")
Back to Journals » Clinical Interventions in Aging » Volume 15
Usefulness of FRAIL Scale in Heart Valve Diseases
Authors Duchnowski P , Szymański P, Kuśmierczyk M, Hryniewiecki T
Received 23 November 2019
Accepted for publication 10 January 2020
Published 9 July 2020 Volume 2020:15 Pages 1071—1075
DOI https://doi.org/10.2147/CIA.S239054
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Richard Walker
Piotr Duchnowski,1 Piotr Szymański,1 Mariusz Kuśmierczyk,2 Tomasz Hryniewiecki1
1Institute of Cardiology, Department of Acquired Cardiac Defects, Warsaw, Poland; 2Institute of Cardiology, Department of Cardiosurgery and Transplantology, Warsaw, Poland
Correspondence: Piotr Duchnowski
Department of Acquired Cardiac Defects, Institute of Cardiology, Alpejska 42, Warsaw 04-628, Poland
Tel +48 3434191
Email [email protected]
Background: The frailty syndrome is a serious health problem for an aging population. The occurrence of frailty in the group of symptomatic patients undergoing heart valve surgery may have additional clinical implications. The predictive ability of the FRAIL scale in patients undergoing heart valve surgery during a 30-day follow-up has not yet been described.
Patients and Methods: A prospective study was conducted on a group of consecutive patients with hemodynamically significant valve disease (aortic stenosis, aortic regurgitation, mitral stenosis and mitral regurgitation) that underwent elective valve surgery in 2016– 2019. The primary endpoint was 30-day mortality. Univariate analysis, followed by multivariate regression analysis, was performed.
Results: The study group included 672 consecutive patients (aortic valve stenosis, aortic regurgitation, mitral stenosis and mitral regurgitation) who underwent replacement or repair of the valve. Twenty-five patients died during the 30-day follow-up. At multivariate analysis, FRAIL scale result (OR 2.802; 95% CI 1.275– 6.157; p=0.01) and red cell distribution width (RDW) (OR 1.810; 95% CI 1.181– 2.775; p=0.006) remained independent predictors of the primary endpoint.
Conclusion: The presented study showed the predictive ability of the FRAIL scale result in patients undergoing heart valve surgery for 30-day mortality.
Keywords: valve surgery, EuroSCORE II, frailty syndrome, FRAIL scale
Introduction
Frailty syndrome is a serious health problem for an aging population. With age, the susceptibility of the human body to the destructive influence of intra- and extra-environmental factors increases, while the body’s adaptability decreases. For a better understanding of the individual diversity of the rate of aging, the concept of frailty is used. Frailty syndrome is a consequence of a decrease in the physiological reserves of many organs.1,3 The factors responsible for the development of the frailty syndrome may be chronic inflammation, hormonal disturbances, osteoporosis, coexistence of other comorbidities or social factors such as bad financial situation or social isolation. To date, it has been shown that the occurrence of frailty syndrome is associated with an increased risk of cognitive impairment, disability and death.4 In clinical practice, the lack of consensus regarding the gold diagnostic standard makes it difficult to accurately assess the severity of frailty syndrome. This results in a large variety of scales used in scientific research. The FRAIL scale is one of the available tools used to assess the occurrence of the frailty syndrome. The FRAIL scale estimates the occurrence of 5 components: fatigue, resistance, aerobic, illness and loss of weight. The presence of 3 out of 5 indicates the presence of frailty syndrome.5,6
Patients undergoing heart valve surgery are at risk of serious postoperative complications, including death. The co-occurrence of preoperative loads such as frailty syndrome may additionally increase this risk.7,11 In the risk assessment of cardiac surgery, risk calculators are used – in European conditions, EuroSCORE II is most often used. However, the reliability of these calculators is limited.12,15 So far, the role of the FRAIL scale has not been evaluated for short-term prognosis in the group of patients undergoing heart valve surgery. Due to the need to supplement tools for accurate heart surgery risk assessment, in the presented study we assessed the suitability of the FRAIL scale for early postoperative mortality in a group of patients undergoing valve surgery.
Patients and Methods
This prospective study included consecutive patients with hemodynamically significant valvular heart disease (aortic stenosis, aortic regurgitation, mitral stenosis and mitral regurgitation) who underwent heart valve surgery (replacement or repair of the valve/valves, with or without additional procedures) at the Institute of Cardiology, Warsaw, between 2014–2019.
The exclusion criteria were: patient age under 18 years; autoimmune diseases, chronic inflammatory bowel, active neoplastic diseases and active endocarditis. The day before surgery, a blood sample for biomarkers was collected from each patient. Complete blood count was performed with K2-EDTA samples, using a Cobas 6000 electronic counter (Roche, Mannheim, Germany). The following data were collected age, gender, body mass index (BMI), comorbidities (atrial fibrillation, chronic obstructive airway disease, coronary artery disease, myocardial infarction, heart failure, current smoker, dyslipidaemia, hypertension, diabetes mellitus, peripheral atherosclerosis, stroke, osteoporosis, chronic kidney disease) the results of echocardiography findings and the assessment of the coronary arteries. The FRAIL scale was used to diagnose the frailty syndrome in every patient before valve surgery. The presence of 3 of the 5 components: fatigue, resistance, aerobics, illness or loss of weight indicated the presence of a frailty. Fatigue was measured by asking patients how much time during the past 1 month they felt tired with responses of “most of the time” or “all of the time” scored 1 point. Resistance was assessed by asking patients if they had any difficulty walking up 10 steps alone without resting and without aids. Ambulation by asking patients if they had any difficulty walking several hundreds of meters alone and without aids, “yes” responses were each scored as 1 point. Illness was scored 1 for patients who reported 5 or more concomitant illnesses. Loss of weight was scored 1 for respondents with a weight decline of 5 kg or greater within the past 12 months based on self-report.16 All procedures were performed through a midline sternotomy incision under general anaesthesia in a normothermia. During the operation, all patients were given cold blood cardioplegia at the initial dose of 15–20 mL/kg followed by booster doses of 5–10 mL/kg every 20 minutes. The primary end-point was death from all causes in 30-day follow-up. All patients were followed by direct observation during hospitalization, telephone interviews, or clinic visits for 30 days after the surgery. Before entering the study, each patient gave informed written consent to participate in the study. The protocol was approved by The Institutional Ethics Committee (Institute of Cardiology, Warsaw, Poland). The research was carried out in accordance with the Declaration of Helsinki.
Statistical Analysis
Data are presented as medians with ranges if continuous, or as frequencies if categorical. Spearman’s rank correlation coefficient was used to search for associations between the FRAIL scale and selected variables. Binary logistic regression was used to assess relationships between variables. The following covariates were investigated for association with the primary end-point in univariate analysis: age, atrial fibrillation, body mass index, chronic kidney disease, chronic obstructive airway disease, coronary artery disease, current smoker, dyslipidaemia, FRAIL scale result, hypertension, diabetes mellitus, left ventricular ejection fraction, peripheral atherosclerosis, previous myocardial infarction, stroke or TIA history, tricuspid annulus plane systolic excursion, mean corpuscular volume, platelets, red blood cell count (RBC), red cell distribution width (RDW), mean platelet volume, white blood cell count. Significant determinants (p < 0.05) identified from univariate analysis were subsequently entered into multivariate models. Receiver operating characteristic (ROC) curves were plotted for the EuroSCORE II alone, and for the combined model of EuroSCORE II and frailty syndrome for 30-day survival following valve surgery. The additional predictive value of frailty syndrome was assessed by a comparison of the areas under the ROC of the respective curves.
Results
The study included 672 patients (381 men, 291 women; mean age 64 ± 12.5 years) who underwent replacement or repair of valve/valves. In 313 patients, a biological valve prosthesis was implanted, and in 261, a mechanical valve. In 22 patients, the frailty syndrome was diagnosed. Baseline characteristics of the patients are presented in Table 1. Twenty-five patients died during the 30-day follow-up (as a result of gradually increasing multi-organ failure). The actual 30-day mortality was 3.7% vs mortality 3.5% predicted by the EuroSCORE II. Statistically significant predictors of primary end-point at univariate analysis are presented in Table 2. At multivariate analysis, FRAIL scale result (OR 2.802; 95% CI 1.275–6.157; p = 0.01) and RDW (OR 1.810; 95% CI 1.181–2.775; p = 0.006) were associated with the occurrence of death. The type of implanted valve did not affect the occurrence of the end point. Moreover, there was no significant difference in the occurrence of the endpoint in terms of gender. A positive correlation was found between the level of FRAIL scale and CRP (r = 0.4; p < 0.001), BMI (r = - 0.2; p < 0.01), RDW (r = 0.2; p < 0.001), creatinine (r = 0.1; p = 0.002), RBC (r = - 0.2; p < 0.001) and NT-proBNP (r = 0.2; p < 0.001). FRAIL scale in patients undergoing heart valve surgery when combined with EuroSCORE II predicted the 30-day mortality better (area under receiver operator characteristic curve [AUROC] = 0.870; 95% CI 0.828–0.920) compared to EuroSCORE II alone (AUROC = 0.805; 95% CI 0.757–0.853) (p = 0.001).
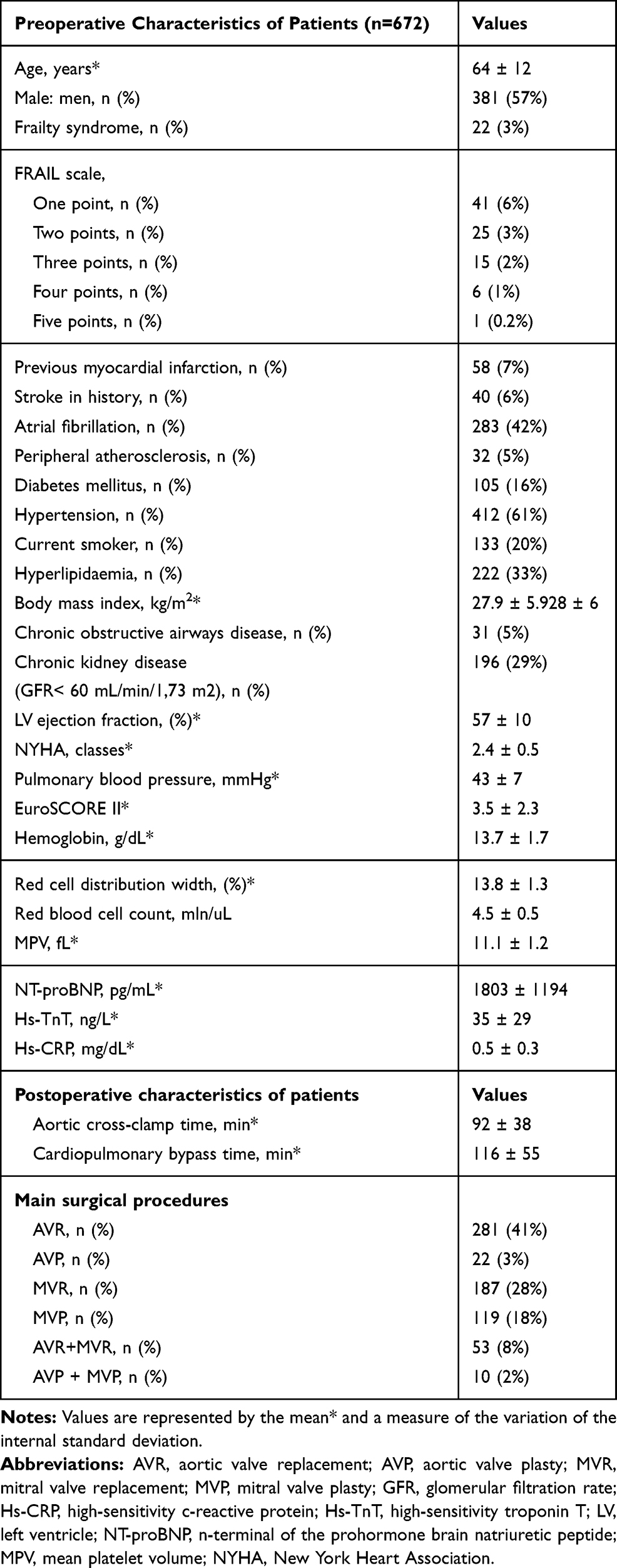 |
Table 1 Baseline Characteristics of the Study Population |
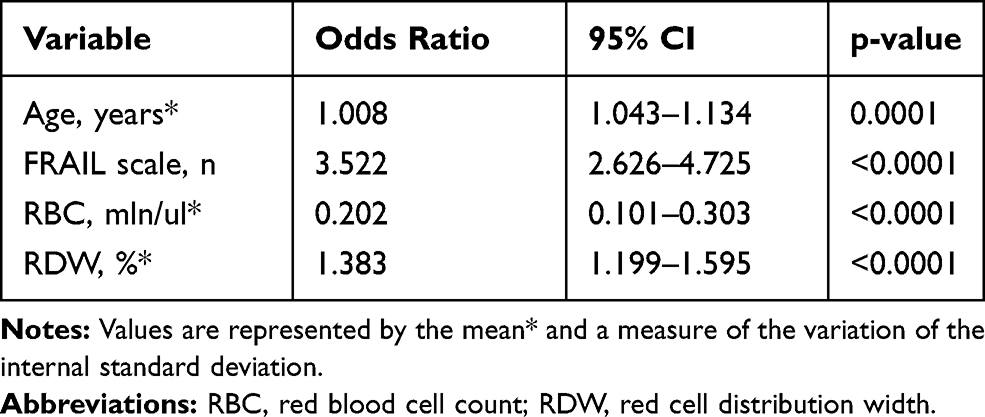 |
Table 2 Univariate Analysis of Predictive Factors for the Occurrence of Death |
The areas under ROC curves of EuroSCORE II and the combined model preoperative FRAIL scale + EuroSCORE II for 30-day survival are shown in Figure 1. The major complications after surgery occurred in 134 patients (postoperative renal failure in 39 patients, prolonged mechanical ventilation in 88 patients, stroke in 24 patients, hemodynamic instability in 126 patients, multi-organ failure in 67 patients. In 46 patients occurred more than one major complications).
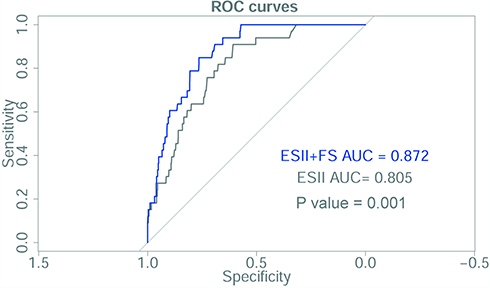 |
Figure 1 Areas under receiver operator characteristic (ROC) curves of EuroSCORE II (ES II) and combined model EuroSCORE II + FRAIL scale (ES II + FS) for 30-day survival following valve surgery. |
Discussion
The frailty syndrome is a serious health problem for an aging population. The FRAIL scale alongside Frailty index, Strawbridge questionnaire, FRAIL scale, Clinical Frailty Scale, Edmonton Frail Scale or Fried scale is one of the tools used to reliably assess the occurrence of the frailty syndrome.5,6 The name of this subjective, simple tool recommended by the International Association of Nutrition and Aging is an acronym formed from the first letters of the English names of its 5 components: fatigue, resistance, aerobic, the occurrence of illnesses (illness) and loss of weight.5,6,16 The occurrence of frailty in the group of symptomatic patients with valvular heart disease may have additional clinical implications.7,11 So far, it has been demonstrated so far that the frailty syndrome is an independent predictor of death mainly in the elderly patients with aortic stenosis undergoing interventional treatment as well as in the group of patients with mitral regurgitation treated percutaneously.7,11,17,20 Also described that frailty indices such as 5-m walk test, Elderly Mobility Scale and handgrip strength as well as normalized values of psoas muscle area (PSA) and psoas muscle volume (PSV) using computed tomography (CT) scans were characterized by strong prediction ability of occurrence death after transcatheter aortic valve implantation (TAVI) in long-term follow-up.21,22 However, there is no unambiguous information on the impact of the onset of the frailty syndrome in the early postoperative period in the general group of symptomatic patients undergoing heart valve surgery. Moreover, the usefulness of the FRAIL scale in the stratification of operational risk in this group of patients has not been described so far.
In the presented study it was shown that the FRAIL scale is an independent predictor of death in a 30-day observation in a group of patients undergoing heart valve surgery. In addition, the FRAIL scale added to the ES II calculation result significantly improves its predictive power. Available literature indicates significant limitations on both the EuroSCORE scale, the revised version – EuroSCORE II and the American STS due to insufficient calibration and discrimination of these calculators.12,15,23 So far, it has been shown that parameters such as RDW, RBC or troponin T can improve the predictive power of commonly known risk calculators.24,26
The presented study showed that the frailty syndrome diagnosed using the FRAIL scale indicating a reduced human physiological reserve may be one of the factors playing a decisive role in the qualification of patients with valvular heart disease for further treatment. Noteworthy is the significant correlation between the FRAIL score and the hs-CRP inflammation parameter, which may confirm that one of the causes of frailty syndrome is a chronic inflammatory process.
In the presented study, also the RDW parameter (described in the literature as an indicator of human physiological reserve) was also an independent predictor of death during the 30-day observation period, and was also significantly correlated with the FRAIL score.27 The presented work touches on the subject of preoperative exponents of human physiological reserve, which are undoubtedly very important in stressful situations, such as cardiac surgery. Elevated values of the FRAIL scale or the RDW parameter reflecting the reduced physiological reserve may explain the more frequent occurrence of deaths in the early postoperative period. This study has some potential limitations. This is a single-center study with a limited number of patients, short follow-up period and a wide age range of patients studied. In future studies, enlarging the group may allow to confirm the obtained results. Further studies are needed regarding the usefulness of an indicator of a patient’s physiologic reserve.
Summary
The results of the present study showed FRAIL scale to be a useful parameter for estimating risk in patients undergoing heart valve surgery. Moreover, the predictive ability of the FRAIL scale, assessed by the area under the ROC curve, may also improve the predictive ability of the EuroSCORE II calculator. The results of our research may be helpful in the perioperative strategy in patients with valvular heart disease.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ferruci L, Guralnik JM, Studenski S, et al. Designing randomized aimed at preventing or delaying functional decline and disability in frail, older persons: a consensus report. J Am Geriatr Soc. 2004;52(4):625–634. doi:10.1111/j.1532-5415.2004.52174.x
2. Campbell AJ, Buckner DM. Unstable disability and the fluctuations of frailty. Age Ageing. 1997;26(4):315–318. doi:10.1093/ageing/26.4.315
3. Rockwood K. What would make a definition of frailty successful? Age Ageing. 2005;34(5):432–434. doi:10.1093/ageing/afi146
4. Bilotta C, Nicolini P, Casè A, et al. Frailty syndrome diagnosed according to the Study of Osteoporotic Fractures (SOF) criteria and adverse health outcomes among community-dwelling older outpatients in Italy. A one-year prospective cohort study. Arch Gerontol Geriatr. 2012;54(2):23–28. doi:10.1016/j.archger.2011.06.037
5. Życzkowska J, Grądalski T. Frailty - an overview for oncologists. Oncol Clin Pract. 2010;6(2):79–84.
6. Uchmanowicz I, Lisiak M, Jankowska-Polańska B. Research instruments used in the assessment of the frailty syndrome. Gerontol Pol. 2014;22(1):1–8.
7. Duchnowski P, Hryniewiecki T, Kuśmierczyk M, Szymański P. The usefulness of selected biomarkers in patients with valve disease. Biomark Med. 2018;12(12):1341–1346. doi:10.2217/bmm-2018-0101
8. Shibata K, Yamamoto M, Kano S, et al. Importance of geriatric nutritional risk index assessment in patients undergoing transcatheter aortic valve replacement. Am Heart J. 2018;202:68–75. doi:10.1016/j.ahj.2018.04.021
9. Goldfarb M, Lauck S, Webb JG, et al. Malnutrition and mortality in frail and non-frail older adults undergoing aortic valve replacement. Circulation. 2018;138(20):2202–2211. doi:10.1161/CIRCULATIONAHA.118.033887
10. Hawkins RB, Mehaffey JH, Charles EJ, et al. Psoas muscle size predicts risk-adjusted outcomes after surgical aortic valve replacement. Ann Thorac Surg. 2018;106(1):39–45. doi:10.1016/j.athoracsur.2018.02.010
11. Anand A, Harley C, Visvanathan A, et al. The relationship between preoperative frailty and outcomes following transcatheter aortic valve implantation: a systematic review and meta-analysis. Eur Heart J Qual Care Clin Outcomes. 2017;3(2):123–132. doi:10.1093/ehjqcco/qcw030
12. Kuwaki K, Inaba H, Yamamoto T, Matsumura T, Morita T, Amano A. Performance of the EuroSCORE II and the society of thoracic surgeons score in patients undergoing aortic valve replacement for aortic stenosis. J Cardiovasc Surg (Torino). 2015;56(3):455–462.
13. Parolari A, Pesce L, Trezzi M, Cavallotti L, Kassem S, Loardi C. EuroSCORE performance in valve surgery: a meta-analysis. Ann Thorac Surg. 2010;89(3):787–793. doi:10.1016/j.athoracsur.2009.11.032
14. Borracci ICA, Allende NG, Ahuad Guerrero RA, Ingino CA, Allende NG, Ahuad Guerrero RA. Prospective validation of EuroSCORE II in patients undergoing cardiac surgery in Argentinean centres. Interact Cardiovasc Thorac Surg. 2014;18(5):539–543. doi:10.1093/icvts/ivt550
15. Duchnowski P, Hryniewiecki T, Kuśmierczyk M, Szymański P. Performance of the EuroSCORE II and the society of thoracic surgeons score in patients undergoing aortic valve replacement for aortic stenosis. J Thorac Dis. 2019;11(5):2076–2081. doi:10.21037/jtd.2019.04.48
16. Morley JE, Malmstrom TK, Miller DK. A simple frailty questionnaire (FRAIL) predicts outcomes in middle aged African Americans. J Nutr Health Aging. 2012;16(7):601–608. doi:10.1007/s12603-012-0084-2
17. Søndergaard L, Kirk BH, Jørgensen TH. Frailty: an important measure in patients considered for transcatheter aortic valve replacement. JACC Cardiovasc Interv. 2018;11(4):404–406. doi:10.1016/j.jcin.2017.12.017
18. Saji M, Higuchi R, Tobaru T, et al. Impact of frailty markers for unplanned hospital readmission following transcatheter aortic valve implantation. Circ J. 2018;82(8):2191–2198. doi:10.1253/circj.CJ-17-0816
19. de Thézy A, Lafargue A, d’Arailh L, et al. Relevance of G8 scale in referring elderly patients with aortic stenosis requiring a TAVI for a geriatric consultation. Geriatr Psychol Neuropsychiatr Vieil. 2017;15(4):357–363. doi:10.1684/pnv.2017.0697
20. Metze C, Matzik AS, Scherner M, et al. Impact of frailty on outcomes in patients undergoing percutaneous mitral valve repair. JACC Cardiovasc Interv. 2017;10(19):1920–1929. doi:10.1016/j
21. Kleczynski P, Tokarek T, Dziewierz A, et al. Usefulness of psoas muscle area and volume and frailty scoring to predict outcomes after transcatheter aortic valve implantation. Am J Cardiol. 2018;122(1):135–140. doi:10.1016/j.amjcard.2018.03.020
22. Kleczynski P, Dziewierz A, Bagienski M, et al. Impact of frailty on mortality after transcatheter aortic valve implantation. Am Heart J. 2017;185:52–58. doi:10.1016/j.ahj.2016.12.005
23. Duchnowski P, Hryniewiecki T, Kuśmierczyk M, Szymański P. The usefulness of selected biomarkers in aortic regurgitation. Cardiol J. 2019;26(5):477–48221. doi:10.5603/CJ.a2018.0108
24. Duchnowski P, Hryniewiecki T, Kuśmierczyk M, Szymanski P. Red cell distribution width as a predictor multiple organ dysfunction syndrome in patients undergoing heart valve surgery. Biol Open. 2018;7(10):bio036251. doi:10.1242/bio.036251
25. Petaja L, Rosio H, Mildh L, et al. Predictive value of high sensitivity troponin T in addition to EuroSCORE II in cardiac surgery. Interact Cardiovasc Thorac Surg. 2016;23(1):133141. doi:10.1093/icvts/ivw060
26. Duchnowski P, Hryniewiecki T, Stokłosa P, Kuśmierczyk M, Szymański P. Number of erythrocytes as a prognostic marker in patients undergoing heart valve surgery. Kardiol Pol. 2018;76(4):791–793. doi:10.5603/KP.2018.0076
27. Bion JF. Susceptibility to critical illness: reserve, response and therapy. Intensive Care Med. 2000;26(S1):57–63. doi:10.1007/s001340051120
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.