")
Back to Journals » Risk Management and Healthcare Policy » Volume 15
Gender Differences in the Attitudes and Management of People with Obesity in Saudi Arabia: Data from the ACTION-IO Study
Authors Almubark RA , Alqahtani S , Isnani AC , Alqarni A , Shams M , Yahia M, Alfadda AA
Received 9 November 2021
Accepted for publication 11 May 2022
Published 3 June 2022 Volume 2022:15 Pages 1179—1188
DOI https://doi.org/10.2147/RMHP.S346206
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Kent Rondeau
Rasha A Almubark,1 Saleh Alqahtani,2,3 Arthur C Isnani,4 Ali Alqarni,5 Mahmoud Shams,6 Moataz Yahia,6 Assim A Alfadda4,7,8
1Sharik Association for Health Research, Riyadh, Saudi Arabia; 2Liver Transplant Unit, King Faisal Specialist Hospital & Research Center, Riyadh, Saudi Arabia; 3Division of Gastroenterology and Hepatology, Johns Hopkins University, Baltimore, MD, USA; 4Obesity Research Center, College of Medicine, King Saud University, Riyadh, Saudi Arabia; 5King Abdulaziz Hospital and King Abdullah International Medical Research Center, Ministry of National Guard Health Affairs, Ahsa, Eastern Region, Saudi Arabia; 6Novo Nordisk, Riyadh, Saudi Arabia; 7Department of Medicine, College of Medicine, King Saud University, Riyadh, Saudi Arabia; 8Obesity, Endocrine, and Metabolism Center, King Fahad Medical City, Riyadh, Saudi Arabia
Correspondence: Assim A Alfadda, Obesity Research Center, College of Medicine, King Saud University, Riyadh, Saudi Arabia, Tel + 966 11 4671315, Email [email protected]
Purpose: Several studies have investigated gender differences in various obesity-related outcomes. Females were found to have more accurate weight perception and reported more frequency of attempted weight loss. The objective of this study was to assess gender differences in the attitudes and management of people with obesity (PwO) in Saudi Arabia using data from the ACTION-IO study.
Patients and Methods: A survey was conducted in Saudi Arabia in June and July 2018 on adults with obesity (based on self-reported body mass index of ≥ 30 kg/m2).
Results: A total of 1000 people with obesity completed the survey; 565 (56.5%) were male (mean age of 36.9 years and mean BMI of 33.5 kg/m2) and 435 (43.5%) were female (mean age of 36.3 years and mean BMI of 34.5 kg/m2). The two most reported motivations for wanting to lose weight for both groups were to improve appearance (38%) and to have more energy (35%). Females were more likely to trust their health-care provider (HCP) advice about weight management when compared to males (87% females, 82% males, p = 0.059) and were more likely to have concerns regarding long-term safety associated with prescription weight loss medications (65% female versus 59% males, p = 0.043). On the other hand, males were more likely to seek their physician to prescribe weight loss medication if they hear of a new medication (55% males versus 46% females, p = 0.014), and more to believe that there are good options available for weight loss medications (74% males versus 67% females, p = 0.040). Also, more males prefer to take weight loss medications than to have a weight loss surgery (65% males, 59% females, p = 0.054).
Conclusion: Overall, this study increases our understanding on the attitudes of both females and males towards the management of weight loss and opens the discussion for gender-specific weight loss interventions.
Keywords: obesity, gender, management, Saudi Arabia, ACTION-IO
Introduction
Obesity is a chronic, complex, relapsing disease and a growing concern in terms of public health due to the increased risk of morbidity and mortality.1,2 Obesity increases the risk of non-communicable diseases such as type 2 diabetes, metabolic syndrome, hypertension, dyslipidemia, coronary heart disease, and certain types of cancer and has recently been associated with worse outcomes in COVID-19.3–6 Obesity is associated with multiple factors, not only genetic but physiological factors, psychological issues, and environmental variables, both physical and social, affecting individuals of all ages and regions.7
High prevalence rates for obesity and overweight are seen in Saudi Arabia due to the increasing westernization over the last few decades, leading to unhealthy eating, sedentary lifestyles, and weight gain.8,9 According to the World Health Organization (WHO), in the Kingdom of Saudi Arabia (KSA), the overall prevalence of obesity is estimated to be 33.7% and of overweight is 68.2%.10 As of 2014, 66–75% of adults and 25–40% of children in the Arab region were either overweight or obese.11 The prevalence of obesity in Saudi population has remained high, indicating that preventive measures are lacking or are inefficient.10
People with obesity (PwO) face a decrease in health-related quality of life and experience social discrimination, negatively impacting their emotional and mental well-being.12 The increased direct and indirect health-care costs associated to obesity poses a significant burden on PwO.13 Although evidence-based policy guidelines are available for the treatment of PwO,14 the low rates of obesity diagnosis, documentation and management, associated with inadequate knowledge of obesity treatment guidelines, reflect the insufficient implementation of these recommendations.15–17 Therefore, suboptimal care is usually provided to PwO.
Additionally, studies have shown that health-care professionals (HCPs) demonstrate knowledge gaps for obesity guidelines and lack the understanding of obesity medication efficacy, safety, and overall management.18 The multi-component lifestyle interventions, behavioral interventions (intensive behavioral therapy), pharmacotherapy, and bariatric surgery are all strategies that support clinically significant weight loss for PwO. However, the application of these evidence-based treatments is uncommon.19,20
Communication barriers between PwO and HCPs have been documented.7 The discomfort of HCPs for initiating the conversation with fear of offending the patients, associated with negative attitudes and beliefs found among HCPs might adversely impact the effectiveness and management of weight loss in PwO.7 Furthermore, weight misperception is associated with fewer weight loss attempts in overweight and obese adults.21
Gender differences in the body image and weight perception have drawn attention in many research studies because of the possible consequent physical and psychological problems that may ensue. Male PwO are less likely to have accurate weight perception and, therefore, less likely to have weight dissatisfaction, attempted weight loss, and successful weight loss compared with females.2,22,23 Distorted perception of body image were found to be more prevalent among middle-aged men.24 Among men, distorted body weight perception was found to be correlated with age (middle-age), income, perceived health status and health behaviors. In contrast to men, women who have distorted body weight perception were mostly psychological in nature.24 Studies have shown the relationship between perceived weight and the intention to lose weight, and may be different across gender with women more likely to attempt weight loss than men.25,26 A study showed that men were more likely to attempt weight loss, exercise more, eat less fat compared to women who prefer to take prescription pills and follow specific diets for weight loss.2 Although individuals who are overweight or PwO have the desire to lose weight, many of them experience weight-related stigma causing psychological distress.27 Apart from this, the Canadian national cross-sectional study found out that weight-related discrimination exists in the health-care system, emphasizing the need to reform and reduce weight-related social stigma for PwO.28
To improve the quality and access to obesity care globally, it is necessary to better understand the disease itself and the way PwO should be managed. Gender-specific interventions can be addressed with proper understanding on female and male attitudes towards management of weight loss. We conducted this study to assess gender differences in the attitudes and management of People with Obesity (PwO) in Saudi Arabia using data from the ACTION-IO study.
Materials and Methods
This study is part of the Awareness, Care and Treatment In Obesity MaNagement-International Observation (ACTION-IO) collaborative study, a cross-sectional observational study designed to identify the perceptions, attitudes, behaviors, and potential barriers to effective obesity management which surveyed over 14,500 PwOs and nearly 2800 HCPs from 11 countries. The ACTION-IO results have been previously published and have identified several gaps between obesity care and a misalignment between the perceptions and attitudes of PwO and HCPs.15,29 However, there are no gender-specific conclusions on weight loss management based on these studies.
Recruitment
All respondents included in this study were recruited via email and/or telephone through an online panel company with which respondents have provided permission to be contacted for research purposes. Outbound samples were sent according to pre-determined demographic targets based on age, gender, household income, education, and area, to minimize any sampling bias. PwO were eligible if they were ≥18 years, with a body mass index (BMI) of ≥30 kg/m2 based on self-reported height and weight. Targets were monitored throughout data collection to ensure representativeness.
Data Collection
This data is part of the ACTION-IO study, in which an online survey was sent to PwO in Saudi Arabia with an average survey length of around 30 minutes. The questionnaires used for this study were developed by an international steering committee of obesity experts, including three medical doctors employed by Novo Nordisk, the study sponsor, and a representative from Saudi Arabia. Questionnaire items were phrased and presented in the same order for each respondent. PwO were offered in both English and Arabic, and pre-tests (n = 8) were conducted to confirm language and understanding (n = 4).
The questionnaire was conducted by a third-party vendor (KJT Group [Honeoye Falls, NY, USA]), who also managed data collection and analysis of de-identified data. The data collection period was from June 4th, 2018, until July 25th, 2018. Ethical approval was approved by the independent review board at King Fahad Medical City, Riyadh, Saudi Arabia (IRB number H-01-R-012). The survey was conducted by a third-party vendor (KJT Group [Honeoye Falls, NY, USA]), who also managed data collection and analysis of de-identified data. We obtained the participants’ consent through ticked checkbox, which indicated consent together with the survey questionnaire. The study conformed to the accepted scientific principles, conducted by qualified and trained persons and safeguard subjects’ integrity and privacy according to the Declaration of Helsinki. A total of 2669 surveys were sent, and 1518 (57%) responded. However, a total of 1031 (68%) surveys were qualified. After that, 1000 (66%) participants completed the survey.
Inclusion Criteria
Respondent had to be 18 years old or above, male or female, living in Saudi Arabia, and having a current BMI of 30 kg/m2 or greater. Respondents were not participating in intense fitness or bodybuilding programs and, if females, not currently pregnant.
Data Validity
Extreme outliers were removed subjectively from mean values where appropriate, based on reported findings’ data distribution implications. Three data validation questions were included in each survey, with clear and obvious responses to identify respondents entering fraudulent data. The survey and dataset omitted respondents who failed to provide the correct answer to 2 or more of these questions.
Data Analysis
Statistical analysis was carried out using the Statistical Program for Social Sciences (SPSS) version 23.0 (SPSS Inc., Armonk, New York, USA). Frequency distribution was reported as numbers and percentages for categorical data. Continuous data were expressed as mean and standard deviation with their corresponding range of values. All reported statistics are weighted accordingly with the exception of demographic data which are reported unweighted as a means to characterize the raw sample data. The final, incoming PwO sample, including those failing to qualify for the survey, was weighted to representative demographic targets for age, gender, household income, education and region, based on data from the 2011 International Standard Classification of Education and the US Census Bureau, International Data Base and other public data. Weights were calculated using a raking technique (also known as iterative proportional fitting or sample-balancing) to achieve the nearest possible sample and target balance. The ranking algorithm adjusted the individual respondent values so the total sample (all respondents) matched the known demographic targets; the weights were repeatedly estimated across each set of variables until the optimal weights that most closely balanced the sample demographic distributions with the target distributions were established. Individual respondents’ weights were capped at 0.5 and 5.00 to avoid extreme design effects (which could result in greater sample variance and larger confidence intervals) and to avoid markedly under- or over-representing any single respondent. Weighting of the sample to resemble demographic characteristics of the general population enables inferences to be made to the entire population, not just the sample. A test of significance between categorical variables was done using the Chi-square test. P-value of <0.05 was considered statistically significant.
Results
Characteristics of PwO Respondents
A total of 1000 PwO completed the survey: 565 (56.5%) were male and 435 (43.5%) were female. Surveys were distributed in the Central, West, North, South and East regions of the KSA, the majority of participants had less than secondary education, most were married (Supplementary Table). There were significant differences between male and female in that the average body BMI was higher for female (p < 0.001), and with a higher proportion of female respondents in Class II and III obesity. Female respondents presented a significantly higher number of comorbidities when compared to males (4.59 ± 1.6 females, 2.60 ± 2.3 males, p < 0.001). Figure 1 shows a detailed proportion of comorbid conditions among male and female respondents. On average, both females and males had a similar number of weight loss attempts (3.4 ± 2.6 females, 3.4 ± 2.9 males, p = 0.966). However, although not statistically significant, males regained the weight after keeping it off (69.0% males versus 66.7%females, p = 0.484) (Table 1).
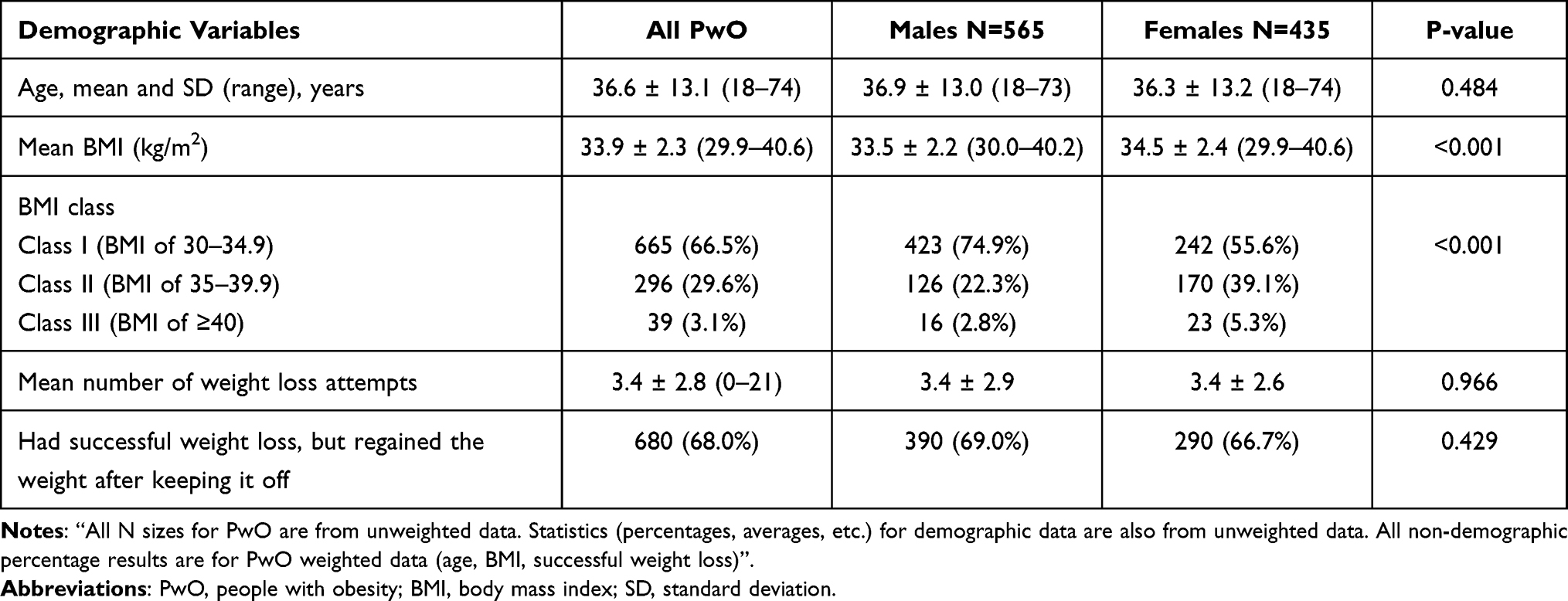 |
Table 1 Baseline Characteristics of PwO Respondents |
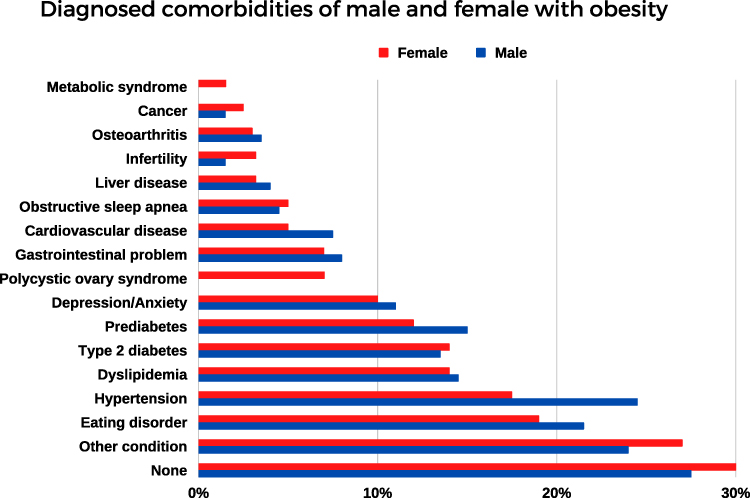 |
Figure 1 Diagnosed comorbidities of males (N = 565) and females (N = 435) with obesity. |
Weight Management and Attitudes Towards the HCP
When asked about prescription medications for weight loss, a majority (71%) of overall respondents agree that there are good options today for prescription weight loss medications and that they prefer to take a prescription medication than to have a surgery to lose weight (63%). Most said that they are concerned about the long-term safety (61%) of such medications (Figure 2). Most also said that they would rather lose weight than depending on medication (58%).
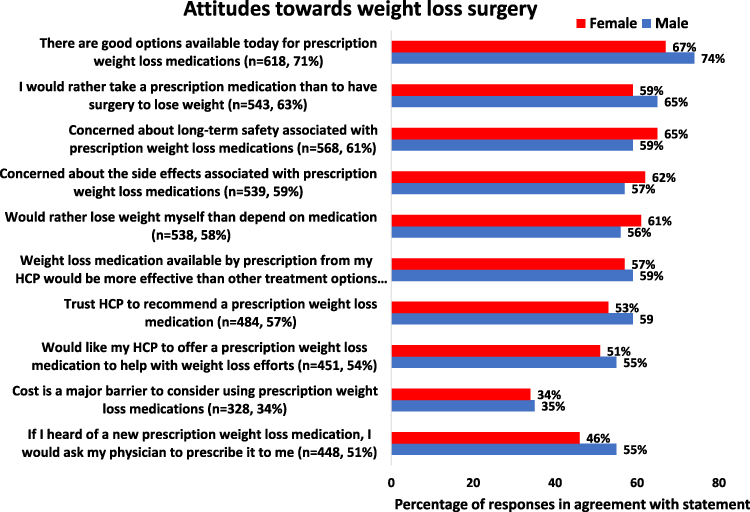 |
Figure 2 Female and male attitudes towards weight management. This figure shows the percentage of females and male respondents agreeing with statements following the question: “Please indicate how much you agree with the following regarding prescription medications for weight loss.” Females = red; males = blue. For each statement, the number of respondents (n) and percentage (%) are indicated, a total of respondents = 1000. |
When comparing gender differences, a significant difference was observed with more males intending to seek their physician to prescribe weight loss medication, if they hear of a new medication (55% males versus 46% females, p = 0.014), and more to believe that there are good options available for weight loss medications when compared to females (74% males versus 67% females, p = 0.040) but females are more concerned about the long-term safety associated with prescription weight loss medication than males (65% female versus 59% males, p = 0.043) (Figure 2).
Various differences were found between males and females in their relationship with the HCP (Figure 3). Females are more likely to trust HCPs advice about weight management (87% females, 82% males, p = 0.059) and believe that their HCPs listen carefully to what they have to say (86% females, 81% males, p = 0.128). They are also more likely to follow HCP advice about weight management (81% females, 77% males, p = 0.198). More females believe that their HCPs understands the difficulties of weight management (86% females, 83% males, p = 0.322) and feel comfortable talking to their HCPs about their weight (83% females, 82% males, p = 0.612). On the other hand, more males than females reported that it is important for them that their HCP is at a healthy weight (82% males, 81% females, p = 0.687).
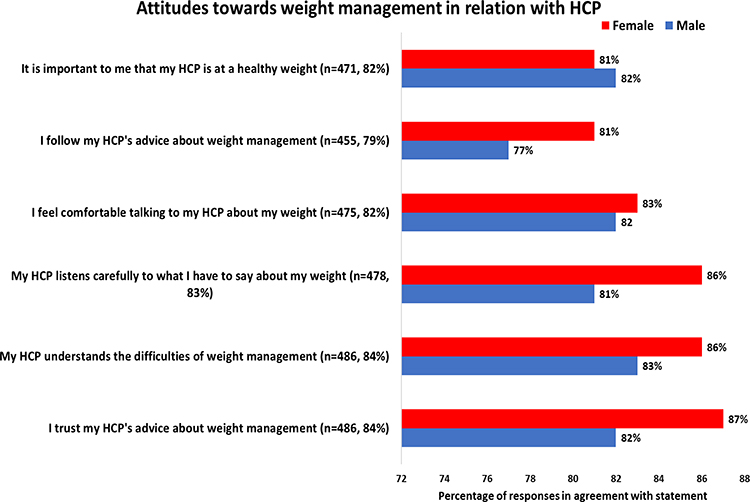 |
Figure 3 Female and male attitudes towards weight management in relation with the HCP. Females = red; males = blue. For each statement the number of respondents (n) and percentage (%) are indicated, total of respondents = 1000. |
Weight Loss Surgery
Overall, most PwO said they have concerns about the safety of weight loss surgery (80%), and they would rather lose weight through diet and exercise (78%) (Figure 4). They believe that surgery is the “easy way out” (76%) and that having surgery represents having a permanent change in lifestyle (73%). Sixty-three percent of the respondents believe there are good options available today for weight loss surgery.
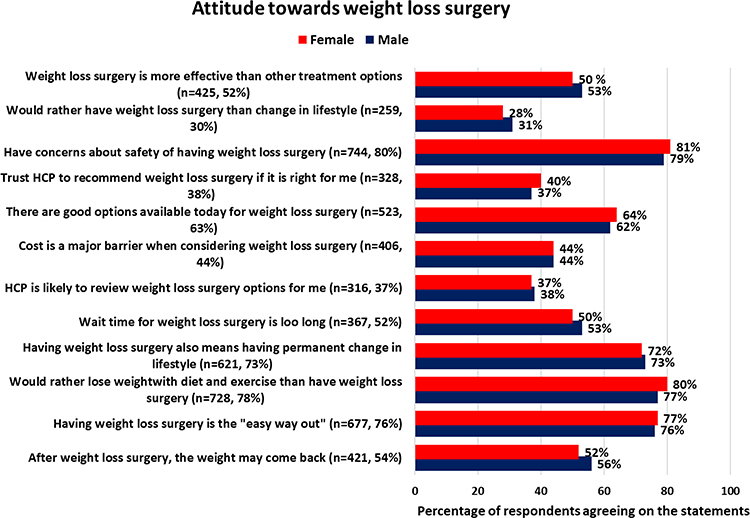 |
Figure 4 Female and male attitudes regarding weight loss surgery. This figure shows the percentage of females and males’ respondents agreeing with statements following the question: “Please indicate how much you agree with the following regarding weight loss surgery” Females = red; males = blue. For each statement, the number of respondents (n) and percentage (%) are indicated, a total of respondents = 1000. |
No significant differences were found between males and females regarding weight loss surgery (Figure 4). However, more females than males trust their HCP to recommend weight loss surgery if they are a good fit (40% females, 37% males, p = 0.358), and they are more likely to have concerns about the safety of weight loss surgery compared to males (81% females, 79% males, p = 0.315). Females prefer to lose weight with diet and exercise than having weight loss surgery (80% females, 77% males, p = 0.225). Nevertheless, they are less to believe that weight may come back after weight loss surgery (52% females, 56% males, p = 0.224).
Goals to Achieve as Part of Weight Management
When asked about the most important goals to personally achieve as part of the weight management, overall, the main reasons stated by PwO for wanting to lose weight were: to improve appearance (38%), to have more energy (35%), to feel more confident/less judged by other people (30%), to live a longer live (28%), to stay active with their family (28%), and to reduce the risks associated with excess weight/prevent a health condition (27%) (Figure 5).
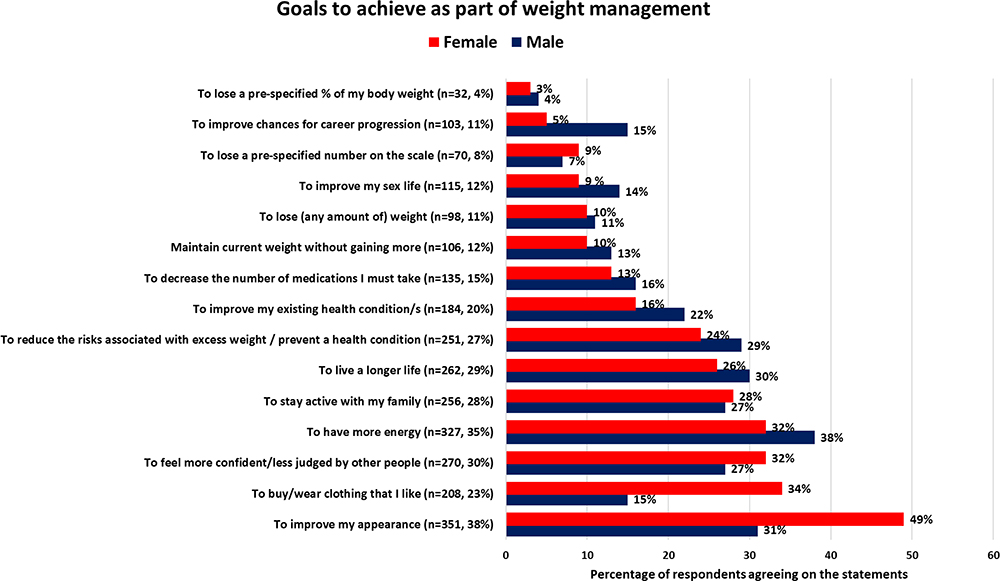 |
Figure 5 Goals and motivations concerning weight and health. This figure shows the percentage of females and males respondents in agreement with statements following the question: “Now, we would like to understand your overall goals concerning your weight and health. Please select the top 3 most important goals for you to personally achieve as part of your weight management, if any”. Females = red; males = blue. For each statement, the number of respondents (n) and percentage (%) are indicated, a total of respondents = 1000. |
Significant differences were observed in some goals and motivations of males and females PwO for losing weight (Figure 5). Males believe that losing weight improves chances of career progression (15% males, 5% females, p < 0.001), improves their existing health condition(s) (22% males, 16% females, p = 0.027), and improves their sex lives (14% males, 9% females, p = 0.023). On the other hand, females are more concerned with their appearance (49% females, 31% males, p < 0.001) and believe that weight loss enables them to buy and wear clothing that they like (34% females, 15% males, p < 0.001).
Discussion
The prevalence of overweight and obesity in the Saudi population is increasing, indicating ineffectiveness or lack of preventive measures.30 Comorbidities associated with obesity are considered a major health and economic problem that requires fast action. ACTION IO is an international study that tried to understand the perceptions, attitudes and behaviors of PwO and HCPs and to identify potential barriers to effective obesity care. Data from countries that participated in ACTION IO are important in understanding patients’ perspectives about obesity in these countries and how this can be used to plan an effective strategy toward obesity management. The main data from ACTION IO in Saudi Arabia has been published recently. Here, we reported the gender differences in the attitudes and management of obesity from the perspective of PwO. To our knowledge, this is the first study to report on these differences in Saudi Arabia.
We found that BMI was higher for females. That is consistent with other studies conducted in Saudi Arabia, which showed that the prevalence of obesity and higher BMI is superior among women compared to men, particularly after 40 years of age.30–32 Physical inactivity level represents a burden on the health of young Saudi females. It might explain the higher prevalence of obesity and BMI in adult Saudi females when compared to males.22,31,33 Most participants in this study had less than secondary education and were married, factors which already have been shown to be significant predictors of high BMI.32,34,35
There were some differences in terms of motivations for weight loss. These are unsurprising and were documented before, but the primary motivators were the same for both groups.23 Regarding weight loss surgery, we found no significant differences between men and women. However, in attitudes toward weight management, there was a clear difference in that males are more likely to ask their physician to prescribe a weight-loss medication, in case they hear of a new prescription weight loss medication, and they are more likely to believe that there are good options available for weight loss medication. In addition, more males than females prefer to take a prescription medication than to have a weight-loss surgery. On the other hand, females are more likely to trust their HCP’s advice about weight management and to voice concerns about medication safety. These novel findings highlight several needs that are important to consider among HCPs. Being aware of these differences in gender HCPs can mediate the conversation about weight management. The relation between trust and gender has been previously studied. Women are less likely to lose trust and more likely to restore trust when compared to men.36 Trust dynamics are different between women and men, with women caring more about maintaining trustful relationships than men.36,37 With this in mind, there should be strategies targeted at making men more likely to trust and listen to their HCP regarding their weight. Also, HCPs should use the time they are being heard to and paid attention to by their female patients to address weight-loss medicine safety issues and weight loss counseling concerns.
Previous studies assessing weight bias from patients have shown that physicians’ excess weight may negatively affect patients’ perceptions of their credibility, level of trust, and inclination to follow medical advice.36,37 Our results showed, although not statistically significant, that more males than females reported that it is important for them that their HCP is at a healthy weight. Moreover, males believe that losing weight improves chances of career progression and their existing health condition(s). On the other hand, females are more concerned with their appearance and believe that weight loss enables them to feel more confident and less judged by others.
We found some differences between our results and those of the global ACTION-IO study regarding motivations and goals for weight loss in PwO in general.29 The most common answer (46%) of global respondents was to reduce the risks associated with excess weight/prevent a health condition, whereas only 27.1% of Saudis mentioned that reason. These results highlight a need for Saudi HCPs to discuss the risks associated with obesity and overweight with their patients.
This study has limitations similar to those found in the global ACTION-IO study,29 including its cross‐sectional and descriptive nature, reliance on self‐reported height and weight, which could underestimate BMI, and respondent recall bias.
Conclusion
There exists a gender difference in the perception of PwO with regard to weight management and their attitude towards weight loss. Data show that many PwO are interested in weight loss however, the motivations for weight loss among females are geared towards a more conservative approach (diet and exercise), whereas male PwO tend to go for surgery and weight loss medications. Understanding the attitudes towards weight management between gender is essential for proper weight counseling and weight management in PwO. We reported differences between genders in comfort with weight discussions, motivations, and preferences for medical management of obesity. This data can be used to tailor weight management discussions to enhance obesity care in Saudi Arabia.
Acknowledgments
The authors would like to thank Alexandra Sanfins PhD, and Ana Rolo PhD, for medical writing support in editing the manuscript. This study was sponsored by Novo Nordisk.
Disclosure
AA Alfadda reports financial support from Novo Nordisk to attend an obesity conference during the conduct of the study, and personal (consultancy) fees and non-financial support from Novo Nordisk outside the submitted work. M Shams and M Yahia are employees of Novo Nordisk. RA Almubark, S Alqahtani, AC Isnani, and Ali Alqarni have no conflicts of interest in this work.
References
1. Lim SS, Vos T, Flaxman AD, et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380(9859):2224–2260. doi:10.1016/S0140-6736(12)61766-8
2. Tsai SA, Lv N, Xiao L, Ma J. Gender differences in weight-related attitudes and behaviors among overweight and obese adults in the United States. Am J Men Health. 2016;10(5):389–398. doi:10.1177/1557988314567223
3. Afshin A, Forouzanfar MH, Reitsma MB, et al. Health effects of overweight and obesity in 195 countries over 25 years. N Engl J Med. 2017;377(1):13–27.
4. Kassir R. Risk of COVID‐19 for patients with obesity. Obes Rev. 2020;21(6):e13034. doi:10.1111/obr.13034
5. Garg S, Kim L, Whitaker M, et al. Hospitalization rates and characteristics of patients hospitalized with laboratory-confirmed coronavirus disease 2019 — COVID-NET, 14 States, March 1 –30, 2020. MMWR Morb Mortal Wkly Rep. 2020;69(15):458–464. doi:10.15585/mmwr.mm6915e3
6. Hajifathalian K, Kumar S, Newberry C, et al. Obesity is associated with worse outcomes in COVID-19: analysis of early data from New York City. Obesity. 2020;28(9):1606–1612. doi:10.1002/oby.22923
7. Leiter LA, Astrup A, Andrews RC, et al. Identification of educational needs in the management of overweight and obesity: results of an international survey of attitudes and practice. Clin Obes. 2015;5(5):245–255. doi:10.1111/cob.12109
8. Alqarni M. A review of prevalence of obesity in Saudi Arabia. J Obes Eat Disord. 2016;2(2):1–6. doi:10.21767/2471-8203.100025
9. DeNicola E, Aburizaiza OS, Siddique A, et al. Obesity and public health in the Kingdom of Saudi Arabia. Rev Environ Health. 2015;30(3):191–205. doi:10.1515/reveh-2015-0008
10. World Health Organization. World health organization diabetes country profiles. Saudi Arabia; 2016. Available from https://www.who.int/diabetes/country-profiles/sau_en.pdf.
11. Rahim HF, Sibai A, Khader Y, et al. Non-communicable diseases in the Arab world. Lancet. 2014;383(9914):356–367. doi:10.1016/S0140-6736(13)62383-1
12. Sikorski C, Luppa M, Kaiser M, et al. The stigma of obesity in the general public and its implications for public health - A systematic review. BMC Public Health. 2011;11(1):1–8. doi:10.1186/1471-2458-11-661
13. Kjellberg J, Tange Larsen A, Ibsen R, Højgaard B. The socioeconomic burden of obesity. Obes Facts. 2017;10(5):493–502. doi:10.1159/000480404
14. Alfadda AA, Al-Dhwayan MM, Alharbi AA, et al. The Saudi clinical practice guideline for the management of overweight and obesity in adults. Saudi Med J. 2016;37(10):1151–1162. doi:10.15537/smj.2016.10.14353
15. Sbraccia P, Busetto L, Santini F, et al. Misperceptions and barriers to obesity management: Italian data from the ACTION-IO study. Eat Weight Disord. 2021;26(3):817–828. doi:10.1007/s40519-020-00907-6
16. Bocquier A, Verger P, Basdevant A, et al. Overweight and obesity: knowledge, attitudes, and practices of general practitioners in France. Obes Res. 2005;13(4):787–795. doi:10.1038/oby.2005.89
17. Rurik I, Torzsa P, Ilyés I, et al. Primary care obesity management in Hungary: evaluation of the knowledge, practice and attitudes of family physicians. BMC Fam Pract. 2013;14(1):156. doi:10.1186/1471-2296-14-156
18. Glauser TA, Roepke N, Stevenin B, et al. Physician knowledge about and perceptions of obesity management. Obes Res Clin Pract. 2015;9(6):573–583. doi:10.1016/j.orcp.2015.02.011
19. Turner M, Jannah N, Kahan S, et al. Current knowledge of obesity treatment guidelines by health care professionals. Obesity. 2018;26(4):665–671. doi:10.1002/oby.22142
20. Dietz WH, Baur LA, Hall K, et al. Management of obesity: improvement of healthcare training and systems for prevention and care. Lancet. 2015;385(9986):2521–2533. doi:10.1016/S0140-6736(14)61748-7
21. Duncan DT, Wolin KY, Scharoun-Lee M, et al. Does perception equal reality? Weight misperception in relation to weight-related attitudes and behaviors among overweight and obese US adults. Int J Behav Nutr Phys Act. 2011;8:20. doi:10.1186/1479-5868-8-20
22. Mahfouz A, Shatoor A, Khan M, et al. Nutrition, physical activity, and gender risks for adolescent obesity in Southwestern Saudi Arabia. Saudi J Gastroenterol. 2011;17(5):318–322. doi:10.4103/1319-3767.84486
23. Crane MM, Jeffery RW, Sherwood NE. Exploring gender differences in a randomized trial of weight loss maintenance. Am J Men Health. 2017;11(2):369–375. doi:10.1177/1557988316681221
24. Song Y, Kwon M, Kim SA. Distorted body weight perception and its gender differences in middle-aged adults: population-based study. BMC Public Health. 2020;20(1):1–9. doi:10.1186/s12889-020-8358-9
25. Assari S, Lankarani MM, Motlagh M-E. Mediating effect of perceived overweight on the association between actual obesity and intention for weight control; role of race, ethnicity, and gender. Int J Prev Med. 2015;6:6. doi:10.4103/2008-7802.151436
26. Lemon SC, Rosal MC, Zapka J, Borg A, Andersen V. Contributions of weight perceptions to weight loss attempts: differences by body mass index and gender. Body Image. 2009;6(2):90–96. doi:10.1016/j.bodyim.2008.11.004
27. Hansen AR, Rustin C, Opoku ST, Shevatekar G, Jones J, Zhang J. Trends in US adults with overweight and obesity reporting being notified by doctors about body weight status, 1999–2016. Nutr Metab Cardiovasc Dis. 2020;30(4):608–615. doi:10.1016/j.numecd.2020.01.002
28. Gupta N, Bombak A, Foroughi I, Riediger N. Discrimination in the health care system among higher-weight adults: evidence from a Canadian national cross-sectional survey. Res Policy Pract. 2020;40:329–335.
29. Caterson ID, Alfadda AA, Auerbach P, et al. Gaps to bridge: misalignment between perception, reality and actions in obesity. Diabetes Obes Metab. 2019;21(8):1914–1924. doi:10.1111/dom.13752
30. Memish ZA, El Bcheraoui CE, Tuffaha M, et al. Obesity and associated factors - Kingdom of Saudi Arabia, 2013. Prev Chronic Dis. 2014;11(10):E174. doi:10.5888/pcd11.140236
31. Al-Raddadi R, Bahijri SM, Jambi HA, et al. The prevalence of obesity and overweight, associated demographic and lifestyle factors, and health status in the adult population of Jeddah, Saudi Arabia. Ther Adv Chronic Dis. 2019;10:2040622319878997. doi:10.1177/2040622319878997
32. Al-Ghamdi S, Shubair MM, Aldiab A, et al. Prevalence of overweight and obesity based on the body mass index; A cross-sectional study in Alkharj, Saudi Arabia. Lipids Health Dis. 2018;17(1):134. doi:10.1186/s12944-018-0778-5
33. Al-Hazzaa HM, Albawardi NM. Activity energy expenditure, screen time and dietary habits relative to gender among Saudi youth: interactions of gender with obesity status and selected lifestyle behaviours. Asia Pac J Clin Nutr. 2019;28(2):389–400. doi:10.6133/apjcn.201906_28(2).0022
34. Cohen AK, Rai M, Rehkopf DH, Abrams B. Educational attainment and obesity: a systematic review. Obes Rev. 2013;14(12):989–1005. doi:10.1111/obr.12062
35. Sobal J, Hanson KL, Frongillo EA. Gender, ethnicity, marital status, and body weight in the United States. Obesity. 2009;17(12):2223–2231. doi:10.1038/oby.2009.64
36. Haselhuhn MP, Kennedy JA, Kray LJ, et al. Gender differences in trust dynamics: women trust more than men following a trust violation. J Exp Soc Psychol. 2015;56:104–109. doi:10.1016/j.jesp.2014.09.007
37. Lewicki RJ, Bunker BB. Developing and maintaining trust in work relationships. In: Kramer RM, Tyler TR, editors. Trust in Organizations. Thousand Oaks: Frontiers of Theory and Research. SAGE Publications; 1996:114–139.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.