")
Back to Journals » Journal of Pain Research » Volume 12
General practitioners and management of chronic noncancer pain: a cross-sectional survey of influences on opioid deprescribing
Authors White R, Hayes C, Boyes AW , Chiu S, Paul CL
Received 20 March 2018
Accepted for publication 24 September 2018
Published 22 January 2019 Volume 2019:12 Pages 467—475
DOI https://doi.org/10.2147/JPR.S168785
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Erica Wegrzyn
Ruth White,1,2 Chris Hayes,1 Allison W Boyes,2,3 Simon Chiu,3 Christine L Paul2,3
1Hunter Integrated Pain Service, Hunter New England Health, Newcastle, NSW, Australia; 2School of Medicine and Public Health, University of Newcastle, NSW, Australia; 3Hunter Medical Research Institute, Newcastle, NSW, Australia
Background: General practitioners’ (GPs) views about deprescribing prescription opioid analgesics (POAs) may influence the care provided for patients experiencing chronic noncancer pain (CNCP). There are limited data addressing GPs’ beliefs about deprescribing, including their decisions to deprescribe different types of POAs.
Aim: To determine the proportion of GPs who hold attitudes congruent with local pain stewardship, describe their deprescribing decisions, and determine whether type of POA influences deprescribing.
Design and setting: In 2016, a cross-sectional survey of all GPs (n=1,570) in one mixed urban and regional primary health network (PHN) in Australia was undertaken.
Methods: A mailed self-report questionnaire assessed agreement with local guidelines for treating CNCP; influences on deprescribing POAs and likelihood of deprescribing in a hypothetical case involving either oral codeine or oxycodone.
Results: A response rate of 46% was achieved. Approximately half (54%) of GPs agreed POAs should be reserved for people with acute, cancer pain or palliative care and a third (32%) did not agree that a medication focus has limited benefits for peoples’ long-term quality of life and function. Most (77%) GPs were less likely to deprescribe when effective alternate treatments were lacking, while various patient factors (eg, fear of weaning) were reported to decrease the likelihood of deprescribing for 25% of GPs. A significantly higher proportion of GPs reported being very likely to deprescribe codeine compared to the equivalent opioid dose of oxycodone for a hypothetical patient.
Conclusions: Many GPs in the PHN hold attitudes at odds with local guidance that opioids are a nonsuperior treatment for CNCP. Attitudinal barriers to deprescribing include: a lack of consistent approach to deprescribing opioids as a class of drugs, perceived lack of effective treatment alternatives and patient fear of deprescribing. Therefore, the next step in this target population is to appropriately train and support GPs in how to apply the evidence in practice and how to support patients appropriately.
Keywords: prescriptions, attitude, general practice, opioid, chronic pain, analgesics
How this fits in
Calls to rethink opioid prescribing for people experiencing chronic noncancer pain (CNCP) have significant implications for general practitioners’ (GPs). This cross-sectional study shows wide variation in GP attitudes with consensus on deprescribing yet to be reached in the pain field. Given that chronic opioid therapy reduces functional recovery, a range of behavior change interventions to modify GP behaviors and support transitioning patients to more effective treatments in order to provide optimal outcomes for patients experiencing CNCP is warranted.
Background
In Australia, between 1990 and 2014 there was an almost fourfold rise in the dispensing of prescription opioid analgesics (POAs). This increase was driven largely by government subsidies for long-acting formulations used to manage pain for people experiencing CNCP, that is, pain lasting longer than 3 months.1–3 Almost 13% of the total Australian population are dispensed at least one government-subsidized POA each year.4
Although there is some evidence worldwide that opioid harms have reached a plateau,5 a substantial rise is evident in Australia in prescription opioid-related harms such as hospitalizations and accidental poisoning deaths.6–8 The available data do not distinguish whether use of illicit opioids or other substances may have contributed, however, the studies do link the rise in harms to an escalation in the use of prescription opioids made available under the government-subsidized system.8 Beyond hospitalization and death, aberrant behavior and dependence are also problematic, particularly when people are younger and on higher prescribed doses.9 Further, there is concern globally when people are coprescribed opioids in combination with benzodiazepines.10,11
Currently, there is evidence that opioids may provide modest short-term (less than 3 months) pain reduction along with minor improvement in physical function when compared with placebo.12,13 Over the longer term the current lack of robust evidence means that, from a clinical ethics perspective, prescribers need to balance a patient-centered approach with population based data that suggest increased harms when opioids are chronically prescribed.14,15
It is now accepted that POAs should not be a first-line treatment for people experiencing CNCP.16 A recent pragmatic randomized controlled trial for chronic back and osteoarthritis-associated pain found that over 12 months treatment the reduction in pain scores was significantly less with opioids than nonopioid treatment. The study found that there were greater adverse events in the opioid arm and opioids brought no improvement in pain interference. Interestingly, the trial also found almost double the use of illicit drugs in the nonopioid arm. Furthermore, it is possible that study outcomes were affected by the limited options for individually titrated dosage in the opioid treatment arm.17
If POAs are initiated in carefully selected patients, that is, those with no substance addiction history, an argument could be made in favor of limiting opioid therapy to a maximum of 3 months as opioid use beyond this time is likely to continue long term.18,19
Across the pain spectrum, widespread clinical variation in opioid prescribing exists.20,21 This variation continues with regard to opioid deprescribing in clinical practice and consensus guidelines. Currently, quality evidence for interventions aiming to reduce prescribed opioids is lacking, though nonrandomized studies indicate that switching to broader treatment approaches, including addressing mental health and physical functioning, may bring about reduction in opioid use.22,23
In practice, consideration of deprescribing after 3 months presents substantial challenges for patients experiencing CNCP and their prescribers.24 Patients may hold concerns regarding opioid withdrawal25 and some prescribers may believe that continuation of POAs poses minimal risk of harm.26 Indeed, targeting early career GPs with teaching of current localized guidelines appears to have had little impact on their actual deprescribing decisions for this patient group.27,28 Currently, although Australian GPs are being urged to consider tapering regimes,29 there is limited evidence about GP perceptions and practices that could be used to guide efforts to improve GPs’ deprescription rates. The available data suggest that GPs regularly face difficulties with patient requests or demands for ongoing opioid treatment.20,30 Further, perceived environmental barriers such as a lack of healthcare providers offering effective treatment alternatives are likely to have an impact on treatment choices.31
In exploring GP perceptions about opioids for CNCP, it is important to consider the various types of opioids available. Low dose codeine (≤30 mg) has consistently been the most widely dispensed formulation in Australia.3,32,33 Codeine is typically classed as a weak opioid or prodrug with its analgesic properties almost entirely attributed to its principal metabolite, morphine.3,34,35 There is risk associated with the drug, however, relating largely to genetic variations which affect the rate at which people convert the prodrug to morphine, plus drug-drug interactions.35,36 This risk was recognized by the Australian Government Therapeutic Goods Administration when legislation passed in Feb 2018 for codeine to be upscheduled from over-the-counter to prescription only.35,37,38 Oxycodone, classed as a strong opioid, is the second most highly dispensed POA in Australia with a substantial portion involving the long-acting formuation.3,4,39 This shift toward a greater reliance on strong and long-acting opioids is relatively recent and has coincided with increased government subsidization.40
It is important to know whether type of POA influences GPs deprescribing decisions, such that peer norms can be shifted via education, training and enablement interventions.41
This study aimed to examine the perceptions and self-reported usual practice regarding POAs among a large urban and regional sample of Australian GPs. Specifically, the study aimed to identify:
- The proportion of GPs who agreed with statements congruent with locally available guidelines27 for CNCP management, ie, POAs should be reserved for people experiencing acute pain, cancer pain, or palliative care; focusing on medication to reduce pain has limited benefits for people’s quality of life and function over the longer term; people who experience CNCP should be screened for depression or anxiety; and addressing sleep problems helps people cope better with their pain.
- The proportion of GPs who report that particular factors (patient prefers to remain on opioids; patient expresses fear of weaning; patient has low score on quality of life measure or functional outcome measure; patient has poor psychological health; lack of availability of effective alternate treatment; lack of availability of access to or support from specialist care) influence their likelihood of deprescribing POAs.
- Whether type of POA influenced GPs’ decision to deprescribe.
Methods
Study design and population
Between February and April 2016 we conducted a cross-sectional survey of GPs in one Australian primary health network (PHN) in the Hunter Central Coast region of NSW. This PHN is the second largest in NSW and 18.3% of the population is aged 65 years and over compared with 14.4% nationally. There are socioeconomically disadvantaged areas within the PHN with 30% of households experiencing rental stress (compared to 25% nationally); 14.4% experience mental and behavioral problems, which is similar to the national average (13.6%).42
Study participants were GPs listed on the PHN register as at February 2016 with correct addresses.
Procedure
We recruited using a multi-step procedure as shown in Figure 1.43 After screening the PHN database for duplicates, remaining GPs were randomized. A further 38 duplicates were detected. A personalized prenotification letter introducing the survey and summarizing current best practice in pain management was sent in February 2016 to all GPs. The PHN produced a newsletter simultaneously with the prenotification mail-out. In March 2016, the first survey (n=1,570) pack was mailed and personally addressed to each individual GP. The pack contained a personalized cover letter, a paper copy of the questionnaire and details of the chance to win an AU$500 value sports watch plus a reply paid envelope. The sender was identified as the University of Newcastle and a respondent-friendly questionnaire design was used.34,44 A professionally designed postcard reminder was mailed to nonresponders 2 weeks after the initial mailing.43,45 A final mail-out of the survey pack was sent to all nonresponders 4 weeks after the prenotification letter. We considered return of the completed survey to imply consent to participate. The University of Newcastle Human Research Ethics Committee approved the study.
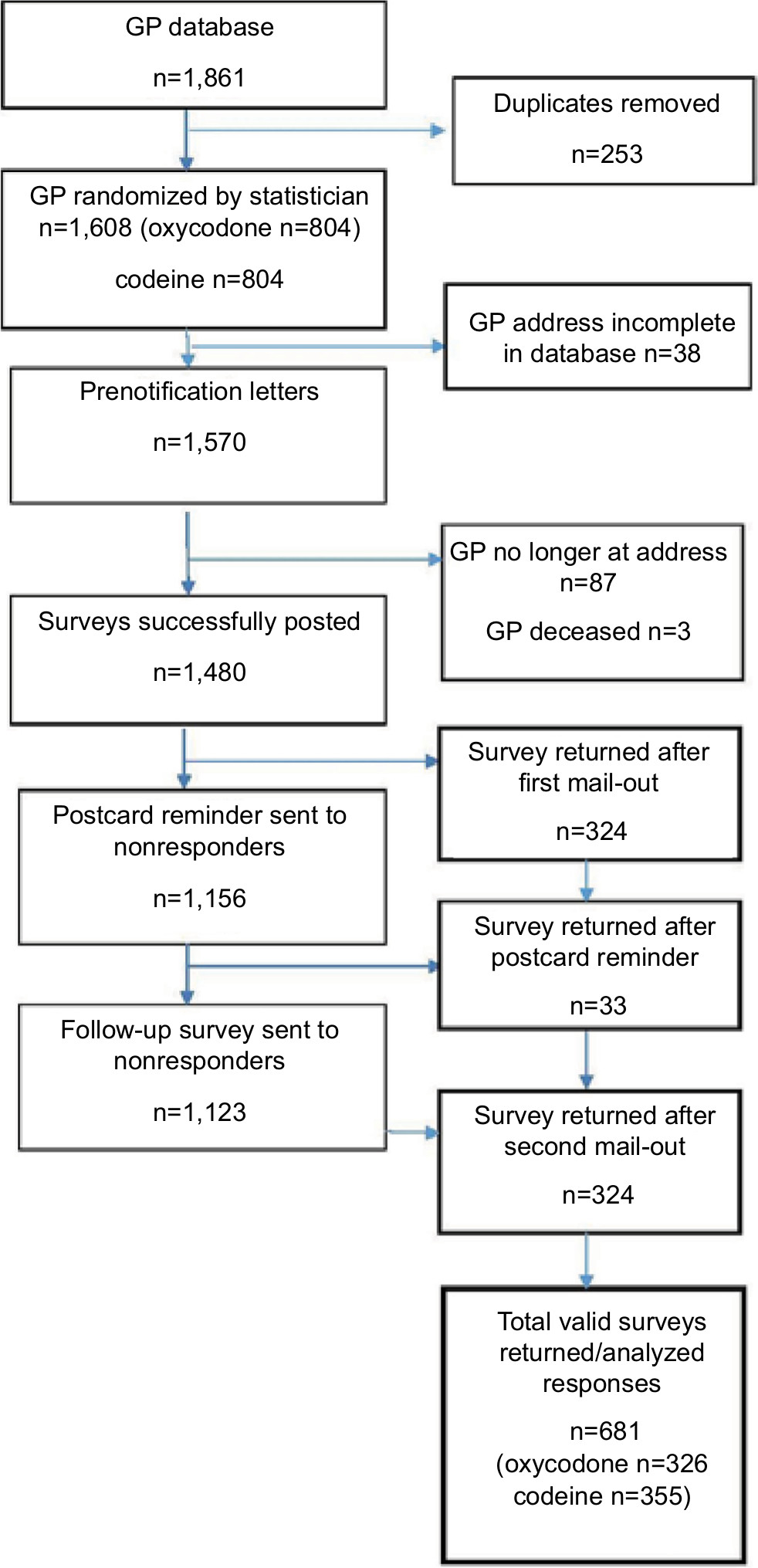 | Figure 1 Survey flowchart. Abbreviation: GP, general practitioner. |
Study measures
A short study-specific questionnaire was developed by the authors and expert clinicians using current best evidence and key elements from locally available guidelines.27 The guidelines were developed in 2014 and promoted via a portal available to local GPs known as HealthPathways46 with links to key messaging videos on YouTube.47 The pool of mutually exclusive attitudinal items described local stewardship in relation to opioid prescribing for CNCP and included four personal attitudes toward CNCP and six attitudinal statements toward deprescribing,27 plus a hypothetical case study. The survey was pilot-tested with three GPs prior to administration to ensure accuracy and face validity with the target group and feasibility of questionnaire completion within 10 minutes. Only the items relevant to the study aims are described here.
GPs medical focus and willingness to prescribe POA was assessed by response to two statements: “opioid therapy should be reserved for people experiencing acute pain, cancer pain, or palliative care” and “focusing on medication to reduce pain has limited benefits for peoples’ quality of life and function over the long-term.”
GPs willingness to screen for underlying mental health comorbidity was assessed by response to two statements: “when caring for people who experience CNCP, screening for depression or anxiety is always important” and “addressing sleep problems help people cope better with their pain experience.”
Five response options for the four personal attitude statements were strongly disagree, disagree, neither agree nor disagree, agree, strongly agree.48 Due to low responses in the “strongly agree” category the responses were collapsed into a three-point Likert scale with, “agree” and “strongly agree” responses aggregated into one category and “strongly disagree” and “disagree” categories were also aggregated. Neither agree nor disagree was maintained for symmetry in the response scale.
Deprescribing attitudes were assessed by response to six attitudinal statements. These statements focused on patient factors (four statements) and health system factors (two statements). Response options for these six statements were in the form of a three-point Likert scale (less likely to initiate wean, no influence on decision, more likely to initiate wean). We then asked respondents to choose which of the following options would encourage them most to deprescribe (lack of therapeutic response, ongoing request for opioids without accepting a broader based approach, other).
Hypothetical patient scenario
Each of the GPs was randomized to receive a case study involving either codeine or immediate release oxycodone of an equivalent oral morphine daily dose of 30 mg. The case study questioned respondents regarding their likelihood to deprescribe opioids to cessation (after 12 months) for a 32-year-old male with the following clinical and psychosocial background: unemployed laborer, chronic shoulder pain, all potentially relevant medical interventions ruled out, attending early for repeat script of opioids, describing his current week as “really tough” eg, medications “taking edge off” only and not reaching his physical or functional treatment goals. Responses were given on a five-point Likert scale (very unlikely, unlikely, neither likely nor unlikely, likely, and very likely).
Sample size
A priori power analysis was conducted to determine a sufficient sample size for the study. It was calculated that a total sample size of 500 GPs was required to estimate proportions with a margin of error of 4% and maintain a type I error rate of 5% and a type II error rate of 20% (80% power)
Statistical analysis
Data were entered and analyzed using STATA Version 14. A sample of 30 surveys was randomly selected to check data quality. There were four errors detected from 720 questions representing a 0.6% data entry error rate (three skipped entry and one incorrect entry) which is below the benchmark of 1%.
We used descriptive statistics (frequencies and percentages with 95% CI) to report the attitudes of the GPs. Chi-squared test was used to compare the observed and expected number of responses to the case study and the type of opioid used in the case study.
Ethics approval
This study received ethics approval from Hunter New England Health and University of Newcastle Human Research Ethics Committees. HNEHREC reference no: 15/10/21/5.01 NSW HREC Reference No: LNR/15/HNE/371 SSA reference no: LNRSSA/15/HNE/372.
Results
Sample
Of 1,570 questionnaires that were mailed, 1,480 were delivered successfully and 681 were returned completed. There were 90 undeliverable surveys, 87 were due to the GP no longer working at, or having retired from, the practice with three returned due to the GP being deceased. The total valid adjusted response rate was thus 46%. No significant gender differences between responders and nonresponders were found.
Of those that responded, 57% were male and 58% had graduated prior to 1995. The majority of the responders’ practices had practice nurses (92%) and worked in practices with between five and ten full-time equivalent GPs (44 %). Half of the GPs indicated that 5%–10% of their casework involved CNCP and only 3% indicated they had never referred a patient to a tertiary pain service.
Local CNCP pain stewardship
Proportions are reported for each item (Table 1). Approximately half (54%) of GPs agreed POAs should be reserved for people with acute pain, cancer pain or needing palliative care as per local guidelines. Approximately one third (32%) did not agree that a medication focus has limited benefits for peoples’ long-term quality of life and function.
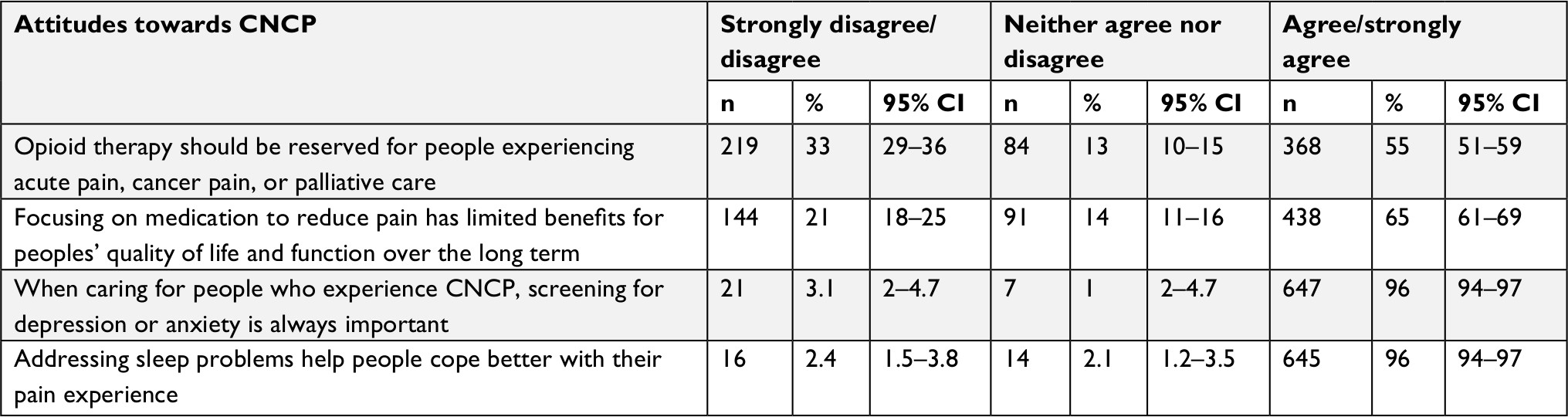 | Table 1 GPs’ agreement with managing patients experiencing CNCP (n=681) Notes: Totals may not add to 681 (or 100%) due to missing data. Abbreviations: CNCP, chronic noncancer pain; GPs, general practitioners. |
Deprescribing decisions
Table 2 describes the reported likelihood of GPs deprescribing opioids for patients with CNCP under various circumstances. More than three quarters (77%) of GPs reported that a lack of effective alternate treatment would make them less likely to initiate a weaning regime. Over one third of GPs would be more likely to deprescribe if the patient had poor psychological health. An ongoing request for opioids was the biggest factor influencing GPs decision to wean the patient off opioids (44%), followed by a lack of therapeutic response 40% (data not shown).
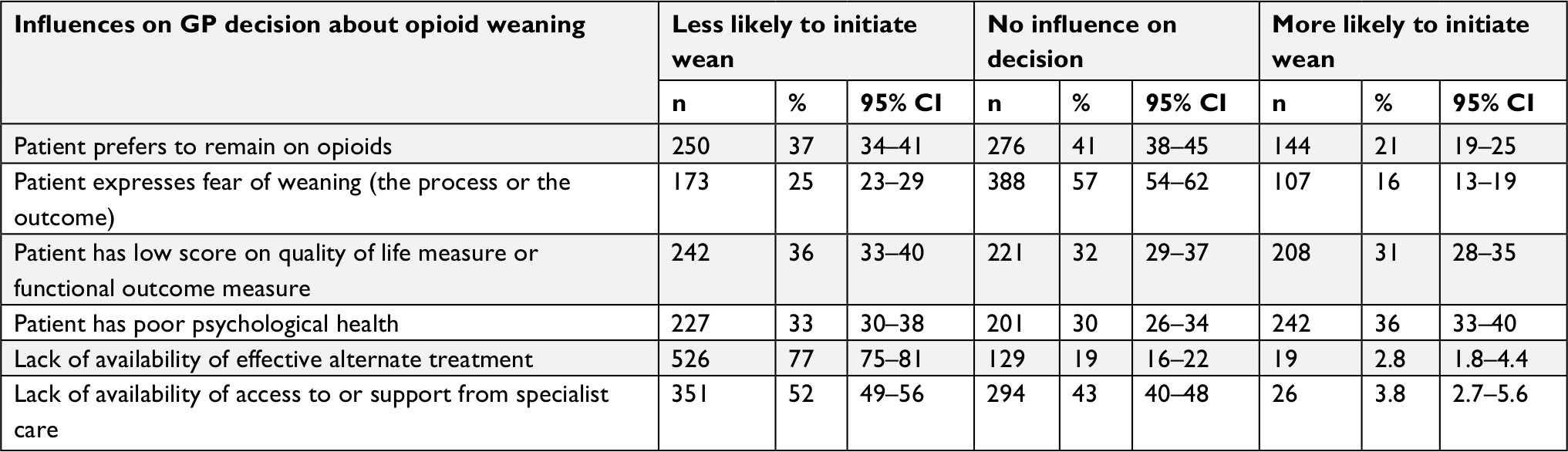 | Table 2 Reported likelihood to deprescribe opioid dose to cessation in relation to various patient and resource factors (n=681) Notes: Totals may not add to 681 (or 100%) due to missing data. |
Opioid type
As shown in Figure 2, there was a significant difference in GPs responses between case studies received (chi-square=17.87, df=4, P=0.001). A higher proportion of GPs who received the codeine case study indicated they were “very likely” to wean the patient off opioids (31%) compared to GPs who received a case study involving oxycodone (18%).
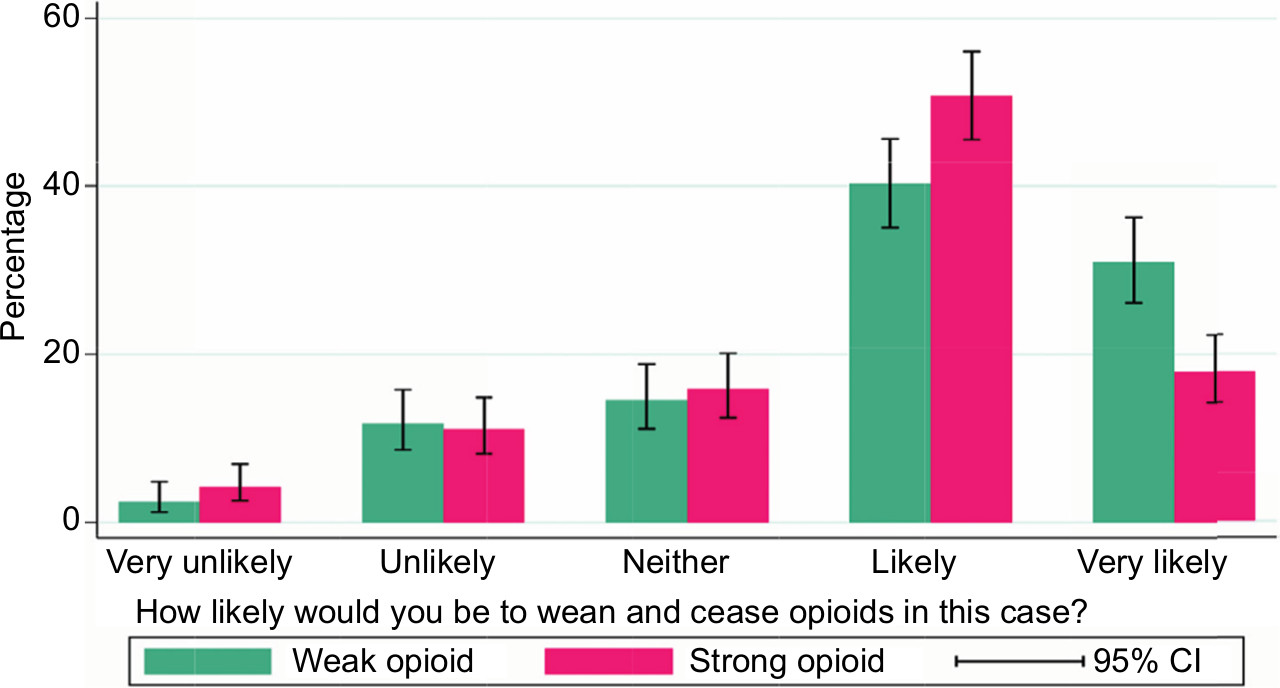 | Figure 2 Oxycodone (strong) versus codeine (weak). |
Discussion
Summary of main findings
Australian GPs have been tasked with initiating opioid deprescribing for patients experiencing CNCP after 3 months, avoiding the creation of a future generation of long-term opioid users. We found that only half the GPs surveyed endorsed the idea of reserving opioid use for acute and cancer pain; and a third did not agree that a medication focus had limited benefits.27,28 Our findings are consistent with those from overseas showing that prescribers’ attitudes and prescribing habits vary widely.49 This wide clinical variation in the pain field relates in part at least to provider factors.50 Further education, training and enablement for providers may assist GPs to restructure their practice and modify their prescribing behaviors in line with local guidance, thereby reducing variations in clinical care.41,51,52
There was strong agreement with the idea of promoting quality sleep and screening for depression. The wider literature is clear on the value of addressing sleep problems.53 Although the link between POAs and depression is well supported,54,55 the specific risk associated with codeine prescriptions has only recently been highlighted.56 In contrast, a recent trial in the UK has cast doubt on the usefulness of screening for depression and anxiety, at least in patients presenting to their GP with osteoarthritis.57 It is possible that screening, in the context of more holistic care is effective, this is an area to be explored.
This study showed that patient preference to stay on opioids or patient fear of the process or outcome of weaning impacts heavily on the GPs’ decision to deprescribe. With Australian data suggesting that two out of three people attempting suicide have chronic pain, this risk may contribute further to a reluctance to deprescribe.58 Current evidence suggests guiding suicidal patients toward nonaddictive alternatives and linking patients with mental health support59 to reduce risk and attain clinical improvement.59,60
Our data showed that GPs’ attitudes vary widely on whether low quality of life measures or poor psychological health influence their decisions to initiate weaning. Practitioners have been urged to examine effects on psychosocial functioning of the select group of patients remaining on long-term opioids.61 While opioid deprescribing may seem logical when patients have poor function and unremitting pain, a rise in aberrant behavior and misuse while tapering is a complex area with little current guidance available.62 We did not explore whether GPs had different attitudes for an older patient requiring “comfort care” compared to a younger person with potential for functional recovery and return to work, though this may have been a factor.63
Arguably, the biggest barrier identified to initiating deprescribing was a perceived lack of effective alternate treatment. While tertiary specialist pain centers are capable of delivering high-quality psychosocial pain care, GPs clearly want access to more accessible evidence based options in primary care.51 Conversely, we showed that a patient actively requesting more opioids was a key factor influencing the GPs’ decision to initiate deprescribing. This may reflect that GPs are aware of guidance to routinely screen for signs of aberrant behavior and are more confident in deprescribing in this patient cohort.27,64
Australian GPs continue to prescribe multiple types of POAs in primary care settings.65 Our data suggest that the majority of GPs favored cessation of opioids in a hypothetical case. While this is good news, management of a hypothetical case does not necessarily correlate with deprescribing in actual practice.66
Study limitations
The response rate to our survey, while low, compares favorably to other surveys of primary care practitioners.67,68 The sample size may result in reduced precision in the study data. Study findings may not be generalizable to nonGP prescribers or GPs in more rural and remote areas.69
Respondents may differ from nonrespondents (response bias) such that GPs more interested in pain management may be more likely to return the survey questionnaire than other GPs. Response bias may result in the data providing a more favorable picture of GPs’ perceptions and practices than is actually the case. While such testing is rare for this type of survey, it is possible that survey responses may not provide a precise estimate of participants’ true views. However, given the dearth of evidence available on this topic and the lack of a strong alternative methodology for obtaining this information the data gathered represent a significant advance on what is currently available for the purposes of service planning and delivery. We did not examine the attitudes of GPs regarding substance use disorder, where the attitudes of GPs toward initiation of deprescribing are less ambiguous.70 Finally, we did not examine the influence of patient characteristics or satisfaction levels on prescribing patterns.71,72
Implications for clinical practice and future research
GPs in the surveyed region have been widely encouraged to deprescribe POAs whenever a patient is encountered who has been taking POAs for longer than 3 months.24 The results of this survey suggest that a large proportion of GPs are not following the evidence base about POAs and locally promoted opioid stewardship.73 This finding lends weight to the view that this complex problem would be better managed from a coordinated regulatory and broad societal perspective.74,75
One option to counter decades of often-misleading pharmaceutical company marketing promotion could be a strong education campaign similar to the Victorian (Australia) back pain campaign in the late 1990s.76 Such a population-based campaign would target both patients and providers and promote key messages around the harms and lack of efficacy of long-term opioid use.
Conclusion
In the short term, however, it is our view that there is a clear need to train and support GPs by assisting them to shift toward potentially more effective psychological or behavioral treatments for patients experiencing CNCP. Competent and compassionate GPs who have learnt to view less liberal opioid prescribing as the new norm will benefit from ready access to viable alternatives in order to confidently proceed with the transition to broader treatments. Training GPs in how to support patients who express fear of the deprescribing process is also likely to be an important element of effective training programs.
Acknowledgments
The authors thank the Hunter New England PHN who supported the survey, GPs who returned the survey, and Sandra Dowley for data management. RW is supported by funding from the Ann Taylor Scholarship. CLP is supported by an NHMRC Career Development Fellowship. AB is supported by Early Career Fellowships from the National Health and Medical Research Council (APP1073317) and Cancer Institute New South Wales (13/ECF/1-37). These funding bodies had no role in determining the study design; in the collection, analysis, and interpretation of data; in the writing of the report; and in the decision to submit the article for publication.
Disclosure
The authors report no conflicts of interest in this work.
References
Merskey H., Bogduk N, editors. Classification of Chronic Pain. Descriptions of Chronic Pain Syndromes and Definitions of Pain Terms. 2nd ed. Seattle, WA: IASP Press; 1994. | ||
International Association for the Study of Pain Subcommittee on Taxonomy. International Association for the Study of Pain. Classification of chronic pain. Descriptions of chronic pain syndromes and definitions of pain terms. Merskey H, editor. Pain. 1986;Suppl 3:S1–S225. | ||
Karanges EA, Blanch B, Buckley NA, Pearson SA. Twenty-five years of prescription opioid use in Australia: a whole-of-population analysis using pharmaceutical claims. Br J Clin Pharmacol. 2016;82(1):255–267. | ||
Gisev N, Pearson SA, Blanch B, et al. Initiation of strong prescription opioids in Australia: cohort characteristics and factors associated with the type of opioid initiated. Br J Clin Pharmacol. 2016;82(4):1123–1133. | ||
Dart RC, Surratt HL, Cicero TJ, et al. Trends in opioid analgesic abuse and mortality in the United States. N Engl J Med. 2015;372(3):241–248. | ||
Karanges EA, Buckley NA, Pearson SA. The rise and rise of prescription opioid use in Australia. Med Today. 2017;(Suppl 2):2–7. | ||
Miller GC, Valenti L, Britt H, Bayram C. Drugs causing adverse events in patients aged 45 or older: a randomised survey of Australian general practice patients. BMJ Open. 2013;3(10):e003701. | ||
Blanch B, Pearson SA, Haber PS. An overview of the patterns of prescription opioid use, costs and related harms in Australia. Br J Clin Pharmacol. 2014;78(5):1159–1166. | ||
Campbell G, Nielsen S, Larance B, et al. Pharmaceutical opioid use and dependence among people living with chronic pain: associations observed within the pain and opioids in treatment (POINT) cohort. Pain Med. 2015;16(9):1745–1758. | ||
Hawkins EJ, Malte CA, Hagedorn HJ, et al. Survey of primary care and mental health prescribers’ perspectives on reducing opioid and benzodiazepine co-prescribing among veterans. Pain Med. 2017;18(3):454–467. | ||
Degenhardt L, Blanch B, Gisev N, Larance B, Pearson S. The POPPY Research programme protocol: investigating opioid utilisation, costs and patterns of extramedical use in Australia. BMJ Open. 2015;4:e007030. | ||
Meske DS, Lawal OD, Elder H, Langberg V, Paillard F, Katz N. Efficacy of opioids versus placebo in chronic pain: a systematic review and meta-analysis of enriched enrollment randomized withdrawal trials. 2018;11:923–934. | ||
Chaparro LE, Furlan AD, Deshpande A, Mailis-Gagnon A, Atlas S, Turk DC. Opioids compared to placebo or other treatments for chronic low back pain: an update of the Cochrane Review. Spine. 2014;39(7):556–563. | ||
Cohen MJ, Jangro WC. A clinical ethics approach to opioid treatment of chronic noncancer pain. AMA J Ethics. 2015;17(6):521–529. | ||
Martin BC, Fan MY, Edlund MJ, Devries A, Braden JB, Sullivan MD. Long-term chronic opioid therapy discontinuation rates from the TROUP study. J Gen Intern Med. 2011;26(12):1450–1457. | ||
Chou R, Turner JA, Devine EB, et al. The effectiveness and risks of long-term opioid therapy for chronic pain: a systematic review for a National Institutes of Health Pathways to Prevention Workshop. Ann Intern Med. 2015;162(4):276–286. | ||
Krebs EE, Gravely A, Nugent S, et al. Effect of Opioid vs nonopioid medications on pain-related function in patients with chronic back pain or hip or knee osteoarthritis pain: The SPACE Randomized Clinical Trial. JAMA. 2018;319(9):872–882. | ||
Edlund MJ, Steffick D, Hudson T, Harris KM, Sullivan M. Risk factors for clinically recognized opioid abuse and dependence among veterans using opioids for chronic non-cancer pain. Pain. 2007;129(3):355–362. | ||
Von Korff M, Korff MV, Saunders K, et al. De facto long-term opioid therapy for noncancer pain. Clin J Pain. 2008;24(6):521–527. | ||
Eid AI, Depesa C, Nordestgaard AT, et al. Variation of opioid prescribing patterns among patients undergoing similar surgery on the same acute care surgery service of the same institution: time for standardization? Surgery. 2018;164(5):926–930. | ||
Australian Commission on Safety and Quality in Health Care and National Health Performance Authority. Australian Atlas of Healthcare Variation. Sydney: ACSQHC; 2015. | ||
Eccleston C, Fisher E, Thomas KH, et al. Interventions for the reduction of prescribed opioid use in chronic non-cancer pain. Cochrane Database Syst Rev. 2017;11:CD010323. | ||
Demirkol A. Tapering off opioid analgesia. Med Today. 2017;Suppl 2:14–16. | ||
Hayes C. Chronic noncancer pain. The challenge of implementing opioid guidelines. Pain Manag Today. 2017;4(2):27–30. | ||
Kiepek N, Hancock L, Toppozini D, Cromarty H, Morgan A, Kelly L. Facilitating medical withdrawal from opiates in rural Ontario. Rural Remote Health. 2012;12:1–9. | ||
Hutchinson K, Moreland AM, de C Williams AC, Weinman J, Horne R. Exploring beliefs and practice of opioid prescribing for persistent non-cancer pain by general practitioners. Eur J Pain. 2007;11(1):93–98. | ||
Hunter Integrated Pain Service. Reconsidering opioid therapy. A Hunter New England Perspective; May 2014. Available from: http://www.hnehealth.nsw.gov.au/Pain/Documents/Reconsidering_opioid_therapy_May%202014.pdf. Accessed December 20, 2018. | ||
Holliday SM, Hayes C, Dunlop AJ, et al. Does brief chronic pain management education change opioid prescribing rates? A pragmatic trial in Australian early-career general practitioners. Pain. 2017;158(2):278–288. | ||
Demirkol A. Tapering off opioid analgesia. Med Today. 2017;1(Supp 2):14–16. | ||
Le CD, Medicine G, Banks E. Deprescribing. Aust Prescr. 2011;34(6):4–7. | ||
Casey DE. Why don’t physicians (and patients) consistently follow clinical practice guidelines? JAMA Intern Med. 2013;173(17):1581–1583. | ||
Rogers KD, Kemp A, McLachlan AJ, Blyth F. Adverse selection? A multi-dimensional profile of people dispensed opioid analgesics for persistent non-cancer pain. PLoS One. 2013;8(12):e80095. | ||
Harrison CM, Charles J, Henderson J, Britt H. Opioid prescribing in Australian general practice. Med J Aust. 2012;196(6):380–381. | ||
Roxburgh A, Hall WD, Burns L, et al. Trends and characteristics of accidental and intentional codeine overdose deaths in Australia. Med J Aust. 2015;203(7):299. | ||
MacDonald N, MacLeod SM. Has the time come to phase out codeine? CMAJ. 2010;182(17):1825. | ||
Iedema J. Cautions with codeine. Aust Prescr. 2011;34(5):133–135. | ||
Nielsen S, Tobin C, Dobbin M. OTC codeine: examining the evidence for and against. Aust Pharm. 2012:236–240. | ||
Australian Government. Prescription strong (Schedule 8) opioid use and misuse in Australia – options for a regulatory response; Consultation paper. Version 1.0, January 2018. Available from: https://www.tga.gov.au/sites/default/files/consultation-prescription-strong-schedule-8-opiod-use-misuse-in-australia-options-for-regulatory-response.pdf. Accessed December 7, 2018. | ||
Degenhardt L, Gisev N, Cama E, Nielsen S, Larance B, Bruno R. The extent and correlates of community-based pharmaceutical opioid utilisation in Australia. Pharmacoepidemiol Drug Saf. 2016;25(5):521–538. | ||
Hollingworth SA, Symons M, Khatun M, et al. Prescribing databases can be used to monitor trends in opioid analgesic prescribing in Australia. Aust N Z J Public Health. 2013;37(2):132–138. | ||
Chauhan BF, Jeyaraman M, Mann AS, et al. Behavior change interventions and policies influencing primary healthcare professionals’ practice-an overview of reviews. Implement Sci. 2017;12(1):3. | ||
Hunter New England Central Coast PHN. Health Planning Compass. Heal Plan Perform Portf. 2016:1–36. Available from: http://www.hneccphn.com.au/media/14230/compass-jun-16-final-002.pdf. Accessed August 13, 2017. | ||
Edwards PJ, Roberts I, Clarke MJ, et al. Methods to increase response to postal and electronic questionnaires. Cochrane Database Syst Rev. 2009;18(3):MR000008. | ||
Glidewell L, Thomas R, Maclennan G, et al. Do incentives, reminders or reduced burden improve healthcare professional response rates in postal questionnaires? Two randomised controlled trials. BMC Health Serv Res. 2012;12:250. | ||
Hunter Integrated Pain Service. Understanding pain: what to do about it in less than five minutes? YouTube. 2011. Available from: https://www.youtube.com/watch?v=5KrUL8tOaQs. Accessed December 7, 2018. | ||
NSW Government. Community HealthPathways; Hunter New England. Available from: hne.healthpathways.org.au. Accessed October 15, 2017. | ||
White R, Hayes C, White S, Hodson FJ. Using social media to challenge unwarranted clinical variation in the treatment of chronic noncancer pain: the “Brainman” story. J Pain Res. 2016;9:701–709. | ||
HIPS. Hunter Integrated Pain Service (HIPS) Website; 2013. Available from: http://www.hnehealth.nsw.gov.au/pain. Accessed December 7, 2018. | ||
Wightman RS, Nelson LS. Opioid prescribing: how well do we know ourselves? J Med Toxicol. 2016;12(3):221–223. | ||
Duggan A, Koff E, Marshall V. Clinical variation: why it matters. Med J Aust. 2016;205(10):3–4. | ||
Slater H, Davies SJ, Parsons R, Quintner JL, Schug SA. A policy-into-practice intervention to increase the uptake of evidence-based management of low back pain in primary care: a prospective cohort study. PLoS One. 2012;7(5):e38037:1–13. | ||
Windmill J, Fisher E, Eccleston C, et al. Interventions for the reduction of prescribed opioid use in chronic non-cancer pain. Cochrane Database Syst Rev. 2013;9:CD010323. | ||
Wilt JA, Davin S, Scheman J. A multilevel path model analysis of the relations between sleep, pain, and pain catastrophizing in chronic pain rehabilitation patients. Scand J. Pain. 2016;2016(10):122–129. | ||
Kroenke K. A practical and evidence-based approach to common symptoms: a narrative review. Ann Intern Med. 2014;161(8):579–586. | ||
Parchman ML, Von Korff M, Baldwin LM, et al. Primary care clinic re-design for prescription opioid management. J Am Board Fam Med. 2017;30(1):44–51. | ||
Scherrer JF, Salas J, Bucholz KK, et al. New depression diagnosis following prescription of codeine, hydrocodone or oxycodone. Pharmacoepidemiol Drug Saf. 2016;25(5):560–568. | ||
Mallen CD, Nicholl BI, Lewis M, et al. The effects of implementing a point-of-care electronic template to prompt routine anxiety and depression screening in patients consulting for osteoarthritis (the Primary Care Osteoarthritis Trial): a cluster randomised trial in primary care. PLoS Med. 2017;14(4):e1002273-23. | ||
Campbell G, Darke S, Bruno R, Degenhardt L. The prevalence and correlates of chronic pain and suicidality in a nationally representative sample. Aust N Z J Psychiatry. 2015;49(9):803–811. | ||
Berna C, Kulich RJ, Rathmell JP. Tapering long-term opioid therapy in chronic noncancer pain: evidence and recommendations for everyday practice. Mayo Clin Proc. 2015;90(6):828–842. | ||
Elman I, Borsook D, Volkow ND. Pain and suicidality: insights from reward and addiction neuroscience. Prog Neurobiol. 2013;109:1–27. | ||
Janke EA, Cheatle M, Keefe FJ, Dhingra L; Society of Behavioral Medicine Health Policy Committee. Society of Behavioral Medicine (SBM) position statement: improving access to psychosocial care for individuals with persistent pain: supporting the National Pain Strategy’s call for interdisciplinary pain care. Transl Behav Med. 2018;8(2):305–308. | ||
Manhapra A, Arias AJ, Ballantyne JC. The conundrum of opioid tapering in long-term opioid therapy for chronic pain: a commentary. Subst Abus. 2017;22(1):1–10. | ||
Ballantyne JC. Opioids for the treatment of chronic pain: mistakes made, lessons learned, and future directions. Anesth Analg. 2017;125(5):1769–1778. | ||
Holliday S, Hayes C, Dunlop A. Opioid use in chronic non-cancer pain-part 2: prescribing issues and alternatives. Aust Fam Physician. 2013;42(3):104–111. | ||
Roxburgh A, Hall WD, Dobbins T, et al. Trends in heroin and pharmaceutical opioid overdose deaths in Australia. Drug Alcohol Depend. 2017;179:291–298. | ||
Holliday SM, Hayes C, Dunlop AJ, et al. Does brief chronic pain management education change opioid prescribing rates? A pragmatic trial in Australian early-career general practitioners. Pain. 2017;158(2):278–288. | ||
Cohen MM, Penman S, Pirotta M, Da Costa C. The integration of complementary therapies in Australian general practice: results of a national survey. J Altern Complement Med. 2005;11(6):995–1004. | ||
Parkinson A, Jorm L, Douglas KA, et al. Recruiting general practitioners for surveys: reflections on the difficulties and some lessons learned. Aust J Prim Health. 2015;21(2):254–258. | ||
Briggs AM, Slater H, Bunzli S, et al. Consumers’ experiences of back pain in rural Western Australia: access to information and services, and self-management behaviours. BMC Health Serv Res. 2012;12(1):357. | ||
Lovejoy TI, Morasco BJ, Demidenko MI, Meath TH, Frank JW, Dobscha SK. Reasons for discontinuation of long-term opioid therapy in patients with and without substance use disorders. Pain. 2017;158(3):526–534. | ||
Foy R, Leaman B, McCrorie C, et al. Prescribed opioids in primary care: cross-sectional and longitudinal analyses of influence of patient and practice characteristics. BMJ Open. 2016;6(5):e010276–e010276. | ||
Onishi E, Kobayashi T, Dexter E, Marino M, Maeno T, Deyo RA. Comparison of opioid prescribing patterns in the United States and Japan:primary care physicians’ attitudes and perceptions. J Am Board Fam Med. 2017;30(2):248–254. | ||
Mccracken LM, Boichat C, Eccleston C. Training for general practitioners in opioid prescribing for chronic pain based on practice guidelines: a randomized pilot and feasibility trial. J Pain. 2012;13(1):32–40. | ||
Dasgupta N, Beletsky L, Ciccarone D. Opioid crisis: no easy fix to its social and economic determinants. Am J Public Health. 2018;108(2):182–186. | ||
Larance B, Degenhardt L, Peacock A, et al. Pharmaceutical opioid use and harm in Australia: the need for proactive and preventative responses. Drug Alcohol Rev. 2018;37(Suppl 1):S203–S205. | ||
Buchbinder R, Jolley D, Wyatt M. 2001 Volvo Award Winner in Clinical Studies: Effects of a media campaign on back pain beliefs and its potential influence on management of low back pain in general practice. Spine. 2001;26(23):2535–2542. |
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.