")
Back to Journals » International Journal of Nephrology and Renovascular Disease » Volume 15
Full and Booster Doses of SARS-CoV-2 mRNA-1273 Vaccine Increase Waning Antibody Levels After Completed Vaccination Among Dialysis Patients at a Large Dialysis Organization
Authors Ficociello LH , Willetts J, Mullon C , Johnson C, Anger MS , Hymes JL
Received 4 August 2022
Accepted for publication 4 November 2022
Published 16 November 2022 Volume 2022:15 Pages 319—321
DOI https://doi.org/10.2147/IJNRD.S383215
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Pravin Singhal
Linda H Ficociello,1 Joanna Willetts,1 Claudy Mullon,1 Curtis Johnson,2 Michael S Anger,1 Jeffrey L Hymes1
1Global Medical Office, Fresenius Medical Care, Waltham, MS, USA; 2Spectra Laboratories, Southaven, MS, USA
Correspondence: Jeffrey L Hymes, Fresenius Medical Care, 1000 Corporate Centre Drive, Suite 400, Franklin, TN, 37067, USA, Email [email protected]
Antibody response to the primary 2-dose regimen of mRNA-based coronavirus disease 2019 (COVID-19) vaccines is reduced in dialysis populations vs healthy controls.1 Moreover, dialysis patients demonstrate a faster decline in antibody levels and diminished long-term antibody response than the general population.2–5 These findings support prioritizing this population for additional vaccine doses following primary vaccination. The antibody response following an initial 2-dose course of the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) mRNA-1273 vaccine and third “full” (100 mcg) or “booster” (50 mcg) doses has not been well characterized.
As part of a continuing quality improvement project, we examined antibody levels among patients who received 2 doses of the mRNA-1273 vaccine across 7 Fresenius Kidney Care clinics in Massachusetts, with follow-up antibody levels at least 250 days after completion of the primary vaccination series. Patients with evidence of any COVID-19 infection (eg, positive polymerase chain reaction test, elevated antibody levels prior to initial vaccination, and/or clinical symptoms of COVID-19), those who received >3 vaccine doses, and those who received other COVID-19 vaccines were excluded from the present analysis. Antibody testing was performed at a centralized laboratory using remnant blood samples originally collected for routine laboratory assessments. A semiquantitative chemiluminescent assay for immunoglobulin G directed against the receptor binding domain of the S1 subunit of the SARS-CoV-2 spike antigen (ADVIA Centaur® XP/XPT sCOVG; Siemens Healthcare Diagnostics Inc.; Tarrytown, NY) was used. Antibody levels were indexed between 0.5 and 750, with indices >1 considered reactive and those >7 considered to represent an “adequate” response.6
Antibody levels were grouped according to time points relative to vaccine dose 1 (before dose 1; after dose 1 but before dose 2), dose 2 (0–15, 16–30, 31–60, 61–120, and 161–220 days after dose 2) and, if applicable, dose 3 (250+ days after dose 2 and after dose 3). No samples were collected 121–160 days after dose 2. If a patient had multiple antibody levels during a given time period, the last value was analyzed. Data are reported through December 1, 2021.
The present analysis includes data from 136 patients. Overall, 125 patients received a third mRNA-1273 dose, which was further classified as “full” (n=113) or booster (n=12); 11 patients did not receive a third dose. Third vaccinations were administered a median (interquartile range) of 247 (245–261) days and 235 (231–237) days after completion of the primary vaccination series for the full and booster doses, respectively.
Following the primary (2-dose) vaccination, median (interquartile range) antibody levels peaked within 15 days after the second dose (142 [37–381]). Thereafter, median antibody levels declined (Figure 1). At 161–220 days after dose 2, 54% of patients with available data had antibody indices >7. At this time point, rates of adequate antibody responses were 51% and 80% among those patients who would go on to receive full and booster doses, respectively, and 71% among those who would not receive a third dose.
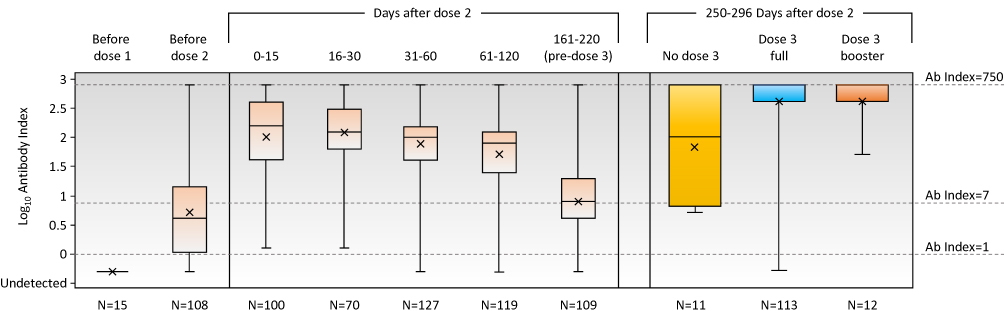 |
Figure 1 Antibody response before and after third dose of mRNA-1273 vaccine. In the box plot, the range (error bars), interquartile range (rectangle), median (horizontal line), and mean (X) antibody indices are depicted. When more than one measurement was available during a given time period, the more recent value was used. Full dose and booster dose defined as 100 mcg of mRNA and 50 mcg of mRNA, respectively. Measurements <0.5 and >750 index were included in the calculation as 0.5 and 750, respectively. For the “No dose 3” group, the last follow-up assessment was completed a median of 272 days after dose 2. For the “Dose 3 – full” group, the last follow-up assessment was completed a median of 272 days after dose 2 and 26 days after dose 3. For the “Dose 3 – booster” group, the last follow-up assessment was completed a median of 261 days after dose 2 and 26 days after dose 3. |
Administration of a third dose of mRNA-1273 vaccine resulted in a marked increase in antibody levels, with median indices of 750 (maximum detectable index) a median of 26 days after administration. All but 3 patients administered a third dose (ie, 122/125; 98%) had antibody indices of >7 at follow-up. Among the 11 patients not receiving a third vaccine exposure, 3 (27%) had antibody indices ≤7.
More than 250 days after completion of the primary series, maximal antibody response was demonstrated in only 27% (3/11) of patients not receiving a third dose. In contrast, among patients administered a third dose (full or booster), 99.2% (124/125) demonstrated reactivity at follow-up and 51.2% (64/125) exhibited antibody levels at the maximum detectable level of 750. This antibody response exceeds that observed approximately 1 month after the second vaccine dose and is consistent with recent data on third doses of mRNA vaccines.3 Although the number of patients in the booster subgroup was small (n=12), the strong humoral response to a booster (50 mcg) dose appears comparable to that observed with a full third (100 mcg) dose: mean index (sd) was 564 (269) and 565 (237), for booster and additional dose, respectively.
Excluding patients who developed recognized COVID-19 infection during follow-up minimizes—but does not eliminate—the potential confounding effects of infection on antibody levels. Asymptomatic infection late in 2021 (coinciding with prevalence of the Omicron variant) may have contributed to the higher antibody indices observed late in the follow-up period. Other limitations include the absence of measures of clinical efficacy and cellular immunity. Importantly, there are no data to suggest that higher antibody index values indicate superior ability to neutralize the virus or fight infection.
Our results support the need for a third dose of mRNA-1273 vaccine, whether full or booster dose, for all eligible dialysis patients who received primary vaccination. Continued longitudinal research will help elucidate the need for, and optimal timing of, a fourth dose in this high-risk population.
Ethical Approval
The purpose of this project was to a) implement a practice to improve the quality of patient care, and b) collect patient data regarding the implementation of clinical practice. Under the HHS regulations, these activities do not satisfy the definition of “research” under 45 CFR 46.102 (d). For this reason, no additional study-specific informed consent or institutional review board approval was required for this quality improvement project. This project was reviewed and determined to be quality improvement using standardized criteria from the Office of Human Research Protection. This process takes into account the project’s intent, design, funding, patient risk above standard of care, and protection of health information.
Acknowledgments
Medical writing and editing support was provided by Adam Perahia, MD, of NorthStar Strategic Consulting, LLC, via funding by Fresenius Medical Care.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by Fresenius Medical Care.
Disclosure
LHF, JW, CM, MSA, and JLH are employees of Fresenius Medical Care, Global Medical Office. CJ Is an employee of Spectra Laboratories. CM, MSA, and CJ, own stock in Fresenius Medical Care North America. MSA is the Chief Medical Officer of Fresenius Renal Therapies Group. JLH is the Global Head of Clinical Affairs for Fresenius Medical Care.
References
1. Moreno NF, McAdams R, Goss JA, Galvan NTN. COVID-19 vaccine efficacy and immunogenicity in end-stage renal disease patients and kidney transplant recipients. Curr Transplant Rep. 2022;2022:1–11. doi:10.1007/s40472-022-00366-1
2. Agur T, Ben-Dor N, Herman-Edelstein M, et al. Longevity of humoral response six months following BNT162b2 vaccine in dialysis patients. Front Med. 2022;9:781888. doi:10.3389/fmed.2022.781888
3. Patyna S, Eckes T, Koch BF, et al. Impact of Moderna mRNA-1273 booster vaccine on fully vaccinated high-risk chronic dialysis patients after loss of humoral response. Vaccines. 2022;10:585. doi:10.3390/vaccines10040585
4. Quiroga B, Soler MJ, Ortiz A, et al. Humoral response to third dose of SARS-CoV-2 vaccines in the CKD spectrum. Clin J Am Soc Nephrol. 2022;17:872–876. doi:10.2215/CJN.01770222
5. Rodríguez-Espinosa D, Broseta JJ, Bedini JL, Rodríguez N, Maduell F. Antibody maintenance and breakthrough infections 6 months after complete COVID-19 vaccination with the mRNA-1273 and BNT162b2 vaccines in hemodialysis patients. Clin Kidney J. 2022;15(4):pages 818–819. doi:10.1093/ckj/sfab282
6. Mulhern JG, Fadia A, Patel R, et al. Humoral response to mRNA versus an adenovirus vector-based SARS-CoV-2 vaccine in dialysis patients. Clin J Am Soc Nephrol. 2021;16:1720–1722. doi:10.2215/CJN.06450521
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.