")
Back to Journals » Psychology Research and Behavior Management » Volume 12
Gender differences in caregiving among a schizophrenia population
Authors Yu Y, Zhou W , Liu ZW, Hu M , Tan ZH, Xiao SY
Received 18 September 2018
Accepted for publication 13 November 2018
Published 20 December 2018 Volume 2019:12 Pages 7—13
DOI https://doi.org/10.2147/PRBM.S187975
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Mei-Chun Cheung
Yu Yu,1 Wei Zhou,2 Zi-wei Liu,3 Mi Hu,1 Zhi-hui Tan,4 Shui-yuan Xiao1
1Department of Social Medicine and Health Management, Xiangya School of Public Health, Central South University, Changsha, Hunan 410008, China; 2Hospital Administration Institute, Xiangya Hospital, Central South University, Changsha, Hunan 410008, China; 3Department of Psychiatry, Mental Health Institute of the Second Xiangya Hospital, Central South University, Changsha, China; 4Department of Gynaecology, Xiangya Hospital, Central South University, Changsha, Hunan 410008, China
Background: The present study aimed to investigate differences in family burden and caregiver distress in a population of caregivers for schizophrenia, by separating patient gender and caregiver gender.
Methods: A sample of 327 primary family caregivers was recruited from a Chinese rural community through a one-stage cluster-sampling method. A cross-sectional design was employed, using validated measures to assess both family burden and primary caregivers’ depression and anxiety.
Results: Significant differences by gender were detected in family burden and caregiver distress. Family burden was significantly higher for male patients on the domains of effect on physical and mental health of others, and significantly higher for female caregivers on the domains of financial burden and effect on physical and mental health of others. Caregivers of male patients were more likely to suffer from anxiety than caregivers of female patients (52.7% vs 38.1%, P=0.012); female caregivers were more likely to suffer from depression (51.2% vs 38.6%, P = 0.031) and anxiety (51.6% vs 38.1%, P=0.020) than male caregivers.
Conclusion: The results reinforced the expected differences in caregiving experiences of a schizophrenia population by gender, which has implications for the future design of gender-specific interventions to alleviate family burden and caregiver distress.
Keywords: gender, caregiving burden, schizophrenia, depression, anxiety
Introduction
Decades of international research have served to confirm that caring for a family member with schizophrenia often engenders an enormous burden, which may lead to an increased risk of depression, anxiety, and mortality among family caregivers.1,2 An accumulating number of studies have also endeavored to explore correlates of family burden. While there is more agreement that family burden is positively associated with the psychopathology and disability of schizophrenia and can be alleviated by strengthening social psychological factors such as social support, family function, and positive coping,1,3,4 conflicting evidence exists on the correlation between family burden and sociodemographic factors. For instance, the literature differs on whether caring for male patients or female patients is more burdensome. Some studies showed that a higher level of burden was associated with caring for male patients,5,6 while others reported that burden was either associated more with caring for female patients7,8 or had no significant association with gender.9 Jenkins and Schumacher6 contended that not only the patient’s gender but also the gender of the caregivers must be considered when it comes to family burden. There is a lack of convincing evidence on gender differences in family burden by separating the gender of both patients and caregivers in a systematic way. In response to this gap in the research, the present study was designed to investigate differences in sociodemographic characteristics, family burden, and caregiver distress between male and female patients and between male and female caregivers.
Methods
Participants
A cross-sectional, descriptive study was conducted in Ningxiang County, Hunan Province of China. A sample of 327 primary family caregivers was recruited from four towns and villages of Ningxiang County through a one-stage cluster-sampling method. The primary family caregiver in each family was self-identified. Inclusion criteria for this study were as follows: 1) older than 16 years of age; 2) living with and most involved with the actual care for patients diagnosed with schizophrenia under the Chinese Classification of Mental Disorders-3 (CCMD-3) or ICD-10 criteria; and 3) able to understand and communicate in Chinese. After excluding 14 participants who refused to participate and 11 who withdrew, our final sample included 327 community-dwelling primary caregivers of individuals with schizophrenia.
Ethical approval was obtained from the Institutional Review Board of the Xiangya School of Public Health of Central South University. The study was conducted in accordance with the Declaration of Helsinki. All participants provided written informed consent before the study.
Data were collected using face-to-face interviews with primary caregivers at their home. Nine postgraduates from the Xiangya School of Public Health of Central South University were recruited as interviewers. All interviewers had a background in public health, and also received basic training in psychology and psychiatry. All interviewers received 1 week of uniform formal training to conduct the interviews, which was provided by a psychologist before the formal study. The training was composed of lectures and practicing role play.
Instruments
Demographic information sheet
Demographic information on both the patients and primary caregivers was collected on a self-designed sheet, which included both patients’ and caregivers’ gender, age, marital status, occupation, education, and kinship between the patients and caregivers. We also collected information on family per-capita annual income to assess financial status. Based on the national rural poverty line of 2,300 yuan in 2010 as the lower limit and the Hunan provincial average of 10,060 yuan in 2014 as the upper limit, we categorized financial status into three levels: low level (≤2,300 yuan/year), middle level (2,300–10,060 yuan/year), and high level (>10,060 yuan/year).
Patient function
The Global Assessment of Function (GAF) scale11 was applied to evaluate patients’ overall social, occupational, and psychological functioning during a particular period. This is a 100-point single-item rating scale, with 1 indicating the lowest functioning and 100 the highest. Examples are given for each 10-level interval. GAF is one of the axes of DSM-IV and has been proved to be a reliable and valid measure of psychiatric functioning.11 The functional level of a patient over the past 1 month was assessed with GAF in this study. For the present study, all nine interviewers showed good inter-rater reliability, with an intraclass correlation coefficient of 0.85 during the pre-study training.
Family burden
Family burden was assessed by the 24-item Family Burden Interview Schedule (FBIS),12 tapping six dimensions: financial burden, disruption of routine family activities, disruption of family leisure, disruption of family interactions, effect on physical health of others, and effect on mental health of others. Each item is rated on a three-point Likert scale from 0 (no burden) to 2 (serious burden). Total scores are the sum of all 24 items, ranging from 0 to 48, with higher scores indicating greater family burden. In the present study, the Chinese version of the FBIS showed acceptable internal consistency, with a Cronbach’s α coefficient of 0.86.
Caregiver depression
Depression was measured by the nine-item Patient Health Questionnaire (PHQ-9),13 which detects the primary caregiver’s depressive symptoms during the past 2 weeks. Each item is rated on a four-point Likert scale from 0 (not at all) to 3 (nearly every day). The total score ranges from 0 to 27, with higher scores implying more depressive symptoms. Scores of 10 or above are viewed as indicative of depression.14 The Chinese version of the PHQ-9 demonstrated good internal consistency in the current study, with a Cronbach’s α coefficient of 0.89.
Caregiver anxiety
Anxiety was measured by the seven-item Generalized Anxiety Disorder Scale (GAD-7),15 which detects the primary caregiver’s anxiety symptoms during the past 2 weeks. Each item is rated on a four-point Likert scale from 0 (not at all) to 3 (nearly every day). The total score ranges from 0 to 21, with a cutoff point of 10 differentiating between anxiety and non-anxiety.16 The Chinese version of the GAD-7 demonstrated good internal consistency in the current study, with a Cronbach’s α coefficient of 0.91.
Data analysis
Descriptive statistics were used to summarize the demographic characteristics and study variables. Group differences for continuous variables were tested using independent t-tests for normally distributed data or the Mann–Whitney U test for non-normally distributed data. Group differences for categorical variables were tested using Pearson’s chi-squared tests. Analysis was carried out using SPSS 16.0 (SPSS Inc.,Chicago, IL, USA). Statistical significance was determined at a value of P<0.05.
Results
Sample characteristics
Demographic and clinical variables are listed in Table 1 for all subgroups of patients and caregivers: male patients, female patients, male caregivers, and female caregivers. Compared to male patients, female patients were of older age, more likely to be married, unemployed, mainly cared for by their spouse, and had better social functioning as indicated by GAF score, all with P<0.05. No significant differences were noted in education and financial status between male and female patients. Compared to male caregivers, female caregivers were more likely to be unmarried, unemployed, had a middle level financial status, and to be parents of patients, all with P<0.05. No significant differences were noted in age, education and patient functioning between male and female caregivers.
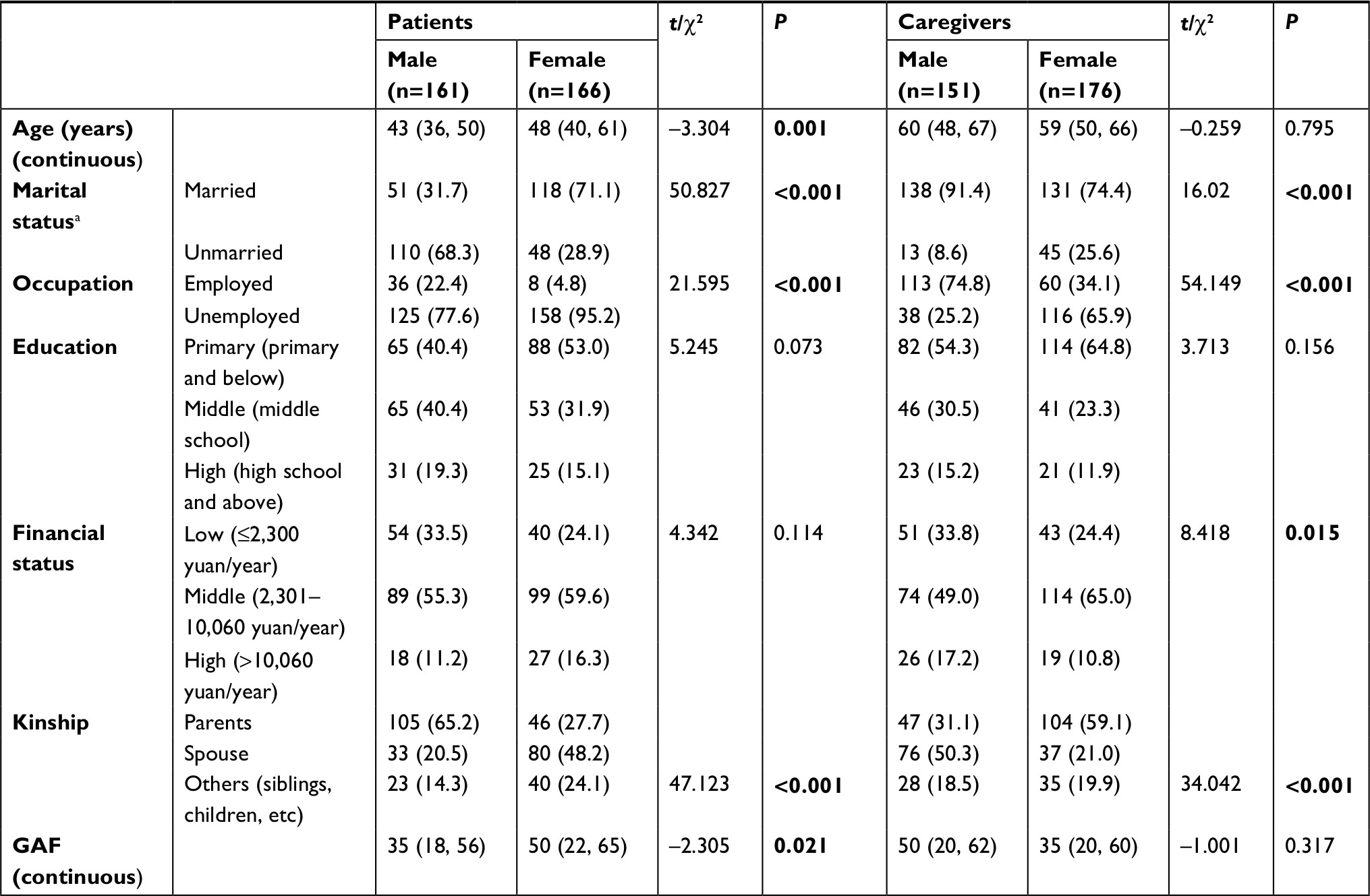 | Table 1 Characteristics of patients and caregivers by gender Notes: Data are shown as median (IQR) or n (%). aMarried includes married and cohabited, unmarried includes single, divorced, and widowed. Bold font indicates a statistically significant difference (P<0.05). Abbreviation: GAF, Global Assessment of Function. |
Family burden
In terms of family burden, no significant difference was detected in the total score of FBIS between male and female patients, yet higher scores were reported in the domains of adverse effect on physical and mental health of other family members for male patients than for female patients. For caregivers, female caregivers reported significantly higher total family burden score than male caregivers, which was also reflected in the following three domains: financial burden, effect on physical health of others, and effect on mental health of others (Table 2).
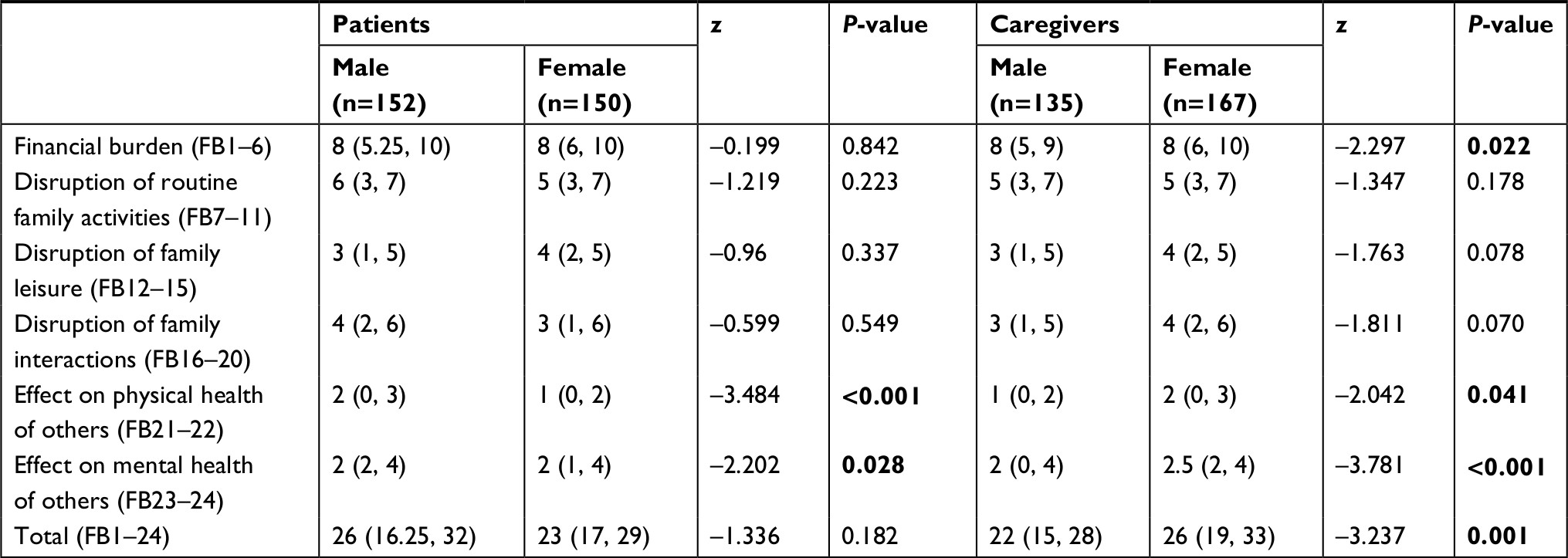 | Table 2 Family burden score by gender Notes: Data are shown as median (IQR). Bold font indicates statistically significant difference (P<0.05). Abbreviation: FB, family burden. |
Psychological distress
Table 3 contrasts the psychological distress including depression and anxiety by subgroups of gender. Compared to caregivers of female patients, caregivers of male patients were more likely to suffer from anxiety (52.7% vs 38.1%, P=0.012), while no significant difference was detected in depression between caregivers of male and female patients. With regard to caregivers, female caregivers were more likely to suffer depression (51.2% vs 38.6%, P=0.031) and anxiety (51.6% vs 38.1%, P=0.020) than male caregivers.
 | Table 3 Psychological distress of caregivers by gender Notes: Data are shown as n (%). Bold font indicates a statistically significant difference (P<0.05). |
Across the entire sample, scores on the FBIS and the PHQ-9 and GAD-7 were positively correlated, indicating that as family burden increases, caregiver depression and anxiety increase. This correlation remained significant within all subgroups (all P<0.05, data not shown).
Discussion
Summary of the findings
To the best of our knowledge, this is the first study to systematically explore differences in caregiving experiences in a rural community population of patients with schizophrenia by separating both patient gender and caregiver gender. Significant differences were detected in sociodemographics, family burden, and caregiver distress between male patients and female patients and between male caregivers and female caregivers.
Gender and sample characteristics
The finding that female patients were older (by 5 years) and had better social functioning than male patients in this study was consistent with other studies in China and may be explained by the fact that female patients live longer than male patients.17,18 A 14-year cohort study on the gender differences in outcomes in people with schizophrenia in rural China found that male patients had significantly higher rates of mortality, suicide and homelessness, and poorer family and social support, which may be a major reason for the shorter lifespan and thus younger average age of male patients than female patients.18
One striking finding is the poignant contrast of the much higher marriage rate in female patients than in male patients (71.1% vs 31.7%), which mirrors the widespread phenomenon of high marriage costs for males in Chinese rural communities.19,20 In most rural areas, a man normally needs at least 100,000 RMB and an additional house to marry a woman,19,20 which is difficult even for a healthy working man, let alone for a man with schizophrenia, whose ability to join the labor force may be impaired or lost. On the other hand, considering the difficulty for a man to marry a woman, it is easier for a woman to be married to a man. Some men who are incapable of marrying a healthy woman may choose to marry a woman with a mental disorder at a lower expense than normally required. Another possible explanation is the different role expectations between men and women, in that men are expected to work outside the home to support the family while women are required to stay at home and perform their main task of childbearing. A man with schizophrenia may be unable to support a family owing to impaired working function, while a woman can still bear children even when she has schizophrenia. Also, in a male-dominated society such as China, it is much easier for a man to marry a woman who is seen as inferior to or less competent than him. As a result, in this study, far more females than males with schizophrenia were married.
The significantly higher unemployment rate for females than for males is consistent with the societal and cultural demands for men to be employed outside the home and women to stay at home and do housework, as mentioned in the previous paragraph. That the majority of female patients were cared for by their spouses (48.2%) while most male patients were cared for by their parents (65.2%) may be a natural result of the much higher marriage rate for females than for males with schizophrenia.
The fact that more male caregivers were married and were mainly the spouse of patients is another reflection of the patients’ characteristics, showing that more female patients were married and thus cared for by their husbands. The findings of higher unemployment rate and higher financial status of female caregivers were consistent with the social and cultural background of Chinese rural communities, where females are married to a family with strong economic status and stay at home as housewives.
Patient gender, family burden, and caregiver distress
Higher family burden scores were reported on the domains of adverse effect on physical and mental health of other family members for male patients than for female patients, which is in accordance with the literature.21 One major reason may be that male patients were generally more involved in violence and other disturbing behaviors than females (as presented in the GAF scores) and thus caused more adverse effects on the physical and mental health of the family. Furthermore, a higher prevalence of anxiety was also detected in caregivers of male patients than in those of female patients, which further corroborates our previous assumption of males’ more problematic behaviors leading to more psychological distress in caregivers.
Caregiver gender, family burden, and caregiver distress
Female caregivers reported significantly higher financial burden than male caregivers, which seems to be in contradiction with the higher financial status of female caregivers. However, considering that more female than male caregivers were unemployed (65.9% vs 25.2%) and mainly relied on other family members to provide financial support, it makes sense that female caregivers were more vulnerable to financial risks and thus endured higher financial burden. Female caregivers also reported more adverse effects on the physical and mental health of others and were more likely to suffer from psychological distress, including anxiety and depression. Although some studies found no gender difference in caregiving burden and caregiver mental health,22 a majority of the existing literature showed that female caregivers are worse off than male caregivers.23 Even in the general population, women are 1.5–3 times more likely than men to suffer depression, a phenomenon that has been widely acknowledged in the literature and can be explained by both biological and social factors.24,25 One explanation is the gender role theory, where female caregivers are more emotionally connected to the patient, more willing to sacrifice their social life, and less likely to seek external help and resources and thus perceive more burden and stress.26 Another possible reason may be the different coping methods used by females and males, with women more often resorting to emotional coping strategies that usually lead to a higher sense of burden and depression.27 In contrast, men use coping strategies that focus on solving challenging problems, avoiding disruption and distractions, and thus block their emotional reactions.28
Limitations
One major concern with this study is that the assessment of patient function using the GAF scale was carried out by a team of postgraduate students asking the primary caregivers, instead of by professional psychiatrists assessing the patients themselves, which may cause potential bias in the scoring. The reason for not interviewing patients themselves was that most of the patients either were not at home (eg, visiting a doctor or in hospital), or were too cognitively impaired to communicate, or had an onset of symptoms during the interview and thus were unavailable or unable to be correctly assessed. Besides, considering the difficulty of reaching each community sample and the constraints of time, money, and human resources, it would have been difficult to hire professional psychiatrists, who are already busy with work, to follow the research team to conduct face-to-face interviews. To minimize the possibility of scoring bias, all interviewers were uniformly trained with standard interviewing methods by a professional psychologist to guarantee internal consistency. A second possible limitation is that the measurement of depression and anxiety relied on the use of rapid screening tools, ie, the PHQ-9 and GAD-7, instead of standard psychometric tools. Future research may consider using more professional measurement tools to increase measurement accuracy, if possible. A third limitation is that the sample came from one single rural county of Hunan Province, which may limit the study’s representativeness. Future multicenter comparative studies, with large samples, are warranted to enable firmer conclusions to be drawn.
Conclusion
The study results reinforced the expected differences in the caregiving experiences of a schizophrenia population by gender. Differences exist in family burden and caregiver psychological distress by both patient gender and caregiver gender.
The findings of our study may provide guidance for future interventions to be gender specific to alleviate family burden and caregiver distress.
Acknowledgments
The authors would like to thank all the families of the individuals with schizophrenia whom we interviewed during the study for openly sharing their feelings and experiences. We would also like to thank the health and family planning bureau of Ningxiang County and the governments of Liushahe town, Shungfupu town, Chengjiao xiang, and Yutan town for their administrative support, as well as all village/community doctors for guiding us to visit the households of the individuals with schizophrenia in the rural areas of Ningxiang County, Hunan Province. The study was funded by “CMB-CSU” Collaborative Program for Mental Health Policy Development (II) (grant number 14-188) and the National Natural Science Foundation of China (grant number 71804197).
Author contributions
YY and SYX contributed to the conception and design of the study, YY, WZ, ZWL, MH, and ZHT contributed to the research conduction and data collection, YY, WZ, and ZWL contributed to data analyses and interpretation. YY drafted the article, and WZ, ZWL, MH, ZHT, and SYX critically appraised and revised it. All authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
Pol MC, Ter Riet G, van Hartingsveldt M, Kröse B, de Rooij SE, Buurman BM. Effectiveness of sensor monitoring in an occupational therapy rehabilitation program for older individuals after hip fracture, the SO-HIP trial: study protocol of a three-arm stepped wedge cluster randomized trial. BMC Health Serv Res. 2017;17(1):3. | ||
Piszczek J, Partlow E. Stepped-wedge trial design to evaluate Ebola treatments. Lancet Infect Dis. 2015;15(7):762–763. | ||
Jagannathan A, Thirthalli J, Hamza A, Nagendra HR, Gangadhar BN. Predictors of family caregiver burden in schizophrenia: Study from an in-patient tertiary care hospital in India. Asian J Psychiatr. 2014;8:94–98. | ||
Zhang Z, Deng H, Chen Y, et al. Cross-sectional survey of the relationship of symptomatology, disability and family burden among patients with schizophrenia in Sichuan, China. Shanghai Arch Psychiatry. 2014;26(1):22–29. | ||
Li S, Wu Y, Du X, et al. Rational and design of a stepped-wedge cluster randomized trial evaluating quality improvement initiative for reducing cardiovascular events among patients with acute coronary syndromes in resource-constrained hospitals in China. Am Heart J. 2015;169(3):349–355. | ||
Jenkins JH, Schumacher JG. Family burden of schizophrenia and depressive illness. Specifying the effects of ethnicity, gender and social ecology. Br J Psychiatry. 1999;174:31–38. | ||
Maxwell AE, Dennis M, Rudd A, Weir CJ, Parker RA, Salman RA. Erratum to: Promoting Recruitment using Information Management Efficiently (PRIME): study protocol for a stepped-wedge cluster randomised controlled trial within the REstart or STop Antithrombotics Randomised Trial (RESTART). Trials. 2017;18(1):146. | ||
Richard L, Piper D, Weavell W, et al. Advancing engagement methods for trials: the CORE study relational model of engagement for a stepped wedge cluster randomised controlled trial of experience-based co-design for people living with severe mental illnesses. Trials. 2017;18(1):169. | ||
Reuther S, Holle D, Buscher I, et al. Effect evaluation of two types of dementia-specific case conferences in German nursing homes (FallDem) using a stepped-wedge design: study protocol for a randomized controlled trial. Trials. 2014;15:319. | ||
Ren Y, Yang M, Li Q, et al. Assessing dose-response effects of national essential medicine policy in China: comparison of two methods for handling data with a stepped wedge-like design and hierarchical structure. BMJ Open. 2017;7(2):e013247. | ||
Rasmussen CD, Holtermann A, Mortensen OS, Søgaard K, Jørgensen MB. Prevention of low back pain and its consequences among nurses’ aides in elderly care: a stepped-wedge multi-faceted cluster-randomized controlled trial. BMC Public Health. 2013;13:1088. | ||
Pai S, Kapur RL. The burden on the family of a psychiatric patient: development of an interview schedule. Br J Psychiatry. 1981;138:332–335. | ||
Spitzer RL, Kroenke K, Williams JB. Validation and utility of a self-report version of PRIME-MD: the PHQ primary care study. Primary Care Evaluation of Mental Disorders. Patient Health Questionnaire. JAMA. 1999;282(18):1737–1744. | ||
Manea L, Gilbody S, Mcmillan D. A diagnostic meta-analysis of the Patient Health Questionnaire-9 (PHQ-9) algorithm scoring method as a screen for depression. Gen Hosp Psychiatry. 2015;37(1):67–75. | ||
Spitzer RL, Kroenke K, Williams JB, Löwe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. 2006;166(10):1092–1097. | ||
Schalet BD, Cook KF, Choi SW, Cella D. Establishing a common metric for self-reported anxiety: linking the MASQ, PANAS, and GAD-7 to PROMIS Anxiety. J Anxiety Disord. 2014;28(1):88–96. | ||
Somerville M, Basham M, Foy C, et al. From local concern to randomized trial: the Watcombe Housing Project. Health Expect. 2002;5(2):127–135. | ||
Ran MS, Mao WJ, Chan CL, Chen EY, Conwell Y. Gender differences in outcomes in people with schizophrenia in rural China: 14-year follow-up study. Br J Psychiatry. 2015;206(4):283–288. | ||
Xing-Yu C. The influence of high betrothal gifts on rural marriage (in Chinese). Reform & Opening. 2014;24:48–49. | ||
Spicer RS, Miller TR. Impact of a workplace peer-focused substance abuse prevention and early intervention program. Alcohol Clin Exp Res. 2005;29(4):609–611. | ||
Page K, Stein ES, Carrico AW, et al. Protocol of a cluster randomised stepped-wedge trial of behavioural interventions targeting amphetamine-type stimulant use and sexual risk among female entertainment and sex workers in Cambodia. BMJ Open. 2016;6(5):e010854. | ||
Jeyagurunathan A, Sagayadevan V, Abdin E, et al. Psychological status and quality of life among primary caregivers of individuals with mental illness: a hospital based study. Health Qual Life Outcomes. 2017;15(1):106. | ||
Bennett JB, Lehman WE. Workplace substance abuse prevention and help seeking: comparing team-oriented and informational training. J Occup Health Psychol. 2001;6(3):243–254. | ||
Kessler RC. Gender differences in major depression. Epidemiological findings. In: Frank E, editor. Gender and Its Effects on Psychopathology. Washington, DC: American Psychiatric Press; 2005; 364–369. | ||
Parker G, Fletcher K, Paterson A, Anderson J, Hong M. Gender differences in depression severity and symptoms across depressive sub-types. J Affect Disord. 2014;167:351–357. | ||
Bennett JB, Beaudin CL. Collaboration for preventing substance abuse in the workplace: modeling research partnerships in prevention. J Healthc Qual. 2000;22(4):24–30. | ||
Alexander S, Bosch JL, Hendriks JM, Visser JJ, van Sambeek MR. The 30-day mortality of ruptured abdominal aortic aneurysms: influence of gender, age, diameter and comorbidities. J Cardiovasc Surg. 2008;49(5):633–637. | ||
Wilmink TB, Quick CR, Hubbard CS, Day NE. The influence of screening on the incidence of ruptured abdominal aortic aneurysms. J Vasc Surg. 1999;30(2):203–208. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.