")
Back to Journals » International Journal of Women's Health » Volume 11
Frontal fibrosing alopecia: efficacy of treatment modalities
Authors Gamret AC , Potluri VS , Krishnamurthy K, Fertig RM
Received 17 January 2019
Accepted for publication 27 March 2019
Published 29 April 2019 Volume 2019:11 Pages 273—285
DOI https://doi.org/10.2147/IJWH.S177308
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
A Caresse Gamret,1 V Sumanth Potluri,1 Karthik Krishnamurthy,2 Raymond M Fertig3
1Department of Dermatology and Cutaneous Surgery, University of Miami Miller School of Medicine, Miami, FL, USA; 2Division of Dermatology, Orange Park Medical Center, Orange Park, FL, USA; 3Department of Graduate Medical Education, Orange Park Medical Center, Orange Park, FL, USA
Abstract: Frontal fibrosing alopecia (FFA) is a primary cicatricial alopecia characterized by loss of follicular stem cells, fibrosis, and a receding frontotemporal hairline, with frequent loss of eyebrows, and less commonly, body hair involvement. Diagnosis is clinical and the disease most often affects postmenopausal women. Treatment is difficult with the goal of disease stabilization rather than hair regrowth due to the scarring nature of FFA. To date, there are no randomized controlled trials evaluating efficacy of treatments. Therefore, much of our knowledge is based on small retrospective studies. In this review, we highlight the various and most current treatment options for FFA, including 5-α-reductase inhibitors, intralesional steroids, hydroxychloroquine, topical steroids, topical calcineurin inhibitors, systemic retinoids, pioglitazone, oral antibiotics, minoxidil, excimer laser, and hair transplantation. Currently, 5-α-reductase inhibitors, intralesional steroids, and hydroxychloroquine have the highest level of evidence for treating FFA, while the remaining therapies have variable results and require further data to draw definitive conclusions.
Keywords: frontal fibrosing alopecia, frontal fibrosing alopecia treatment, FFA, FFA therapy
Introduction
Frontal fibrosing alopecia (FFA) is a primary cicatricial alopecia that involves the frontotemporal and parietal hairline, and is commonly accompanied by loss of eyebrows, resulting in progressive band like recession of hair with scarring. It was first described in 1994 by Kossard who described six cases of FFA in postmenopausal women.1 Although the exact prevalence of FFA is unknown, it has increased in recent years.2–4 Additionally, while this clinical entity is most common in postmenopausal, Caucasian women, it can be seen in men,5,6 premenopausal women,7–9 and all races.2,3,10–15
Clinically, FFA presents as perifollicular erythema, hyperkeratosis, and loss of follicular openings, as well as the frontotemporal hairline recession and early eyebrow loss.16 The “lonely hair sign”, where a few terminal hairs remain at the original hairline location, may be seen and aid in diagnosis.17 Progression of disease can lead to loss of axillary, limb, and pubic hair; eyelash loss also occurs and facial vellus hair involvement may lead to facial papules and pigmented macules.2 On dermatoscopy, loss of vellus hair, peripilar casts, perifollicular erythema, and hyperkeratosis are markers of disease.18,19 Histologically, FFA presents as perifollicular fibrosis and T-lymphocytic inflammation centered around the isthmus and infundibular areas of follicles.1 These biopsy findings are indistinguishable from lichen planopilaris (LPP), which manifests as scarring hair loss in discrete patches involving the scalp, rather than the localized hairline specific loss characteristic of FFA. Due to these similarities, FFA is thought to be a distinct clinical variant of LPP, although this remains controversial, and as such, they share many treatment modalities.20
While the cause of FFA remains unknown, genetic, hormonal, and autoimmune factors likely play a role and lead to the loss of both epithelial hair follicle stem cells and immune privilege at the bulge region of the hair follicle, resulting in cytotoxic attack and subsequent fibrosis.2,21,22 The natural history of the disease proceeds with slow, progressive hair loss resulting in recession of the hair line followed by spontaneous disease stabilization. Unfortunately, response to treatment is often underwhelming and currently there are no randomized controlled trials of treatment options. Therefore, it is unclear if treatment induces disease stabilization or if spontaneous remission occurs and is unaltered by interventions.23 Nonetheless, treatment approaches are used with the goal of disease suppression and induction of early stabilization, as hair regrowth is unlikely after significant scaring and loss of follicles occurs. These therapies include 5-α-reductase inhibitors (5ARi), intralesional steroids, hydroxychloroquine, topical steroids, topical calcineurin inhibitors, systemic retinoids, pioglitazone, oral antibiotics, minoxidil, excimer laser, and hair transplantation. This review aims to compile the retrospective studies to determine the efficacy of each modality.
Materials and methods
A PubMed search (1994–2018) was conducted to identify published articles relevant to FFA treatment. The search terms “frontal fibrosing alopecia,” “frontal fibrosing alopecia treatment,” “FFA 5ARi,” “FFA steroids,” “FFA hydroxychloroquine,” “FFA calcineurin inhibitors,” “FFA retinoid,” “FFA pioglitazone,” “FFA antibiotic,” “FFA minoxidil,” “FFA excimer laser,” “FFA hair transplant” were used. Case reports, case series, retrospective reviews, and clinical trials that investigated treatment options and outcomes for FFA were included. After the initial search was performed, references of the articles gathered were reviewed to ensure inclusion of all relevant publications in the present manuscript.
The American College of Physicians grading system was used to rank the level of evidence of each study from high to very low, as outlined below, and is reported in Table 1.24
- High: well-designed randomized controlled trials (RCTs)
- Moderate: RCTs with marked limitations, nonrandomized controlled trials, well designed cohort or case-control studies, and upgraded observational studies
- Low: observational studies or case series
- Very low: downgraded observational studies, downgraded case series, and case reports
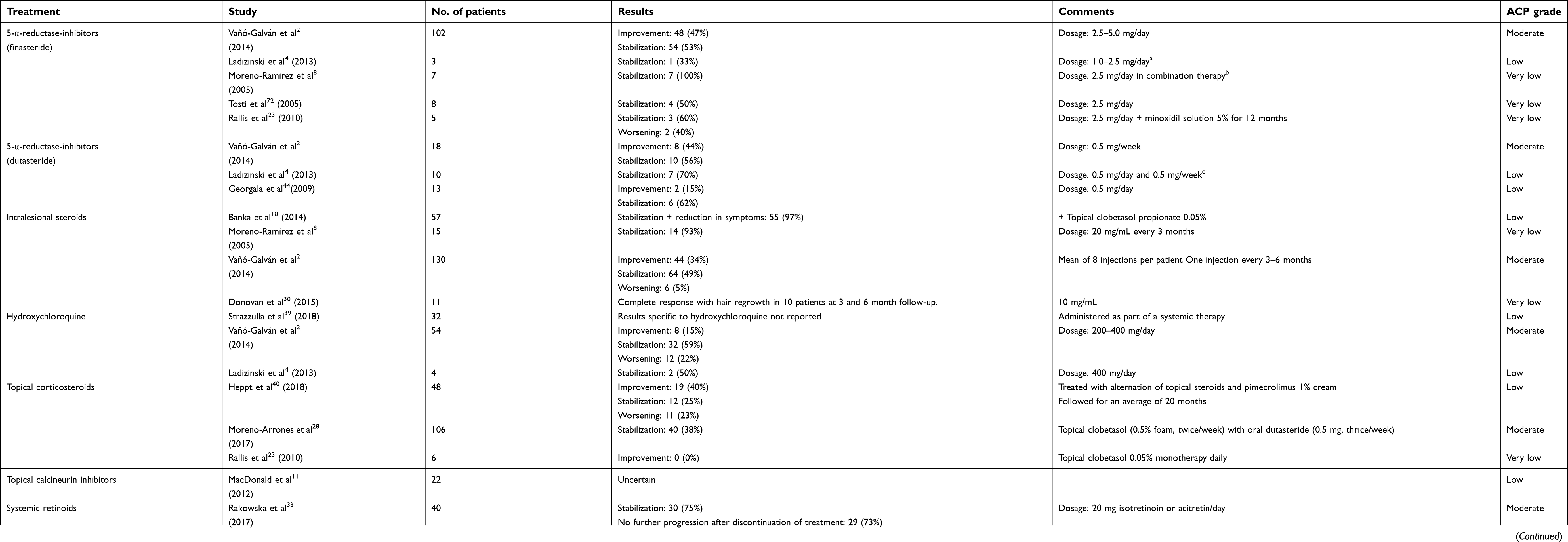 | Table 1 Summary table of FFA treatment studies included in this review. |
5-α-reductase inhibitors
5-α-reductase-inhibitors (5ARi) are amongst the most efficacious treatment options for FFA.25 Finasteride and dutasteride, well established in the treatment of androgenetic alopecia, are antiandrogens, and prevent the enzyme 5-α-reductase from converting testosterone into dihydrotestosterone.26 Finasteride, a type-II 5ARi, prevents this conversion in hair follicles, while dutasteride, a type I and II inhibitor, is less selective and inhibits conversion at hair follicles, and sweat and sebaceous glands.25,27
Vano-Galvan et al, in the largest retrospective study to date, included 120 FFA patients from 12 Spanish centers from 1994 to 2013 treated with both 5ARis.2 Diagnosis was made by histology and clinical presentation. Severity of FFA was based on the area of cicatricial skin produced by the recession of the frontal and temporal hairlines. Severity was classified as mild (0–2.99 cm) or severe (>3 cm) based on the greatest measurement from the frontal or temporal region. Response to therapy was assessed as worsening, stabilized, or improved, based on these measurements from clinical notes and photographic evaluations at visits one year apart. Patients were followed on average for 2.1 years. Of the finasteride group, who received 2.5–5 mg daily as mono or combination therapy, 48 of the 102 patients (47%) showed improvement and 54 (52.9%) showed stabilization. Of the dutasteride treatment group, treated with 0.5 mg weekly as monotherapy or in combination, 8 of 18 patients (44.4%) showed improvement and 10 of 18 (55.6%) showed stabilization of their disease.2
Moreno-Arrones et al conducted a retrospective analytical study of 106 female FFA patients who received oral dutasteride (0.5 mg three times weekly) and topical corticosteroid (clobetasol propionate 0.05% twice weekly). The patients were followed for 1 year and 37.3% achieved stabilization, although none experienced hair regrowth. Of note, this clinical response occurred in the setting of combination therapy of dutasteride and topical steroids, so it is not possible to attribute clinical outcome to the 5ARi alone, and was limited to female patients.28
A retrospective study conducted by Ladizinski et al reviewed 5ARi use in female FFA patients with biopsy confirmed lymphocytic cicatricial alopecia (N=13).4 Of the patients prescribed dutasteride, 7 of 10 (70%) achieved disease stabilization over an average of 28 months, although half were using doxycycline, topical steroids, or topical tacrolimus concurrently. Finasteride was given to 3 patients and stabilization was only seen in 1 (33%). No patients achieved hair regrowth. Exclusions were prior 5ARi’s exposure. Many had failed prior therapies, such as topical/intralesional steroids, topical immunomodulators, oral antibiotics, and hydroxychloroquine.4
Georgala et al reported the retrospective results of one year of dutasteride (0.5 mg/day) use in 13 postmenopausal female FFA patients.29 After 12 months, 61.5% were responders. Specifically, 6 patients (46.1%) had disease stabilization and 2 (15.3%) had improvement by way of evident hair regrowth. All of these patients remained in remission at the 18-month point.29
Moreno-Ramirez and Camacho Martinez reported 7 biopsy-confirmed FFA cases and treatment responses to finasteride.8 The all-female patients were an average of 61.4 years old and presented after 2.5 years of disease. Measurements from the eyebrows and frontal/pre-auricular hairline were used to track disease. The patients were given finasteride 2.5 mg/day, topical minoxidil 5% twice daily, and intralesional triamcinolone acetonide injections (20 mg/mL three times monthly). Progression of disease was halted in all 7 patients who underwent this treatment for an average of 24 months. An increase in hair density was also observed in patients who had concurrent androgenetic alopecia.8
Tosti et al reports a case series of 8 postmenopausal women with FFA treated with finasteride (2.5 mg/day) and topical minoxidil (2% twice daily). Of these patients, 4 (50%) had disease stabilization after 12–18 months of treatment. Again, due to the nature of combination therapy and the natural tendency for FFA to stabilize in time, assessing the effect of 5ARi monotherapy is difficult.
Finally, several case reports tell of success with 5ARi therapies. A woman who developed FFA was treated with finasteride (2.5 mg/day) for a year and experienced substantial scalp hair regrowth as well as reduced erythema and reversal of skin atrophy.30 A premenopausal woman achieved adequate FFA stabilization to allow for artificial hair transplantation after 3 years of dutasteride (0.5 mg/day) and oral minoxidil (1 mg/day).31 Another case was reported of FFA treated with dutasteride (0.5 mg/day) for 6 months in combination with topical pimecrolimus 1% cream twice daily. This treatment resulted in regrowth of eyebrows and moderate regrowth of frontal scalp hair without recurrence in the 6 months of follow-up reported.32
Of the studies evaluating 5ARi efficacy for the treatment of FFA, many demonstrated the ability to stabilize disease and some reported modest hair regrowth. While 5ARis were not effective for all patients, and combination treatment outcomes were often reported which confound results, there was success seen in many patients. For the patient seeking to halt disease progression, especially those who present early in the disease course, a trial of 5ARis should be considered as they have an overall positive treatment outcome. However, it is important to note that 5ARis may have adverse sexual and psychiatric side effects, and may increase breast cancer risk, so they should be prescribed with caution.25 Furthermore, 5ARis are category X drugs and cannot be prescribed to women who are, or are planning to become, pregnant. Finally, to truly tease out the efficacy of 5ARi monotherapy for the treatment of FFA, a prospective, RCT is warranted.
Intralesional steroids
Intralesional corticosteroids are a preferred treatment modality for FFA and are the first-line treatment for LPP.33 They are administered to decrease the dermal inflammatory process and help stabilize disease.34 Treating the inflammation suppresses the T-cell-mediated immune attack of the follicular stem cells and hair follicles.35
A multicenter retrospective study of 130 FFA patients who received intralesional steroids was reported by Vano-Galvan et al. Patients received injections every 3–6 months, with an average of eight injections over the course of treatment. Of those, 44 (34%) patients achieved improvement, 64 (49%) patients achieved stabilization, and 6 (5%) patients had continued disease progression (efficacy data was unavailable for 16 patients). This translates to 83% of patients experiencing a positive clinical response to treatment, which the authors note was the most effective treatment option after 5ARi’s in their study.2
Banka et al reported a retrospective study of 57 FFA patients treated with intralesional triamcinolone acetonide (0.5–3 mL/session, every 6–8 weeks) and daily topical clobetasol 17 propionate 0.05% lotion.10 Patients that had significant symptoms or perifollicular erythema also received tetracycline 500 mg twice daily (N=8), doxycycline 100 mg twice daily (N=5), topical tacrolimus 0.1% (N=11), 5ARi’s (N=3), or hydroxychloroquine (N=2). In 10 patients, the disease progressed initially, but hairline recession stabilized after 4–5 intralesional triamcinolone acetonide injections. The remaining 47 patients showed no progression of disease after initiation of treatment. Interestingly, 3 other patients refused the intralesional steroids and opted instead for topical clobetasol alone; these patients experienced further hairline recession. Arguably, this may provide insight on the treatment outcome of intralesional versus topical steroids, with injections seemingly superior based on this report. None of the patients experienced hairline regrowth although some achieved partial eyebrow regrowth.10
Moreno-Ramirez and Camacho Martinez reported a retrospective review of 15 female FFA patients treated with 20 mg/mL triamcinolone acetonide injections to the frontal hairline and eyebrows, when involved.8 The mean age of the patients was 61.4 years and treatment response was based on measurements from the glabella to the frontal/pre-auricular hairline. The injections were given every 3 months and disease stabilization was achieved in all patients except one who abandoned treatment. Seven women also had female androgenetic alopecia and were concurrently treated with finasteride (2.5 mg/day) and minoxidil 5% twice daily. The authors concluded that intralesional corticosteroids seem to induce FFA stabilization due to a direct anti-inflammatory effect.8
Finally, Donovan et al reports the treatment response to intralesional steroids in patients with eyebrow loss due to FFA. Eleven women with partial to complete eyebrow loss received intralesional triamcinolone acetonide, while 20 other women with FFA eyebrow loss did not.35 The triamcinolone acetonide injections were given at a dose of 10 mg/mL, 0.125 mL per eyebrow at varying intervals. All patients received adjuvant systemic therapy at the time of initial injection, including doxycycline, hydroxychloroquine, or mycophenolate mofetil. Ten patients showed signs of eyebrow hair regrowth at 3 and 6 months. At follow-up, 2 (20%) patients were satisfied with the amount of regrowth and ceased treatment, 6 (60%) patients experienced moderate regrowth, and 2 (20%) patients demonstrated initial regrowth but were later seen to have slight eyebrow hair loss while receiving injections. None of the patients demonstrated treatment-induced skin atrophy. Of note, the 20 patients with FFA and eyebrow hair loss that did not receive intralesional injections did not experience eyebrow hair regrowth. This prompted the authors to conclude that intralesional steroids can be effective at inducing eyebrow regrowth when combined with systemic treatment.35
While there is a lack of high quality evidence to support the use of intralesional steroids for FFA treatment, the available studies report good clinical effect, making this treatment one of the first-line options.2,10,35 Some authors have suggested that 5ARis should be coupled with intralesional steroids when the clinical signs of perifollicular erythema or follicular hyperkeratosis are present.2 Potential side effects of intralesional steroid treatment include skin atrophy and telangiectasias.36
Hydroxychloroquine
Hydroxychloroquine is an antimalarial drug used to treat a wide variety of diseases and is prescribed frequently for patients that present with active signs of FFA, as its anti-lymphocytic effect is thought to be of benefit.37 It acts by dampening the upregulation of T cells, which is responsible for the cell mediated inflammatory reaction that is present in FFA.38
There are several studies that have reported the treatment outcome of administering hydroxychloroquine to patients with FFA. The largest study to date on the treatment outcome of hydroxychloroquine is a multicenter retrospective study of 355 FFA patients. Oral hydroxychloroquine was utilized in 54 patients with doses ranging from 200–400 mg daily. Improvement, as defined by any regrowth of the hair at the hairline, was seen in 8 of 54 (15%) patients, stabilization of disease was achieved in 32 (59%), and worsening of disease occurred in 12 (22%) patients.2
Strazzulla et al conducted a retrospective review of 92 FFA patients. The overall rate of disease stabilization in these 92 patients was 70.7% and average time to stabilization was 10.4 months.39 Of this cohort, 32 patients were administered hydroxychloroquine in conjunction with other systemic therapies. Of the 70.7% that stabilized, these results include the findings of all patient therapies including antibiotics, 5ARis, and corticosteroids, among others, and are not specific to hydroxychloroquine which is a significant limitation. As these results are reported as a conglomerate for all therapies, no conclusions can be drawn on the efficacy of hydroxychloroquine monotherapy from this study. However, the one treatment specific result the authors report was that the outcomes of those treated with hydroxychloroquine were not significantly different from those treated with anti-inflammatory antibiotics (doxycycline/tetracycline/minocycline).39
Ladizinski et al reported a retrospective review of 19 women with FFA treated with various therapies. Of these patients, 4 received hydroxychloroquine (400 mg/day) therapy. Two of the 4 (50%) patients received hydroxychloroquine monotherapy and achieved disease stabilization after an average of 26 months. The other 2 patients received either hydroxychloroquine plus adjuvant class-I topical steroids or hydroxychloroquine plus class-I topical steroids and systemic tacrolimus; both experienced disease progression.4
Cranwell and Sinclair reported a case of a 54-year-old perimenopausal woman with FFA and concomitant female pattern hair loss.21 She was taking hydroxychloroquine 200 mg daily and topical clobetasole diproprionate 0.5% upon presentation. The authors continued her on hydroxychloroquine, dutasteride (0.1 mg/day), and intralesional triamcinolone injections (5 mg/mL every six weeks for 10 months). Female pattern hair loss improved but the FFA progression continued. In this case, the patient’s FFA did not to benefit from the use of hydroxychloroquine and the authors note that disease improvement was only achieved after cessation of application of sunscreen to the forehead.21
Heppt et al reports a patient who received 200–400 mg hydroxychloroquine monotherapy daily and experienced hairline recession of 0.7 cm over the 13 month follow-up period.40 Tolkachjov et al reviewed 7 male patients who presented with FFA. Four received hydroxychloroquine in combination with various other treatments such as, topical clobetasol, pimecrolimus, intralesional steroids, and fluocinonide ointment. Three of the 4 patients achieved stabilization, while no other patients did.41 Finally, a retrospective study of 2 male FFA patients who received hydroxychloroquine (200 mg/day) reports disease stabilization after 15 and 18 months of treatment.42
Given the lack of RCTs studying hydroxychloroquine use for treating FFA, and that many reports use combination therapy, efficacy of hydroxychloroquine monotherapy for FFA remains uncertain. However, there have been reports of disease stabilization with the use of hydroxychloroquine, likely due to its anti-lymphocytic effect. Of note, prescribers should keep in mind hydroxychloroquine has a slow onset of action and peak effectiveness is not achieved until 6–12 months.43 Side effects include gastrointestinal upset, headache, myopathy, and rarely retinal toxicity, but hydroxychloroquine is safe in pregnancy.44
Topical corticosteroids
While intralesional steroids have had some success in FFA treatment, topical corticosteroid efficacy remains questionable. In the Vano-Galvan et al study, topical steroids and topical minoxidil were used in combination with various systemic therapies, although the exact therapies were not reported, and the authors found that clinical response varied based on the systemic therapy utilized (N=276).2 Thus, it seems topical steroids did not make a quantifiable difference in clinical outcomes when incorporated with systemic therapies.2
Additionally, a retrospective study of 106 patients with FFA treated with oral dutasteride (0.5 mg, three times/week) and topical clobetasol (0.5% foam, twice/week), resulted in 37.3% of patients achieving disease stabilization after one year of treatment.28 In a retrospective study, a group of 48 FFA patients were treated with alternating topical high-potency steroids and pimecrolimus 1% cream and followed for an average of 20 months. Therapy started with use of each topical three times weekly and was tapered to eventual steroid discontinuation with long-term pimecrolimus maintenance.40 Subjective improvement was reported in 19 (39.6%) and stabilization in 12 (25%). However, subjective worsening occurred in 11 (22.9%).40 Rallis et al described the treatment outcomes of 6 postmenopausal FFA patients treated with topical clobetasol 0.05% monotherapy daily for 6 months alone compared to no treatment in 6 postmenopausal FFA patients. The authors found that there was no significant improvement in either group and advocated that treatment may not be necessary if disease stabilization has occurred prior to treatment initiation.23
Several case reports detail the use of topical steroids used in combination with other therapies which successfully induced disease stabilization prior to hair transplantation. These combination therapies included topical steroids plus hydroxychloroquine 400 mg and tacrolimus 0.1% ointment,45 intralesional triamcinolone 2.5 mg/mL and finasteride 2 mg daily,6 and topical minoxidil 2% and finasteride 1 mg daily.46 Varying success was seen post-transplant for each regimen and the results of each are discussed in the hair transplantation section.
Topical steroids seem to produce a range of results when paired with other therapies for FFA treatment with some patients obtaining clinical benefit. However, FFA treatment is typically long-term, and topical corticosteroids are prescribed with caution as the side effects of skin atrophy and telangiectasia are seen most commonly with extended use.40 To reduce the risk, it has been proposed to treat FFA with alternating topical steroids and another topical therapy, such as topical calcineurin inhibitors, however this has not been investigated on a large scale.47
Topical calcineurin inhibitors
Topical calcineurin inhibitors (TCIs), tacrolimus and pimecrolimus, are treatment options for a variety of dermatological diseases. They work by blocking calcineurin phosphate, a protein that contributes to cytokine production and activation of T cells.48 Accordingly, they have an anti-inflammatory and immunomodulatory effect. Given that FFA is thought to be caused by T cell-mediated attack of follicular stem cells, TCIs may be a useful treatment option, although there are very few studies at this time.
Heppt et al described 48 patients who received alternating high-potency topical steroids and pimecrolimus 1% cream.40 Both agents were applied three times weekly when disease activity was high. This regimen was gradually tapered to decrease frequency and eventually the topical steroid was discontinued while twice weekly pimecrolimus was continued for long-term maintenance. Subjective improvement was achieved in 19 (39.6%) while stabilization was achieved in 12 (25.0%). However, subjective worsening was reported in 11 (23%). Two patients experienced side effects of erythema and scaling but steroid induced atrophy and telangiectasia were rare.40 MacDonald et al reported a retrospective review of 22 FFA patients who received topical calcineurin inhibitors. This therapy was shown to reduce signs of inflammation but did not slow progression of disease.11 The available studies seem to indicate TCIs may benefit FFA when there are clinical signs of active inflammation present, although, conclusions cannot be drawn as to the disease alteration based on current evidence.
Systemic retinoids
Some authors suggest the use of retinoids for those patients diagnosed with LPP that have not responded to other treatment options,49 and there have been several studies that reported variable success in treating LPP with systemic retinoids.50–53 However, the use of retinoids for FFA, in contrast to LPP, has only been documented in two studies. Although the mechanism of retinoids is complex, they may lead to normalization of the hair follicular keratinocyte antigen expression and suppression of inflammatory cellular infiltration, reducing the T cell-mediated reaction in FFA.54,55
Rakowska et al conducted a 10-year retrospective study to assess the efficacy of systemic retinoids in the treatment of FFA (N=54). The diagnosis was determined by clinical and trichoscopic evaluation. Patients were treated with 20 mg isotretinoin daily (N=29) or 20 mg of acitretin daily (N=11).33 The control group received finasteride 5 mg daily (N=14). Measurement of the distance between the frontal hairline and the glabellar crease was used to determine disease progression. The mean duration of treatment in the retinoid cohort was 13.5 months. The primary goal of treatment was to achieve disease stabilization, defined as no further recession of hairline after one year of treatment, with a secondary aim to maintain stabilization one year after treatment ceased. In the isotretinoin group, 22 of 29 (76%) achieved stabilization at 12 months and 21 of 29 (72%) had no further progression of the disease one year after discontinuation of treatment. In the acitretin cohort, 8 of 11 patients (73%) achieved both stabilization after 12 months of treatment and no further progression of disease one year after discontinuation of treatment.33 However, in patients treated with finasteride, only 6 of 14 patients (43%) achieved both stabilization after 12 months of treatment and no further progression after discontinuation of treatment. Neither treatment group reported adverse side effects. Interestingly, patients treated with retinoid monotherapy in this study showed higher stabilization rates than patients in the finasteride control group.33 These results warrant further evaluation with larger prospective, RCTs to evaluate the efficacy of systemic retinoids for FFA.33
In the only other report of isotretinoin use for FFA, Pirmez et al treated 3 female FFA patients’ facial papules with 3 months of isotretinoin (20 mg/day titrated to 40 mg/day).56 These patient were all on concurrent finasteride 5 mg/day and various topicals, however, within one month of initiation of isotretinoin the authors report a dramatic reduction in the unsightly papules, with complete disappearance achieved after 3 months. This report may support the use of isotretinoin for FFA facial papules, although the hairline involvement showed no clinical change with this therapy.56
While retinoids lack RCTs to corroborate their use for FFA, the two available studies seem to show some promise and may warrant a trial in certain patients. Of note, oral retinoids have a wide spectrum of adverse effects including reproductive, cutaneous, and neurological manifestations.57 Isotretinoin is also a category X drug that causes fetal malformations and should be prescribed with caution to women of childbearing age.58
Pioglitazone
Pioglitazone, a synthetic peroxisome proliferator-activated receptor (PPAR)-γ ligand traditionally used to manage type 2 diabetes mellitus, is a proposed treatment for cicatricial alopecia.59,60 PPAR-γ is an endogenous transcription factor that normally regulates peroxisomes and lipid metabolism, appropriate expression is necessary for function of pilosebaceous units, and decreased expression is evident in cicatricial alopecia.61,62 Considering FFA is a primary cicatricial alopecia, pioglitazone is a potential treatment option, however, there are very few reports of trials for FFA. Pioglitazone has, however, been used more extensively in LPP, with mixed results.
A report of 24 LPP patients who used pioglitazone (15–30 mg/day) resulted in remission in 5 patients and improvement in 12, however, 4 discontinued therapy due to the side effects, which included calf pain, nausea, dizziness, lightheadedness, and hives.63 Mesinkovska et al reported a retrospective case analysis of 22 LPP patients treated with pioglitazone.59 It was found that pioglitazone (15 mg/day) was effective in stabilizing disease progression and inflammation in 72.7% of patients. Hair regrowth was also noted in 6 (27.3%) of the patients, however, 2 patients relapsed after discontinuing pioglitazone. Side effects included lower-extremity edema in 50% of patients and weight gain in 41% of patients and 9 ultimately discontinued use because of these side effects.59 In another retrospective study of 22 LPP patients who received a year of pioglitazone 15 mg/day, 3 achieved cessation of disease activity and 4 had clinical improvement, although disease activity resumed after treatment cessation.64 Finally, a case report by Mirmirani and Karnik tells of successful treatment of LPP using 15 mg pioglitazone daily. The patient had failed multiple previous therapies but 8 months of pioglitazone resulted in disease stabilization; there was no further inflammation or hair loss after one year post-treatment follow-up.62
As demonstrated above, pioglitazone seems to have some success in LPP, however, in the only report of pioglitazone therapy for FFA, disease stabilization was not achieved after 8 months of monotherapy in 1 patient.4
Currently, there is a lack of evidence to support the use of pioglitazone for FFA, and while patients with LPP have shown some response with the treatment, those result are mixed as well. Further high quality RCTs are warranted in this field before definitive conclusions as to efficacy can be made. However, due to the side effect profile, including edema, hypoglycemia, heart failure, bone fractures, and upper respiratory tract infection, careful consideration should be given when prescribing these medications for FFA.65
Oral tetracyclines
Tetracyclines are antibiotics that are commonly used to treat various gram-positive and gram-negative bacterial infections.66 In addition to their bacteriostatic antimicrobial properties, tetracyclines, including doxycycline and minocycline are known to have anti-inflammatory effects.67 This anti-inflammatory property is the reason why these medications have been used to treat symptoms in FFA.
In a retrospective report, Strazzulla et al found that FFA patients treated with doxycycline, tetracycline, or minocycline (N=65) had no difference in outcomes compared to hydroxychloroquine (N=32) but were more likely to experience adverse side effects compared to other treatments (P=0.0189). These antimicrobial adverse effects included nausea, candida infection, esophagitis, lightheadedness, photosensitivity, and skin eruption.39 Banka et al reports the use of doxycycline (100 mg twice daily) or tetracycline (500 mg twice daily) in combination with intralesional triamcinolone acetonide injections in 13 FFA patients. The role of the tetracyclines was to treat significant inflammation or perifollicular erythema, and all patients achieved disease stability.10 Samrao et al performed a retrospective case review in which 4 FFA patients received doxycycline (dose not reported); after 6 months 1 patient responded to therapy and 1 patient partially responded, as measured by a reduction in the Lichen Planopilaris Activity Index. Unfortunately, 3 of the patients also reported adverse effects including photosensitive reaction and gastrointestinal upset.12 Lastly, in a retrospective study of 3 FFA patients treated with a combination of dutasteride and doxycycline for a mean duration of 31 months, 2 achieved disease stabilization.4 It would appear that tetracyclines may benefit FFA patients, however, optimal dosing has yet to be established; side effects may limit use.
Minoxidil
Topical minoxidil is a treatment that has long been used for male and female pattern hair loss, to good effect. It is typically used twice daily, continually, to maintain hair regrowth. Side effects are relatively uncommon but can include itching or contact dermatitis.68 While its exact mechanism of action is unknown, it likely promotes hair follicle angiogenesis through increased vascular endothelial growth factor expression and inhibited fibroblast proliferation, which increases hair growth and count.68,69
While minoxidil monotherapy is likely to be of little benefit to FFA,4,65,70,71 it has been used as adjuvant therapy in several studies previously discussed. One case series used oral finasteride 2.5 mg/day in combination with topical minoxidil 2% twice daily in 8 FFA patients, of which 50% achieved disease stabilization after 12–18 months of therapy.72 Tan et al tells of 2 patients treated with intralesional steroid injections and topical minoxidil who achieved disease stabilization, however, the time to stabilization was not reported and disease stabilization may have been due to the natural course of FFA.9 Finally, a premenopausal woman with FFA treated with dutasteride 0.5 mg daily and oral minoxidil 1 mg daily for 3 years resulted in disease stabilization.31 Based on these findings it is reasonable to conclude that minoxidil may be most beneficial when combined with other therapies for the treatment of FFA and when there is a condition of mixed FFA and androgenetic alopecia, which is common.
Excimer laser
The excimer laser, which delivers 308 nm wavelength of ultraviolet-B light, is widely used in the treatment of various dermatological diseases, including vitiligo, psoriasis, and alopecia areata, among others.73 Treatment is thought to be beneficial for inflammatory skin disorders through modulating T-lymphocytes and cytokine profiles.74 Given the lymphocyte involvement and inflammatory nature of FFA, excimer laser may be a viable treatment option, particularly in patients with signs of active inflammation. Unfortunately, there have been no published reports of its use for FFA,65 although two studies do report the use of excimer laser for LPP.
In the Vavricka et al study, 13 LPP patients were treated with an average of 10 excimer laser treatments and 3 responded—2 of which had increased hair growth and 1 had decreased pruritus/erythema.75 Navarini et al also treated patients with LPP and its variants, including some FFA patients, with twice weekly excimer laser. This treatment was successful in all 13 patients, as evidenced by decreased signs of inflammation. Furthermore, increased hair growth occurred in 3 patients, but was only sustained in 2 patients after treatment cessation.74 Given a lack of RCTs regarding FFA treatment with excimer laser there is insufficient evidence for or against its use, however, from a theoretical perspective it may benefit those with an active inflammatory component.
Hair transplantation
It is easy to understand that FFA can be both disfiguring and distressing for patients, especially given the difficulty to treat and achieve hair regrowth.76 This can leave patients desperate for help, leading many to inquire about hair transplantation. Unfortunately, there have been limited studies investigating the use of hair transplantation in patients with FFA, and the few published case reports demonstrate mixed results. Nusbaum and Nusbaum reported the first case of hair transplantation for a man with FFA. The transplanted hair began to grow normally for 15 months after the procedure, but progression of disease destroyed the transplanted follicles and by 4 years essentially all transplanted follicles had been lost.6 Gurfinkiel et al also performed hair transplantation on an FFA patient who was treated with topical betamethasone, topical minoxidil 2%, and oral finasteride (1 mg/day) post-transplant. Hair growth was sustained and 85% of follicles remained after 6 years.46
Jimenez and Poblet performed hair transplantation on 3 female FFA patients whom initially showed promising results, however, by the 4 year mark nearly all grafted hairs had been lost.77 Finally, Liu et al reported successful outcomes of hair transplantation in 2 patients, 1 with FFA and 1 with LPP and FFA.45 Results were best seen one year post-transplant and graft survival was maintained during the 3–4 year follow-up period. They concluded that transplantation should only be considered for patients with at least 2 years of clinical remission and advocate for follow-up every 4–6 months post-procedure to allow for medication initiation based on outcomes.45
Ultimately, the published hair transplantation outcomes for FFA do not lend themselves to making broad recommendations for all patients, except to say that appropriate patient selection is important as disease stabilization is a prerequisite. Patient should also be counselled to keep expectations appropriately low, as some transplantations fail with time.
Conclusion
FFA is a primary cicatricial alopecia that is increasing in prevalence and difficult to treat, causing marked distress to patients.2 Currently, there are no randomized controlled trials evaluating efficacy of treatments and much of what we know is based on small scale retrospective studies which report outcomes primarily involving a combination of therapies. This review serves to compile the current literature on the various treatment options to provide evidence-based guidance to practitioners and to highlight the need for further research in this area. The treatments reviewed include 5ARis, intralesional steroids, hydroxychloroquine, topical steroids, topical calcineurin inhibitors, systemic retinoids, pioglitazone, oral antibiotics, minoxidil, excimer laser, and hair transplantation. It is our assessment that 5ARis, intralesional steroids, and hydroxychloroquine have the highest level of evidence for use at this time and should be among the first-line treatment options to induce disease stabilization in patients. The remaining therapies may have some efficacy in the treatment of FFA and can be used as adjuncts, particularly TCIs and excimer laser therapy when there are clinical signs of active inflammation present. However, more data is needed to draw definitive conclusions.
Disclosure
Dr Karthik Krishnamurthy has been a speaker for Regeneron, Sanofi-Genzyme, Abbvie, and Janssen. Dr Karthik Krishnamurthy reports personal fees from Regeneron, Sanofi-Genzyme, Janssen, and Abbvie, outside the submitted work. The other authors report no conflicts of interest in this work.
References
1. Kossard S. Postmenopausal frontal fibrosing alopecia: scarring alopecia in a pattern distribution. Arch Dermatol. 1994;130(6):770–774. doi:10.1001/archderm.1994.01690060100013
2. Vañó-Galván S, Molina-Ruiz AM, Serrano-Falcón C, et al. Frontal fibrosing alopecia: A multicenter review of 355 patients. J Am Acad Dermatol. 2014;70(4):670–678. doi:10.1016/j.jaad.2013.12.003
3. Chew A-L, Bashir SJ, Wain EM, Fenton DA, Stefanato CM. Expanding the spectrum of frontal fibrosing alopecia: A unifying concept. J Am Acad Dermatol. 2010;63(4):653–660. doi:10.1016/J.JAAD.2009.09.020
4. Ladizinski B, Bazakas A, Selim MA, Olsen EA. Frontal fibrosing alopecia: A retrospective review of 19 patients seen at Duke University. J Am Acad Dermatol. 2013;68(5):749–755. doi:10.1016/j.jaad.2012.09.043
5. Kossard S, Shiell RC. Frontal fibrosing alopecia developing after hair transplantation for androgenetic alopecia. Int J Dermatol. 2005;44(4):321–323. doi:10.1111/j.1365-4632.2004.02251.x
6. Nusbaum BP, Nusbaum AG. Frontal fibrosing alopecia in a man: results of follicular unit test grafting. Dermatol Surg. 2010;36(6):959–962. doi:10.1111/j.1524-4725.2010.01580.x
7. Faulkner CF, Wilson NJ, Jones SK. Frontal fibrosing alopecia associated with cutaneous lichen planus in a premenopausal woman. Australas J Dermatol. 2002;43(1):65–67. doi:10.1046/j.1440-0960.2002.00558.x
8. Moreno-Ramírez D, Martínez FC. Frontal fibrosing alopecia: A survey in 16 patients. J Eur Acad Dermatol Venereol. 2005;19(6):700–705. doi:10.1111/j.1468-3083.2005.01291.x
9. Tan KT, Messenger AG. Frontal fibrosing alopecia: clinical presentations and prognosis. Br J Dermatol. 2009;160(1):75–79. doi:10.1111/j.1365-2133.2008.08861.x
10. Banka N, Mubki T, Bunagan MJK, McElwee K, Shapiro J. Frontal fibrosing alopecia: a retrospective clinical review of 62 patients with treatment outcome and long-term follow-up. Int J Dermatol. 2014;53(11):1324–1330. doi:10.1111/ijd.12479
11. MacDonald A, Clark C, Holmes S. Frontal fibrosing alopecia: a review of 60 cases. J Am Acad Dermatol. 2012;67(5):955–961. doi:10.1016/j.jaad.2011.12.038
12. Samrao A, Chew A-L, Price V. Frontal fibrosing alopecia: a clinical review of 36 patients. Br J Dermatol. 2010;163(6):1296–1300. doi:10.1111/j.1365-2133.2010.09965.x
13. Miteva M, Whiting D, Harries M, Bernardes A, Tosti A. Frontal fibrosing alopecia in black patients. Br J Dermatol. 2012;167(1):208–210. doi:10.1111/j.1365-2133.2012.10809.x
14. Dlova NC, Jordaan HF, Skenjane A, Khoza N, Tosti A. Frontal fibrosing alopecia: a clinical review of 20 black patients from South Africa. Br J Dermatol. 2013;169(4):939–941. doi:10.1111/bjd.12424
15. Inui S, Nakajima T, Shono F, Itami S. Dermoscopic findings in frontal fibrosing alopecia: report of four cases. Int J Dermatol. 2008;47(8):796–799. doi:10.1111/j.1365-4632.2008.03681.x
16. Ross EK, Tan E, Shapiro J. Update on primary cicatricial alopecias. J Am Acad Dermatol. 2005;53(1):1–37. doi:10.1016/J.JAAD.2004.06.015
17. Tosti A, Miteva M, Torres F. Lonely Hair. Arch Dermatol. 2011;147(10):1240. doi:10.1001/archdermatol.2011.261
18. Tosti A. Dermoscopy of the Hair and Nails. 2nd Edition.
19. Errichetti E, Stinco G. Dermoscopy in general dermatology: a practical overview. Dermatol Ther (Heidelb). 2016;6(4):471–507. doi:10.1007/s13555-016-0141-6
20. Rácz E, Gho C, Moorman PW, Noordhoek Hegt V, Neumann HAM. Treatment of frontal fibrosing alopecia and lichen planopilaris: a systematic review. J Eur Acad Dermatol Venereol. 2013;27(12):1461–1470. doi:10.1111/jdv.12139
21. Cranwell WC, Sinclair R. Frontal fibrosing alopecia: regrowth following cessation of sunscreen on the forehead. Australas J Dermatol. 2018;1:1–2. doi:10.1111/ajd.12833
22. Harries MJ, Jimenez F, Izeta A, et al. Lichen planopilaris and frontal fibrosing alopecia as model epithelial stem cell diseases. Trends Mol Med. 2018;24(5):435–448. doi:10.1016/j.molmed.2018.03.007
23. Rallis E, Gregoriou S, Christofidou E, Rigopoulos D. Frontal fibrosing alopecia: to treat or not to treat? J Cutan Med Surg. 2010;14(4):161–166. doi:10.2310/7750.2010.09041
24. Qaseem A, Snow V, Owens DK, Shekelle P. The development of clinical practice guidelines and guidance statements of the American college of physicians: summary of methods. Ann Intern Med. 2010;153(3):194. doi:10.7326/0003-4819-153-3-201008030-00010
25. Murad A, Bergfeld W. 5-alpha-reductase inhibitor treatment for frontal fibrosing alopecia: an evidence-based treatment update. J Eur Acad Dermatol Venereol. 2018;32(8):1385–1390. doi:10.1111/jdv.14930
26. Yamana K, Labrie F, Luu-The V. Human type 3 5α-reductase is expressed in peripheral tissues at higher levels than types 1 and 2 and its activity is potently inhibited by finasteride and dutasteride. Horm Mol Biol Clin Investig. 2010;2(3):293–299. doi:10.1515/HMBCI.2010.035
27. Bayne EK, Flanagan J, Einstein M, et al. Immunohistochemical localization of types 1 and 2 5α-reductase in human scalp. Br J Dermatol. 1999;141(3):481–491. doi:10.1046/j.1365-2133.1999.03042.x
28. Moreno-Arrones OM, Saceda-Corralo D, Fonda-Pascual P, et al. Frontal fibrosing alopecia: clinical and prognostic classification. J Eur Acad Dermatol Venereol. 2017;31(10):1739–1745. doi:10.1111/jdv.14287
29. Georgala S, Katoulis AC, Befon A, Danopoulou I, Georgala C. Treatment of postmenopausal frontal fibrosing alopecia with oral dutasteride. J Am Acad Dermatol. 2009;61(1):157–158. doi:10.1016/j.jaad.2008.12.026
30. Donovan JC. Finasteride-mediated hair regrowth and reversal of atrophy in a patient with frontal fibrosing alopecia. JAAD Case Rep. 2015;1(6):353. doi:10.1016/J.JDCR.2015.08.003
31. Cranwell WC, Sinclair R. Familial frontal fibrosing alopecia treated with dutasteride, minoxidil and artificial hair transplantation. Australas J Dermatol. 2017;58(3):e94–e96. doi:10.1111/ajd.12499
32. Katoulis A, Georgala S, Bozi E, Papadavid E, Kalogeromitros D, Stavrianeas N. Frontal fibrosing alopecia: treatment with oral dutasteride and topical pimecrolimus. J Eur Acad Dermatol Venereol. 2009;23(5):580–582. doi:10.1111/j.1468-3083.2008.02963.x
33. Rakowska A, Gradzinska A, Olszewska M, Rudnicka L. Efficacy of isotretinoin and acitretin in treatment of frontal fibrosing alopecia: retrospective analysis of 54 cases. J Drugs Dermatol. 2017;16(10):988–992.
34. Martínez-Pérez M, Churruca-Grijelmo M. Frontal fibrosing alopecia: an update on epidemiology and treatment. Actas Dermosifiliogr. 2015;106(9):757–758. doi:10.1016/j.ad.2014.12.002
35. Donovan JC, Samrao A, Ruben BS, Price VH. Eyebrow regrowth in patients with frontal fibrosing alopecia treated with intralesional triamcinolone acetonide. Br J Dermatol. 2010;163(5):1142–1144. doi:10.1111/j.1365-2133.2010.09994.x
36. Srivastava S, Patil AN, Prakash C, Kumari H. Comparison of intralesional triamcinolone acetonide, 5-fluorouracil, and their combination for the treatment of keloids. Adv Wound Care. 2017;6(11):393–400. doi:10.1089/wound.2017.0741
37. Contin LA, Martins Da Costa Marques ER, Noriega L. Frontal fibrosing alopecia coexisting with lupus erythematosus: poor response to hydroxychloroquine. Skin Appendage Disord. 2017;2(3–4):162–165. doi:10.1159/000452925
38. Al-Bari MAA. Chloroquine analogues in drug discovery: new directions of uses, mechanisms of actions and toxic manifestations from malaria to multifarious diseases. J Antimicrob Chemother. 2015;70(6):1608–1621. doi:10.1093/jac/dkv018
39. Strazzulla LC, Avila L, Li X, Lo Sicco K, Shapiro J. Prognosis, treatment, and disease outcomes in frontal fibrosing alopecia: A retrospective review of 92 cases. J Am Acad Dermatol. 2018;78(1):203–205. doi:10.1016/j.jaad.2017.07.035
40. Heppt MV, Letulé V, Laniauskaite I, et al. Frontal fibrosing alopecia: a retrospective analysis of 72 patients from a German academic center. Facial Plast Surg. 2018;34(1):88–94. doi:10.1055/s-0037-1615281
41. Tolkachjov SN, Chaudhry HM, Camilleri MJ, Torgerson RR. Frontal fibrosing alopecia among men: A clinicopathologic study of 7 cases. J Am Acad Dermatol. 2017;77(4):683–690.e2. doi:10.1016/j.jaad.2017.05.045
42. Alegre-Sánchez A, Saceda-Corralo D, Bernárdez C, Molina-Ruiz AM, Arias-Santiago S, Vañó-Galván S. Frontal fibrosing alopecia in male patients: a report of 12 cases. J Eur Acad Dermatol Venereol. 2017;31(2):e112–e114. doi:10.1111/jdv.13855
43. Van Beek MJ, Piette WW. Antimalarials. Dermatol Clin. 2001;19(1):147–60, ix. doi:10.1016/S0733-8635(05)70236-9
44. Fertig R, Aleid NM, Antonella T. Therapeutic options in frontal fibrosing alopecia. Expert Opin Orphan Drugs. 2016;4(5):461–468. doi:10.1517/21678707.2016.1173539
45. Liu Y-CS, Jee S-H, Chan J-YL. Hair transplantation for the treatment of lichen planopilaris and frontal fibrosing alopecia: A report of two cases. Australas J Dermatol. 2018;59(2):e118–e122. doi:10.1111/ajd.12682
46. Gurfinkiel A, Garcia-Igarza H. Hair transplantation in a patient with frontal fibrosing alopecia associated with lichen scleroatrophicus vulvae. Dermatologia Argentina. 2011;17:110–115.
47. Wollenberg A, Bieber T. Proactive therapy of atopic dermatitis–an emerging concept. Allergy. 2009;64(2):276–278. doi:10.1111/j.1398-9995.2008.01803.x
48. Wong E, Kurian A. Off-label uses of topical calcineurin inhibitors. Skin Therapy Lett. 2016;21(1):8–10. Available from:
49. Spano F, Donovan JC. Efficacy of oral retinoids in treatment-resistant lichen planopilaris. J Am Acad Dermatol. 2014;71(5):1016–1018. doi:10.1016/j.jaad.2014.06.013
50. Farah RS, Ferguson NN, Swick BL. Lichen planopilaris. Cutis. 2013;92:1. doi:10.1111/j.1529-8019.2008.00206.x
51. Tan E, Martinka M, Ball N, Shapiro J. Primary cicatricial alopecias: clinicopathology of 112 cases. J Am Acad Dermatol. 2004;50(1):25–32. doi:10.1016/j.jaad.2003.04.001
52. Spencer LA, Hawryluk EB, English JC. Lichen planopilaris: retrospective study and stepwise therapeutic approach. Arch Dermatol. 2009;145(3):333–334. doi:10.1001/archdermatol.2008.590
53. Assouly P, Reygagne P. Lichen planopilaris: update on diagnosis and treatment. Semin Cutan Med Surg. 2009;28(1):3–10. doi:10.1016/j.sder.2008.12.006
54. Beckenbach L, Baron JM, Merk HF, Löffler H, Amann PM. Retinoid treatment of skin diseases. Eur J Dermatol. 2015;25(5):384–391. doi:10.1684/ejd.2015.2544
55. Lyakhovitsky A. Frontal fibrosing alopecia update. World J Dermatol. 2015;4(1):33. doi:10.5314/wjd.v4.i1.33
56. Pirmez R, Duque-Estrada B, Barreto T, Quintella DC, Cuzzi T. Successful treatment of facial papules in frontal fibrosing alopecia with oral isotretinoin. Skin Appendage Disord. 2017;3(2):111–113. doi:10.1159/000464334
57. Brelsford M, Beute TC. Preventing and managing the side effects of isotretinoin. Semin Cutan Med Surg. 2008;27(3):197–206. doi:10.1016/j.sder.2008.07.002
58. McLane J. Analysis of common side effects of isotretinoin. J Am Acad Dermatol. 2001;45(5):S188–S94. doi:10.1067/mjd.2001.113719
59. Mesinkovska NA, Tellez A, Dawes D, Piliang M, Bergfeld W. The use of oral pioglitazone in the treatment of lichen planopilaris. J Am Acad Dermatol. 2015;72(2):355–356. doi:10.1016/j.jaad.2014.10.036
60. Imanishi H, Ansell DM, Chéret J, et al. Epithelial-to-mesenchymal stem cell transition in a human organ: lessons from lichen planopilaris. J Invest Dermatol. 2018;138(3):511–519. doi:10.1016/J.JID.2017.09.047
61. Karnik P, Tekeste Z, McCormick TS, et al. Hair follicle stem cell-specific PPARγ deletion causes scarring alopecia. J Invest Dermatol. 2009;129(5):1243–1257. doi:10.1038/JID.2008.369
62. Mirmirani P, Karnik P. Lichen planopilaris treated with a peroxisome proliferator-activated receptor gamma agonist. Arch Dermatol. 2009;145(12):1363–1366. doi:10.1001/archdermatol.2009.283
63. Baibergenova A, Walsh S. Use of pioglitazone in patients with lichen planopilaris. J Cutan Med Surg. 2012;16(2):97–100. doi:10.2310/7750.2011.11008
64. Spring P, Spanou Z, de Viragh PA. Lichen planopilaris treated by the peroxisome proliferator activated receptor-γ agonist pioglitazone: lack of lasting improvement or cure in the majority of patients. J Am Acad Dermatol. 2013;69(5):830–832. doi:10.1016/j.jaad.2013.04.066
65. Fertig R, Tosti A. Frontal fibrosing alopecia treatment options. Intractable Rare Dis Res. 2016;5(4):314–315. doi:10.5582/irdr.2016.01065
66. Rok J, Buszman E, Delijewski M, Otręba M, Beberok A, Wrześniok D. Effect of tetracycline and UV radiation on melanization and antioxidant status of melanocytes. J Photochem Photobiol B. 2015;148:168–173. doi:10.1016/j.jphotobiol.2015.04.009
67. Brodersen DE, Clemons WM, Carter AP, Morgan-Warren RJ, Wimberly BT, Ramakrishnan V. The structural basis for the action of the antibiotics tetracycline, pactamycin, and hygromycin B on the 30S ribosomal subunit. Cell. 2000;103(7):1143–1154. doi:10.1016/S0092-8674(00)00216-6
68. Herskovitz I, Tosti A. Female pattern hair loss. Int J Endocrinol Metab. 2013;11(4):e9860. doi:10.5812/ijem.9860
69. Blumeyer A, Tosti A, Messenger A, et al. Evidence-based (S3) guideline for the treatment of androgenetic alopecia in women and in men. J Dtsch Dermatol Ges. 2011;9(Suppl 6):S1–S57. doi:10.1111/j.1610-0379.2011.07802.x
70. Naz E, Vidaurrazaga C, Hernandez-Cano N, et al. Postmenopausal frontal fibrosing alopecia. Clin Exp Dermatol. 2003;28(1):25–27. doi:10.1046/j.1365-2230.2003.01131.x
71. Kossard S, Lee M-S, Wilkinson B. Postmenopausal frontal fibrosing alopecia: A frontal variant of lichen planopilaris. J Am Acad Dermatol. 1997;36(1):59–66. doi:10.1016/S0190-9622(97)70326-8
72. Tosti A, Piraccini BM, Iorizzo M, Misciali C. Frontal fibrosing alopecia in postmenopausal women. J Am Acad Dermatol. 2005;52(1):55–60. doi:10.1016/j.jaad.2004.05.014
73. Mehraban S, Feily A. 308nm excimer laser in dermatology. J lasers Med Sci. 2014;5(1):8–12. Available from:
74. Navarini A, Kolios A, Prinz-Vavricka B. Low-dose excimer 308-nm laser for treatment of lichen planopilaris. Arch Dermatol. 2011;147(11):1325–1326. doi:10.1001/archdermatol.2011.335
75. Vavricka BP, Haug S, Eliades I, Trueb R. 308-nm excimer laser treatment of lichen planopilaris of the scalp. Dermatology. 2006;213:74.
76. Cevasco NC, Bergfeld WF, Remzi BK, de Knott HR. A case-series of 29 patients with lichen planopilaris: the Cleveland clinic foundation experience on evaluation, diagnosis, and treatment. J Am Acad Dermatol. 2007;57(1):47–53. doi:10.1016/j.jaad.2007.01.011
77. Jiménez F, Poblet E. Is hair transplantation indicated in frontal fibrosing alopecia? The results of test grafting in three patients. Dermatol Surg. 2013;39(7):1115–1118. doi:10.1111/dsu.12232
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.