")
Back to Journals » Infection and Drug Resistance » Volume 10
Genotypic distribution of multidrug-resistant and extensively drug-resistant tuberculosis in northern Thailand
Authors Jaksuwan R, Tharavichikul P, Patumanond J, Chuchottaworn C, Chanwong S, Smithtikarn S, Settakorn J
Received 14 December 2016
Accepted for publication 16 March 2017
Published 10 June 2017 Volume 2017:10 Pages 167—174
DOI https://doi.org/10.2147/IDR.S130203
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Risara Jaksuwan,1 Prasit Tharavichikul,2 Jayanton Patumanond,3 Charoen Chuchottaworn,4 Sakarin Chanwong,5 Saijai Smithtikarn,6 Jongkolnee Settakorn7
1Clinical Epidemiology Unit, 2Department of Microbiology, Faculty of Medicine, Chiang Mai University, Chiang Mai, 3Division of Clinical Epidemiology, Faculty of Medicine, Thammasat University, Pathum Thani, 4Division of Respiratory Medicine, Chest Disease Institute, Nonthaburi, 5Office of Disease Prevention and Control Region 10, Chiang Mai, 6Bureau of Tuberculosis, Department of Disease Control, Ministry of Public Health, Bangkok, 7Department of Pathology, Faculty of Medicine, Chiang Mai University, Chiang Mai, Thailand
Background: Multidrug/extensively drug-resistant tuberculosis (M/XDR-TB) is a major public health problem, and early detection is important for preventing its spread. This study aimed to demonstrate the distribution of genetic site mutation associated with drug resistance in M/XDR-TB in the northern Thai population.
Methods: Thirty-four clinical MTB isolates from M/XDR-TB patients in the upper northern region of Thailand, who had been identified for drug susceptibility using the indirect agar proportion method from 2005 to 2012, were examined for genetic site mutations of katG, inhA, and ahpC for isoniazid (INH) drug resistance and rpoB for rifampicin (RIF) drug resistance. The variables included the baseline characteristics of the resistant gene, genetic site mutations, and drug susceptibility test results.
Results: All 34 isolates resisted both INH and RIF. Thirty-two isolates (94.1%) showed a mutation of at least 1 codon for katG, inhA, and ahpC genes. Twenty-eight isolates (82.4%) had a mutation of at least 1 codon of rpoB gene. The katG, inhA, ahpC, and rpoB mutations were detected in 20 (58.7%), 27 (79.4%), 13 (38.2%), and 28 (82.3%) of 34 isolates. The 3 most common mutation codons were katG 315 (11/34, 35.3%), inhA 14 (11/34, 32.4%), and inhA 114 (11/34, 32.4%). For this population, the best genetic mutation test panels for INH resistance included 8 codons (katG 310, katG 340, katG 343, inhA 14, inhA 84, inhA 86, inhA 114, and ahpC 75), and for RIF resistance included 6 codons (rpoB 445, rpoB 450, rpoB 464, rpoB 490, rpoB 507, and rpoB 508) with a sensitivity of 94.1% and 82.4%, respectively.
Conclusion: The genetic mutation sites for drug resistance in M/XDR-TB are quite variable. The distribution of these mutations in a certain population must be studied before developing the specific mutation test panels for each area. The results of this study can be applied for further molecular M/XDR-TB diagnosis in the upper northern region of Thailand.
Keywords: tuberculosis, drug resistance, MDR-TB, XDR-TB, genotype, mutation
Introduction
Tuberculosis (TB) is an important global problem, especially multidrug-resistant TB (MDR-TB) and extensively drug-resistant TB (XDR-TB). In 2015, the world-wide estimation of MDR-TB cases and deaths was 80,000 and 250,000, respectively.1 MDR-TB is caused by Mycobacterium tuberculosis (MTB), which resists at least 2 drugs (isoniazid [INH] and rifampicin [RIF]). Pre-XDR-TB is a disease caused by the M. tuberculosis strain, which resists INH and RIF and either a fluoroquinolone or a second-line injectable drug, but not both.1 XDR-TB is defined as MDR-TB, which adds more resistance to any fluoroquinolone and at least 1 of 3 injectable second-line drugs (amikacin, capreomycin, and kanamycin [KAN]).2 Approximately 9.5% of MDR-TB patients developed XDR-TB.1 Unfortunately, about 20% of MDR-TB cases were undetectable.1 Thailand is among the countries with a TB burden, as it was ranked within the top 20 countries with TB in 2015.1
Early and accurate detection of M/XDR-TB is important for effectively treating and preventing its transmission.3–6 However, the phenotypic drug susceptibility test (DST) takes weeks or months for culturing MTB and identifying the resisted drugs and requires a high level of microbiological safety.7,8 Diagnosis and treatment delays are among the major causes of the spread of the disease, which interferes with the TB control programs. A rapid molecular TB-DST test greatly increases the efficacy of MDR-TB treatment5,6,9 as the minimal turnaround time is <1 day.10,11
As the distribution of mutation in drug-resistant genes is region specific, knowing the epidemiology of the genetic drug resistance of M/XDR-TB in certain areas would be beneficial for developing specific and rapid molecular tests,8,12 as well as treatment protocols,13 because the prevalence of such resistance differs in various populations.14–16 Many studies have focused on genetic drug resistance in MTB. INH is the main drug used; it is an effective anti-TB drug and has been used till date.2,11 The mechanism of INH resistance in MTB is associated with the mutations of katG, inhA, and ahpC.17–19 The katG mutation was found in high levels of INH resistance,20,21 and the inhA mutation was found at low levels or monoresistance to INH.20,22 RIF is combined with INH as the main anti-TB drug, and it is inferred with transcription by the DNA-dependent RNA polymerase by binding to the β-subunit hindering transcription organisms related to rpoB 531 mutation,23–25 which destroys the organisms.26,27
In this study, we examined the distribution of drug-resistant gene mutations, including katG, inhA, ahpC, and rpoB, in M/XDR-TB isolates in the northern Thai population. Then, we identified the best mutation test panels for INH and RIF resistance.
Materials and methods
Two hundred and sixty-one M/XDR-TB isolates first diagnosed with MDR-TB or XDR-TB from patients between January 2005 and June 2012 were retrieved from an archive of the Laboratory of the Office of Disease Prevention and Control Region 10 (DPC10). According to the World Health Organization (WHO) criteria, MDR isolates resisted at least INH and RIF; and XDR isolates resisted INH, RIF, ofloxacin (OFX), and KAN. DPC10 hosts a regional TB laboratory, covering 8 provinces in the north of Thailand, and the isolates were subcultured. Only 34 specimens (9.5%) were grown in 5 mL of 7H9 broth supplemented with PANTA in 6 weeks and 3% Ogawa within 8 weeks. The bacterial agents were further examined for phenotypic DST and DNA sequencing.
Phenotypic drug susceptibility test
Thirty-four growing M/XDR-TB isolates were tested for first- and second-line drug resistance (INH, RIF, OFX, and KAN) using the proportion method with Lowensentein Jensen (LJ) medium28 at DPC10 laboratory. The DOTS-plus DST was performed according to the WHO guidelines,29 and all suspected TB and MDR-TB patients were investigated using 3 methods: 3 direct acid-fast bacilli sputum smear examinations, a Mycobacterium culture, and first-line DST,29 during the first diagnosis. Additionally, at the same time, a molecular test was carried out in order to confirm M. tuberculosis. DST was determined using the indirect agar proportion method with INH, RIF, streptomycin, and ethambutol. If there was resistance to INH and/or RIF, a second-line anti-TB DST was performed with OFX and KAN. For our study, LJ medium was supplemented individually with anti-TB drugs. INH (0.2 µg/mL), RIF (40.0 µg/mL), OFX (2.0 µg/mL), and KAN (30 µg/mL) were repeated in order to confirm that the results were the same as the previous results; if the results were not the same then they were excluded from the study.
DNA extraction
Thirty-four M/XDR-TB isolates were cultured on solid media (LJ and OGAWA). Chromosomal DNA was extracted using the MolecuTech REBA MTB-MDR 2011 commercial kit. Briefly, 1 loop (0.2 μL diameter sterile inoculating loop) of the cultured bacteria was resuspended in 50 μL of DNA extraction solution. The solution was vortexed for 1 min, boiled for 10 min, and centrifuged (13,000 rpm) for 3 min at room temperature. Then, 5–10 μL of the supernatant was transferred to a microtube (cryovial tube). The purified DNA pellet was stored at 4°C.
Sequencing method
The polymerase chain reaction (PCR) and DNA sequencing parts were carried out at Macrogen Laboratory, Seoul, Republic of Korea. Four genetic loci, katG, inhA, ahpC (INH), and rpoB (RIF), were amplified by PCR, as shown in Table S1.30,31 The used primers are shown in Table S1. The amplified products were purified with a multiscreen filter plate (Millipore Corp., Bedford, MA, USA).
Analysis
DNA sequencing analysis
The sequencing data obtained from the ABI3730XL DNA analyzer were investigated for the presence or absence of mutations by alignments with the corresponding nucleotide sequences of M. tuberculosis (H37RV) using the NCBI nucleotide blast program.
Data analysis
The phenotypic DST and genetic site mutation for the DST data sets were compiled using an Excel 2010 database. Statistical analysis was performed using STATA version 11.0. The resistant genes and genetic site mutations were presented according to frequency and percentage.
Results
Among the 34 growing M/XDR-TB isolates, 24 (70.5%) MDR-TB, 9 (26.5%) Pre-XDR-TB, and 1 (3.0%) XDR-TB were identified. All of the isolates were resistant to both INH and RIF. The frequency and patterns of genetic loci mutation are demonstrated in Tables 1 and 2. Table 3 exhibits the raw data of genetic mutation in all 34 isolates. Mutations were found, including katG in 20 isolates (58.8%), inhA in 27 isolates (79.4%), ahpC in 13 isolates (38.2%), and rpoB in 28 isolates (82.3%). INH-resistant gene mutations were found in 32 isolates (94.1% sensitivity). RIF-resistant gene mutations were identified in 28 isolates (82.4% sensitivity).
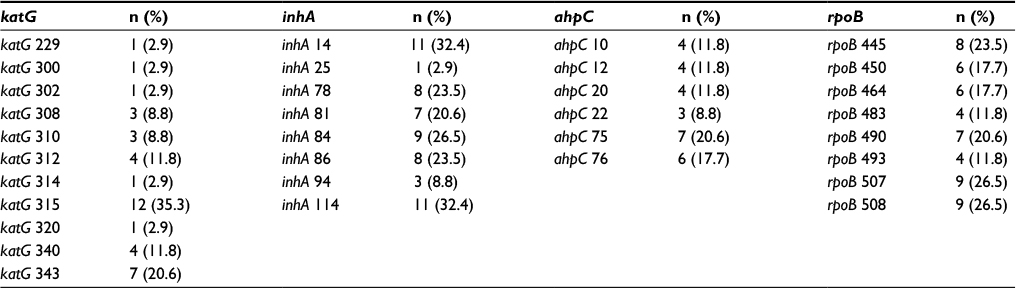 | Table 1 Frequency of genetic site mutations of katG, inhA, ahpC, and rpoB genes in 34 M/XDR-TB isolates Abbreviation: M/XDR-TB, multidrug/extensively drug-resistant tuberculosis. |
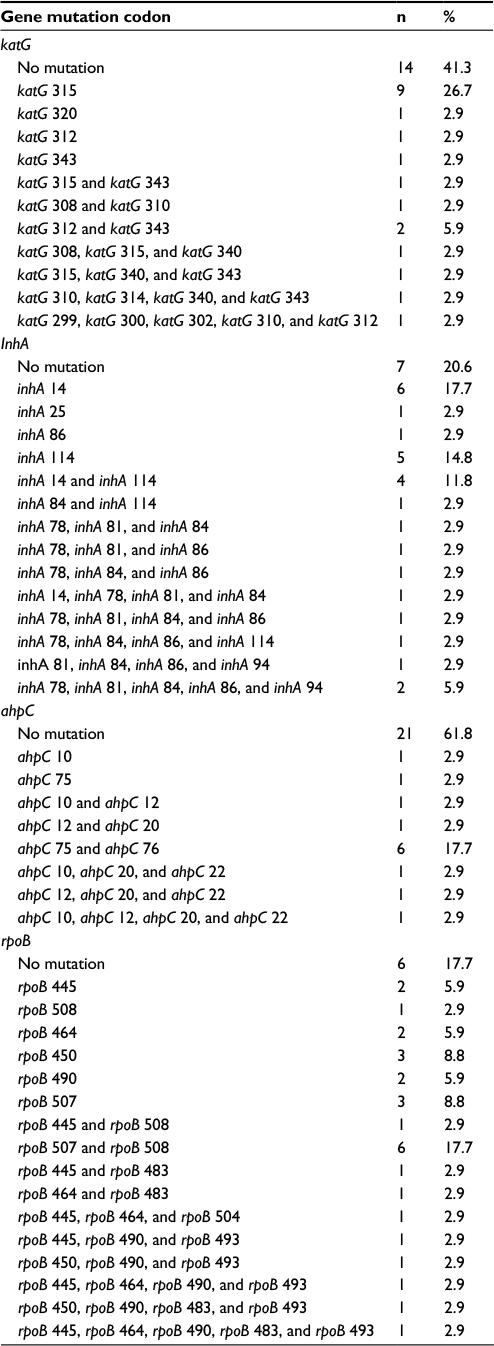 | Table 2 Distribution of Mycobacterium tuberculosis genetic mutations with isoniazid and rifampicin resistance |
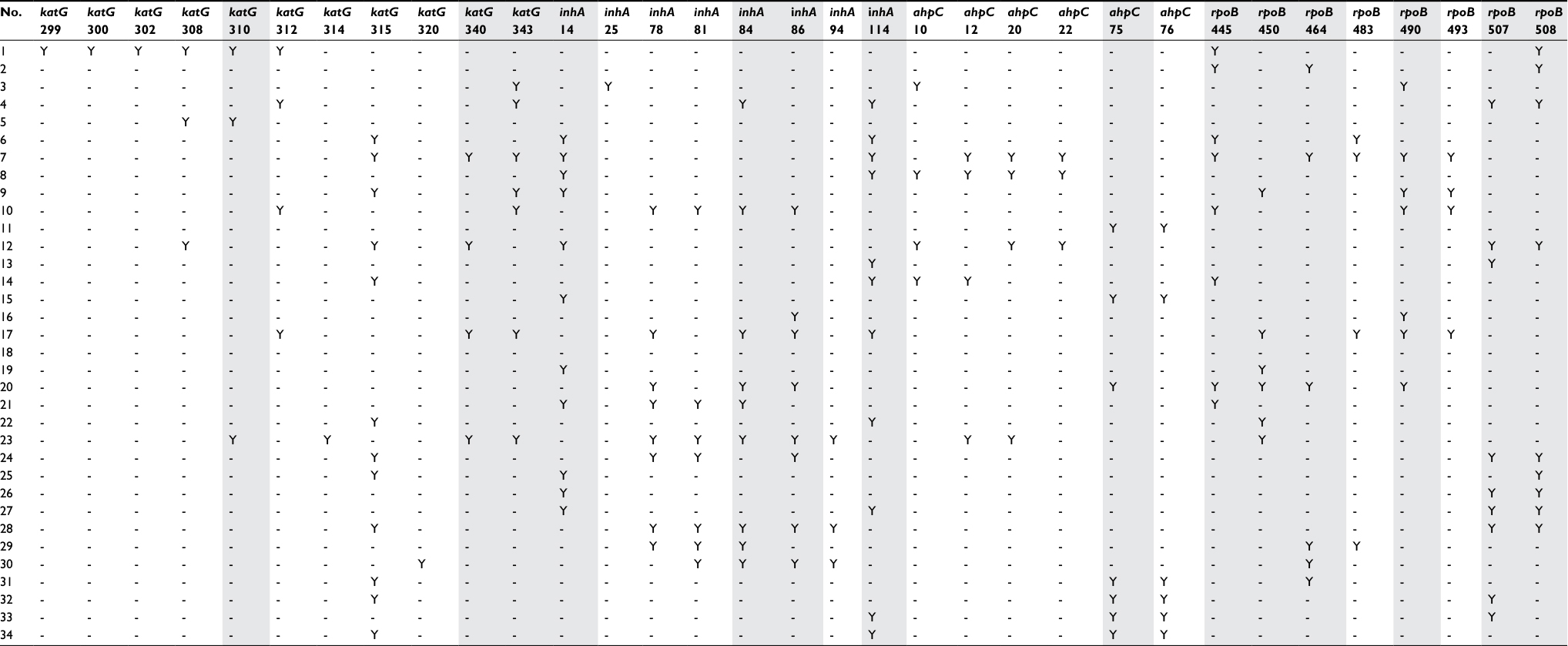 | Table 3 Raw distribution of genetic site mutations of katG, inhA, ahpC, and rpoB genes in M/XDR-TB isolates Notes: -, no mutation; Y, presence of mutation; gray column, proposed mutation test panels. Abbreviation: M/XDR-TB, multidrug/extensively drug-resistant tuberculosis. |
One isolate revealed no mutation for the studied genetic loci (no. 18). Two isolates showed no mutation for katG, inhA, or ahpC. (no. 2 and 18). For the INH-resistant genes, a single-gene mutation was found in 10 isolates (29.4%), 2 for katG, 7 for inhA, and 1 for ahpC. Double mutation was found in 16 isolates (47.1%), 10 for katG/inhA, 4 for ihnA/ahpC, and 2 for katG/ahpC. Triple katG/inhA/ahpC mutation was seen in 6 isolates (17.6%). Regarding the RIF-resistant gene, no rpoB mutation was found in 6 isolates (no. 5, 8, 11, 15, 8, and 34).
The common mutated genetic loci found in M/XDR-TB were katG 315 (n=12, 35.3%), inhA 14 (n=11, 32.4%), ihnA 114 (n=11, 32.4%), ihnA 84 (n=9, 26.5%), rpoB 507 (n=9, 26.47%), and rpoB 508 (n=9, 26.47%).
Discussion
The frequency and distribution of drug-resistant mutations are variable across regions and countries (Table 4). The frequency of katG mutation ranged from 58.5% to 93.7%,39 and the most commonly mutated katG locus was katG 315.32–37,39,40 The reported frequency of inhA mutation was 4.7%–79.4%,32,33 and the most commonly mutated inhA locus was inhA 15.32–40 The frequency of ahpC mutation was relatively low (9.1%–38.2%)34,35 and was extremely variable. The frequency of rpoB mutation was relatively high (80.8%–97.0%),33,34,39 predominantly at the locus rpoB 531.
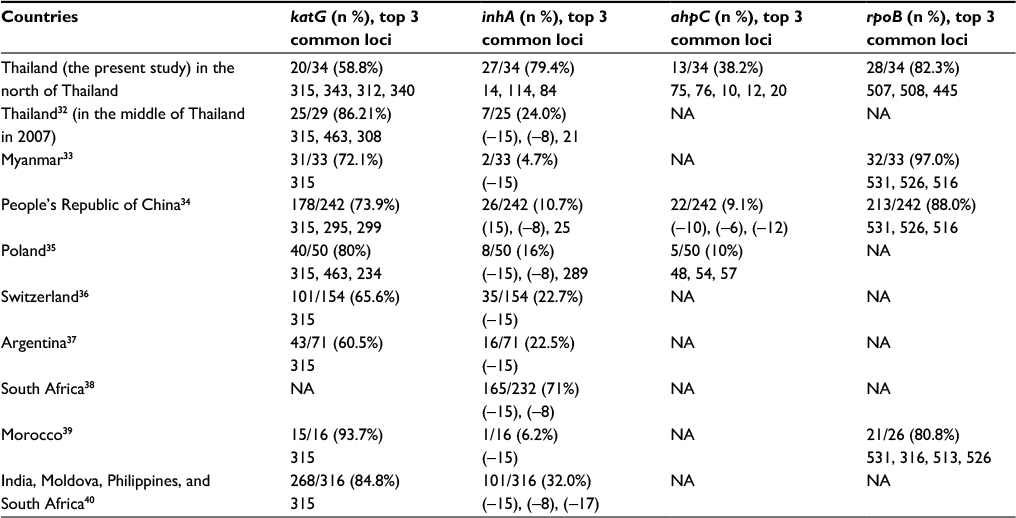 | Table 4 Distribution of genetic mutation for isoniazid and rifampicin resistance Abbreviation: NA, not available. |
Genomic tests or multiple genetic loci tests are not suitable for resource-limited countries. Developing test panels for M/XDR-TB drug-resistant genes would be more cost-effective if the test panels of the selected genetic loci provide high sensitivity and specificity. However, as the distributions of the gene mutations across the regions varied, a deeper analysis should be considered in further studies. The distribution of mutation patterns should be examined in each geographical areas before routine diagnostic services being implemented. According to the results of this study, we selected 8 INH-resistant gene mutation loci (katG 310, katG 340, katG 343, inhA 14, inhA 84, inhA 86, inhA 114, and ahpC 75) and 6 RIF-resistant gene mutation loci (rpoB 445, rpoB 450, rpoB 464, rpoB 490, rpoB 507, and rpoB 508) as the best panels for genetic drug resistance tests. Both the panels were able to detect all isolates with at least 1 mutation site for any katG/inhA/ahpC mutation and rpoB mutation. The sensitivities of the proposed INH resistance mutation test was 94.1% (32/34), while that of the RIF resistance mutation test was 82.4% (28/34).
Limitations
The limitations of this study were the small sample size and the retrospective design. Only 34 isolates were available from a total of 261 isolates. Another weak point was that there was no control group, such as non-M/XDR-TB isolates.
Conclusion
The results of this study confirm the presence of genetic drug-resistant mutations in the M/XDR-TB isolates in upper northern Thailand. We showed that our mutation patterns were different from other parts of Thailand and other countries. The distribution of these mutations in certain populations must be studied before developing specific mutation test panels for each area. These data and proposed mutation panels can be applied for further molecular M/XDR-TB diagnosis in the upper northern region of Thailand.
Acknowledgments
We would like to thank all the staff members in DPC10 as well as Nakornping Hospital, Chiang Rai Hospital, Lampang Hospital, Phayao Hospital, Chiang Kam Hospital, Lamphun Hospital, Phrae Hospital, and Nan Hospital for their cooperation. This study was supported by the National Research Council of Thailand and the Faculty of Medicine, Chiang Mai University, Chiang Mai, Thailand. The study was also partly supported by the Thailand National Research University (NRU) Fund.
Author contributions
All authors contributed toward data analysis, drafting and critically revising the paper and agree to be accountable for all aspects of the work.
Disclosure
All the authors report no conflicts of interest in this work.
References
World Health Organization. Global tuberculosis report 2016. WHO/HTM/TB/2016.13 ed. France: World Health Organization; 2016. | ||
World Health Organization. Companion handbook to the WHO guidelines for the programmatic management of drug-resistant tuberculosis. Geneva, Switzerland: WHO Document Production Services; 2014. | ||
Ahmad S, Mokaddas E. Current status and future trends in the diagnosis and treatment of drug-susceptible and multidrug-resistant tuberculosis. J Infect Public Health. 2014;7(2):75–91. | ||
Liang L, Wu Q, Gao L, et al. Factors contributing to the high prevalence of multidrug-resistant tuberculosis: a study from China. Thorax. 2012; 67(7):632–638. | ||
Lange C, Abubakar I, Alffenaar JW, et al; TBNET. Management of patients with multidrug-resistant/extensively drug-resistant tuberculosis in Europe: a TBNET consensus statement. Eur Respir J. 2014;44(1):23–63. | ||
Porwal C, Kaushik A, Makkar N, et al. Incidence and risk factors for extensively drug-resistant tuberculosis in Delhi region. PLoS One. 2013; 8(2):e55299. | ||
Paramasivan CN, Lee E, Kao K, et al. Experience establishing tuberculosis laboratory capacity in a developing country setting. Int J Tuberc Lung Dis. 2010;14(1):59–64. | ||
Parsons LM, Somoskövi A, Gutierrez C, et al. Laboratory diagnosis of tuberculosis in resource-poor countries: challenges and opportunities. Clin Microbiol Rev. 2011;24(2):314–350. | ||
Boehme CC, Nabeta P, Hillemann D, et al. Rapid molecular detection of tuberculosis and rifampin resistance. N Engl J Med. 2010;363(11):1005–1015. | ||
World Health Organization. Guidelines for the programmatic management of drug-resistant tuberculosis – 2011 update. Version March 2010. Available from: http://apps.who.int/iris/bitstream/10665/44597/1/9789241501583_eng.pdf. Accessed May 17, 2017. | ||
Heysell SK, Houpt ER. The future of molecular diagnostics for drug-resistant tuberculosis. Expert Rev Mol Diagn. 2012;12(4):395–405. | ||
Lin SY, Desmond EP. Molecular diagnosis of tuberculosis and drug resistance. Clin Lab Med. 2014;34(2):297–314. | ||
Chan RC, Hui M, Chan EW, et al. Genetic and phenotypic characterization of drug-resistant Mycobacterium tuberculosis isolates in Hong Kong. J Antimicrob Chemother. 2007;59(5):866–873. | ||
Hofmann-Thiel S, van Ingen J, Feldmann K, et al. Mechanisms of heteroresistance to isoniazid and rifampin of Mycobacterium tuberculosis in Tashkent, Uzbekistan. Eur Respir J. 2009;33(2):368–374. | ||
Ilina EN, Shitikov EA, Ikryannikova LN, et al. Comparative genomic analysis of Mycobacterium tuberculosis drug resistant strains from Russia. PLoS One. 2013;8(2):e56577. | ||
Lopez-Alvarez R, Badillo-Lopez C, Cerna-Cortes JF, et al. First insights into the genetic diversity of Mycobacterium tuberculosis isolates from HIV-infected Mexican patients and mutations causing multidrug resistance. BMC Microbiol. 2010;10:82. | ||
Sherman DR, Mdluli K, Hickey MJ, et al. Compensatory ahpC gene expression in isoniazid-resistant Mycobacterium tuberculosis. Science. 1996;272(5268):1641–1643. | ||
Almeida Da Silva PE, Palomino JC. Molecular basis and mechanisms of drug resistance in Mycobacterium tuberculosis: classical and new drugs. J Antimicrob Chemother. 2011;66(7):1417–1430. | ||
Seifert M, Catanzaro D, Catanzaro A, Rodwell TC. Genetic mutations associated with isoniazid resistance in Mycobacterium tuberculosis: a systematic review. PLoS One. 2015;10(3):e0119628. | ||
Miyata M, Pavan FR, Sato DN, et al. Drug resistance in Mycobacterium tuberculosis clinical isolates from Brazil: phenotypic and genotypic methods. Biomed Pharmacother. 2011;65(6):456–459. | ||
Ameeruddin NU, Luke Elizabeth H. Impact of isoniazid resistance on virulence of global and south Indian clinical isolates of Mycobacterium tuberculosis. Tuberculosis (Edinb). 2014;94(6):557–563. | ||
Banerjee A, Dubnau E, Quemard A, et al. inhA, a gene encoding a target for isoniazid and ethionamide in Mycobacterium tuberculosis. Science. 1994;263(5144):227–230. | ||
Li QJ, Jiao WW, Yin QQ, et al. Compensatory mutations of rifampin resistance are associated with transmission of multidrug-resistant Mycobacterium tuberculosis Beijing genotype strains in China. Antimicrob Agents Chemother. 2016;60(5):2807–2812. | ||
Meftahi N, Namouchi A, Mhenni B, Brandis G, Hughes D, Mardassi H. Evidence for the critical role of a secondary site rpoB mutation in the compensatory evolution and successful transmission of an MDR tuberculosis outbreak strain. J Antimicrob Chemother. 2016;71(2):324–332. | ||
Pavankumar AR, Engström A, Liu J, Herthnek D, Nilsson M. Proficient detection of multi-drug-resistant Mycobacterium tuberculosis by padlock probes and lateral flow nucleic acid biosensors. Anal Chem. 2016;88(8):4277–4284. | ||
Herrera L, Jiménez S, Valverde A, García-Aranda MA, Sáez-Nieto JA. Molecular analysis of rifampicin-resistant Mycobacterium tuberculosis isolated in Spain (1996–2001). Description of new mutations in the rpoB gene and review of the literature. Int J Antimicrob Agents. 2003;21(5):403–408. | ||
Palomino JC, Martin A. Drug resistance mechanisms in Mycobacterium tuberculosis. Antibiotics. 2014;3(3):317–340. | ||
World Health Organization. Guidelines for drug susceptibility testing for second-line anti-tuberculosis drugs for DOTS-plus 2001. Geneva: World Health Organization; 2001. Available from www.WHO_CDS_TB_2001.288_eng.pdf. Accessed May 8, 2017. | ||
Department of Disease Control, Ministry of Public Health, Bangkok, Thailand. [The Thailand’s 2008 National MDR-TB Management Guidelines. Bangkok, Thailand]: The Bureau of Tuberculosis of Thailand; 2001. Thai. | ||
Afanas’ev MV, Ikryannikova LN, Il’ina EN, et al. Molecular characteristics of rifampicin- and isoniazid-resistant Mycobacterium tuberculosis isolates from the Russian Federation. J Antimicrob Chemother. 2007; 59(6):1057–1064. | ||
Valvatne H, Syre H, Kross M, et al. Isoniazid and rifampicin resistance-associated mutations in Mycobacterium tuberculosis isolates from Yangon, Myanmar: implications for rapid molecular testing. J Antimicrob Chemother. 2009;64(4):694–701. | ||
Khadka DK, Eampokalap B, Panitchakorn J, Ramasoota P, Khusmith S. Multiple mutations in katG and inhA identified in Thai isoniazid-resistant Mycobacterium tuberculosis isolates. Southeast Asian J Trop Med Public Health. 2007;38(2):376–382. | ||
Aung WW, Ei PW, Nyunt WW, et al. Phenotypic and genotypic analysis of anti-tuberculosis drug resistance in Mycobacterium tuberculosis isolates in Myanmar. Ann Lab Med. 2015;35(5):494–499. | ||
Luo T, Zhao M, Li X, et al. Selection of mutations to detect multidrug-resistant Mycobacterium tuberculosis strains in Shanghai, China. Antimicrob Agents Chemother. 2010;54(3):1075–1081. | ||
Jagielski T, Bakuła Z, Roeske K, et al. Detection of mutations associated with isoniazid resistance in multidrug-resistant Mycobacterium tuberculosis clinical isolates. J Antimicrob Chemother. 2014;69(9):2369–2375. | ||
Fenner L, Egger M, Bodmer T, et al; Swiss HIV Cohort Study and the Swiss Molecular Epidemiology of Tuberculosis Study Group. Effect of mutation and genetic background on drug resistance in Mycobacterium tuberculosis. Antimicrob Agents Chemother. 2012;56(6):3047–3053. | ||
Imperiale BR, Zumárraga MJ, Di Giulio AB, Cataldi AA, Morcillo NS. Molecular and phenotypic characterisation of Mycobacterium tuberculosis resistant to anti-tuberculosis drugs. Int J Tuberc Lung Dis. 2013; 17(8):1088–1093. | ||
Niehaus AJ, Mlisana K, Gandhi NR, Mathema B, Brust JC. High prevalence of inhA promoter mutations among patients with drug-resistant tuberculosis in KwaZulu-Natal, South Africa. PLoS One. 2015;10(9):e0135003. | ||
Zakham F, Chaoui I, Echchaoui AH, et al. Direct sequencing for rapid detection of multidrug resistant Mycobacterium tuberculosis strains in Morocco. Infect Drug Resist. 2013;6:207–213. | ||
Torres JN, Paul LV, Rodwell TC, et al. Novel katG mutations causing isoniazid resistance in clinical M. tuberculosis isolates. Emerg Microbes Infect. 2015;4(7):e42. |
Supplementary material
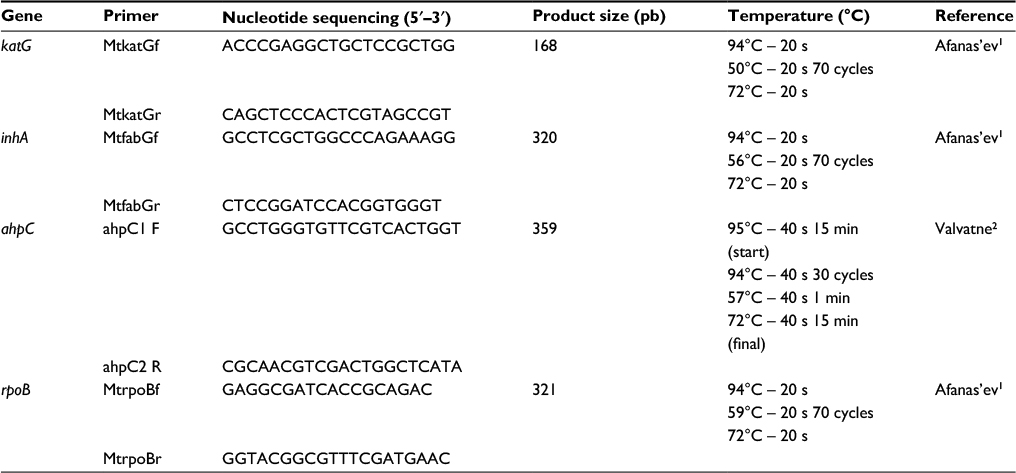 | Table S1 Primers used for sequencing |
References
Afanas’ev MV, Ikryannikova LN, Il’ina EN, et al. Molecular characteristics of rifampicin- and isoniazid-resistant Mycobacterium tuberculosis isolates from the Russian Federation. J Antimicrob Chemother. 2007;59(6):1057–1064. | ||
Valvatne H, Syre H, Kross M, et al. Isoniazid and rifampicin resistance-associated mutations in Mycobacterium tuberculosis isolates from Yangon, Myanmar: implications for rapid molecular testing. J Antimicrob Chemother. 2009;64(4):694–701. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.