4.489
23. Littbrand H, Lindelöf N, Rosendahl E. The High-Intensity Functional Exercise (HIFE) Program. Sweden: Department of Community Medicine and Rehabilitation, Umeå University; 2018. Available from: https://www.hifeprogram.se/en.
24. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders.
25. Mahoney FI, Barthel DW. Functional evaluation: the Barthel index. Md State Med J. 1965;14:61–65
26. Wade DT. Measurement in Neurological Rehabilitation. Oxford: Oxford Univ, Press; 1992.
27. Sonn U, Törnquist K, Svensson E. The ADL taxonomy- from individual categorical data to ordinal categorical data. Scand J Occup Ther. 1999;6(11):11–20. doi:10.1080/110381299443807
28. Katz S, Akpom CA. A measure of primary sociobiological functions. Int J Health Serv. 1976;6(3):493–508. doi:10.2190/UURL-2RYU-WRYD-EY3K
29. Hasselgren Nyberg L, Omgren M, Nyberg L, Gustafson Y. Den svenska versionen av physiotherapy clinical outcome variable scale [the swedish version of the scale]. Nordisk Fysioterapi. 1997;1:109–113.
30. Folstein MF, Folstein SE, McHugh PR. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. 1975;12(3):189–198. doi:10.1016/0022-3956(75)90026-6
31. Sheikh J, Yesavage J. Geriatric depression scale (GDS): recent evidence and development of a shorter version. Clin Gerontol. 1986;5:165–173. doi:10.1300/J018v05n01_09
32. Berggren D, Gustafson Y, Eriksson B, et al. Postoperative confusion after anesthesia in elderly patients with femoral neck fractures. Anesth Analg. 1987;66(6):497–504. doi:10.1213/00000539-198706000-00003
33. Tinetti ME, Baker DI, Gottschalk M, et al. Home-based multicomponent rehabilitation program for older persons after hip fracture: a randomized trial. Arch Phys Med Rehabil. 1999;80(8):916–922. doi:10.1016/S0003-9993(99)90083-7
34. Crotty M, Whitehead CH, Gray S, Finucane PM. Early discharge and home rehabilitation after hip fracture achieves functional improvements: a randomized controlled trial. Clin Rehabil. 2002;16(4):406–413. doi:10.1191/0269215502cr518oa
35. Ziden L, Frändin K, Kreuter M. Home rehabilitation after hip fracture. A randomized controlled study on balance confidence, physical function and everyday activities. Clin Rehabil. 2008;22(12):1019–1033. doi:10.1177/0269215508096183
36. Shyu YI, Liang J, Wu CC, et al. Interdisciplinary intervention for hip fracture in older Taiwanese: benefits last for 1 year. J Gerontol a Biol Sci Med Sci. 2008;63(1):92–97. doi:10.1093/gerona/63.1.92
37. Shyu YI, Liang J, Tseng MY, et al. Comprehensive care improves health outcomes among elderly Taiwanese patients with hip fracture. J Gerontol a Biol Sci Med Sci. 2013;68(2):188–197. doi:10.1093/gerona/gls164
38. Burton E, Cavalheri V, Adams R, et al. Effectiveness of exercise programs to reduce falls in older people with dementia living in the community: a systematic review and meta-analysis. Clin Interv Aging. 2015;10:421–434. doi:10.2147/CIA.S71691
39. Hopewell S, Adedire O, Copsey BJ, et al. Multifactorial and multiple component interventions for preventing falls in older people living in the community. Cochrane Database Syst Rev. 2018;7:CD012221.
40. Cameron ID, Dyer SM, Panagoda CE, et al. Interventions for preventing falls in older people in care facilities and hospitals. Cochrane Database Syst Rev. 2018;9:CD005465.
41. World Health Organisation. Geneva: dementia: a public health priority. 2012. Available from: http://www.who.int/mental_health/publications/dementia_report_2012/en/.
42. Magaziner J, Hawkes W, Hebel JR, et al. Recovery from hip fracture in eight areas of function. J Gerontol a Biol Sci Med Sci. 2000;55(9):M498–507. doi:10.1093/gerona/55.9.M498
43. Gill N, Hammond S, Cross J, Smith T, Lambert N, Fox C. Optimising care for patients with cognitive impairment and dementia following hip fracture. Z Gerontol Geriatr. 2017;50(Suppl 2):S39–43. doi:10.1007/s00391-017-1224-4
44. McGilton KS, Chu CH, Naglie G, van Wyk PM, Stewart S, Davis AM. Factors influencing outcomes of older adults after undergoing rehabilitation for hip fracture. J Am Geriatr Soc. 2016;64(8):1601–1609. doi:10.1111/jgs.14297
45. van Halteren-van Tilborg IA, Scherder EJ, Hulstijn W. Motor-skill learning in Alzheimer’s disease: a review with an eye to the clinical practice. Neuropsychol Rev. 2007;17(3):203–212. doi:10.1007/s11065-007-9030-1
46. van Alphen HJ, Hortobagyi T, van Heuvelen MJ. Barriers, motivators, and facilitators of physical activity in dementia patients: a systematic review. Arch Gerontol Geriatr. 2016;66:109–118. doi:10.1016/j.archger.2016.05.008
47. Moher D, Hopewell S, Schulz KF, et al. CONSORT 2010 explanation and elaboration: updated guidelines for reporting parallel group randomised trials. Int J Surg. 2012;10(1):28–55. doi:10.1016/j.ijsu.2011.10.001
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.