")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 10
Future challenges for occupational health services can be prevented by proactive collaboration with the companies using the services: a participatory and reflection project
Authors Lydell M, Hildingh C, Söderbom A, Ziegert K
Received 30 December 2016
Accepted for publication 26 April 2017
Published 24 May 2017 Volume 2017:10 Pages 217—225
DOI https://doi.org/10.2147/JMDH.S131382
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Marie Lydell,1 Cathrine Hildingh,1 Arne Söderbom,2 Kristina Ziegert1
1Center of Research on Welfare, Health and Sport (CVHI), School of Social and Health Sciences, 2Center for Innovation, Entrepreneurship and Learning Research (CIEL), School of Economics, Technology and Science, Halmstad University, Halmstad, Sweden
Background: There is clearly a need for research in the field of occupational health service (OHS) for applying new perspectives. Proactive collaboration is needed between the OHSs and the companies. The customers of the companies using the services should be able to safeguard themselves from the health problems caused by the work environment through proactive collaboration with the OHSs.
Objective: The main purpose of this interdisciplinary study was to explore how the stakeholders reflected to create and agree on core values for future challenges in OHS, as seen from the perspectives of OHS professionals and customer companies.
Methodology: An action research process was conducted. This study was divided into three phases. In phase I, the data were collected from interviews and diaries of interdisciplinary occupational health professionals (n=12). A focus group that sampled the eight managers of the customer companies was also included. In phase II, a questionnaire was developed with 24 questions focusing on examining the future challenges for OHS. The questionnaire was sent to customer companies (n=116). In phase III, a scoping review was undertaken.
Results: Three categories emerged from the analysis: “Balancing complex situations” clarified the complexity regarding senior employees; “Working with a proactive approach” indicated the need for working with a new proactive approach supporting sustainable health; and “Collaborate internally and externally” showed good relationships between the customer and the OHS, which is a mutual responsibility to both the partners.
Conclusion: The results outlined that it is necessary to take action to apply new proactive health promotions, with a focus on workplace health promotion. The results also indicated that interventions for senior employees are of importance. This study was done in collaboration with the stakeholders from the occupational health care service center and the managers from the customer companies. The use of a participatory research design, including close collaboration with the participants, allows the researchers to see the challenges.
Keywords: health-promoting workplace, managers, future challenges, participatory approach, senior workers
Introduction
Occupational health services (OHSs) of today face several important and complex challenges. Some challenges are related to the understanding of the health concept, while others concern the organization of OHSs.1 The modern OHS is supposed to be multiprofessional and customer-oriented but seems foremost to be driven by a traditional pathogenic biomedical agenda,1 with a primary focus on preventing disease (pathogenic perspective) rather than promoting positive measures of health (salutogenic perspective).2 A salutogenic perspective is to be used as a guide for health promotion because it highlights opportunities and identifies resources instead of focusing on risk factors for diseases. To meet these challenges in occupational health, it is vital to draw attention to health promotion built on a salutogenic perspective.3 The organization of OHSs is also important to take into account. The process of OHS can be seen as a transition in the workplace-oriented health programs for helping people cope with social, emotional, and physical conditions.1,4 However, the majority of studies until today have not focused on changing the workplace, which is a limitation.5 Workplace health promotion (WHP) has been defined as “the combined efforts of employers, employees and society to improve the health and well-being for people at work”.6 The major role of a good organizational climate at a workplace has been found as an occasion for supporting the employee’s well-being at work in a salutogenic way.7
Other challenges focus on the very quick increase of the elderly population, addressed to the labor market.
Sweden confronts, such as many other countries, a demographic “time bomb” in the form of an ever-increasing elderly population8 resulting in a need for strategic changes in the institutional health care arrangement. Employees are expected to work longer, which demands strategic changes in the institutional health care arrangement.9 Senior employees often have a good idea themselves about what they want when it comes to their health. This requires different innovative health care logic methods,10 other than what traditionally are offered in order to meet different customer situations.11,12
The challenges described above address both theoretical and practical gaps in the current understanding of OHS and suggest that the field needs further research. Therefore, the main purpose of this interdisciplinary study was to explore how the authors reflected with the stakeholders to create and agree on core values for future challenges in the OHS seen from the perspectives of OHS professionals and customer companies. The purpose was also to describe what components were important for OHS in a scoping review.
Methods
Participants and settings
This study is based on participatory and reflection approach.13 Action research is characterized by stakeholders who participate and work together with researchers to create knowledge about problems in practice in order to develop practical knowledge.
The particular occupational health service center (OHSC) is a part of a bigger OHS limited, which owns one-fourth of all OHSCs in Sweden. In Sweden, there are three big owners of occupational health centers and also some small private centers. This study included a three-phase process; the first phase included collecting qualitative data from diaries and interviews with occupational health professionals in the OHSC in southwest Sweden as well as focus groups, interviewing the managers of the customer companies affiliated to the OHSC. The second phase was a quantitative part with a questionnaire to managers of the customer companies. Finally, the third phase was a scoping review of research on occupational health.14
The occupational health professionals included seven health care professionals: a physician, two occupational nurses, a physiotherapist, a social worker, a psychologist, and a nurse assistant. There was also the vice director and a secretary.
In this collaborative and interdisciplinary study, stakeholders who participated from OHS served a total of 160 companies with a total of 3,600 employees, in the area of industry, trade, and services, and were affiliated to the local OHS.
This study was supported by the Knowledge Foundation and has undergone a review process for identifying ethical issues (KKS dnr 20130309). Ethical permission was not required because the questions were not of a sensitive nature. However, the ethical issues were reflected on, and harm was minimized. The autonomy and integrity of the study persons were respected, the principles were followed in line with the Declaration of Helsinki, and the participants were assured of the confidentiality of the collected material.15 Written information about the project was sent to the participants of the study (occupational health care professionals and managers of the customer companies). Participation in the study was voluntary and could be discontinued at any time. Before the beginning of individual and focus group interviews, written and verbal consent was obtained from all the participants of the research project. All the collected material was treated according to the Swedish law of personal particular data (Personuppgiftslagen, 1998:204). Therefore, the data material was coded with non-identifiable codes and was locked in cabinets, and only the researchers had access to the data.
Data collection and data analysis
Phase I
Interviews with occupational health care professionals
All multiprofessional persons from the OHSC were interviewed individually (n=9). The professionals included the vice director, one physician, two occupational nurses, one physiotherapist, one social worker, one psychologist, one nurse assistant, and one secretary. The semi-structured questions dealt with their own role in the OHSC, future challenges and goals, and processes for achieving these goals. They were also asked to describe their view of health promotion at work. The interviews lasted between 45 and 60 minutes, and notes were written down during the interviews.
Diaries written by occupational health care professionals
All occupational health care professionals were asked to write down the experiences and thoughts of their daily work at the OHSC in a logbook. The logbooks were written during one year and collected by the researchers three times during this year. On these occasions, short seminars (Figure 1) were held with the staff where they had the opportunity to discuss important issues and also how they felt writing down the experiences and reflections of their daily work on a regular basis.
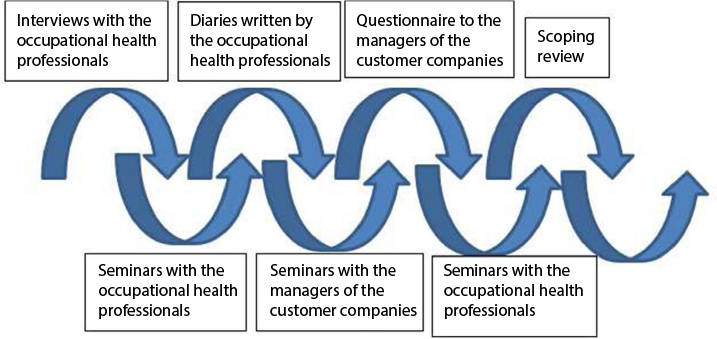 | Figure 1 Ongoing action-process. |
Focus group interviews with managers of the customer companies
Eight managers from the customer companies affiliated to the OHSC participated in two focus group interviews. The focus groups were strategically selected based on business branch. Eight managers were representing bank office, engineering, automotive, economist in vehicle industry, builders company, social insurance, service company, and food industry respectively. The questions dealt with, and managers reflected on, the following theme: customer role, dialogue with the OHSs, future challenges, workplace health, health promotion leadership, and elderly persons within the company. The interviews with the focus groups lasted for ~1 hour per session.
The data from the diaries and the interviews with occupational health professionals and focus group interviews with managers were analyzed using inductive qualitative content analysis.18 First, the text was read several times to comprehend the whole picture of the data. Second, the text units relevant to the aim were identified and open-coded. While rereading the codes, categories emerged, and each text unit was retested for accuracy to be classified under the respective categories. The analysis was validated by discussions in a cross-professional group consisting of four people (two nurses, one physiotherapist, and one economist). Throughout data analysis, several meetings between this cross-professional group took place to discuss categories until a consensus was met. After data analysis, translation into the English language was carried out. Quotations from different informants were also chosen to illustrate the findings.
Phase II
A questionnaire was developed based on interviews with the focus groups including managers of the customer companies. The think-aloud method was used to validate the questionnaire.16,17 Six persons with insight in business companies participated in the validation, which resulted in minor revisions of the questionnaire.
The questionnaire consisted of 24 statements and three open questions about today’s OHSs, health promotion work, and future challenges. The questionnaire was sent to the managers of the customer companies, which were randomly selected (n=116).
Descriptive statistics including frequency, mean, median, and percentage were used to summarize the data. The companies affiliated to OHSC consisted of few employees, and hence, they were divided into three groups: 1–10, 11–50, and more than 50 employees. To determine the differences between the companies, independent samples t-test was used. P values <0.05 were considered statistically significant. SPSS version 20 (IBM Corp., Armonk, NY, USA) was used to run statistical analysis.19 The questionnaire was answered by 61 managers (53%).
Phase III
Literature review
A scoping review of the literature was conducted14 to explore the components important for OHS. Databases such as PubMed, ABI Inform, and Academic Search Elite ASE were searched for articles. The following keywords and combinations of keywords were used in PubMed and modified for other databases when appropriate:
(“Occupational health service” OR “customer”) AND (Exp*) AND (Care taker) AND (“Health promotion”) published from 2010 to February 2015
(“Workplace health” OR “customer” OR “Care taker”) AND (Exp*) AND (Health promotion) AND (perception) published from 2010 to February 2015
The keywords were also searched as free text in the databases. The search was limited to English-language articles in all databases with the keyword “Occupational health service”. Inclusion criteria were occupational health and results based on caretakers’ perception of workplace health. The articles focusing on health care professionals’ perspective, illness perspective, and specific diseases such as cancer were excluded.
The search with the keywords “occupational health service” and “workplace health” in combination with exp* AND perception with the keyword “customer” generated a total of 309 references. However, after removing duplicates, 123 references remained. The titles were read, and 62 appeared to be relevant to the aim. The articles that were excluded based on their titles focused on illness perspective, body image, inpatient care, and specific diseases. Then, the abstracts were read, and 45 articles were included. Those excluded focused on illnesses, dietary program for diabetes mellitus, specific disease, psychiatric illnesses, and cognition. Finally, these 45 articles were read in full text, and 17 were included (Figure 2).
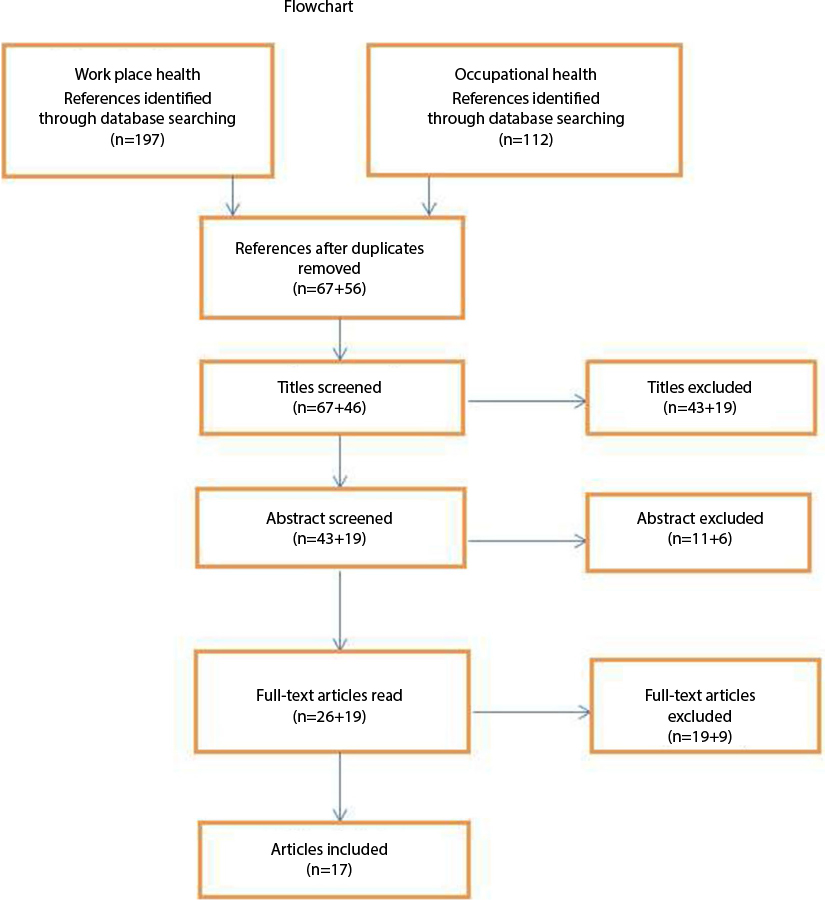 | Figure 2 Flow chart over literature search. |
The literature was analyzed by extracting and summarizing all the data relevant to the aim of the study by using a matrix including information, such as authors, years of publication, country, journal, aim, overview of method, important factors for occupational health, and OHS. When analyzing the literature data, the categories developed from the qualitative content analysis (stage 1) were used to sort the data.
Results
Results from the diaries, individual interviews, focus group interviews, the questionnaire as well as the literature review are presented in three categories regarding experiences and important components of OHSs and their future challenges. The categories were developed inductively from statements from occupational health professionals as well as from managers of the affiliated companies. The emerged categories were “Balancing complex situations”, “Working with a proactive approach”, and “Collaborate internally and externally”.
Balancing complex situations
The literature points out some complex situations to balance in the workplace and shows that there are different ways to handle these situations.20 Higher-rank employees tend to see the challenges they face at work as being in their own expectations of how they and their colleagues should make use of their time. Lower-rank employees, on the other hand, tend to see themselves as being in their prescribed jobs and others’ expectations of them.
To work in an OHSC involves handling and balancing complex situations in relation to employees as well as to employers. Loyalty to the employees versus the companies’ beneficial interests may cause severe moral conflicts for the occupational health care professionals. To be loyal to the employee can imply disloyalty to the employer. One of the occupational nurses (female) said:
To stand on the employee’s side may cause a moral conflict. There must be a balance in my loyalties. [Interview 1]
The results of the questionnaire answered by the employers also showed that OHSC was perceived to be loyal to the company customers (n=34), but sometimes they implied that OHSC took the employees side instead of the work management (n=33).
The occupational health professionals were of the opinion that employers were not always conscious of their responsibility towards employees and that the company culture was a hindrance for an effective OHS. This was sometimes difficult to balance for the occupational health professionals.
In relation to the ages of the employees, there may also be further complex situations to balance. For example, employers described that young employees’ attitudes to “short sick leave” have changed over time and many young employees do not care about their health. They live a sedentary and unhealthy life which influences their working capacity; they do not exercise, and in many cases, do not eat breakfast before coming to work. This was described by the employers as a complex situation in today’s working life that had to be dealt with, which meant that the young employees, in some cases, almost have to be brought up by the employers. When it comes to the senior employees, the employers described that several persons are stuck in old habits which can be difficult to deal with at the workplace. Furthermore, the literature pointed out that work-related values differ between generations and have to be considered.21,22 The increase of senior workers also put other demands on the OHSs, as they may have difficulties to manage the rapid development in many areas. The results from the questionnaire further showed that the managers of the companies (n=33) wanted to stimulate the employees to work after the age of retirement and they were also of the opinion that OHSC, in collaboration with their company, could create a health-promoting workplace for senior employees (n=32). To motivate aging employees to stay longer at work is one of the greatest challenges of this decade, according to literature concerning human resource managers. If a growing number of senior employees retire from their jobs, organizations will face strong challenges in terms of finding replacement workers and preventing knowledge loss.23,24
The results of the questionnaire also showed that independent of ages, psychosocial problems among employees have increased which requires great efforts from OHSs. Half of the managers who answered the questionnaire were of the opinion that OHSCs were good at supporting the employees’ psychosocial problems and do not ignore these complex situations.
Also, research results have confirmed that psychosocial problems in a working population are highly prevalent and often result in further deterioration of mental health and consequently absence from work. Therefore, the OHS needs to evaluate health promotion programs to reduce psychosocial problems among employees.25,26
Another complexity in OHSs is the lack of time for the health professionals to perform their tasks. The occupational health professionals described, in the diaries, a stressful working situation exemplified by how they must undertake their daily work without necessary reflections. This was experienced as a difficulty to deal with. The social worker (female) from the OHSC said:
Our work requires reflection but it is tangible work without reflection. [Interview 3]
New complex contracts with the affiliated companies also cause problems for the occupational health professionals and constitute further stressful situations to handle.
Working with a proactive approach
There are increased requirements of OHSC from the customer companies which call for more flexibility regarding the range of services. They wanted new professionals to be employed in the OHSC and more external activities such as lectures given at their company. They suggested replacing some of the professionals at the OHSC and instead employing, for example, health coaches. A manager of the customer companies from a bank office (male) said:
Important that there are many different professionals in the OHSC. [Focus group 1]
Managers of companies with more than 10 employees were of the opinion that the OHSC should adjust the range of services more after the company’s needs (p=0.008). They were also of the opinion that the OHSC could be better in helping them with the challenges their company faces (p=0.016). Twenty-seven managers thought that the OHSC was open for change regarding its services.
They also pointed out that the OHSC is left “in the old” and that there is a lack of innovation within the OHSC. However, the occupational health professionals themselves meant that they were innovative and have changed direction, for example, from health examinations to a more proactive work.
Moreover, the result of the questionnaire showed that all the managers felt that it was important to promote employees’ health and not only prevent disease (n=40), and 26 managers felt that the OHSs can work more with health promotion. In the literature, health promotion in workplaces was described as a process of enabling employees to increase control over determinants of health, thereby improving their health. Work health promotion needs to include positive health measures and settings approaches in intervention programs,27–31 such as mindfulness at workplaces, which has shown positive effects on job performance.32 It was also described how important it is to anchor health promotion among stakeholders by arguing that sustainable production is dependent on employees’ health.27 Job and personal resources are described as the main predictors of engagement, and engaged employees proactively change their work environment in order to stay engaged.33 The resources gain their salience in the context of high job demands. Job design theory as well as job crafting theory was found to be helpful in recognizing the value of employees’ proactivity at work.20,34
Collaborate internally and externally
There were 29 managers who were of the opinion that the OHSC should collaborate more with external partners, such as primary health care centers and wellness companies.
In addition, the occupational health professionals wanted to work more, and in a different way, with external partners strengthening their operation. They were aware of the fact that collaboration with external partners was necessary to avoid OHSC from becoming its own small oasis. A manager of the customer companies from a service company (female) said:
Sometimes there is routine in the collaboration with others and then there is a need for retakes. [Focus group 2]
They also pointed out how important it is to listen to the customers’ wishes and identify their needs in a better way. Some of the customer companies wanted extended information about the services available; however, 34 of the managers were of the opinion that the health professionals informed about their services in a good manner. They wanted better communication with the OHSC and more education regarding work environment. They also pointed out how important it is that the health professionals visit the companies for meetings and discussions with the employees more often. One study in the literature review showed that there are benefits for the companies when they invest in the workplace health and implement comprehensive strategies. In particular, involving external stakeholders is important and could improve the quality and conditions of working life. They could be an integral part of management practices and daily working life at all levels of an enterprise.35
The occupational health care professionals in the OHSC sometimes had strained external collaborations, and their meetings with the affiliated companies were experienced as frustrating. However, if the collaboration was good, it was easier to handle even acute situations. Good relationships between the customer and the OHSC were seen as mutual responsibility according to both the partners.
In the literature review, the recommendations of one study for implementation of an occupational health guideline included the formation of a linkage group, collaboration with other experts, formations of peer support groups, and communicating benefits of investments, expectations, and ethical considerations.36
Discussion
This study contributes to novel perspectives of future challenges for OHS.
The OHS is facing several complex situations as well as the managers at the customer companies. The results showed, both via the professionals at the OHSC and via the managers at the customer companies, that there was a different complexity regarding younger and older persons at workplaces. This result is in line with the studies of Parry and Urwin and Schullery, which concluded that different generations have different work-related values.21,22 Furthermore, the young ones had to learn to be at work in time, and some of them also had to learn to sleep well and eat breakfast before starting work. The elderly working population had other difficulties, such as new technical elements, and they sometimes needed more time when doing their working tasks. Today, there is an increasing older population, and some would probably work longer than retirement9 and that was also something that the managers of the companies both hoped for and encouraged. Therefore, it is of importance to plan for senior workers before they are at the age of retirement. As the managers in the study stated, the OHS must be aware of this and promote health and create a health-promoting workplace for future senior workers, maybe with inspiring new knowledge regarding difficulties they may experience at work as well as promoting occupational self-efficacy which is shown to predict job satisfaction and intrinsic job motivation.37,38 This was also what the managers at the customer companies wanted the OHSC to do. Organizational stimulation and work motivation, as well as the various job characteristics, was positively related to the employees’ willingness to continue working,38 and this must be an important information for the managers at the customer companies. According to Inceoglu et al who examined age-related differences in work motivation, the OHS must have a more reflected attitude to older workers and the age-related changes in motivational variables.24
Another complexity to be balanced was the increasing psychosocial problems, and this is a challenge for the OHS, as well as the managers at workplaces, to handle. The results from the questionnaire showed that the managers at the customer companies were satisfied with the OHSCs way of supporting the employees’ psychosocial problems, but it is still important that the OHS evaluates health promotion program to reduce psychosocial problems among employees.25,26 These problems could otherwise result in long-term sick leave with high costs for the companies. Persons on sick leave often have problems when returning to work,39 and therefore, it is of importance to put more emphasis on promoting health and not act only when symptoms of disease exist.
The managers at the customer companies implied that the OHSC is stuck in old habits and has to change and be more proactive, quite the opposite of what the professionals themselves thought. Bringsén et al showed that occupational health in general must focus more on health promotion.3 To work with health promotion with a salutogenic approach can be the future for OHSs. However, health promotion at workplace and a salutogenic concept may have crucial roles, and this concept can be a huge challenge for academic public and vocational practitioners if they have economic demands.40 As the results from both the interviews and the questionnaire pointed out that health promotion is an important proactive approach, the OHS has to change focus. There is a need for more health promotion interventions, and maybe, focusing on the senior workers is most important now. In this case, the senior workers must be involved in the planning of interventions, and they should be asked about what interventions they would prefer for their well-being at work. Managers at workplaces have to take the responsibility, and they need to include work environment and organizational factors in their work, and therefore, integration with OHS is needed.5,27,41
To collaborate more with the OHSC, and other health organizations, was also a suggestion from managers in this study. Primary health care could be a collaborative partner, and to work together with wellness companies could be one solution. The occupational health professionals were also aware of the fact that collaboration with external partners was necessary to avoid OHSC from being its own small oasis. No development can be made without input from other companies in a similar branch.42 As studies have shown, external stakeholders could be invited in order to improve the quality and conditions of working life.5,35
It is important that the OHSC is listening to the customers’ wishes and the managers are also called for more and better communication, and this must be in a good atmosphere. To be clear and have a direct communication is of importance in order to avoid misunderstandings.43 The OHSC also has to be available for the customers and should possibly have more planned meetings.44 They pointed out how important it is that the occupational health professional visit the companies more frequently for meetings and discussions with the employees. This can be in a salutogenic approach making employees feel involved and included.3 The managers wanted more education regarding work environment, and this is something that the OHSC should develop. In the future, the workplace managers and OHSC could work together more intensively with person-centered health in the education program.45 Regarding the work environment, it is the managers’ responsibility to plan for a successful workplace, but the OHSC could also assist with this. Making a healthy workplace needs a health-promoting leadership, although it is also the employees’ responsibility.46 Good teamwork, with good leadership, is a challenge that needs further collaboration between the customer companies and the OHSC.
Strengths and limitations
This study could have been done with different methods used separately. However, the aim was to explore and reflect, and this required a collaboration of methods and participation of both professionals from OHS and managers from customer companies. The authors chose to conduct the action research process in three phases to collect data in order to gain a deeper understanding of the problem and its context. In the first phase, the analysis and reflection were conducted twice. The qualitative part was the first phase, and the questionnaire was developed based on interviews with the focus groups including managers of the customer companies. The quantitative part was built from the managers’ experiences which could be seen as a strength of this study. However, only 53% of managers answered the questionnaire. The companies were rather similar in their size, which could be a limitation; however, there was a big variation regarding the type of branches, and this is a strength in the study. The literature search with the keywords “occupational health service” and “workplace health” resulted in a limited number of references despite workplace health being an important term globally. This might be because research within “work health” more often includes working people in a general perspective. The studies included samples from various groups with both similarities and multidisciplinary working contexts.
Conclusion
The future challenges of OHSCs seen from the perspectives of interdisciplinary occupational health care professionals and customer companies and from research literature included balancing complex situations, working with a proactive approach, and collaborating internally and externally. The results suggested that it is important to stimulate the employees to work after the age of retirement, and the managers wanted to create a health-promoting workplace for senior employees in collaboration with the OHSC. Furthermore, the managers were of the opinion that it is important to promote the health of their employees and not only prevent disease; that is, they wanted to work in a salutogenic approach. The occupational health professionals were also aware of the fact that collaboration with external partners was necessary to avoid OHSC from being its own small oasis, which was also the managers’ opinion. These future challenges must be discussed and resolved through collaboration between the OHSC and the managers at the customer companies. Further research is needed though, and implementation studies regarding WHP for senior employees are of importance.
Acknowledgments
This work was supported by the Knowledge Foundation, and the School of Business, Engineering and Science and School of Social and Health Sciences at Halmstad University. The authors thank Eva-Carin Lindgren, assistant professor at Halmstad University, for the valuable advice on the readability of this paper.
Disclosure
The authors report no conflicts of interest in this work.
References
Jensen IB, Bush H, Bodin L, Hagberg J, Nygren A, Bergström G. Cost effectiveness of two rehabilitation programmes for neck and back pain patients: a seven year follow-up. Pain. 2009;142:202–208. | ||
Eriksson M. Unravelling the Mystery of Salutogenesis. The Evidence Base of Salutogenic Research as Measured by Antonovsky’s Sence of Coherence Scale [dissertation]. Turku: Åbo Akademi University; 2007. | ||
Bringsén Å, Andersson I, Ejlertsson G, Troein M. Exploring workplace related health resources from a salutogenic perspective: results from a focus group study among healthcare workers in Sweden. Work. 2012;42:403–414. | ||
Powers BJ, Trinh JV, Bosworth HB. Can this patient reads and understand written health information? JAMA. 2010;304(1):76–84. | ||
Torp S, Vinje H. Is workplace health promotion research in the Nordic countries really on the right track? J Public Health. 2014;42(15):74–81. | ||
Barbeau E, Calderon P, Hartman C, et al. Results of a union-based smoking cessation intervention for apprentice iron workers (United States). Cancer Causes Control. 2006;17(1):53–61. | ||
Feldt T, Kinnunen U, Mauno S. A mediational model of sense of coherence in the work context: a one-year follow-up study. J Organ Behav. 2000;21(4):461–476. | ||
Toossi M. Labor force projections to 2014: retiring boomers. Labor Force. 2005;11:25–44. | ||
Silverstein M. Meeting the challenges of an aging workforce. Am J Ind Med. 2008;51(4):269–280. | ||
Jonson G, Melin L, Whittington R. Editors introduction: micro-strategy and strategizing: towards an activity-based view. J Manag Studies. 2003;40(1):3–22. | ||
Nyström G. Entreprenörens återkomst [Entrepreneur’s Return]. Rättvik: Vincents Förlag; 2007. Swedish. | ||
Nilsson N. Entreprenörens blick, om förståelse, identitet och handling i det mindre företaget [Entrepreneur’s Look, About Understanding, Identity and Action in the Smaller Company]. Kalmar: Högskolan i Kalmar; 2003. Swedish. | ||
Reason P, Bradbury H. The SAGE Handbook of Action Research. Participative Inquiry and Practice. 2nd ed. London: SAGE Publications; 2013. | ||
Armstrong R, Hall BJ, Doyle J, Waters E. Cochrane update. “Scoping the scope” of a Cochrane review. J Public Health. 2011;33(1):147–150. | ||
Helsinki Declaration. Ethical Principles for Medical Research Involving Human Subjects. With Later Amendments. Helsinki: World Medical Association; 1964. | ||
Elo S, Kyngäs H. The qualitative content analysis process. J Adv Nurs. 2008;61(1):107–115. | ||
Fonteyn M, Kuipers B, Grobe S. A description of think aloud method and protocol analysis. Qual Health Res. 1993;3(4):430–441. | ||
French DP, Cooke R, McLean N, Williams M, Sutton S. What do people think about when they answer theory of planned behaviour questionnaires? A ‘think aloud’ study. J Health Psychol. 2007;12(4):672–687. | ||
IBM Corp. Released 2011. IBM SPSS Statistics for Windows, Version 20.0. Armonk, NY: IBM Corp. | ||
Berg JM, Wrzesniewski A, Dutton EJ. Perceiving and responding to challenges in job crafting at different ranks: when proactivity requires adaptivity. J Organ Behav. 2010;31:158–186. | ||
Parry E, Urwin P. Generational differences in work values: a review of theory and Evidence. Int J Manag Rev. 2011;13:79–96. | ||
Schullery MN. Workplace engagement and generational differences in values. Bus Commun Q. 2013;76(2):252–265. | ||
Kooij D, De Lange A, Jansen P, Kanfer R, Dikkers J. Age and work-related motives: results of a meta-analysis. J Organ Behav. 2011;32:197–225. | ||
Inceoglu I, Segers J, Bartram D. Age-related differences in work motivation. J Occup Organ Psychol. 2012;85:300–329. | ||
Aelfers E, Bosma H, Houkes I, van Eijk JT. Effectiveness of minimal psychological intervention to reduce mild to moderate depression and chronic fatigue in a working population: the design of a randomized controlled trial. BMC Public Health. 2013;13:129. | ||
Lamers F, Jonkers C, Bosma H, et al. A minimal psychological intervention in chronically ill elderly patients with depression: a randomized trial. Psychother Psychosom. 2010;79:217–226. | ||
Bartel C, Wrzesniewski A, Wiesenfeld BM. Knowing where you stand: physical isolation, perceived respect, and organizational identification among virtual employees. Organ Sci. 2011;23(3):743–757. | ||
Noben YGC, Nijhuis JNF, de Rijk EA, Evers SM. Design of trial-based economic evaluation on the cost-effectiveness of employability interventions among work disabled employees or employees at risk of work disability: the CASE-study. BMC Public Health. 2012;12:43. | ||
Baicker K, Cutler D, Song Z. Workplace wellness programs can generate savings. Health Aff (Millwood). 2010;29(2):304–311. | ||
Aittasalo M, Rinne M, Pasanen M, Kukkonen-Harjula K, Vasankari T. Promoting walking among office employees – evaluation of randomized controlled intervention with pedometers and e-mail messages. BMC Public Health. 2012;12:403. | ||
Cancelliere C, Cassidy JD, Ammendolia C, Cote P. Are work health promotion programs effective at improving presenteeism in workers? A systematic review and best evidence synthesis of the literature. BMC Public Health. 2011;11:395. | ||
Dane E, Bradley JB. Examining workplace mindfulness and its relations to job performance and turnover intention. Hum Relat. 2013;67(1):105–128. | ||
Bakker BA. An evidence-based model of work engagement. Curr Dir Psychol Sci. 2011;20(4):265–269. | ||
Braveman B, Bass-Haugen DJ. Social justice and health disparities: an evolving discourse in occupational therapy research and intervention. Am J Occup Ther. 2010;63:7–12. | ||
Guazzi M, Faggiano P, Mereddu GF, Faden G, Niebauer J, Temporelli PL. Worksite health and wellness in the European Union. Prog Cardiovasc Dis. 2014;56:508–514. | ||
Verweij LM, Proper K, Leffelaar ER, et al. Barriers and facilitators to implementation of an occupational health guideline aimed at preventing weight gain among employees in the Netherlands. J Occup Environ Med. 2012;54(8):954–960. | ||
Paggi ME, Jopp DS. Outcomes of occupational self-efficacy in older workers. Int J Aging Hum Dev. 2015;80(4):357–378. | ||
van den Berg PT. Characteristics of the work environment related to older employees’ willingness to continue working; intrinsic motivation as a mediator. Psychol Rep. 2011;109(1):174–186. | ||
Lydell M, Marklund B, Baigi A, Mattsson B, Månsson J. Return or no return – psychosocial factors related to sick leave in persons with musculoskeletal disorders: a prospective cohort study. Disabil Rehabil. 2011;33(8):661–666. | ||
Arandjelovic M. A need for holistic approach to the occupational health developing. Int J Occup Med Environ Health. 2011;24(3):229–240. | ||
Larsson R, Åkerlind I, Sandmark H. Managing workplace health promotion in municipal organizations: the perspective of senior managers. Work. 2015;53(3):485–498. | ||
Schaafsma FG, Anema JR, van der Beek AJ. Back pain: prevention and management in the workplace. Best Pract Res Clin Rheumatol. 2015;29(3):483–494. | ||
Zacharatos A, Barling J, Iversen RD. High-performance work systems and occupational safety. J Appl Psychol. 2005;90(1):77–93. | ||
Bramwell DL, Sanders C, Rogers A. A case of tightrope walking: an exploration of the role of employers and managers in supporting people with long-term conditions in the workplace. Int J Workplace Health Manag. 2016;9(2):238–250. | ||
Varekamp I, Boudien K, van Dijk FJH. Empowering employees with chronic diseases: process evaluation of an intervention aimed at job retention. Int Arch Occup Environ Health. 2011;84:35–43. | ||
Lindström B, Eriksson M. From health education to healthy learning: implementing salutogenesis in educational science. Scand J Public Health. 2011;39:85–92. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.