")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 13
Fungal Isolates of the Respiratory Tract in Symptomatic Patients Hospitalized in Pulmonary Units: A Mycological and Molecular Epidemiologic Study
Authors Rafat Z, Hashemi SJ, Ashrafi K, Nikokar I, Jafari A , Rahimi Foroushani A , Roohi B, Borjian Boroujeini Z , Rashidi N, Najar-Shahri N
Received 4 March 2020
Accepted for publication 10 July 2020
Published 22 July 2020 Volume 2020:13 Pages 661—669
DOI https://doi.org/10.2147/JMDH.S252371
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Zahra Rafat,1 Seyed Jamal Hashemi,1,2 Keyhan Ashrafi,3 Iraj Nikokar,4 Alireza Jafari,5 Abbas Rahimi Foroushani,6 Behrad Roohi,7 Zeinab Borjian Boroujeini,1 Niloofar Rashidi,1 Niki Najar-Shahri4
1Department of Medical Parasitology and Mycology, School of Public Health, Tehran University of Medical Sciences, Tehran, Iran; 2Food Microbiology Research Center, Tehran University of Medical Sciences, Tehran, Iran; 3Department of Medical Microbiology, School of Medicine, Guilan University of Medical Sciences, Rasht, Iran; 4Laboratory of Microbiology and Immunology of Infectious Diseases, Paramedicine Faculty, Guilan University of Medical Sciences, Langeroud, Iran; 5Urology Research Center, Razi Hospital, Guilan University of Medical Sciences, Rasht, Iran; 6Department of Statistics and Epidemiology, School of Public Health, Tehran University of Medical Sciences, Tehran, Iran; 7Department of Medical Mycology, Mazandaran University of Medical Sciences, Sari, Iran
Correspondence: Seyed Jamal Hashemi Tel +98 21 4293 3150
Fax +98 21 88951392
Email [email protected]
Introduction: Fungal respiratory infections are being recognized with increasing frequency in parallel with an expanding population of immunocompromised patients. In most cases, colonization is the first step in the progression to pulmonary fungal infection. This study was designed to evaluate the distribution of fungal elements in the respiratory tract of symptomatic patients hospitalized in pulmonary units.
Methods: This descriptive cross-sectional study was carried out over a period of two years, from October 2017 to October 2019 in Guilan province, located in Iran’s northern region. In the current study, bronchoalveolar lavage or sputum specimens were collected. All samples were analyzed by direct microscopy using KOH 10% and culture. Fungal identification was accomplished by internal transcribed spacer (ITS) and beta-tubulin sequencing. Also, in patients suspected of invasive pulmonary aspergillosis, BAL specimens were tested for galactomannan (GM) antigen.
Results: A total of 384 lung specimens (192 bronchoalveolar lavage (BAL) and 192 sputum samples) were obtained from symptomatic patients hospitalized in pulmonary units. Of these, 137 (35.67%) were positive in direct examination and culture. Among the 137 positive cases, most isolates were from male patients 86 (62.77%) and most of them were between 46 and 72 years. Candida albicans (37.22%) and Candida tropicalis (21.89%) represent the two most commonly isolated species in the current study. Cough (94.16%), dyspnea (81.02%), purulent sputum (62.04%) and weight loss (56.2%) were the predominant symptoms and tuberculosis (24.81%), chemotherapy (21.89%) and diabetes mellitus (19.70%) were the predominant underlying conditions. Also, 5 cases of invasive pulmonary aspergillosis and 1 case of mucormycosis were diagnosed.
Conclusion: Candida albicans was the most common fungal species isolated from symptomatic patients hospitalized in pulmonary units. Tuberculosis, chemotherapy and diabetes mellitus were important underlying conditions for pulmonary fungal colonization and/or infection.
Keywords: pulmonary fungal infection, bronchoalveolar lavage, sputum, respiratory tract, Iran
Introduction
Respiratory tract diseases are globally responsible for one-third of infectious disease-associated mortality, accounting for 4.3 million annual deaths.1 Despite treatment, most invasive pulmonary fungal infections are associated with high mortality rates of > 50%.2 The air we breathe is filled with thousands of fungal spores (conidia). After inhalation these tiny elements, hosts may have no symptoms or may cough up blood or have a fever or chest pain or may have symptoms ranging from allergies to life-threatening invasive mycoses.3,4 The outcome depends on the immune status of the host. Pulmonary fungal diseases consist of fungal colonization, allergy, and infection of the pulmonary tract and lungs and in most cases, colonization is the first step in the progression to pulmonary fungal infection. During recent decades, pulmonary fungal diseases are being diagnosed with increasing frequency,5 largely because of the increasing size of the population at risks, such as patients receiving immunosuppressive therapy, those undergoing bone marrow transplantation or solid-organ transplant (SOT) and those with HIV infection, tuberculosis or cystic fibrosis. In addition, the widespread implementation of fluconazole antifungal prophylaxis has rendered the host at greater risk for colonization with more resistant fungal species, enhancing the increase of invasive fungal infections in these already immune-suppressed patients.3,6 The incidence and etiology of pulmonary fungal diseases can vary in various types of patient’s hospital settings, and geographical locations. Fungi which affect immunosuppressed individuals are frequently species of Aspergillus, Candida, Cryptococcus, geographically restricted agents, and newly emerging fungal pathogens.7,8 In one study, Aspergillus spp. was isolated from 33% (86/251 cases) of lung-transplantation recipients, which involved colonization (n = 50), tracheobronchial lesions (n = 17) or invasive aspergillosis (n = 19).9 Also, invasive pulmonary aspergillosis mortality of neutropenic patients was 40 to 60% in early reports.10 Candida infection was reported as the most dominant pulmonary fungal diseases in patients with non-hematologic malignant tumors and in non-lung SOT recipients. Taken together, the clinicians must remain vigilant for invasive and serious pulmonary fungal diseases even to individuals who were once considered only moderately immunocompromised. The present study evaluated the incidence of fungal elements detected or isolated from symptomatic patients hospitalized in pulmonary units, by direct microscopy, culture, and molecular typing techniques. Determining the clinical spectrum, underlying conditions, and demographic characteristics associated with pulmonary fungal colonization and/or infection were the other purposes of the current study.
Methods
Sampling
This descriptive cross-sectional study was carried out over a period of two years, from October 2017 to October 2019 in Guilan province, located in Iran’s northern region.
The presence of two or more following conditions was used as inclusion criteria in this study:
(1) Patients who displayed at least one of the following host factors: receiving chemotherapy within the last 3 months before admission in order to treat solid tumors, chronic obstructive pulmonary disease (COPD), steroid use: at least 4 mg methylprednisolone (or equivalent) per day for at least 7 days in the past 3 weeks before admission or a cumulative dose of at least 250 mg of methylprednisolone (or equivalent) in the past 3 months before enrollment and recipient of any other immunosuppressive treatment (tacrolimus, cyclosporine, methotrexate, cyclophosphamide, and sirolimus).
(2) Patient with clinical symptoms indicative of pulmonary fungal diseases according to a pulmonary diseases specialist opinion (dyspnea, cough, high and persistent fever, recurrent fever, chest pain, purulent sputum, weight loss, night fever, hemoptysis, rhinitis, and wheezing)
(3) Patients with suspicious radiographic findings indicative of pulmonary fungal diseases according to a pulmonologist opinion.
Demographic features including age, gender, underlying diseases, and patient’s clinical manifestations (fever, purulent sputum, dyspnea, etc.,) were recorded. Bronchoalveolar lavage or sputum specimens from each patient were obtained. Patients who had taken any systemic antifungal agents before enrollment for treating infections other than pulmonary fungal disease were excluded from the study in order to prevention of false-negative results. Once collected, the specimens were rapidly transported to the laboratory, and microscopic and culture experiments performed on the specimens for less than one hour. Sputum samples were diluted by adding sterile saline and vortex mixing. Also, BAL samples were centrifuged and the deposit was used for examination. For direct microscopic examination, the samples were dissolved in KOH 10% solution and observed under a microscope (Olympus. Germany) for fungal elements. Calcofluor white staining (Sigma, Deisenhofen, Germany) was done to detect the presence of fungal elements and Indian ink stain was used to check for Cryptococcus neoformans.11–13 All specimens were cultured on Sabouraud Dextrose Agar (SDA) with chloramphenicol and Brain Heart Infusion (BHI) agar media (Merck, Germany). Any growth obtained was further identified by its rate of growth, colony morphology, and lactophenol cotton blue mounts. Slide culture was performed as required.14,15 Yeast isolates were identified based on production chlamydoconidia in cornmeal agar (Becton, France) and colony color on chromogenic CHROMagar Candida medium (CHROMagar, Paris, France).16 Furthermore, for confirmation of diagnosis, all isolates were subjected to PCR and sequencing techniques. In this study, criteria such as the presence of budding yeast cells, pseudohyphae, or true hyphae in direct examination and/or significant growth of pure creamy mucoid colonies on culture media were considered as positive results for Candida isolation from the respiratory tract.17,18
BAL Galactomannan (GM) Test
Platelia Aspergillus GM EIA (Bio-Rad, France) was used to measure the galactomannan of Lavage samples according to the manufacturer procedures.13 Briefly, 300 μL of BAL was added to 100 μL of treatment solution, boiled for three minutes at 104◦C and then centrifuged for 10 minutes in 10,000 g. Next, 50 μL of supernatant and 50 μL of conjugate were mixed and incubated in microtiter plates precoated with monoclonal antibody EB-A2 for 90 minutes at 37◦C. The plates were washed five times; after which they were incubated with 200 μL of tetramethylbenzidine in the dark for 30 minutes. The reaction was stopped by 100 μL of sulfuric acid and absorbance at 450 and 620 nm read using a plate reader. Positive and negative controls were included in each assay. Results were recorded as an index relative to the optical density (OD) of the cut-off control. The GM of Lavage was considered positive when OD index was ≥1.0. All positive cases were repeated in the same sample before they were considered positive.
Molecular Technique
DNA Extraction
Fungal genomic DNA was extracted from harvested colonies using phenol-chloroform method.19
PCR Conditions and Sequencing
PCR amplification for each isolate was performed as described previously.19,20 PCR products were sent for sequencing. The DNA sequencing results were compared against the NCBI GenBank database (http://www/ncbi.nlm.nih.gov/BLAST). Fungal identifications were made based on maximum identities ≥ 99% and query coverage ≥ 98% with this method. All of the sequences had been deposited in GenBank under the accession number reported in Table 1.
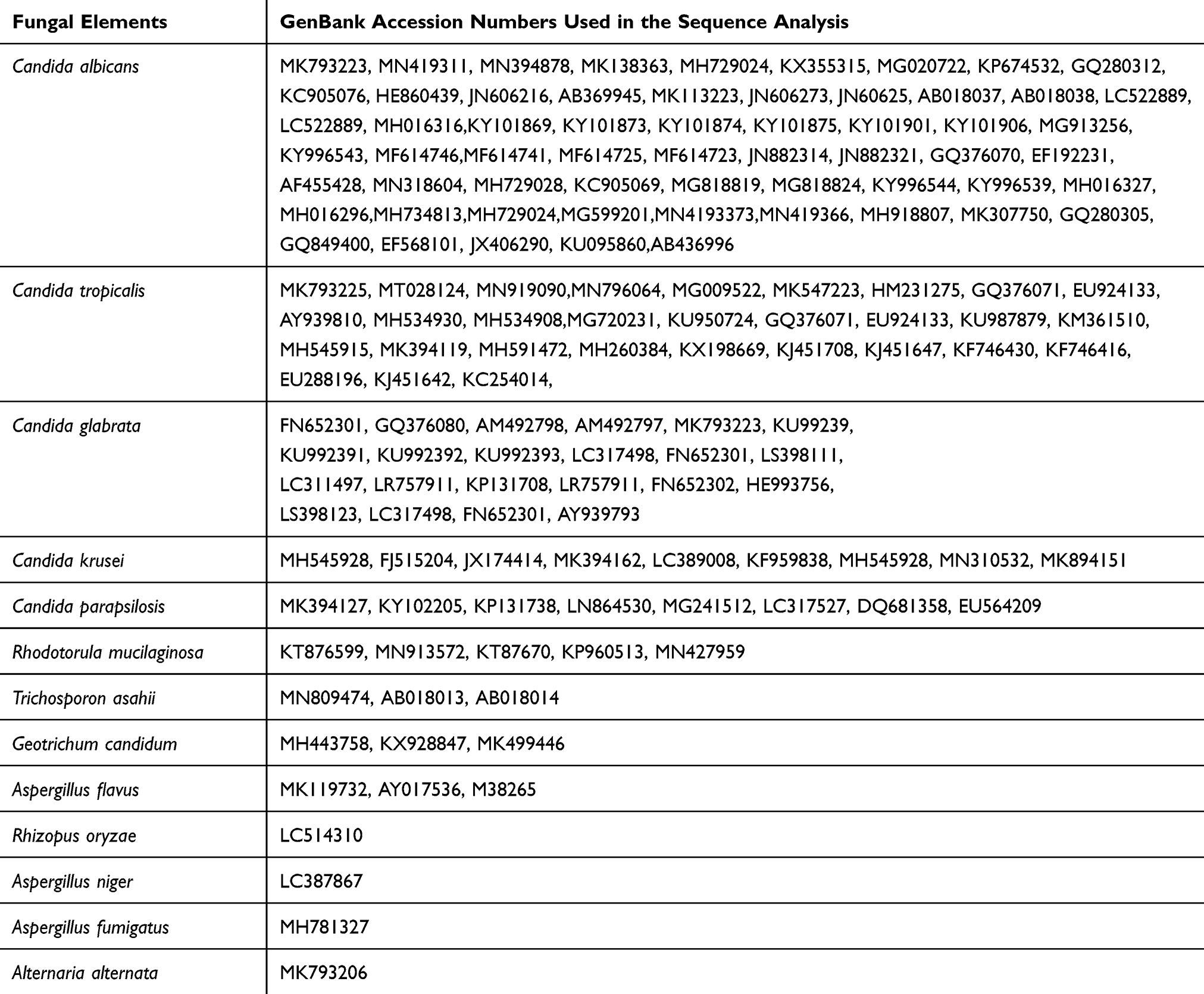 |
Table 1 GenBank Accession Numbers of DNA Sequences Included in This Study |
Statistical Tests
The data analysis was performed by SPSS software (IBM SPSS Statistics for Windows, Version 21.0, IBM Corp, Armonk, NY, USA). The study was assessed by using standard Chi-squared and 95% Confidence intervals (CI). Statistically, P-value <0.05 was considered as significant difference or correlation.
Patient and Public Involvement
This research was done without patient involvement. Patients were not invited to comment on the study design and were not consulted to develop patient relevant outcomes or interpret the results.
Results
Totally 384 symptomatic hospitalized patients (including 238 Males and 146 females) who met the eligibility criteria were enrolled. A total of 384 lung specimens including 192 bronchoalveolar lavage (BAL) and 192 sputum samples were obtained from symptomatic patients hospitalized in pulmonary units. Of this population, in 137 (35.67%) patients, fungal agents were isolated. The patients were within the age range of 1–86 years and the highest prevalence of fungal agents isolated from respiratory specimens was found in the age group of 46–72 years (n=75, 54.74%) (Table 2) and showed the age of subjects was not significantly effective on the prevalence of fungal agents isolated from symptomatic patients hospitalized in pulmonary units (P = 0.546).
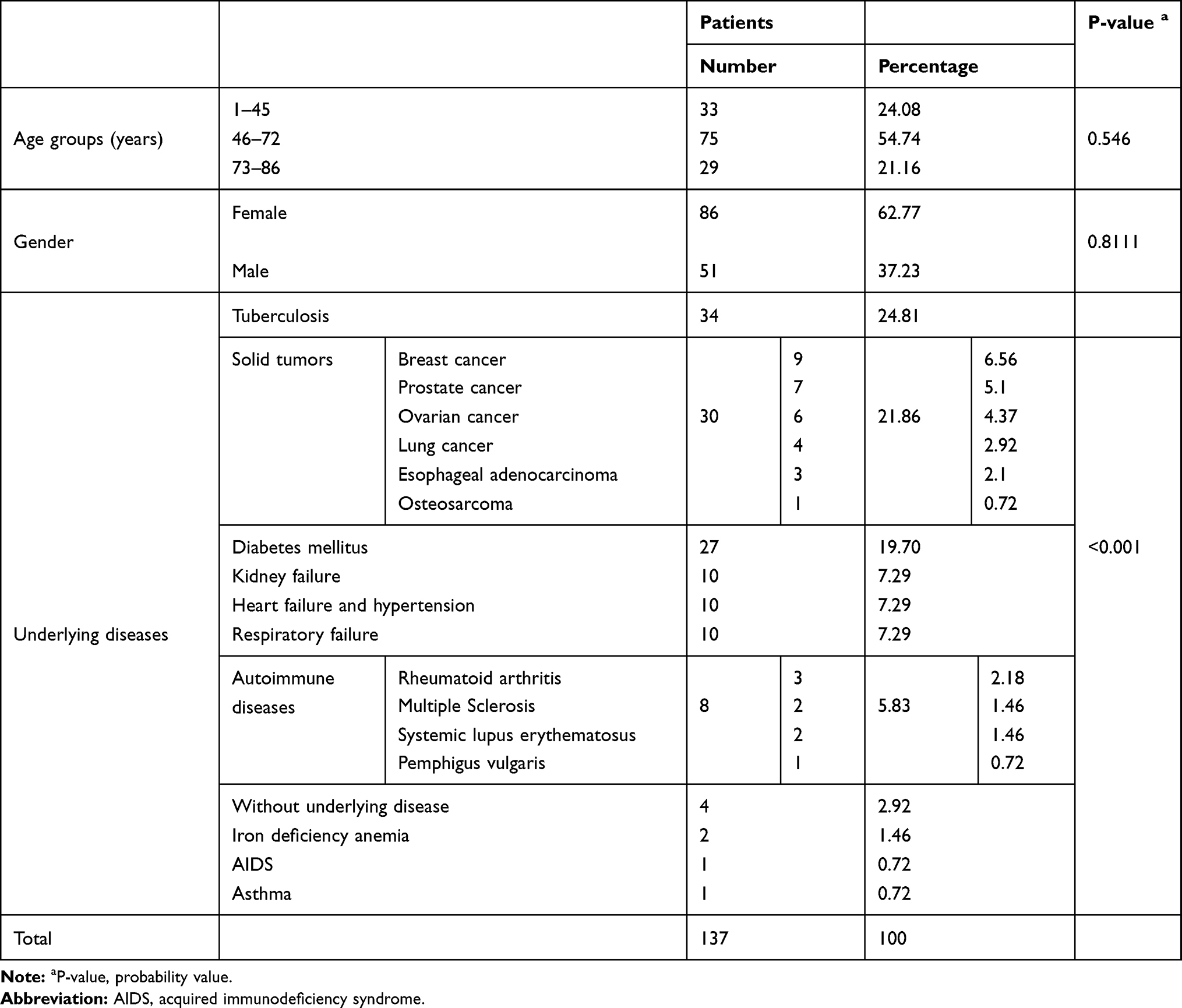 |
Table 2 The Distribution of 137 Symptomatic Patients Hospitalized in Pulmonary Units from Which Fungal Agents Were Isolated Based on Age Groups, Gender and Underlying Diseases |
Among the 137 positive cases in this research, most isolates were from male patients 86 (62.77%) (Table 2) and statistical analysis could not find any association between the prevalence of fungal agents isolated from symptomatic patients hospitalized in pulmonary units and patient’s gender (P= 0.811).
Among 137 positive cases, cough (n=129, 94.16%), dyspnea (n=111, 81.02%), purulent sputum (n= 85, 62.04%) and weight loss (n=77, 56.2%) were the most common symptoms followed by chest pain (n=36, 26.28%), wheezing (n=32, 23.36%), high and persistent fever (n=25, 18.25%), recurrent fever (n=22, 16.06%), night fever (n=19, 13.87%), hemoptysis (2.19%) and rhinitis (n=1, 0.73%). Statistical analysis showed that there was a significant relationship between the prevalence of fungal agents isolated from symptomatic patients hospitalized in pulmonary units and clinical symptoms. (P < 0.001).
A previous history of tuberculosis, receiving chemotherapy within the last 3 months before admission in order to treat solid tumors, and diabetes mellitus were found in 24.81%, 21.89%, and 19.70% of patients, respectively (Table 2). These predisposing factors were significantly associated with the prevalence of fungal agents isolated from symptomatic patients hospitalized in pulmonary units. (P < 0.001).
Candida albicans (37.22%) and Candida tropicalis (21.89%) represent the two most commonly isolated species in the current study followed by Candida glabrata (12.4%), Candida krusei (5.83%), Candida parapsilosis (5.1%), Trichosporon asahii (2.18%), Geothricum candidum (2.18%), Aspergillus flavus (2.18%), Rhizopus orizae(0.72%), Aspergillus niger (0.72), Aspergillus fumigatus (0.72%) and Alternaria alternata (0.72%). Also, mixed fungal elements in some examined specimens were detected in this study (Table 3).
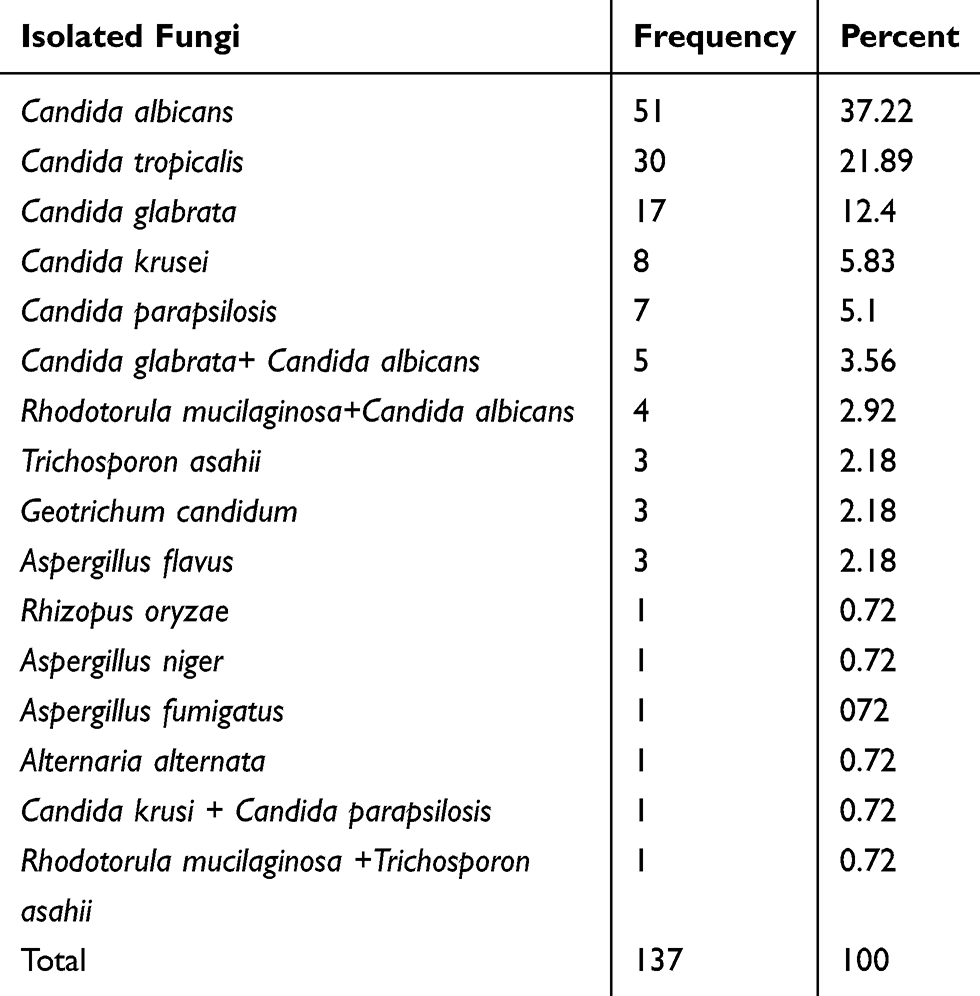 |
Table 3 The Frequency Distribution of Fungal Elements Isolated from 137 Positive Cases Hospitalized in Pulmonary Units |
From 8 patients suspected of pulmonary aspergillosis, 5 cases (62.5%) of IPA were reported. For all cases positive results in direct examination with forming branching septate hyphae in BAL samples along with positive results in culture media were obtained. In 3 patients (2.19%) Aspergillus flavus was the etiologic agent of invasive aspergillosis, in one patient (0.72%) A. fumigatus was the etiologic agent and in one other patient (0.72%) Aspergillus niger was the cause of respiratory disease. Aspergillus flavus was the most common cause of invasive aspergillosis in the present study. It should be noted that all sequencing results were consistent with macroscopic and microscopic identifications of the isolates according to culture appearance and sporulation characteristics. Also during the period of this study, GM test was performed for all patients suspected of invasive aspergillosis. In this EIA test, the OD index of 1.0 or more was taken as a positive result.
According to the revised and updated (2019) European Organization for Research and Treatment of Cancer and Mycoses Study Group (EORTC/MSG) definitions for invasive fungal infections,21 from 5 cases of pulmonary aspergillosis, 2 (40%) cases of probable invasive pulmonary aspergillosis and 3 (60%) cases of possible invasive pulmonary aspergillosis were diagnosed in this study (Table 4).
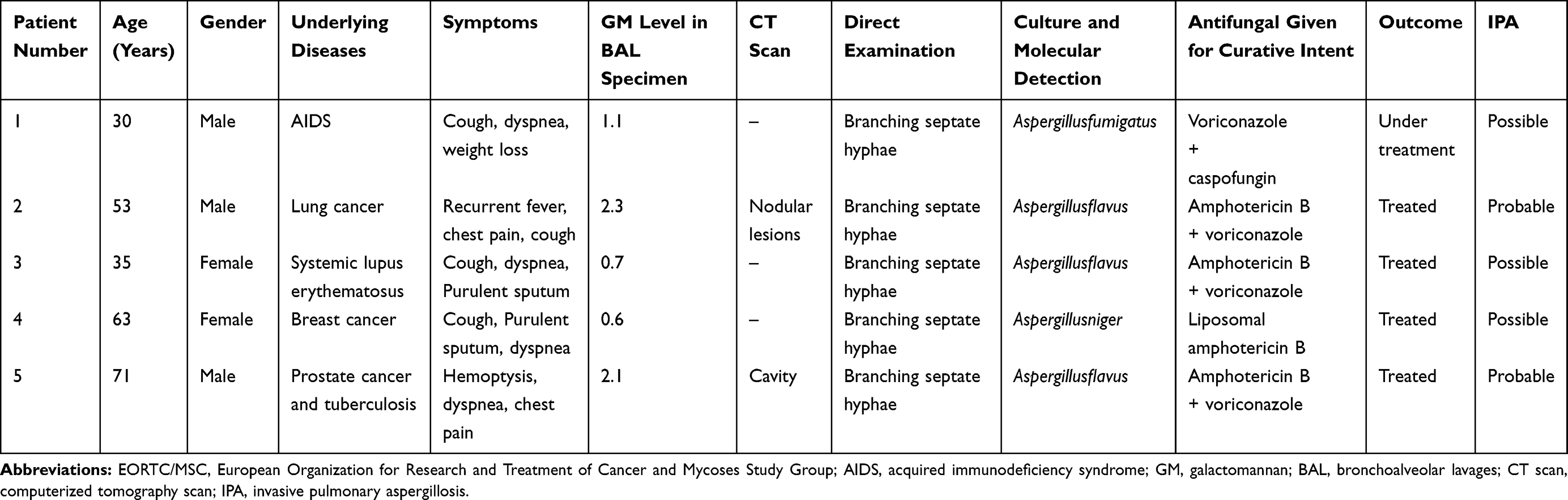 |
Table 4 Detailed Information of Each Patient Involved with Invasive Pulmonary Aspergillosis Categorized Based on EORTC/MSC (2019) Criteria |
Also in this study, from 137 positive cases, one case of mucormycosis (0.72%) in a 76 years old man receiving chemotherapy in order to treat prostate cancer was reported. After culture on SDA medium and sequencing, Rhizopus oryzae was reported as the etiologic agent. Besides, one case of Alternaria alternata (0.72%) was isolated from the BAL sample belonged to a 30 years old woman with a history of chronic nasal congestion and drainage, asthma and allergic rhinitis from 8 years ago. In addition, 3 cases (2.19%) of pulmonary Geothricum involvement due to Geothricum candidum and 4 cases (2.92%) of pulmonary Trichosporon involvement due to Trichosporon asahi, were reported in this study (Table 3).
Discussion
The respiratory tract is the most common site for developing fungal infection and in most cases, colonization is the first step in the progression to pulmonary fungal infection. In this study, a total of 384 lung specimens related to symptomatic patients hospitalized in pulmonary units were examined and in 137 (35.67%) cases fungal elements were detected. In agreement with our results, Jahromi et al reported the same prevalence (36.6%) for fungal isolates of the respiratory tract in Tehran, Iran.22 Also, Akhtar et al reported a prevalence of 31.3% for pulmonary fungal involvement in Bhagalpur, India.23 While the Egyptian study of Ahmed and colleagues showed that the prevalence of fungal pneumonia in respiratory intensive care unit was 66.67%.24 Most of the patients who were positive for fungal elements isolation from the respiratory tract in the current study (54.74%) were at an age range of 46–72 years old. Older adults become more susceptible to diseases due to predisposing factors such as diabetes mellitus, renal insufficiency, and arthritis. Also, when people age, there is immunosenescence, which means that the immune system does not function as well or as vigorously. The combination of predisposing factors and the decrease in the activity of the immune system can make these age groups more prone to fungal colonization and/or infection.25
In this study, in accordance with the results of another report,22 in positive cases the male-to-female ratio was 86 to 51 and there was no significant difference in the prevalence of fungal elements isolated from symptomatic patients hospitalized in pulmonary units between the genders. Similar exposure to pollution sources due to equal sociodemographic conditions, occupations, and responsibilities for men and women in society could be the reason for the observed similarity between two gender groups. Cough (n=129, 94.16%), dyspnea (n=111, 81.02%), purulent sputum (n= 85, 62.04%) and weight loss (n=77, 56.2%) were the most common symptoms among 137 positive cases in the current study. Considering the fact that pulmonary fungal involvements often cause symptoms that are similar to other illnesses, such as the flu or tuberculosis, clinical and laboratory findings should be used simultaneously for making the final decision on drug administration.
Tuberculosis was the main predisposing factor observed in 24.81% of positive cases in the current study. Tuberculosis (TB) is still one of the biggest killers among infectious diseases especially in developing countries like Iran.26 This country shares geographic borders with three countries in which, tuberculosis is endemic: Afghanistan, Iraq, and Pakistan. In addition, Iran is in a close association with other countries where tuberculosis is highly prevalent, ie China, India, Nepal, Bosnia, Bangladesh, Tajikistan, Sri Lanka, and Azerbaijan. It should be noted that the percentage of mycotic diseases increase in pulmonary tuberculosis patients. The results of different studies showed that physicians should pay particular attention to fungal co-infection with pulmonary TB.27,39,40 In a study of Kali and colleagues Candida co-infection was observed in 40% of patients with pulmonary tuberculosis.39 Also, Denning et al reported that from 21% (United States of America) to 35% (Taiwan, China) of pulmonary tuberculosis patients developed pulmonary cavities and about 22% of these patients developed chronic pulmonary aspergillosis.40 A history of receiving chemotherapy within the last 3 months before admission in order to treat solid tumors (21.89%), and diabetes mellitus (19.70%) were the other common underlying conditions for fungal colonization and/or infection in this study. Studies showed that after intensive chemotherapy, the estimated risk of developing invasive pulmonary fungal infections is about 5%, and the reported mortality ranges from 30 to 80%.28 Diabetes patients have an immune system with a lower ability to respond to and deal with diseases of any type. This means they are more prone to illnesses than the general population. Diabetes can contribute to the development of fungal/bacterial/viral pneumonia, tuberculosis and chronic obstructive pulmonary disease (COPD).29
Candida albicans (37.22%) and Candida tropicalis (21.89%) were the most common isolated species in this study. In Accordance with our results, Spahr et al reported that Candida albicans and Candida tropicalis are the most important causes of pulmonary fungal diseases.30 Also in the current study, from 5 patients with IPA, in 3 patients (60%) Aspergillus flavus was the etiologic agent of invasive aspergillosis. Studies showed that Aspergillus flavus was the most distributed species among genus Aspergillus in indoor and outdoor environments in Iran.31,32 More distribution of Aspergillus flavus in the environment can facilitate exposure and increase the risk of colonization and infection with this species. Since in most of the studies in Iran, Candida albicans and Aspergillus flavus were specified as the most prevalent etiology of pulmonary fungal colonization and/or infection,22,31,33,34 uncommon species like Geothricum candidum, Trichosporon asahii, the Mucorales, and non-albicans Candida species should not be ignored. Given that some of the uncommon species are intrinsically resistant to routine antifungal drugs, they could cause treatment failure and should be taken into account.
According to the revised and updated EORTC/MSG (2019) definitions for invasive fungal infections, from 5 cases of pulmonary aspergillosis (IPA), 2 (40%) cases of probable IPA and 3 (60%) cases of possible IPA were diagnosed in this study. In a study conducted by Hedayati et al in Iran, out of 36 suspected patients to IA, 36.1% of cases showed IA which were categorized as 4 cases of possible IA and 9 of probable IA.35 In the present study we applied GM detection in BAL. Some authors suggested that it can be beneficial to detect GM in BAL fluid for IA diagnosis.36–38 To the best of our knowledge, this is the first study on the epidemiology, clinical spectrum, underlying conditions, and demographic characteristics associated with pulmonary fungal colonization and/or infection in Guilan province, located in Iran’s northern region.
Conclusions
Of 384 pulmonary specimens, 137 (35.67%) were positive in direct examination and culture for fungal isolation. Tuberculosis, receiving chemotherapy within the last 3 months before admission in order to treat solid tumors and diabetes mellitus were important risk factors, and Candida albicans was the most common fungal species responsible for pulmonary fungal colonization and/or infection.
Ethics Approval
This study was approved by the ethical committee of Tehran University of Medical Sciences (the number of Ethics Committee protocol: IR.TUMS.SPH.REC.1397.002). A written informed consent was obtained from all subjects or their guardians prior to sample collection. All data were de-identified.
Acknowledgments
The authors wish to thank the financial support of Tehran University of Medical Sciences.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that there is no conflicts of interest.
References
1. Fauci AS, Morens DM. The perpetual challenge of infectious diseases. N Engl J Med. 2012;366(5):454–461. doi:10.1056/NEJMra1108296
2. Brown GD, Denning DW, Gow NA, et al. Hidden killers: human fungal diseases. Sci Transl Med. 2012;4(165):165rv13. doi:10.1126/scitranslmed.3004404
3. Ben-Ami R, Lewis RE, Kontoyiannis DP. Invasive mould diseases in the setting of hematopoietic cell transplantation: current trends and new challenges. Curr Opin Infect Dis. 2009;22(4):376–384. doi:10.1097/QCO.0b013e32832db9f3
4. Aimanianda V, Bayry J, Bozza S, et al. Surface hydrophobin prevents immune recognition of airborne fungal spores. Nature. 2009;460(7259):1117–1121. doi:10.1038/nature08264
5. Panda B. Fungal diseases of lungs: the emerging scenario. Indian J Tubercul. 2004;51(2):63–70.
6. Wilson LS, Reyes CM, Stolpman M, Speckman J, Allen K, Beney J. The direct cost and incidence of systemic fungal diseases. Value Health. 2002;5(1):26–34. doi:10.1046/j.1524-4733.2002.51108.x
7. Kubak BM. Fungal infection in lung transplantation. Transpl Infect Dis. 2002;4(3):24–31. doi:10.1034/j.1399-3062.4.s3.4.x
8. Pagano L, Caira M, Fianchi L. Pulmonary fungal infection with yeasts and pneumocystis in patients with hematological malignancy. Ann Med. 2005;37(4):259–269. doi:10.1080/07853890510037374
9. Sole A, Morant P, Salavert M, et al. Aspergillus infections in lung transplant recipients: risk factors and outcome. Clin Microbiol Infect. 2005;11(5):359–365. doi:10.1111/j.1469-0691.2005.01128.x
10. Tripathy U, Yung GL, Kriett JM, Thistlethwaite PA, Kapelanski DP, Jamieson SW. Donor transfer of pulmonary coccidioidomycosis in lung transplantation. Ann Thorac Surg. 2002;73(1):306–308. doi:10.1016/S0003-4975(01)02723-0
11. Hageage GJ, Harrington BJ. Use of calcofluor white in clinical mycology. Lab Med. 1984;15(2):109–112. doi:10.1093/labmed/15.2.109
12. Cheesbrough M. District Laboratory Practice in Tropical Countries.
13. Lai -C-C, Hsu HL, Lee LN, Hsueh P-R. Assessment of Platelia Aspergillus enzyme immunoassay for the diagnosis of invasive aspergillosis. J Microbiol Immunol Infect. 2007;40(2):148–153.
14. Abe M, Ogawa Z, Tanuma H, Kume H. Study of mycological examination methods in clinical laboratories-specimen pretreatment and isolation. Jpn J Med Mycol. 2009;50(4):235–242. doi:10.3314/jjmm.50.235
15. Procop GW, Church D, Hall G, et al. Koneman’s Color Atlas and Textbook of Diagnostic Microbiology.
16. Agarwal S, Manchanda V, Verma N, Bhalla P. Yeast identification in routine clinical microbiology laboratory and its clinical relevance. Indian J Med Microbiol. 2011;29(2):172–177. doi:10.4103/0255-0857.81794
17. Topely & Wilsons. Microbiology and Microbial Diseases.
18. Badiee P. Evaluation of human body fluids for the diagnosis of fungal diseases. Biomed Res Int. 2013;2013.
19. Nasri T, Hedayati MT, Abastabar M, et al. PCR-RFLP on β-tubulin gene for rapid identification of the most clinically important species of Aspergillus. J Microbiol Method. 2015;117:144–147. doi:10.1016/j.mimet.2015.08.007
20. Ferrer C, Colom F, Frasés S, Mulet E, Abad JL, Alio JL. Detection and identification of fungal pathogens by PCR and by ITS2 and 5.8 S ribosomal DNA typing in ocular infections. J Clin Microbiol. 2001;39(8):2873–2879. doi:10.1128/JCM.39.8.2873-2879.2001
21. Donnelly JP, Chen SC, Kauffman CA, et al. Revision and update of the consensus definitions of invasive fungal disease from the European Organization for research and treatment of cancer and the mycoses study group education and research Consortium. Clin Infect Dis. 2019. doi:10.1093/cid/ciz1008
22. Jahromi SB, Khaksar AA. Fungal isolates of the respiratory tract. Crit Care Med. 2002;30(12):A111. doi:10.1097/00003246-200212001-00378
23. Akhtar A, Roohani AH, Fatima N, Shameem M, Khan HM, Khan PA. Comparing the profile of respiratory fungal pathogens amongst immunocompetent and immunocompromised hosts, their susceptibility pattern and correlation of various opportunistic respiratory fungal diseases and their progression in relation to the CD4+ T-cell counts. Indian J Med Microbiol. 2018;36(3):408.
24. Ahmed M, Farghaly A, Raafat R, Abd Elsattar W. Study of the prevalence and pattern of fungal pneumonias in respiratory intensive care unit. Egypt J Bronchol. 2019;13(4):545–550. doi:10.4103/ejb.ejb_37_19
25. Gavazzi G, Krause K-H. Ageing and disease. Lancet Infect Dis. 2002;2(11):659–666. doi:10.1016/S1473-3099(02)00437-1
26. Rafiee S, Besharat S, Jabbari A, Golalipour F, Nasermoaadeli A. Epidemiology of tuberculosis in northeast of Iran: a population-based study. Iran J Med Sci. 2009;34(3):193–197.
27. Fontalvo DM, Jiménez Borré G, Gómez Camargo D, et al. Tuberculosis and fungal co-disease present in a previously healthy patient. Colomb Med. 2016;47(2):105–108. doi:10.25100/cm.v47i2.2271
28. Joos L, Tamm M. Breakdown of pulmonary host defense in the immunocompromised host: cancer chemotherapy. Proc Am Thorac Soc. 2005;2(5):445–448. doi:10.1513/pats.200508-097JS
29. Ramirez LC, Dal Nogare A, Hsia C, et al. Relationship between diabetes control and pulmonary function in insulin-dependent diabetes mellitus. Am J Med. 1991;91(4):371–376. doi:10.1016/0002-9343(91)90154-P
30. Spahr J, Weiner DJ, Stokes DC, Kurland G. Pulmonary Disease in the pediatric patient with acquired immunodeficiency states. In: Kendig’s Disorders of the Respiratory Tract in Children. Elsevier; 2019:923–943.
31. Hedayati MT, Mayahi S, Denning DW. A study on Aspergillus species in houses of asthmatic patients from Sari city, Iran and a brief review of the health effects of exposure to indoor Aspergillus. Environ Monit Assess. 2010;168(1–4):481–487. doi:10.1007/s10661-009-1128-x
32. Hedayati MT, Mayahi S, Movahedi M, Shokohi T. A Study on fungal flora of tap water as a potential reservoir of fungi in hospitals from Sari city, Iran. J Mycol Méd. 2011;21(1):10–14. doi:10.1016/j.mycmed.2010.12.001
33. Zarrinfar H, Saber S, Kordbacheh P, et al. Mycological microscopic and culture examination of 400 Bronchoalveolar Lavage (BAL) samples. Iran J Public Health. 2012;41(7):70–76.
34. Zanganeh E, Zarrinfar H, Rezaeetalab F, et al. Predominance of non-fumigatus Aspergillus species among patients suspected of pulmonary aspergillosis in a tropical and subtropical region of the Middle East. Microb Pathog. 2018;116:296–300. doi:10.1016/j.micpath.2018.01.047
35. Hedayati MT, Khodavaisy S, Alialy M, Omran SM, Habibi MR. Invasive aspergillosis in intensive care unit patients in Iran. Acta Medica (Hradec Kralove). 2013;56(2):52–56. doi:10.14712/18059694.2014.24
36. Clancy CJ, Jaber RA, Leather LH, et al. Bronchoalveolar lavage galactomannan in diagnosis of invasive pulmonary aspergillosis among solid-organ transplant recipients. J Clin Microbiol. 2007;45:1759–1765.
37. Husain S, Clancy CJ, Nguyen MH, et al. Performance characteristics of the Platelia Aspergillus enzyme immunoassay for detection of Aspergillus galactomannan antigen in bronchoalveolar lavage fluid. Clin Vaccine Immunol. 2008;15(12):1760–1763. doi:10.1128/CVI.00226-08
38. Sanguinetti M, Posteraro B, Pagano L, et al. Comparison of real-time PCR, conventional PCR, and galactomannan antigen detection by enzyme- linked immunosorbent assay using bronchoalveolar lavage fluid samples from hematology patients for diagnosis of invasive pulmonary aspergillosis. J Clin Microbiol. 2003;41:3922–3925. doi:10.1128/JCM.41.8.3922-3925.2003
39. Kali A, Charles MP, Noyal MJ, Sivaraman U, Kumar S, Easow JM. Prevalence of Candida co-infection in patients with pulmonary tuberculosis. Australas Medical J. 2013;6(8):387–391. doi:10.4066/AMJ.2013.1709
40. Denning DW, Pleuvry A, Cole DC. Global burden of chronic pulmonary aspergillosis as a sequel to pulmonary tuberculosis. Bull World Health Organ. 2011;89(12):864–872. doi:10.2471/BLT.11.089441
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.