")
Back to Journals » Clinical Epidemiology » Volume 12
Genetic Liability to Smoking and Breast Cancer Risk
Received 2 July 2020
Accepted for publication 8 September 2020
Published 20 October 2020 Volume 2020:12 Pages 1145—1148
DOI https://doi.org/10.2147/CLEP.S270509
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Eyal Cohen
Zhouming Xu,1 Hongxia Xu,1 Yunlong Lu2
1Department of Breast Surgery, Huzhou Maternal and Child Health Care Hospital, Huzhou, Zhejiang, 313000, People’s Republic of China; 2Department of Cardiology, The First Affiliated Hospital, School of Medicine, Zhejiang University, Hangzhou, Zhejiang 310003, People’s Republic of China
Correspondence: Yunlong Lu Tel/ Fax +86-571-87236502
Email [email protected]
Keywords: breast cancer, estrogen receptor, Mendelian randomization, smoking
Introduction
Cigarette smoking is a potential modifiable risk factor for breast cancer, which accounts for 30% of female cancer and is the second cause of cancer deaths in 2020.1 However, there are limited studies and inconsistent results on the association between smoking and breast cancer with different estrogen receptor (ER) status.2 In addition, the potential confoundings by alcohol use in observational studies may interfere with relation between smoking and breast cancer.2 Smoking is also genetically correlated with alcohol consumption.3
Mendelian randomization (MR) is a method using genetic variants associated with risk factors to determine the association with a disease.4 In the progress of heredity, the germline genetic variants are randomly assigned to the offspring and remain constant after conception, which means they are not affected by environmental factors and thus, minimizes the influence of bias and reverse causation in the observational epidemiology. Therefore, we carried out a two-sample MR analysis to explore the potential causal relationship of smoking with breast cancer and its subtypes regarding the ER status.
Materials and Methods
Data Source
Publicly available summary statistics were used to conduct the MR analyses. All participants of the original studies had been approved by their appropriate ethics review board and provided informed consent. Summarized data for the association of smoking with breast cancer were derived from the Breast Cancer Association Consortium, including 122,977 breast cancer patients, among whom 69,501 ER-positive cases and 21,468 ER-negative cases, and 105,974 controls of European ancestry.5
We used summary-level data from the Genome-wide Association Study (GWAS) and Sequencing Consortium of Alcohol and Nicotine use on smoking initiation (n=1,232,091 individuals), which identified 378 single nucleotide polymorphisms (SNPs) at a genome-wide significance level (P<5×10−8) across a 1-Mb region, explaining 2.3% of the heritability in smoking (Supplementary Table 1).3 Smoking initiation was defined ever being a regular smoker in the life (current or former). All 378 SNPs were satisfied with our inclusion criteria. We further conducted a sensitivity analysis of the associations between lifetime smoking index and breast cancer. Lifetime smoking index is a continuous measure constructed with smoking status (current, former, never), age at smoking initiation and cessation, cigarettes smoked per day, and smoking duration and time since cessation, which is significantly associated with lung cancer risk.6 The GWAS on lifetime smoking index identified 126 independent SNPs (P<5×10−8) in a linkage disequilibrium r2< 0.001 across a 10-Mb window in up to 462,690 individuals of UK Biobank (Supplementary Table 2).6 All 126 SNPs were available in the breast cancer database. There were only 9 SNPs overlapped between instrument variables related to smoking initiation and lifetime smoking index.
Statistical Analysis
The inverse-variance weighted method was used as standard analysis, supplemented with maximum likelihood, weighted median and MR-Pleiotropy Residual Sum and Outlier methods (a method corrected for horizontal pleiotropy and detect outliers). The result estimate of inverse-variance weighted method was considered credible if there was no directional pleiotropy (P for MR-Egger intercept >0.05). In addition, we conducted the multivariable MR to intervene on effect of alcohol use in smoking-breast cancer risk. A two-sided P-value of 0.05 was set as the threshold for significance.
Results
Genetically predicted smoking initiation was positively associated with overall breast cancer in the inverse-variance weighted analysis, with an odds ratio (OR) of 1.05 (95% confidence interval [CI], 1.01–1.09; P=0.02) per unit increase in log odds of smoking initiation. The maximum likelihood, weighted median and MR-Pleiotropy Residual Sum and Outlier methods yielded similar results (ORs ranged from 1.05 to 1.07, all P<0.05) (Supplementary Table 3). Corresponding analyses for estrogen receptor subtypes revealed significant associations for ER-positive breast cancer risk (OR, 1.05; 95% CI, 1.01–1.10; P=0.03), but not for ER-negative disease (Figure 1).
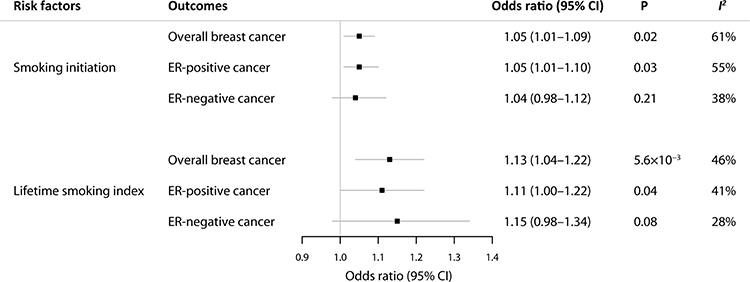 |
Figure 1 Mendelian randomization association of genetically predicted smoking with overall, ER-positive, and ER-negative breast cancer. Smoking initiation was defined ever being a regular smoker in the life (current or former). Lifetime smoking index is a continuous measure constructed with smoking status (current, former, never), age at smoking initiation and cessation, cigarettes smoked per day, and smoking duration and time since cessation, which is significantly associated with lung cancer risk. Odds ratios are scaled to per 2.72-fold (1-unit log-odds) increase in genetically predicted smoking initiation, and per one standard deviation (corresponds to an individual smoking 20 cigarettes a day for 15 years and stopping 17 years ago, or smoking 60 cigarettes a day for 13 years and stopping 22 years ago) increase in the genetically predicted lifetime smoking index. |
The association between smoking and breast cancer was in line with the sensitivity analysis using lifetime smoking index as the exposure. Lifetime smoking increased risk of overall breast cancer and ER-positive breast cancer, but not ER-negative disease (Figure 1) (Supplementary Table 3).There was no evidence of directional pleiotropy (All P>0.05).
To evaluate the effect of alcohol use on smoking-breast cancer risk, we conducted multivariable MR analysis. After adjusting for alcohol use, the lifetime smoking index was still associated with overall breast cancer (OR, 1.17; 95% CI, 1.02–1.34; P=0.02) and ER-positive breast cancer (OR, 1.18; 95% CI, 1.01–1.38; P=0.03), but not with ER-negative breast cancer (Supplementary Table 3). On the contrary, the adjustment of alcohol use weakened the relationship between smoking initiation and breast cancer risk, which may due to the genetic correlation between smoking initiation and alcohol use (rg = 0.34).3
Discussion
This MR analyses demonstrated a significant association of smoking with higher risk of overall and ER-positive breast cancer. Ham et al7 reported that women with family history of cancer were more prone to simultaneously smoke and be exposed to passive smoking (OR, 1.65; 95% CI, 1.17–2.31).
Tobacco smoke contains a lot of carcinogens, including polycyclic aromatic hydrocarbons, aromatic amines, and nitrosamines, which all promote the occurrence of breast cancer. These substances have both estrogen-like and anti-estrogen effects, while in premenopausal women, the anti-estrogen effect form smoking is unable to overcome high endogenous circulating estrogen levels. For its estrogen-like effect, experimental data show that cigarette condensates activate the ER in breast cancer cell.8 Therefore, the causality from smoking to ER-positive breast cancer may be derived from the estrogen-like effect of smoking.
Gaudet et al2 performed a large prospective cohort study including 73,388 women, in which 3721 invasive breast cancer case patients were identified during a follow-up of 13.8 years. Results showed that both current and former smokers increased the risk of ER-positive, but not ER–negative, breast cancer, which was in line with our study.
One of the strengths of this study is the large number of breast cancer cases and their subtypes of European descent only. Second, the biases which potentially exist in conventional observational studies can be reduced. Third, by using two-sample MR analysis, we can broaden the availability of data, and explore the association between smoking and breast cancer avoiding the influence of other diseases. This MR analysis was also subject to some limitations. First, there may be unknown pleiotropy affecting the results. Despite the lack of indication of directional pleiotropy and the consistent results in the complementary analyses, we cannot exclude that the association is mediated through other causal pathways. Second, there is one study (Women’s Health Initiative) included both in the GWAS of smoking initiation and breast cancer, which may affect the MR estimates.
Conclusion
In conclusion, our MR study indicates that genetic liability to smoking increased the risk of overall breast cancer and ER-positive subtype, but not ER-negative breast cancer.
Data Sharing Statement
Summarized data for breast cancer are derived from the Breast Cancer Association Consortium (http://bcac.ccge.medschl.cam.ac.uk/).
Ethics Approval and Consent to Participate
All participants of the original studies included in the original study had provided ethics approval and informed consent.
Acknowledgments
The authors thank the Breast Cancer Association Consortium, for providing GWAS data publicly available.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Siegel RL, Miller KD. Cancer statistics, 2020. CA Cancer J Clin. 2020;70(1):7–30. doi:10.3322/caac.21590
2. Gaudet MM, Gapstur SM, Sun J, et al. Active smoking and breast cancer risk: original cohort data and meta-analysis. J Natl Cancer Inst. 2013;105(8):515–525. doi:10.1093/jnci/djt023
3. Liu M, Jiang Y, Wedow R. Association studies of up to 1.2 million individuals yield new insights into the genetic etiology of tobacco and alcohol use. Nat Genet. 2019;51(2):237–244. doi:10.1038/s41588-018-0307-5
4. Lawlor DA, Harbord RM, Sterne JA, Timpson N, Davey Smith G. Mendelian randomization: using genes as instruments for making causal inferences in epidemiology. Stat Med. 2008;27(8):1133–1163. doi:10.1002/sim.3034
5. Michailidou K, Lindstrom S, Dennis J, et al. Association analysis identifies 65 new breast cancer risk loci. Nature. 2017;551(7678):92–94.
6. Wootton RE, Richmond RC, Stuijfzand BG. et al. Evidence for causal effects of lifetime smoking on risk for depression and schizophrenia: a Mendelian randomisation study. Psychol Med;2019. 1–9. doi:10.1017/S0033291719002678
7. Ham Y, Oh HY, Seo SS, Kim MK. Association between health behaviors and a family history of cancer among Korean women. Cancer Res Treat. 2016;48(2):806–814. doi:10.4143/crt.2015.083
8. Meek MD, Finch GL. Diluted mainstream cigarette smoke condensates activate estrogen receptor and aryl hydrocarbon receptor-mediated gene transcription. Environ Res. 1999;80(1):9–17. doi:10.1006/enrs.1998.3872
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.