")
Back to Journals » International Journal of Women's Health » Volume 14
Gender-Based Violence and Associated Factors Among Women with Disabilities in Jimma Town, Ethiopia
Authors Getachew S , Debelew GT , Abdullahi M
Received 27 June 2022
Accepted for publication 13 October 2022
Published 26 October 2022 Volume 2022:14 Pages 1531—1545
DOI https://doi.org/10.2147/IJWH.S380233
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Selamawit Getachew,1 Gurmesa Tura Debelew,2 Misra Abdullahi2
1Department of Public Health, Wachemo University, Hosanna, Ethiopia; 2Department of Population and Family Health, Faculty of Public Health, Jimma University, Jimma, Ethiopia
Correspondence: Selamawit Getachew, Department of Public Health, Wachemo University, Hosanna, Ethiopia, Email [email protected]
Background: Globally, women with disabilities have two times higher chance of suffering from violence compared to their non-disabled peers due to double discrimination. However, there is little evidence that quantifies the situation in this segment of the population by considering disability-related factors which make this group more vulnerable to gender-based violence in Ethiopia.
Objective: To assess the prevalence of gender-based violence and its associated factors among women with disabilities in Jimma town, southwest Ethiopia, 2020.
Methods: A community based cross-sectional study was conducted among a total of 308 women with disabilities. Bivariate and multivariable logistic regression analyses were carried out to identify factors associated with gender-based violence. The significance of the association was decided by using the 95% confidence interval of AOR at a p-value of < 0.05 in the multivariable analysis.
Results: The lifetime prevalence of gender-based violence among women with disabilities was found to be 73.1, while 46.1% had experienced it during the last 12 months. Gender-based violence in the past 12 months was significantly associated with non-schooling (AOR=5.10; 95% CI, 1.51, 17.14), being in age group of 20– 34 (AOR=3.5; 95% CI, 1.74, 7.30), having visual impairment (AOR=3.1; 95% CI, 1.27, 7.54), having hearing impairment (AOR=3.0; 95% CI, 1.36, 6.89), alcohol use behavior (AOR=4.1; 95% CI, 1.74, 9.55), and perceived stigma and discrimination (AOR=4.2; 95% CI, 2.44, 7.39).
Conclusion: Prevalence of gender-based violence among women with disabilities was found to be high in the study area. Educational status, age, type of disability, alcohol use behavior, and perceived stigma and discrimination were independent predictors of gender-based violence. Measures have to be taken to curb the problem by taking integrated interventions like enrolling girls in school and targeted health education towards identified factors by considering the heterogeneity of disabilities.
Keywords: gender-based violence, violence against women, disability, southwest Ethiopia
Background
People with disabilities are estimated to be 15% of the world’s population. Of these, the female disability prevalence rate is 19.2%. In Ethiopia, it is estimated that 15 million people live with disabilities, representing 17.6% of the total population.1
Persons with disabilities of both genders are predominantly exposed to abuse but women with disabilities have a high risk of experiencing violence due to “double discrimination” as both female gender and disability are viewed as notions of vulnerability and lack of power.2–5
When talking about violence against women and girls with disabilities, it is not just only about gender-based violence: it is an intersectional category dealing with both gender-based and disability-based factors.6 Disability-based factors like dependence on others, reduced personal defenses, social myth, absence of a supportive environment, and socio-economic exclusions make them highly vulnerable to different kinds of abuse than their non-disabled peers.7–9
Globally, people with disabilities have a 50% higher chance of suffering from violence when compared with non-disabled people.10 In low and middle-income countries, women with disabilities are two to four times more likely to experience intimate partner violence than women without disabilities.11,12 In Ethiopia, 30.8% and 57.7% of women with disabilities have experienced physical and sexual violence, respectively.8
Gender-based violence among women with disabilities results in 475,000 deaths worldwide.13 It has also been linked with psychological and physical harm like anxiety, depression and lower levels of self-esteem, unwanted pregnancy, abortion, HIV/AIDS, and STIs.8,14–16 Additionally, it results in adverse socio-economic consequences; the cost of the societal effects of threatened or actual violence against people with disabilities in England was £1.51 billion.14
Several international and national instruments, as well as programs, have a strong will for eliminating gender-based violence and protecting the rights of people with disabilities.17,18 This goal of eliminating gender-based violence among women and girls is unlikely to be achievable without knowing the nature of violence among this segment of the population.13
Even though studies are conducted in determining the extent of violence in this group, almost solely the majority of the studies were mainly undertaken in the developed world4,14,19,20 and there are also contradicting ideas regarding some factors associated with gender-based violence.7,21–23
To the best search of the literature, there is little evidence in Ethiopia regarding the extent of GBV among women with disabilities, and some disability-related factors which make them more vulnerable were not taken into account in the previous studies.8 This study, therefore, fills these gaps by determining the magnitude of the problem and identifying the potential factors including those disability-related factors. Consequently, this research may provide evidence-based information which can be useful for the implementation and maintenance of intersectionality-based violence prevention policies and practices, using a “disability perspective” in violence preventionwork.
Methods
Study Design
A community-based cross-sectional study design was carried out from March 21 to May 20,2020.
Study Setting
The study was conducted in Jimma town which is the capital of the Jimma zone. Jimma town is one of the towns in Oromia regional state located in the Southwest of Ethiopia at 352 km from the capital of Ethiopia, Addis Ababa. A report from Jimma town labor and social affairs; shows that at the time of the study, there were about 1231 persons with disabilities in Jimma town; of which, 326 were women with disabilities aged >15 years.
Source Population
All women with disabilities aged 15 years and above in Jimma town, Ethiopia.
Study Population
All women with disabilities aged 15 years and above in Jimma town who fulfills the inclusion criteria and selected and included in the study.
Eligibility Criteria
Inclusion Criteria
All women with disabilities aged 15 years and above who were permanent residents in the study areas for more than 6 months were included.
Exclusion Criteria
Those who have both visual and hearing impairment and those having mental impairment were excluded because of the difficulty to interview them as they neither hear nor see to apply sign language.
Sample Size Determination
The sample size was calculated by using EPI Info version 7 by considering different assumptions. To determine the prevalence of gender-based violence, the sample size was determined by assuming the prevalence of gender-based violence among women with disabilities to be 57.7% (P = 0.57),8 95% level of confidence, 5% margin of error, and 10% non-response rate. Considering the finite population correction formula, this gave a final sample size of 191.
To identify the factors associated with GBV among women with disabilities, the sample size was determined by considering the following assumptions; 95% Confidence level, 80% power, and taking the probability of outcome among exposed to be 58.6%, with an odds ratio=2.03, and 10% non-response rate. So, the final sample size of the study was 301. Since the source population was too small (326), all of them were taken.
Sampling Procedure
The specific data concerning the participants (the type of disability and Kebele where they live) were obtained from the registration book which is found at each Kebele. Then, all 326 women with disabilities aged 15 and above were included. This meant that once their living place was obtained from the Kebele registration book, the data collectors visited their home with the help of the guide and the interviews were done at their home/living place.
Variables
Disability
Disability is defined as chronic physical, mental, intellectual, or sensory impairments in which interaction with several barriers may impede their full and active involvement in society equally with others.17 For this study, a disability includes either physical or sensory disabilities (visual impairment, hearing impairment, physical impairment, and leprosy).22
Gender-Based Violence(Lifetime Experience)
Women who had experienced at least one act of physical, sexual, or emotional violence by a current partner, former partner, or non-partner(s) at any point in their lives.22
Gender-Based Violence (in the Past 12 Months)
Women who had experienced at least one act of physical, sexual, or emotional violence by a current partner, former partner, or non-partner(s) at any point in the past 12 months.22
Measurements
Physical Violence
Six questions were asked about physical violence including being slapped or having something thrown at that could hurt, being pushed or shoved, being hit with a fist or something else that could hurt, being kicked, dragged or beaten up, being choked, or burnt on purpose, and/or being threatened with, or, having a gun, knife or other weapon used on you, A woman is said to have physical violence when she responds “yes” to at least one of the questions or more.22
Sexual Violence
The three questions on sexual violence includes being physically forced to have sexual intercourse when you did not want to, having sexual intercourse because you were afraid of what your partner might do, and/or being forced to do something sexual that you found humiliating or degrading. A woman is said to have sexual violence when she responds “Yes” to at least one question or more.22
Emotional/Psychological Violence
The four questions on psychological violence include being Insulted or making you feel bad about yourself, Belittled or humiliated in front of other people, Doing things to scare or intimidate you on purpose, and Threatening to hurt you or someone you care about. A woman is said to have emotional violence when she responds “Yes” to at least one question or more.22
Substance Use
Taking any of the three commonly used psychoactive substances: alcohol, cigarettes, and/or chat, which are assumed to affect the level of thinking.
Ever Use
If participants respond yes to any of the questions Have you ever drunk/chewed/smoked alcohol/chat/tobacco in life?24
Perceived Social Stigma and Discrimination
Perceived stigma and discrimination by people with disabilities when having a painful inner struggle about a disability even without any encounter with actual stigmatization. A scale that comprises 12 items with the response of not at all, little, moderately, and a lot was used to construct a composite score.25,26 A score above the mean is said to have high social stigma and discrimination.
Decision-Making Power
Twelve questions were used to construct a composite score. Each question has four response options on the degree of women’s involvement in decision-making (Another family member, the husband only, joint, and self). Based on the responses each question was scored as follows:Another family member decides only=0, husband only=0, Joint decision-making=1, and self-decide only=2. If the response indicates as the decision is made by others, the score given was similar to the husband’s decided score since it is taken by another party, not the woman. After computing altogether, a score above the mean is said to have good decision-making power.
A Gender Equitable Attitude
is an attitude that a society considers appropriate for both males and females. About 12 items with a response of agree, neutral, and disagree were used to construct a composite score. First, negatively stated questions were reverse coded during data processing. Then, it was summed up and a score above the mean is said to have a favorable gender-equitable attitude.
Data Collection Tool, Personnel, and Procedure
An interviewer-administered structured questionnaire was prepared based on the standard WHO Multi-country study on women’s health and domestic violence against women and reviewed different kinds of literature.26–28 The questionnaire includes socio-demographic characteristics; types of violence, disability-related factors, behavioral attributes, and gender-related barriers. Five female data collectors who can speak the local language and two supervisors who are qualified with BSc in public health were recruited. To collect data from participants with hearing impairment, one sign language translator was recruited.
Data Quality Management
To ensure the quality of the data, first, the prepared questionnaire was translated to the local language Afaan Oromo and Amharic by language experts.Then, it was translated back to the English language to check its consistency. Before the actual data collection, a pretest was conducted on 5% of the sample size in the “Asendabo” town and the feedback was incorporated accordingly. The reliability and internal consistency of the scales (perceived stigma and discrimination scale, gender attitude, and decision-making power) were measured for each variable using Cronbach’s alpha (value of α =0.872, 0.721, and 0.876, respectively). The data collectors and supervisors were trained for one day on the objective of the study, the data collection tool, the approach to the interviewees, and the ethical and safety aspects of doing violence research. At the end of each day, questionnaires were reviewed and cross-checked and corrective measures were taken.
Data Analysis
The data was coded and entered into Epidata version 3.1 and exported to SPSS version 25 for analysis. A descriptive analysis was computed for selected variables. The wealth index was calculated using Principal component analysis. Before further analysis normality curve and the presence of multi-collinearity between variables were checked using the Variance inflation factor. The prevalence of GBV was determined by running frequencies with their 95% Confidence Interval estimates. A bivariable analysis was executed to examine the association between independent variables and gender-based violence in the last 12 months. Then, variables that had a P-value <0.25 on Bivariable analysis were selected as candidates for multivariable analysis. Odds ratio and 95% CI were used to measure the existence of statistically significant association, and P-value <0.05 was used to determine the statistical significance of the tests. The goodness of fit of the models was checked by Hosmer–Lemeshow goodness of fit test (p=0.173). Finally, the result was presented in texts, tables, and graphs.
Ethical Consideration
Ethical clearance and approval were obtained from the Ethical Review Board of Jimma University, Institute of Health. All of the study participants were informed about the purpose of the study, their right to refuse, and assured confidentiality, and written informed consent was obtained before the interview. For minors (<18 years), written informed consent from their parent/legal guardian and assent from the children was obtained to participate as per Ethiopian National Research Ethics Review Guideline. At the end of each interview, those women who are a victim of violence and who did not seek care were informed about the necessity of medical care and legal protection as well as where it is given.
Result
Sociodemographic Characteristics of the Participants
A total of 308 women had completed their interviews making a response rate of (94.5%). The median age of the respondents was 29 years (age range 15–60 years). One hundred thirty-five (43.8%) were Muslims by religion. One hundred twenty-two (39.6%) had a primary level of education and more than one-third 112(36.4%) of the respondent were unemployed (Table 1).
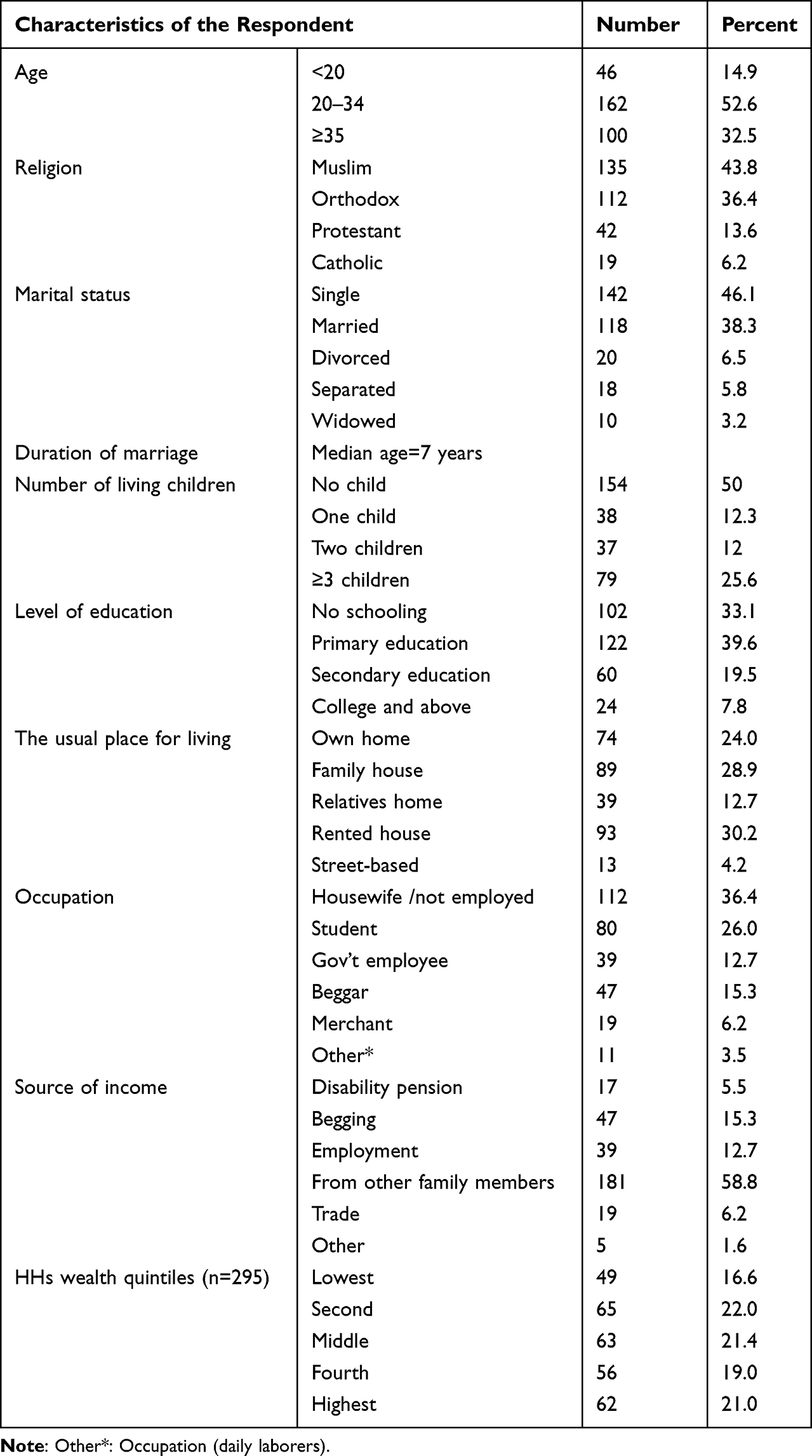 |
Table 1 Socio-Demographic Characteristics of Women with Disability Aged 15 and Above in Jimma, Ethiopia, 2020 (n=308) |
Gender-Related Characteristics
The respondent’s score for attitude ranges from 12 to 36, and the mean score (SD) was 26.06 (±5.49). More than half 175 (56.8%) of the women scored below the mean indicating they had an unfavorable gender-equitable attitude. And also, the score range for decision-making power was 0–24 and the mean score for decision-making power was 9.94 (±5.58). Almost half 156(50.6%) of the women scored above the mean, ie, they had good decision-making power (Table 2).
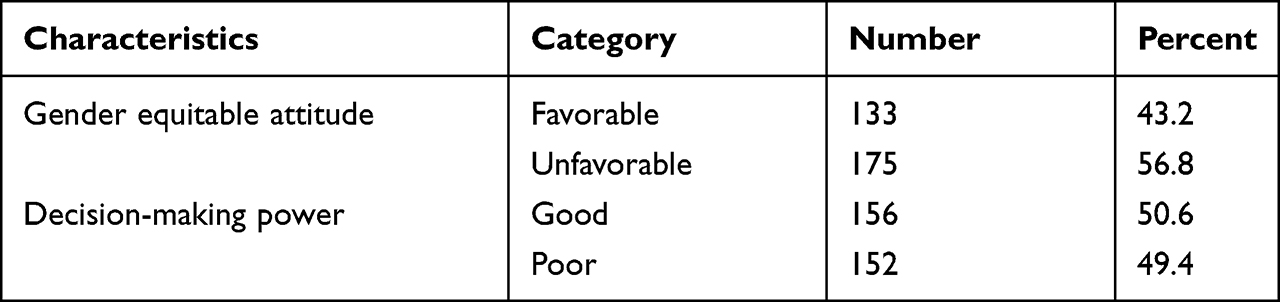 |
Table 2 Gender-Related Characteristics of Women with Disability Aged 15 and Above in Jimma, Ethiopia, 2020 (n=308) |
Disability Characteristics of the Participants
Nearly half of the women with disabilities149 (48.4%) had a physical impairment. A quarter 75(24.4%)) of respondents reported that they had the disability since birth, whereas 113 (36.6%) became disabled after birth during childhood. The majority (74%) of the respondents were economically dependent on others, while 13.6% and 19.5% of the respondent were dependent on personal care and movement, respectively. Regarding perceived stigma and discrimination, the respondent’s score for perceived stigma and discrimination ranges from 12 to 48 and the mean score (SD) was 17.4(±5.45). One hundred thirty-two (42.9%) of the women scored above the mean, ie, had high perceived stigma and discrimination (Table 3).
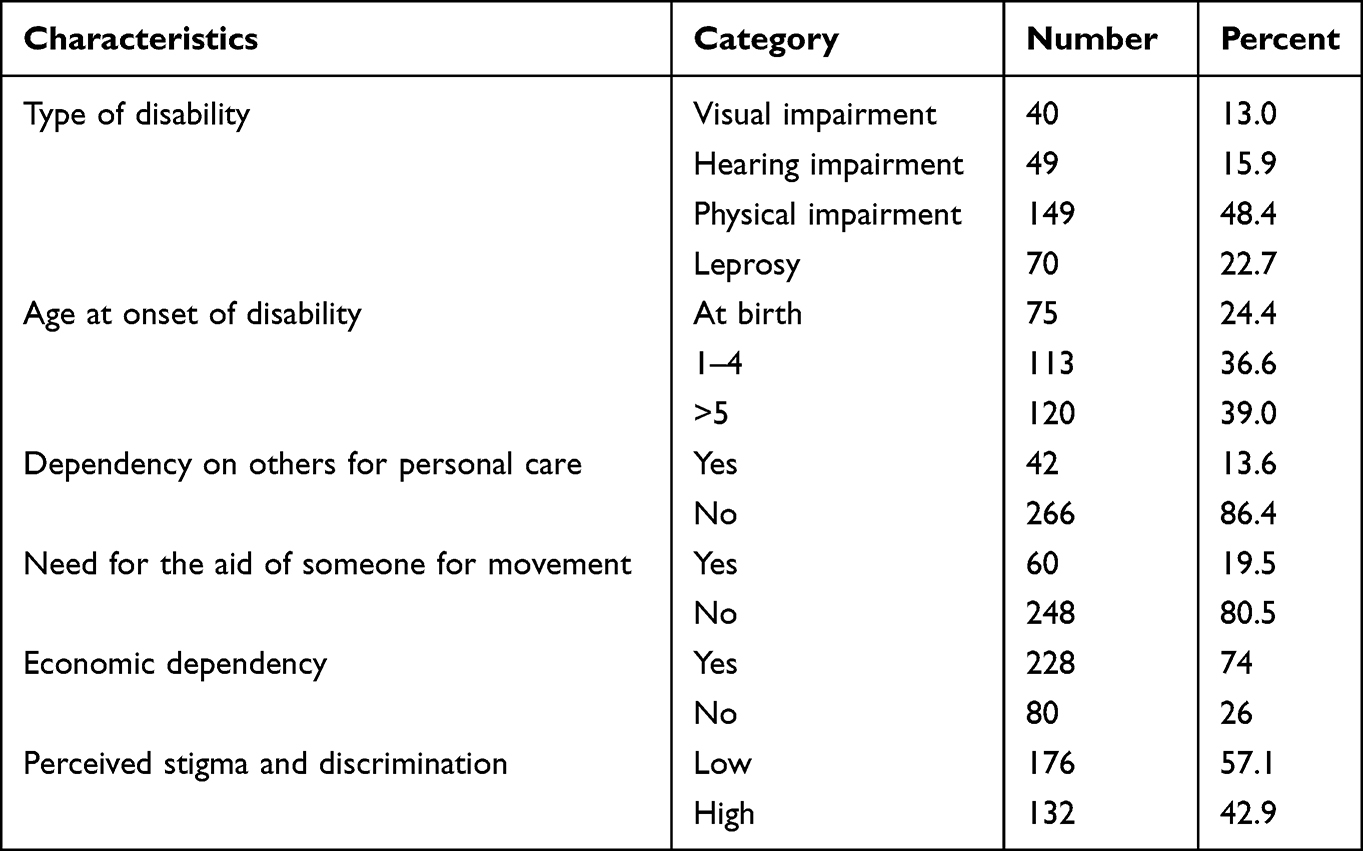 |
Table 3 Disability-Related Characteristics of Women with Disability Aged 15 and Above in Jimma, Ethiopia, 2020 (n=308) |
Substance Use Behavior of the Participants
Concerning their substance use, more than one-third 105(34.1%) of the respondents use at least one substance during their lifetime. 76(24.7%), 38(12.3%), and 5(1.6%) of them reported that they had chewed chat, drank alcohol and smoke cigarette at least once in their lifetime, respectively. Similarly, 69(22.4%), 38(12.3), and 4(1.3) of them reported that they had chewed chat, drank alcohol, and smoked a cigarette at least once in the past 12 months (Table 4).
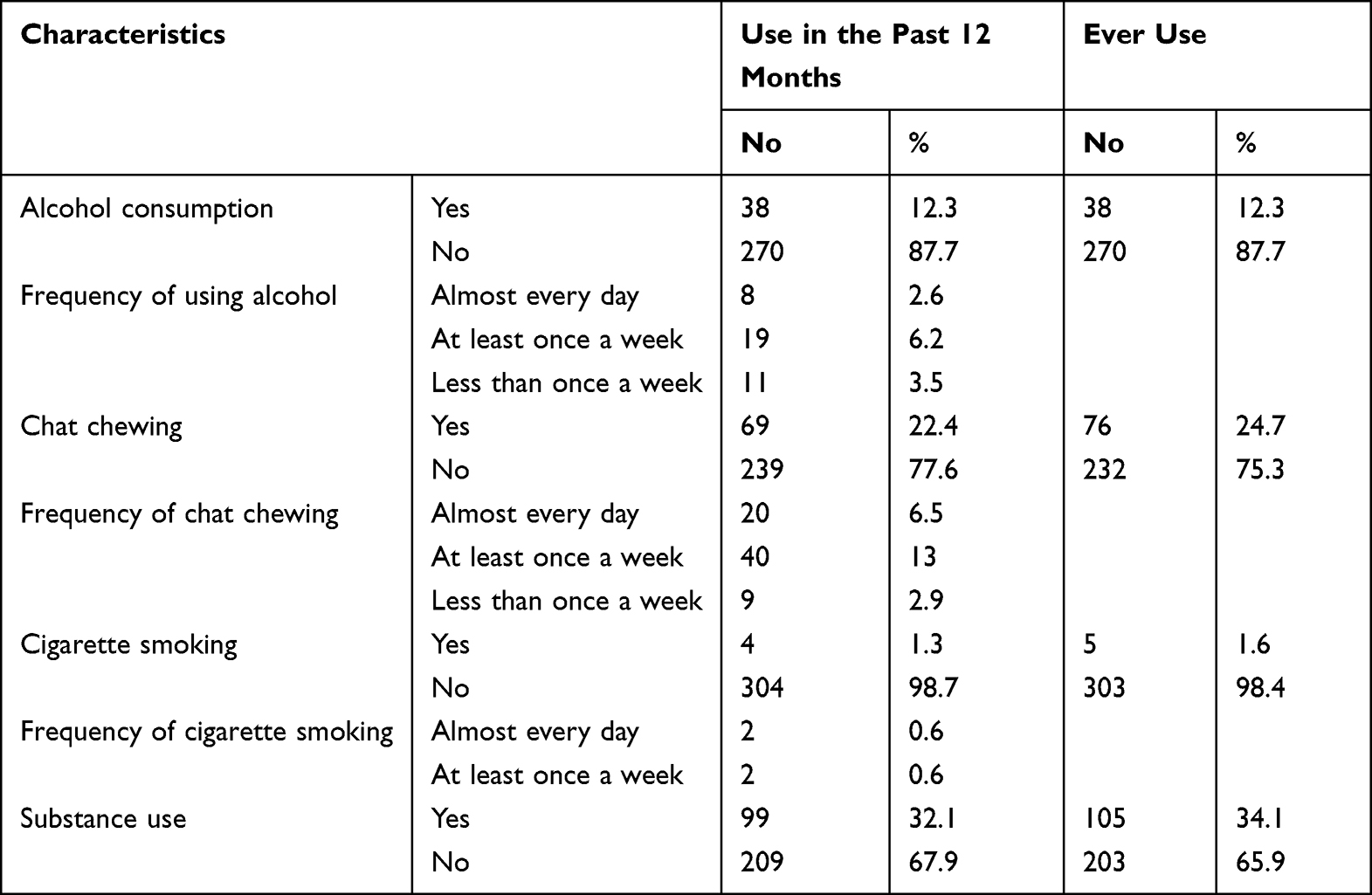 |
Table 4 Behavioral Characteristics of Women with Disabilities Aged 15 and Above, in Jimma, Ethiopia, 2020 (n=308) |
Prevalence and Type of Violence
Type of Gender-Based Violence
Physical Violence
Almost half 50.3% (95% CI: 44.7%, 56.6%) of the women had experienced at least one type of physical violence during their lifetime and 26.6% (95% CI: 21.4, 31.8) of the women had experienced physical violence in the past 12 months.
Emotional Violence
Of all study participants, more than half 57.5% (95% CI: 52.5, 63.1) of the women had experienced at least one type of emotional violence during their lifetime and 34.1% (95% CI: 29.2, 39.3) of the women had experienced at least one type of emotional violence in past 12 months.
Sexual Violence
One-fifth of the women 19.8% (95% CI: 15.5, 24.7) had experienced at least one type of sexual violence during their lifetime and 9.7% (95% CI: 6.5, 13) of the women had experienced at least one type of sexual violence in the past 12 months. The mean age that they were forced to have sexual intercourse for the first time was 17.28 years±4.74 (Figure 1).
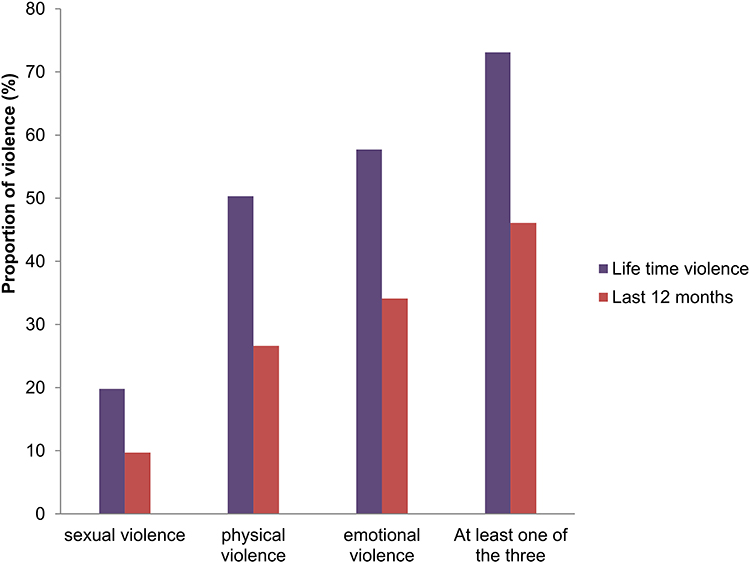 |
Figure 1 The past 12 months and lifetime experience of violence among women with disabilities aged in Jimma, 2020. |
Overlap Between Physical, Emotional, and Sexual Violence
Of all study participants, 7.1% of the women experienced physical violence only, 15.6% experienced emotional only and 3.2% experienced sexual violence only in the past 12 months. While 13.6% of the women experienced both emotional and physical violence, 1.6% and 0.6% of them experienced both physical+sexual and emotional+sexual violence, respectively. Around 4.3% of them reported they experienced physical, emotional and sexual violence at the same time in the past 12 months (Figure 2).
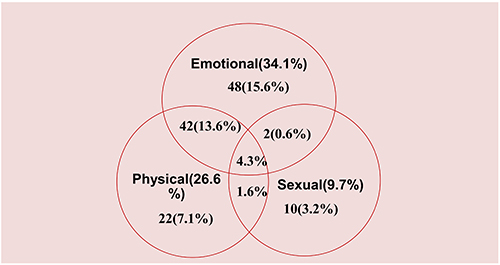 |
Figure 2 Overlap between sexual, physical, and emotional violence among women with disabilities in Jimma, 2020. |
Gender-Based Violence
The occurrences of different forms of gender-based violence were assessed. One hundred forty-two (46.1%; 95% CI: 40.9%, 51.9%) women reported that they had experienced gender-based violence during the last 12 months and the majority 225(73.1%; 95% CI: 68.4%, 78.0%) of the women had experienced gender-based violence during their lifetime (Figure 3).
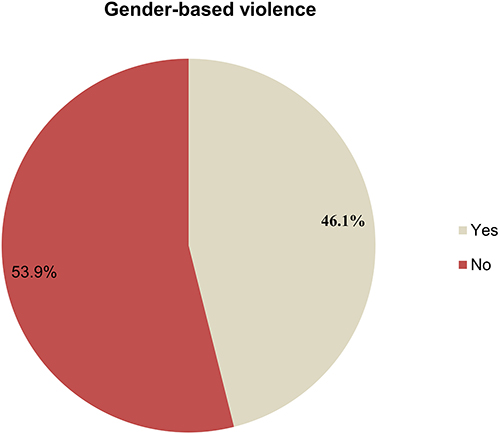 |
Figure 3 The past 12 month’s experience of gender-based violence among women with disabilities aged 15 and above in Jimma town, 2020. |
Overlap Between Before and Within the Past 12 Months of Gender-Based Violence Experience
More than one-third 129(41.9%) of the women had experienced at least one type of violence during their lifetime before 12 months as well as during the past 12 months while 83(27.0%) and 13 (4.2%) had experienced at least one type of violence only during their lifetime before 12 months and only in past 12 months respectively (Figure 4).
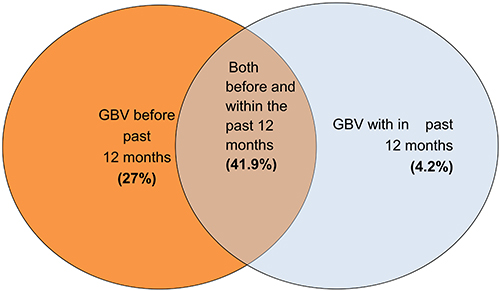 |
Figure 4 Overlap between before and within past 12 months GBV experienced by women with disabilities aged 15 and above in Jimma town, 2020. |
Seeking Care and Support
All women reporting any experience of sexual violence were asked whether and from whom they had sought help. The vast majority (90.2%) of the respondents who experienced sexual violence did not try to seek help from others. More than half of the respondents reported that not knowing where to go (52.7%) and being afraid that others may not believe them (50.9%) were the reasons for not seeking help at the time.
Perpetrators of Gender-Based Violence
Half (50.6%) of women experienced physical violence from family members followed by boyfriends/husbands (48.1%) and other relatives (28.8%). Sexual violence was mostly perpetrated by husbands/intimate partners (39.3%) and other relatives (31.1) while family members (52.2) and husband/intimate partners (33.7) were the main perpetrators of emotional violence (Figure 5).
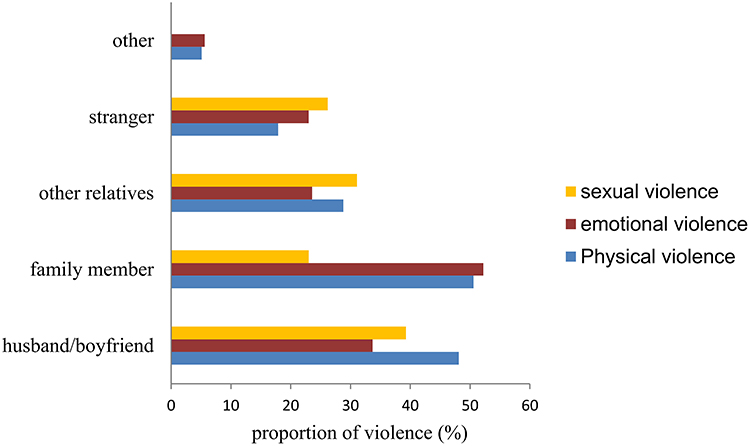 |
Figure 5 Perpetuators of physical, emotional, and sexual violence among women with disabilities in Jimma town, 2020 (multiple responses were possible, “other” includes neighbors and friends). |
Factors Associated with Gender-Based Violence Against Women with Disabilities
Multivariable logistic regression analysis revealed that the age of the women, educational status, alcohol use behavior, type of disabilities, and perceived social stigma and discrimination were found to be independent predictors of gender-based violence against women with disabilities.
Women in the age group 20–34 were 3.5 times (AOR=3.5; 95% CI, 1.74, 7.30) more likely to experience gender-based violence in the past 12 months compared with women aged 35 and above. Women with no schooling were 5.1 times (AOR=5.1; 95% CI, 1.51, 17.14) more likely to experience gender-based violence in the past 12 months compared with women with the educational level of college and above. Women who have visual impairment and hearing impairments were 3.1 times (AOR=3.1; 95% CI, 1.27, 7.54) and 3.0 times (AOR=3.0; 95% CI, 1.36, 6.89) more likely to be violated compared with those who have a physical impairment, respectively. Women who had alcohol use behavior in the past 12 months were 4 times (AOR=4.1; 95% CI, 1.74, 9.55) more likely to experience gender-based violence than their counterparts. Women with high perceived stigma and discrimination were 4.2 times (AOR=4.2; 95% CI, 2.44, 7.39) more likely to experience gender-based violence in the past 12 months as compared with women who had low perceived stigma and discrimination (Table 5).
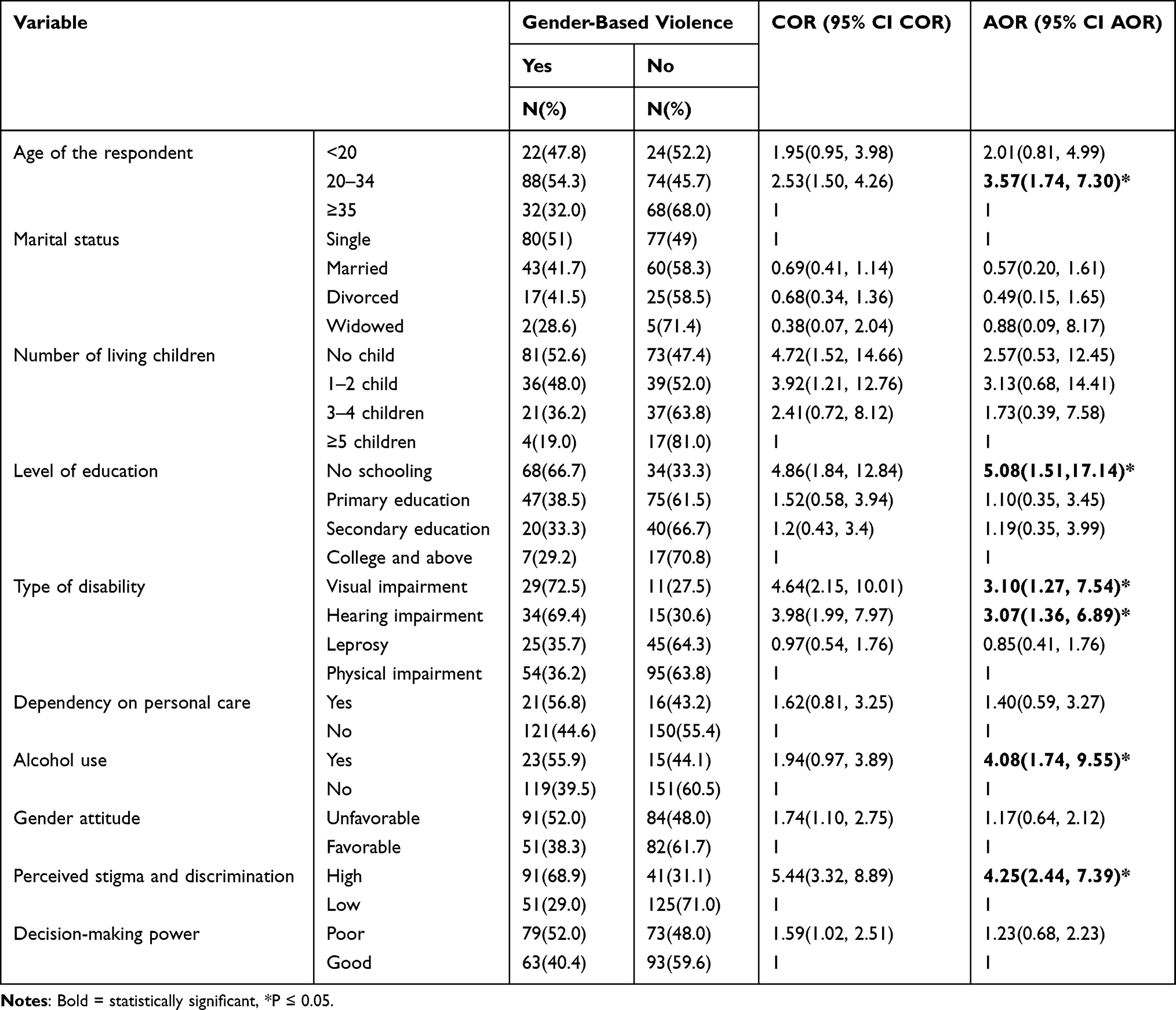 |
Table 5 Multivariable Analysis Showing Factors Associated with Gender-Based Violence Among Women with Disabilities in the Past 12 Months in Jimma, Ethiopia, 2020 |
Discussion
This study determined the prevalence of gender-based violence and associated factors among women with disabilities. In this study, the lifetime prevalence of gender-based violence was 73.1%. The current finding is consistent with a report from a study on women with disabilities conducted in Colombia which stated the magnitude of gender-based violence during a lifetime as 72%.3
The finding of this study is lower than a report from a study conducted in Bangladesh that stated the lifetime prevalence as 84%.21 The variation may be due to the difference in the study area in which the study in Bangladesh encompasses rural and urban areas while the current study includes the only urban area. This might be due to a lack of employment opportunities and having a low income in a rural part of Bangladesh increases their dependence on others and makes them more vulnerable to violence.
However, it is higher when compared with studies conducted in Germany (25–45%), Australia (62%), Nepal (58%), and Uganda (64%).20,22,29,30 This variation might be due to differences in cultural characteristics, socioeconomic status, and the study population. Germany and Australia were a country among highly developed countries with better socioeconomic development; rank 4thand 6th on the United Nations 2019 Human Development Index (HDI) while Ethiopia ranks 173rd out of 189 countries.31 This implies the prevalence can be higher in the current study as women living in poverty were more likely to experience violence though it occurs in all social and economic classes. Also, the difference might be due to the presence of culture and traditional gender norms in which patriarchal societies create privileges for men giving them power over women; in the current study more than half (56.8%) of women had unfavorable gender-equitable attitudes.
The finding of this study showed that the prevalence of gender-based violence in the past 12 months was 46.1%. This finding is lower than a finding from the study conducted in low and middle-income countries and India found that 61.5% and 73% of women had experienced violence in the past 12 months.11,23 The variation might be due to differences in the study area and period. In recent years, there are several activities implemented regarding ending gender-based violence in the country which might have a positive impact on reducing violence. But this finding is consistent with a finding of a study conducted in Nepal that stated the prevalence as 42%.22
This study revealed that women in the age group 20–34 were three times more likely to experience gender-based violence in the past 12 months compared with women aged 35 and above. This finding is supported by studies conducted in Canada, North Carolina, Nepal, and Addis Ababa.7,8,22,32 On the contrary; a study conducted in Bangladesh revealed that older women were more likely to experience gender-based violence as compared to women with disabilities who are younger.21 This variation might be due to the difference in the type of violence. Bangladesh’s study was conducted on IPV only among ever-married women and those older women might be lived longer with their partners and faced violence as compared to young married women. However, the current study includes both intimate and non-intimate partner violence in which younger women were more likely to experience violence as they are dependent on others.
Women with no schooling were five times more likely to experience gender-based violence in the past 12 months compared with women with the educational level of college and above. This finding is supported by a study conducted in North Carolina and India.7,23 This may be since the experience of violence declines sharply with increasing the level of education because as women’s educational level increases they may have access to information; their awareness and struggle for their right against the traditional gender norm will increase and also results in improved interpersonal skill and healthier communicative relationship that prevent the risk of violence. Besides, educated women are more likely to be engaged in occupations that make them economically independent.33 These points toward and confirm the importance of empowering and promoting social and economic inclusion of all, irrespective of sex and disability as recommended by SDGs.
Women who have visual impairment were three times more likely to be violated compared with those who have a physical impairment. This finding is supported by the studies conducted in Denmark and Addis Ababa.8,34 and also the current study showed women with hearing impairment were three times more likely to be violated compared with those who have a physical impairment. This might be since disabilities that require a dependency on others for support are exploited by perpetrators to exercise power and control which increases vulnerability to GBV and the perpetrator regards them as an easy target. Additionally, they might be incapable of defending themselves or might not use opportunities around to escape abusive states.9,35
Those women who had alcohol use behaviour in the past 12 months were four times more likely to experience gender-based violence than their counterparts. This finding is supported by the study conducted in the United States.24 The reason might be because substance use is assumed to impair judgment and ability to recognize and avoid a violent situation which makes them vulnerable to violence.36
Women with high perceived stigma and discrimination were four times more likely to experience gender-based violence in the past 12 months as compared with women who had low perceived stigma and discrimination. This finding is supported by a study conducted in Bangladesh where social stigma against disability makes them vulnerable to intimate partner violence.21 This might be due to the reason that stigma and discrimination support the marginalization of women with disabilities and make women more vulnerable to violence.20
When interpreting the finding of the present study, the following limitations should be considered; the magnitude of violence might be underestimated since the study deals with a sensitive issue under-reporting is inevitable (social desirability bias). However, privacy was maintained by interviewing them alone and the data collectors were females to minimize social desirability bias. On the other hand, there could be a recall bias. However, recall bias ought to be less in the studies of such serious life-threatening experiences. Additionally, an attempt was made to reduce the bias by asking about their past12 months’ experiences in addition to their life experience. Moreover, it is difficult to show the cause and effect relationship as it is a cross-sectional study.
Conclusion
This study revealed that the prevalence of gender-based violence among women with disabilities was high. Independent predictors of gender-based violence against women with disabilities were the age of the women, educational status, alcohol use behavior, type of disabilities, and perceived social stigma and discrimination. Addressing such determinants will require multi-sectoral interventions. So, taking integrated interventions like increasing the school enrollment of young girls with disabilities and targeted health education towards identified factors by considering the heterogeneity of disabilities will help to curb the problem.
Abbreviations
IPV, intimate partner violence; GBV, gender-based violence; SDGs, Sustainable Development Goals; WHO, World Health Organization.
Data Sharing Statement
The dataset for the current study is available from the corresponding authors on reasonable request.
Ethics Approval and Consent to Participate
The study was ethically approved by the institutional review board (IRB) of Jimma University. Written informed consent was obtained before the interview. For minors (<18 years), written informed consent from their parent/legal guardian and assent from the children was obtained. Their right not to participate, not to answer any or all questions, and to withdraw from the interview at any time they want was respected and this study was conducted per the Declaration of Helsinki.
Acknowledgments
We express our heartfelt thanks to all individuals who participated in the study: respondents, data collectors, and Jimma University for funding the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research work was funded by Jimma University. The funders had no role in study design, data collection, and analysis, decision to publish, or preparation of the manuscript.
Disclosure
The authors declare no competing interests in this work.
References
1. World Health Organization and World Bank. World report on disability. Geneva, Switz; 2011: 69.
2. Katsui H, Mojtahedi MC. The intersection of disability and gender: multi-layered experiences of Ethiopian women with disabilities. Dev Pract. 2015;25(4):563–573. doi:10.1080/09614524.2015.1031085
3. Ortiz D, Urban A. Violence Against Women and Girls with Disabilities, Latin America and the Caribbean. Gender and Diversity Division, Inter-American Dev Bank; 2019.
4. Campos Pinto P. Out of the shadows: violence against girls and women with disabilities in Portugal. Alter. 2016;10(2):137–147. doi:10.1016/j.alter.2016.03.009
5. International Network Of Women With Disabilities(INWWD). Violence against women with disabilities; 2010: 4–8. Available from: http://wwda.org.au/wp-content/uploads/2013/12/inwwdviol2010.pdf.
6. UN general assembly. General situation of women and girls with disabilities and the status of the convention on the rights of persons with disabilities and the optional protocol thereto; 2017.
7. Sandra LM, Neepa Ray LLK. Physical and sexual violence of women with disabilities. Violence Against Women. 2010;12(9):823–837.
8. Sebisbe N. Gender-Based Violence and Adverse Reproductive Health Outcomes Among Women with Disabilities in Selected Associations of People with Disabilities in Addis Ababa, Ethiopia [master’s thesis]. Addis Ababa University; 2011. Available from: http://etd.aau.edu.et/handle/123456789/12199.
9. Dessie S, Bekele Y, Bilgeri M. Sexual violence against girls and young women with disabilities in Ethiopia. Including a capability perspective. J Glob Ethics. 2019;1–19. doi:10.1080/17449626.2019.1690554
10. Hughes K, Bellis MA, Jones L, et al. Prevalence and risk of violence against an adult with disabilities_Systematic Review. Lancet. 2012;379(9826):1621–1629. doi:10.1016/S0140-6736(11)61851-5
11. Dunkle K, Van Der Heijden I, Stern E, Chirwa E. Disability and violence against women and girls: what works to prevent violence against women and girls global programme; 2018: 1–6.
12. Mahider M. Gender-Based Violence, Women with Disabilities and Access to Justice: Ethiopia and Kenya. Central Eur Univ; 2015:1–112.
13. World Health Organization (WHO). Global Status Report on Violence Prevention. Geneva, Switzerland: World Health Organization; 2014.
14. Khalifeh H, Howard LM, Osborn D, Moran P, Johnson S, Bayer A. Violence against people with disability in England and wales: findings from a National Cross-Sectional Survey. PLoS One. 2013;8(2):1–9. doi:10.1371/journal.pone.0055952
15. UNAIDS. Disability and HIV; 2017: 1–10. Available from: http://www.unaids.org/sites/default/files/media_asset/JC2905_disability-and-HIV_en.pdf.
16. Del Río Ferres E, Megías JL, Expósito F. Violencia de género en mujeres con discapacidad física y visual. Psicothema. 2013;25(1):67–72. doi:10.7334/psicothema2012.83
17. United Nations. Optional protocol to the convention on the rights of persons with disabilities(adopted December 13, 2006) UNGA Res 61/611. Dev. 2006;49(4):158–160.
18. UNDP. Report of the Inter-Agency and Expert Group on sustainable development goal indicators (E/CN.3/2016/2/Rev.1); 2016.
19. Krnjacki L, Emerson E, Llewellyn G, Kavanagh AM. Prevalence and risk of violence against people with and without disabilities: findings from an Australian population-based study. Aust N Z J Public Health. 2016;40(1):16–21. doi:10.1111/1753-6405.12498
20. Schröttle M, Glammeier S. Intimate partner violence against disabled women as a part of widespread victimization and discrimination over the lifetime: evidence from a German representative study. Int J Conf Violence. 2013;7(2):232–248.
21. Hasan T, Muhaddes T, Camellia S, Selim N, Rashid SF. Prevalence and experiences of intimate partner violence against women with disabilities in Bangladesh. J Interpers Violence. 2014;29(17):3105–3126. doi:10.1177/0886260514534525
22. Puri M, Misra G, Hawkes S. Hidden voices: prevalence and risk factors for violence against women with disabilities in Nepal Health behavior, health promotion, and society. BMC Public Health. 2015;15(1):1–11. doi:10.1186/s12889-015-1610-z
23. Deepak S, Kumar J, Santhosh B, et al. Violence against persons with disabilities in Bidar district, India. Disabil CBR Incl Dev. 2014;25(2):35–53. doi:10.5463/dcid.v25i2.305
24. Alriksson-Schmidt AI, Armour BS, Thibadeau JK. Are adolescent girls with a physical disability at increased risk for sexual violence? J Sch Health. 2010;80(7):361–367. doi:10.1111/j.1746-1561.2010.00514.x
25. Vidojević IM, Tošković O. Experienced and anticipated discrimination in persons with physical disabilities in Serbia. Eur J Interdiscip Stud. 2017;3(2):65–74.
26. Chung EYH, Lam G. Validation of two scales for measuring participation and perceived stigma in Chinese community-based rehabilitation programs. Health Qual Life Outcomes. 2018;16(1):15–20. doi:10.1186/s12955-018-0938-3
27. World Health Organization (WHO). WHO multi-country study on women’s health and domestic violence against women; 2014 [cited January 29, 2020]. Available from: http://www.cih.uib.no/journals/EJHD/ejhd17-special-issue-2/ejhdv17-specialissue-2-2003-cover.html.
28. Semahegn A, Torpey K, Manu A, Assefa N, Aankomah A. Adapted tool for the assessment of domestic violence against women in a low-income country setting: a reliability analysis. Int J Women’s Health. 2019;11:65–73. doi:10.2147/IJWH.S181385
29. Valentine A, Akobirshoev I, Mitra M. Intimate partner violence among women with disabilities in Uganda. Int J Environ Res Public Health. 2019;16:6. doi:10.3390/ijerph16060947
30. Dowse L, Soldatic K, Spangaro J, Van Toorn G. Mind the gap: the extent of violence against women with disabilities in Australia. Aust J Soc Issue. 2016;51(3):341–359. doi:10.1002/j.1839-4655.2016.tb01235.x
31. United Nations Development P. Human development report [Internet]; 2020. Available from: http://hdr.undp.org/sites/default/files/hdr2019.pdf.
32. Yoshida K, Dumont J, Odette F, Lysy D. Factors associated with physical and sexual violence among Canadian women living with physical disabilities. Health Care Women Int. 2011;32(8):762–775. doi:10.1080/07399332.2011.555826
33. Weitzman A. Does increasing women’s education reduce their risk of intimate partner violence? Evidence from an education policy reform. HHS Public Access. 2019;56(3):574–607.
34. Dammeyer J, Chapman M. A national survey on violence and discrimination among people with disabilities. BMC Public Health. 2018;18(35):1–9. doi:10.1186/s12889-018-5277-0
35. Dockerty C, Varney JJR. Disability and domestic abuse risk, impacts and response. Public Heal Engl. 2015;2015:11–13.
36. Kilpatrick DG, Acierno R, Resnick H, Best C. A 2-year longitudinal analysis of the relationships between violence and substance abuse in women. Consult Clin Psychol. 1997;65(5):1–45.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.