")
Back to Journals » Clinical Interventions in Aging » Volume 14
The Effectiveness Of Radial Extracorporeal Shock Wave Therapy In Patients With Chronic Low Back Pain: A Prospective, Randomized, Single-Blinded Pilot Study
Authors Walewicz K , Taradaj J , Rajfur K , Ptaszkowski K , Kuszewski MT, Sopel M , Dymarek R
Received 21 July 2019
Accepted for publication 26 September 2019
Published 30 October 2019 Volume 2019:14 Pages 1859—1869
DOI https://doi.org/10.2147/CIA.S224001
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Richard Walker

Karolina Walewicz,1 Jakub Taradaj,2,3 Katarzyna Rajfur,1 Kuba Ptaszkowski,4 Michał Tomasz Kuszewski,2 Mirosław Sopel,5 Robert Dymarek5
1Faculty of Physiotherapy, Opole Medical School, Opole, Poland; 2Institute of Physiotherapy and Health Sciences, Academy of Physical Education, Katowice, Poland; 3College of Rehabilitation Sciences, University of Manitoba, Winnipeg, MB, Canada; 4Department of Physiotherapy, Wroclaw Medical University, Wroclaw, Poland; 5Department of Nervous System Diseases, Wroclaw Medical University, Wroclaw, Poland
Correspondence: Robert Dymarek
Department of Nervous System Diseases, Faculty of Health Sciences, Wroclaw Medical University, Bartla 5, Wroclaw 51-618, Poland
Tel +48 71 784 18 05
Fax +48 71 341 95 33
Email [email protected]
Purpose: This prospective, randomized and single-blinded study assesses the influence of radial extracorporeal shock wave therapy (rESWT) in patients with low back pain (LBP).
Methods: A total of 52 patients with LBP were enrolled in the study, out of which a homogeneous group of 40 patients with mean age of 53.45±4.9 years was included. Patients were randomized into group A (n=20) treated with rESWT (2000 pulses; 2.5 bars; 5 Hz, 7 mins) performed twice a week for five weeks (10 sessions) and stabilization training, as well as group B (n=20) treated with sham rESWT and stabilization training. To analyze the therapeutic progress, the following tests were performed (before and after therapy; 1 and 3 months follow-up) to assess pain and functional efficiency: (1) Visual Analog Scale (VAS), (2) Laitinen Pain Scale (LPS), and (3) Oswestry Disability Index (ODI).
Results: The control group had a statistically significant advantage over the rESWT group (4.4 vs. 3.1 points on the VAS; p=0.039). However, in long-term observations, group A gradually experienced more pain relief than group B (2.7 vs. 3.5 points, p>0.05, at one month and 2.0 vs. 4.4 points at three months after treatment; p<0.0001). Similar findings can be seen in the analysis of changes in pain sensations measured with the LPS. The functional state (ODI) was better in rESWT group, especially in follow-up observation (9.3 vs. 14.6 points, p=0.033, at one month and 9.3 vs. 17.8 points, p=0.004, at three months after treatment).
Conclusion: The rESWT combined with stabilization training is particularly effective in the long-term and achieves a stable beneficial effect for patients with LBP. The use of rESWT has a significant long-term influence on the reduction of pain and the improvement of the general functional state in relation to the conventional motor improvement program.
Keywords: shock waves, ESWT, low back pain, functional state, physical therapy
Introduction
Low back pain (LBP) is fundamentally a medical problem, but also a sociological and an economic one. At present, pain in the lumbar and sacral segments of the spine, due to its universality, is considered a disease of civilization, which, in addition to the suffering of patients, causes significant limitations in the professional and social spheres. The symptoms lead to a decrease in the quality of life for patients and sometimes disturb the proper functioning of the entire body, stimulating the development of several complications and comorbidities.1,2
The basic approach of choice for LBP therapy is still conservative management, which includes mainly pharmacotherapy,3–5 physical exercises and manual methods,6–8 and physiotherapeutic procedures;9,10 more recently, modern extracorporeal shock wave therapy (ESWT) have been also used.
In biophysical terms, ESWT is defined as a sequence of high energy mechanical (acoustic) impulses of alternating course, producing short-lived and turbulent pressure changes in a center (alternating compression and decompression phases), in which the phenomenon of wave propagation in space takes place.11 In principle, there are two types of shock waves that differ in the form and extent of the propagation of acoustic energy, the shape of the beam, and their physical properties.
Focused ESWT (fESWT) was initially only used as a lithotripsy device in interventional urology or abdominal surgery, as a non-invasive procedure for urinary or biliary stone crushing. Devices emitting this type of wave are most often based on electromagnetic, electrohydraulic, or piezoelectric methods. Typical physical parameters start with the pressure, which increases rapidly over less than 10 ns and reaches 100–1000 bar (10–100 MPa), so that it is absorbed in soft tissues theoretically to a depth of up to 12 cm. The focal wave beam is characterized by a concentrated propagation shape—the so-called focal point (the place with the highest energy density in a relatively small area, located at a depth of 4–6 cm). In contrast, radial ESWT (rESWT) is generated by the pneumatic (ballistic) method using a device that produces compressed air, which sets in motion a special bullet placed inside the applicator. This bullet, after accelerating, hits the head, which causes the transformation of kinetic energy into the phenomenon of the shock wave, which then propagates into the tissue. This wave is characterized by a slow-growing pressure that takes up to 5 µs to reach 1–10 bar (0.1–1.0 MPa) and is absorbed at a depth of up to 3 cm, with a typically dispersed (unfocused) beam shape.12
To explore the phenomena of ESWT in biological tissues, many studies attempted to elucidate the mechanism of shock waves from the basic science study and translate into clinical application. For example, Wang et al13 in animal study reported that application of ESWT caused the ingrowth of neovascularization associated with up-regulation of angiogenic and osteogenic growth factors including endothelial nitric oxide synthase (eNOS), vessel endothelial growth factor (VEGF), proliferating cell nuclear antigen (PCNA), and bone morphogenic protein-2 (BMP-2) at the tendon–bone junction of the Achilles tendon in rabbits.
In a study by Yin et al14 bone marrow stromal cells (BMSCs) were harvested from the bone marrow cavity of the proximal femur in six patients with osteonecrosis. There were significant increases in cell proliferation, VEGF, alkaline phosphatase, BMP-2, runt-related transcription factor 2 (RUNX2) and osteoclast in mRNA expressions in the shockwave group. These results demonstrated that ESWT significantly enhances the angiogenic and osteogenic effects.
The chondroprotective effect was studied too. Researchers from Taiwan15 observed site-specific phenomena in the initiation of osteoarthritis (OA) changes of the knee in rats. There were significant increases of VEGF, BMP-2, and osteocalcin in the subchondral bone as compared to the control at week 2, 4, 8, and 12. The most beneficial effects of ESWT in the OA knee occurred at 4 weeks after shockwave application. Such effects seemed to continue until 12 weeks.
Santamato et al16 in a clinical study with twelve patients after Achilles tendinopathy noticed the mechanisms such as direct stimulation of healing, neovascularization and direct suppressive effects on nociceptors and hyperstimulation, which would block the gate-control system. The neovascularization observed in phlogistic tissue was associated with stimulated nerve fibers around tendons.
The analysis of the available literature on the use of ESWT in LBP shows that, despite its high popularity and novelty, there have been only a small number of randomized clinical trials, especially for rESWT (Table 1).17–20 Moreover, a significant number of these studies do not meet the highest criteria of Evidence-Based Physiotherapy, which ultimately makes it extremely difficult to unequivocally and objectively analyze the clinical effectiveness of the procedures that are widely used in everyday practice. This study, therefore, aimed to assess the influence of rESWT in the treatment of patients with LBP.
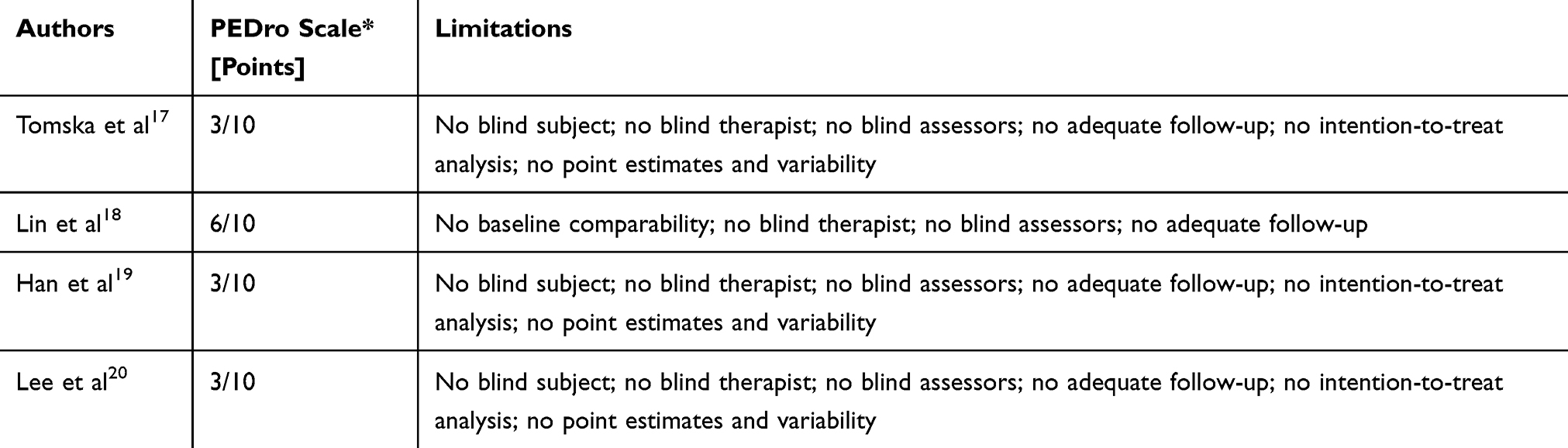 |
Table 1 Quality Of Clinical Studies On rESWT And LBP |
Methods
Ethics, Design, And Setting
The research was conducted from April 2018 to November 2018 at the Clinical Research Laboratory in the Physiotherapy Department of the Opole Medical School, Poland. The study was approved by the independent Bioethics Committee of the Wroclaw Medical University, Poland (approval no. KB–75/2017). All participants gave written informed consent after a thorough explanation of both the procedures involved and that their anonymity would be preserved. The study was carried out in accordance with the guidelines of the Declaration of Helsinki and Good Clinical Practice. The research project was prospectively registered as a randomized clinical trial in the Australian New Zealand Clinical Trial Registry supervised by the World Health Organization (registration no. ACTRN12618000593235).
Study Participants
A total of 52 patients with LBP were enrolled in the study, out of which a homogeneous group of 40 patients with mean age of 53.45±4.9 years was included. Patients were randomized into two comparative groups: A (n=20) with mean age of 51.1±8.4 years, and B (n=20) with mean age of 55.8±9.3 years. Patients from the comparative groups were homogeneous in terms of the basic characteristics of the studied population (Table 2) and in terms of baseline measurements of pain and functional status. The detailed CONSORT flow chart of participants in each stage of the project is presented in Figure 1.
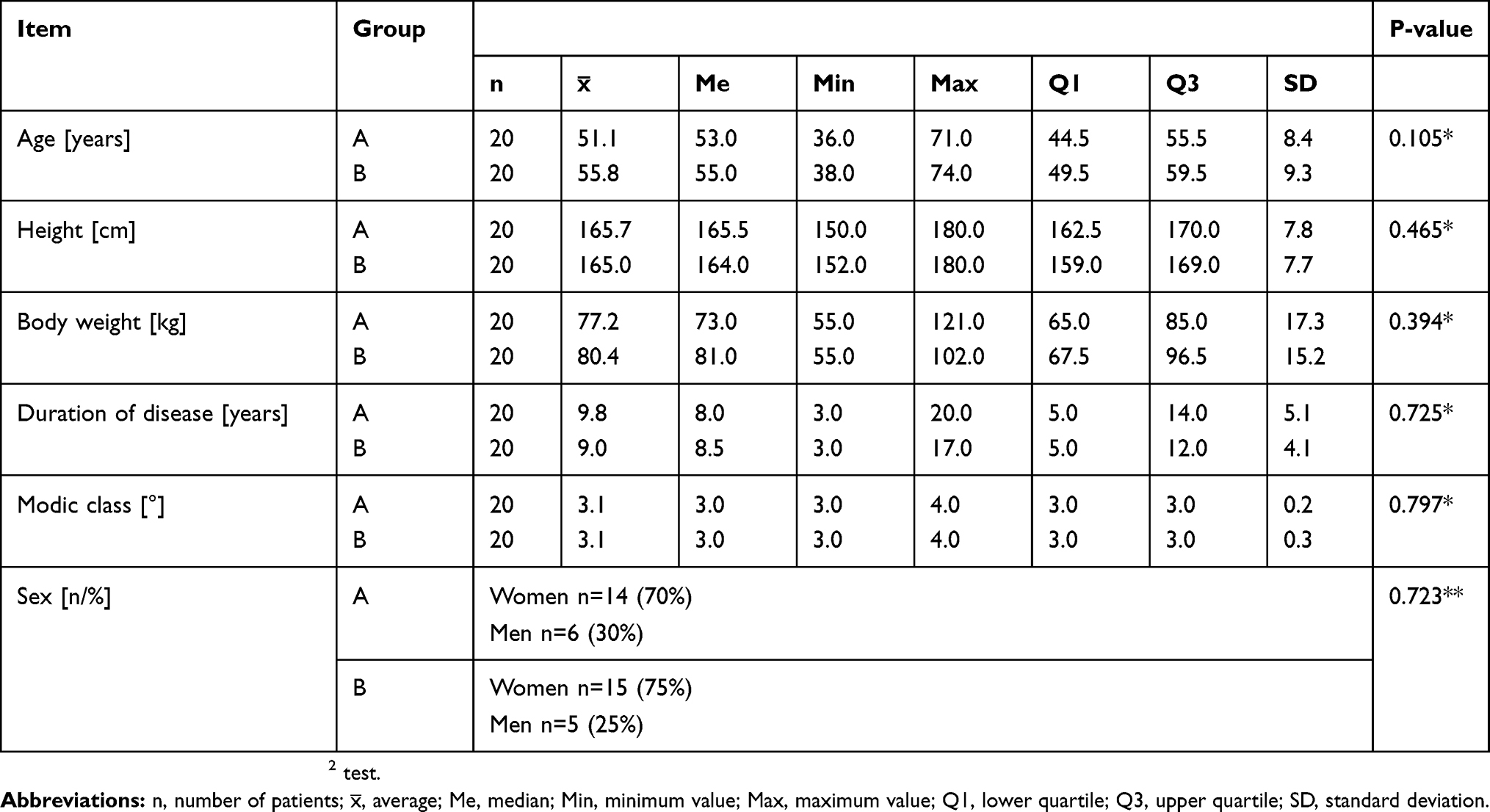 |
Table 2 Demographic Characteristics Of Participants In The Study |
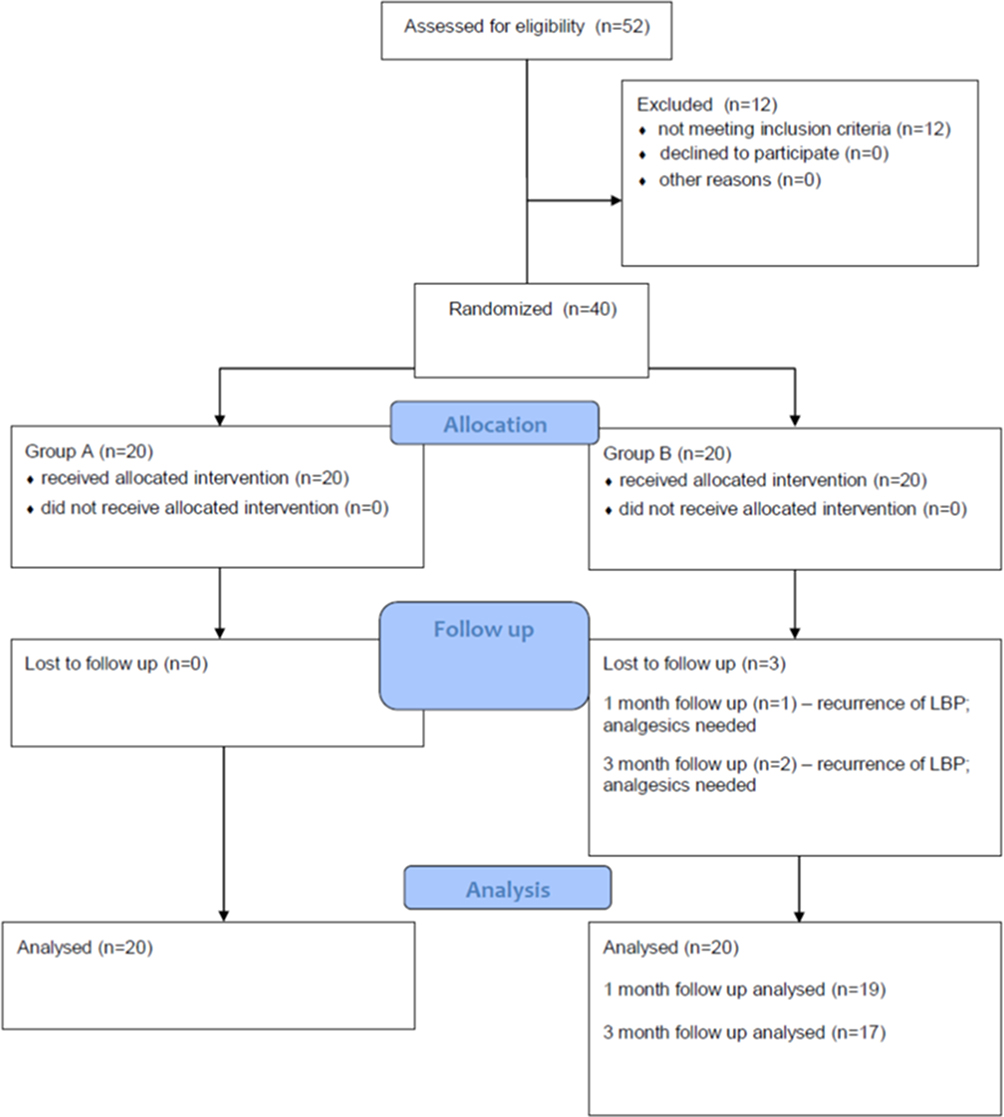 |
Figure 1 The CONSORT flow chart diagram. |
Qualification And Randomization
Recruitment was conducted among patients with LBP. Patients were qualified by a team consisting of an orthopedist, a neurologist, a neurosurgeon, an internist, a radiologist, and a physiotherapist. The selection of patients for participation in the research was purposeful. Patients with discopathy of the L5-S1 spine segment, chronic pain lasting more than three months, and pseudo-radicular pain syndrome, who had not been treated with spine surgery before, were qualified for the study. Patients had to be at least 18 years old and have a current magnetic resonance imaging (MRI) examination confirming the diagnosis (at least III° according to the Modic classification, in the L5-S1 segment of the spine). The allocation to the groups of patients who passed the qualification procedure was random. Participants were randomized with equal probability to ESWT or sham using a central computer-generated random allocation by a senior researcher. The group allocation was independent of the persons delivering the treatment and analyzing the results/data.
Inclusion And Exclusion Criteria
Patients with discopathy of the L5-S1 spine segment with chronic pain lasting more than three months were included in the study. The exclusion criteria applied to the patients were acute spinal pains (occurring for less than three months, because ailments of longer duration were treated as chronic); radicular pain syndrome; discopathy on a different level of the spine (patients with early lesions I° and II° according to Modic classification were not excluded from the study, only degeneration III° was a basis for exclusion); lack of pain and reduced mobility in the lumbar and sacral regions; other diseases within the spine (spondylolisthesis, fractures, tumors, rheumatic diseases, cauda equina syndrome); pregnancy; pacemaker; neurological deficit symptoms; cardiovascular diseases; blood coagulation disorders; metal implants, such as hip and/or knee endoprosthesis; mental disorders; cancer; psoriasis; scleroderma; and viral and bacterial infections. Patients undergoing spinal surgery or receiving analgesics or anti-inflammatory drugs were also excluded from the study.
Patients not qualified for the next stages of the scientific project for various reasons were provided with basic treatment—administration of analgesics and non-steroidal anti-inflammatory drugs—as well as elements of movement improvement according to medical indications. Participants were assigned computer-generated random numbers and assigned to a comparative group based on a draw of those numbers.
Procedures And Measurements
Patients from group A were treated with rESWT using a Pro-Shock Waves pneumatic device (Cosmogamma, Indonesia; see Figure 2). Each treatment was performed using a contact method, with the labile movement of the applicator (head) in the spinal region at the level of the lumbar and sacral spine in the area of the most severe painful ailments reported by the patient (Figure 3). The following treatment parameters were used: 2000 pulses with the pressure of 2.5 bars (corresponding to an energy flux density of 0.1 mJ/mm2), 5 Hz frequency, and treatment time of seven minutes. A standard ultrasound gel was used to connect the applicator head to the skin, reduce tissue resistance, and maintain proper coupling and energy propagation. The procedures were performed twice a week (Monday and Thursday) for a period of five weeks (i.e., each patient underwent a series of ten procedures).
 |
Figure 2 The rESWT device used in the study. |
 |
Figure 3 The rESWT procedure in LPB. |
Patients from group B were treated with sham rESWT. The sham stimulation was voided of biologically active components by applying a special polyethylene applicator cap, which absorbed energy and limited its propagation to the patient’s tissue. The treatment technique was identical to that of group A, with the same sound signals during the procedure of the pneumatic head and the same technical parameters as in the real procedures. This group was a single-blind (patients did not know to which group they belonged) to estimate the placebo effect of this type of therapy.
In addition to physical treatment, patients from both groups underwent identical basic treatment by means of physical improvement in the form of functional training (45 mins, once a day, five days a week). Standard stabilization training included the following elements: techniques for relaxing the musculofascial system on the erector spinae muscle, techniques for activating the neutral position of the lumbo-pelvic-hip complex and deep muscles, activation of proper breathing, transverse abdominal muscle work, coordination of superficial and deep muscles, and postural and dynamic training.
Outcome Evaluation
To analyze the therapeutic progress, the following tests were performed to subjectively assess pain and functional efficiency: (1) Visual Analog Scale (VAS), (2) Laitinen Pain Scale (LPS), and (3) Oswestry Disability Index (ODI).
These tests were performed before the start and after the end of the full cycle of ESWT treatment. In the second stage of the project, the measurements were repeated as a follow-up at one and three months after the end of the study. During this period, patients were not subjected to any treatment aimed at reducing possible LBP.
All tests were performed by the same technician in the same laboratory. Physical treatments and stabilization training were carried out by the same therapist. Persons performing statistical analysis of the results received data in the form of coded numbers and had no knowledge about the state of health of the patients or their group assignment.
Statistical Analysis
The statistical analysis was performed using Statistica 13 (TIBCO Software Inc., USA) and STATA 15 (StataCorp LLC, USA). Arithmetic means, medians, lower and upper quartiles, standard deviations, and ranges of variability (extreme values) were calculated for measurable variables. Frequencies of occurrence (percentages) were calculated for qualitative variables. All quantitative variables were tested using the Shapiro–Wilk test to determine the distribution type. Due to the lack of a normal distribution and the low sample size, the analyses were performed using non-parametric tests. The Mann–Whitney U and chi-squared tests were used to test the homogeneity of the groups. The comparison of the results between the groups was performed using the Mann–Whitney U-test. In each group, the comparison of the results obtained before and after the intervention, and at one and three months follow-up, was carried out using Friedman test for non-parametric repeated-measures analysis of variance. A significance level of α=0.05 was used for all comparisons.
In calculating our sample size, we allowed for (1) 20% loss to follow-up and (2) historical information from our unit that 45% of patients who are offered conservative (standard physical therapy) management for this condition opt for ESWT within six months. The sample size analysis was performed using Statistica 13 (TIBCO Software Inc., USA). All calculations were carried out before the prospective study began. Based on the available results in the unit’s database, it was assessed how pain varied between two groups three months after rESWT treatment. The means and standard deviations of VAS (the primary outcome) results in both groups three months after treatment of rESWT were used in the analysis of estimating the sample size. The estimated sample size for a two-sample unpaired-means test (unpaired t-test). Parameters: mean in rESWT group was 2.1 (SD=1.1); mean in sham rESWT group was 4.6 (SD=1.4); the alpha level was set at 0.05, and the power of the test at 0.9. It also assumed no correlation of evaluated variables and adopted 2-sided null hypothesis. On the basis of the parameters, the estimated sample size has been obtained equal to 8 people in each group. In addition, the risk of losing patients in the follow-up assessment (20%) was assumed. The final sample size equals 10 participants in each group.
Results
After the end of the study, an extremely strong analgesic effect (p<0.0001) was observed in the group treated with rESWT and stabilization training. Interestingly, the pain reduction was not effective (p=0.957) immediately after treatment (pain reduction in VAS scale from 4.7 to 4.4 points, on average), but the therapeutic progress accelerated significantly in later observations (2.7 points, on average, at one month and 2.0 points at three months after treatment). This means that rESWT was particularly effective in the long term and achieved a stable analgesic effect without sudden relapse (p=0.021 for results immediately after treatment in relation to one month of follow-up and p=0.001 compared to three months without follow-up). Detailed results are shown in Table 3.
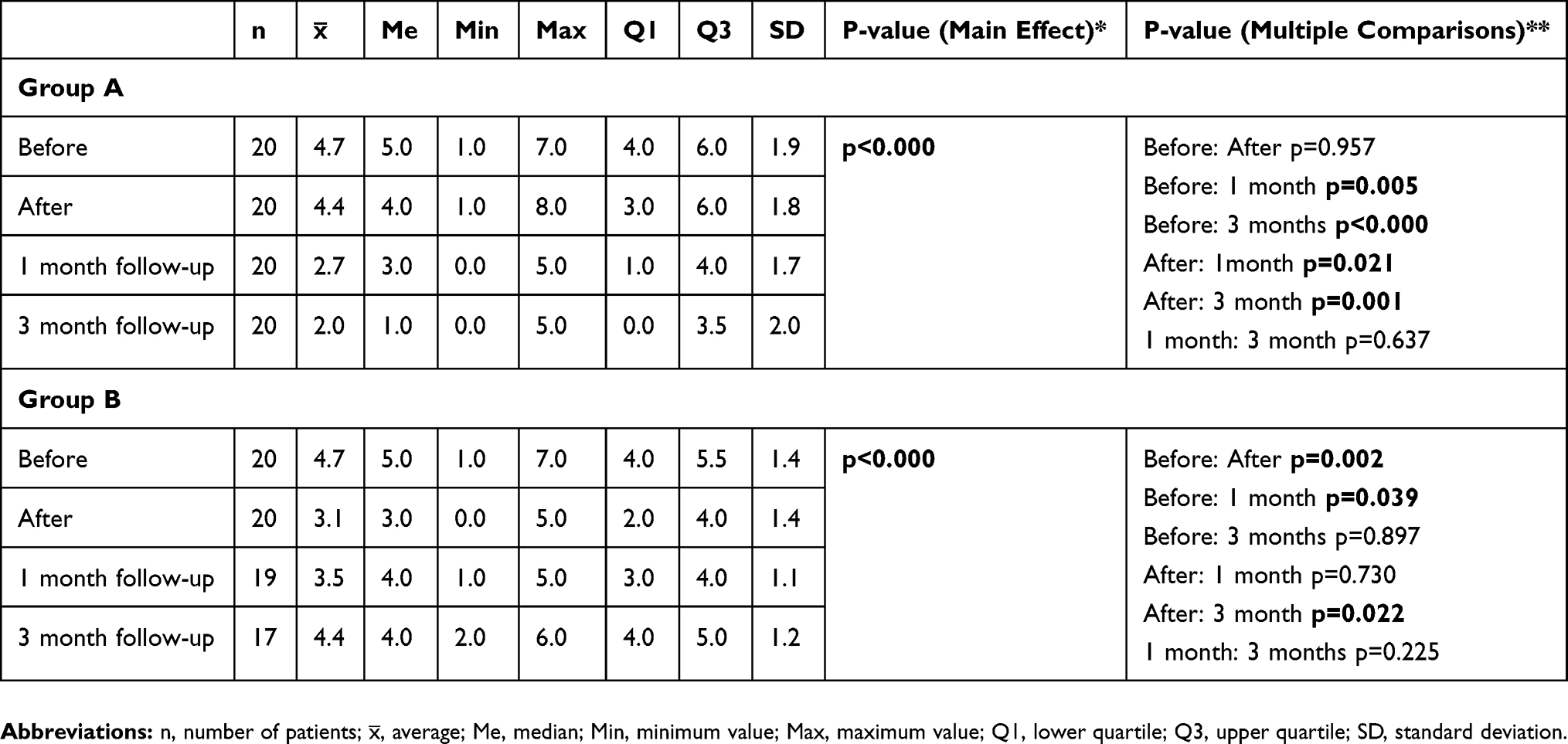 |
Table 3 The VAS Scale Results In Both Groups A And B [points] |
In group B, the analgesic effect was also effective (p<0.0001), as shown in Table 4. In patients receiving only sham rESWT treatment in addition to movement improvement, a rapid and statistically significant pain reduction was observed, from 4.7 points on the VAS scale before treatment to 3.1 points after (p=0.002). Unfortunately, in later observations, a gradual recurrence of pain and worsening of results was observed (on average, 3.5 at one month and 4.4 points at three months after the end of therapy). It was clear that, initially, the beneficial effects of the therapy were only of a short-term nature.
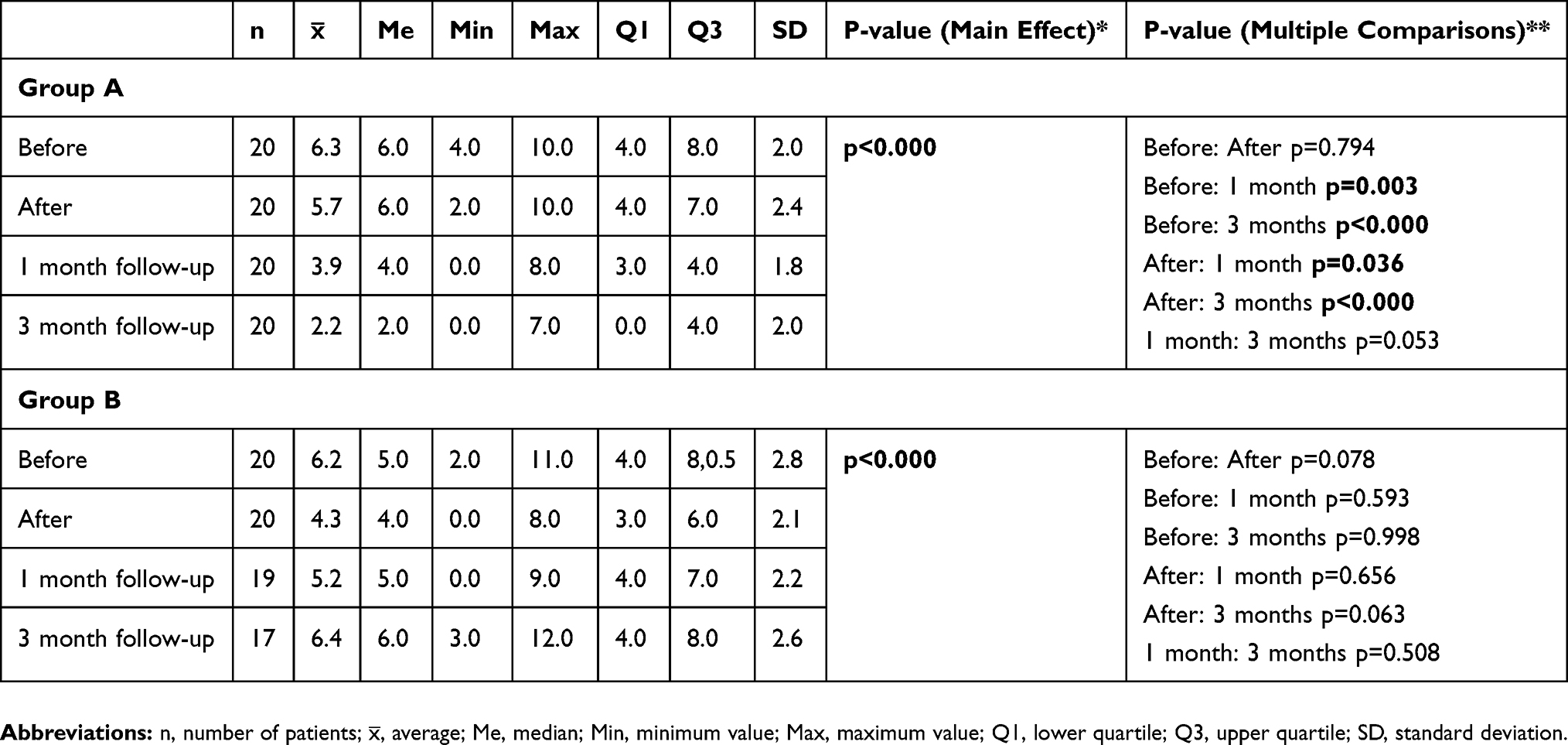 |
Table 4 The LPS Results In Both Groups A And B [points] |
The situation was very similar for the assessment of pain with the LPS (Table 4), for which rehabilitation was effective in both groups (p<0.0001). However, in the shock wave group, the therapeutic effect was initially relatively small (p=0.794), but, as before, it accelerated significantly in later observations (p=0.036 at one month and p<0.0001 at three months after the end of the therapy program), indicating that this physical treatment counteracted the potential recurrence of pain symptoms. In contrast, in the sham rESWT group, although the general effect was statistically significant, no significance was found in the post hoc analyses (p>0.05). As before, we could observe a deterioration of the results in long-term observations.
Functional efficacy in the stabilization and rESWT group initially improved slightly, from an average of 16.1 points before the start of the study to 13.6 points immediately after the therapy. However, it is worth noting that, one month after the end of treatment, the ODI score was already 9.3 and remained so for up to three months. The analysis of variance indicated that these changes were statistically significant (p<0.0001), as did post hoc comparisons (Table 5). In the control group, however, a change in ODI scores was noted, from 16.1 to 12.3, on average, after the end of treatment. Although the analysis of variance showed statistically significant positive changes (p=0.002), in the long-term evaluation, a gradual deterioration of patients’ fitness was unfortunately observed (14.6 at one month and 17.8 points at three months). The exact results with post hoc analyses are presented in Table 5.
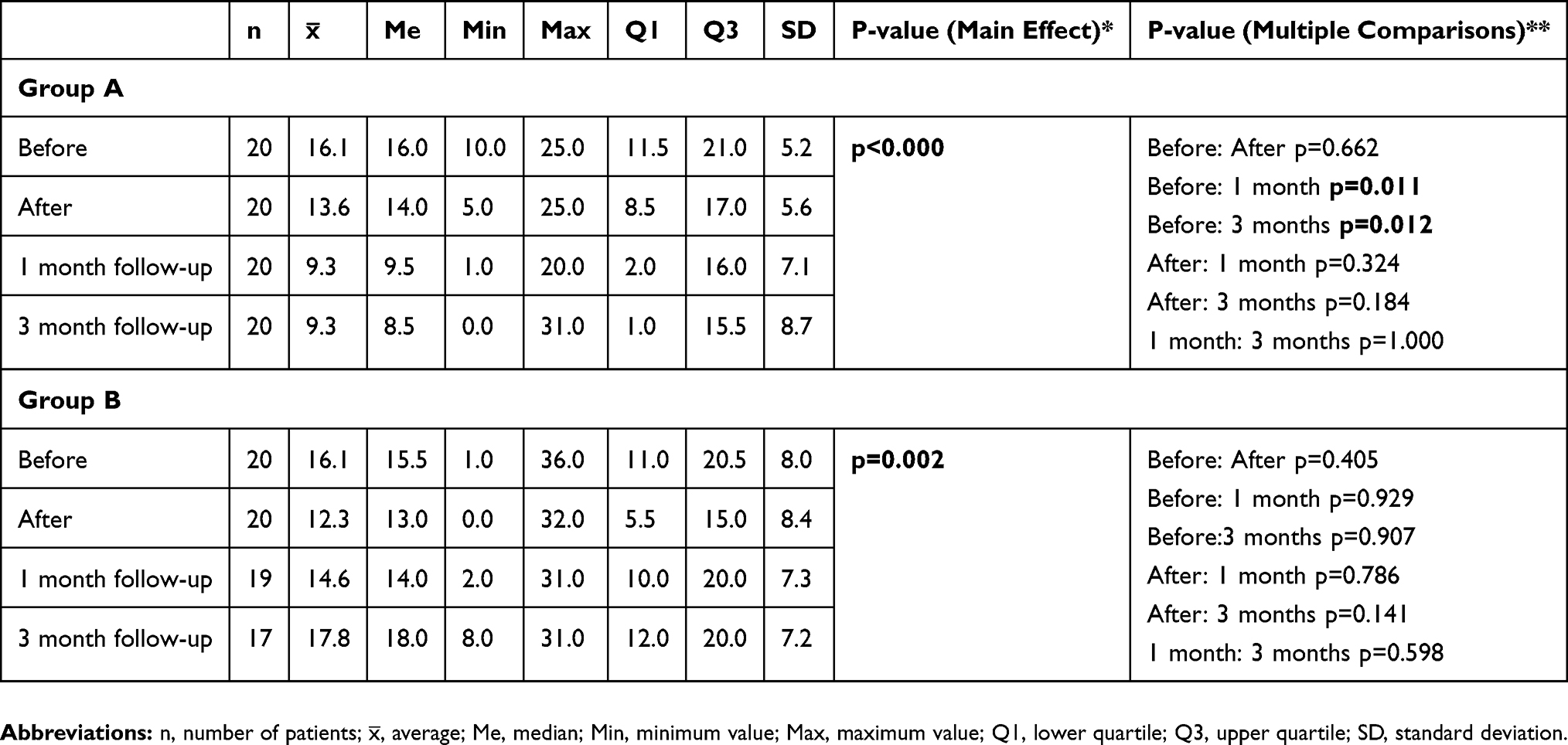 |
Table 5 The ODI Results In Both Groups A And B [points] |
No significant differences (p>0.05) were found before the study, which means that patients from the comparison groups were homogeneous in this range. Interestingly, the control group had a statistically significant advantage over the shock wave group (4.4 vs. 3.1 points on the VAS; p=0.039). However, in long-term observations, group A gradually experienced more pain relief than group B (2.7 vs. 3.5 points, p>0.05, at one month after treatment and 2.0 vs. 4.4 points, p<0.0001, at three months after treatment). This may mean that rESWT, as a relatively invasive physical treatment, does not show significant pain relief effects immediately after the end of the treatment period, however, it allows for longer remission of symptoms later, which is not possible for the standard movement improvement.
Similar findings can be seen in the analysis of changes in pain sensations measured with the LPS. Initially, the comparative groups were homogeneous (p>0.05). After treatment, although the pain was greater in group A, there was no difference from group B (5.7 vs. 4.3 points, p>0.05). Again, interestingly enough, the situation completely changes in the analysis of later results. Patients with active rESWT treatments, compared with the group with passive sham-rESWT treatments, saw a significant analgesic effect (p=0.043 at one month and p<0.0001 at three months after the end of therapy). The decreasing significance level over time clearly illustrates that rESWT allowed for a stable analgesic effect, while, in the control group, a gradual relapse and deterioration of results was observed. The increasing statistical difference between the two groups demonstrates this claim.
For functional status evaluation with the ODI, the groups were also homogeneous at the pre-start stage (p>0.05). After treatment, it is clear that the group treatments were effective at similar levels (p>0.05), although, as time passed after the end of the therapy program, rESWT started to gain a significant advantage over the sham therapy (9.3 vs. 14.6 points, p=0.033, at one month and 9.3 vs. 17.8 points, p=0.004, at three months after cessation of active treatment).
Discussion
There are few studies in the available literature (Web of Science, Scopus, Pubmed, Medline, PEDro) on the use of shock waves in the treatment of LBP, and most such publications examine the fESWT type.
Lee et al20 recruited 28 patients with LBP, who were assigned to one of two groups. The ESWT group consisted of 13 patients (age 53.92 years, height 163.15 cm, body weight 64.54 kg), and the control group consisted of 15 participants (age 54.33 years, body height 160.27 cm, body weight 60.20 kg). All patients, regardless of group, underwent a movement recovery program (30 mins, twice a week, for 1.5 months). The rehabilitation consisted of McKenzie exercises and central stabilization training. Additionally, in the ESWT group, a single application was performed (2000 pulses, frequency 5 Hz, dose 0.1 mJ/mm2). In the control group, thermotherapy using local warm gel wraps, ultrasound therapy, and transcutaneous electrical nerve stimulation (TENS) were performed daily. After the end of the study, it was found that pain measured by VAS significantly decreased in both groups, but much more so under the influence of shock waves (p<0.05).
Notarnicola et al21 conducted a randomized clinical trial in which 30 patients with LBP were divided into two groups. In the first group, the impact wave was focused (in our study it was radial); the second group received standard kinesiotherapy. The researchers also evaluated the groups at one and three months after the end of the therapy (as in our study). They showed the therapeutic advantage of the physical procedures over the control group: VAS scale, p=0.02 at one month and p=0.002 at three months; ODI, p=0.002 at one month and p=0.002 at three months.
Moon et al22 included 30 patients with cross pain in their study; in one group they used slightly stronger shock waves than in our project (0.2 mJ/mm2; the other parameters were identical, but it should be pointed out that they used fESWT, not rESWT) compared to the placebo group (no treatment). To evaluate the therapeutic effect, the ODI was used at one and four weeks after the end of procedures. The researchers confirmed the high effectiveness of the wave in the treatment of LBP, which is consistent with our results.
Results of Schneider23 seem to correspond with the above findings, as the author postulated, on the basis of his own research, that the combination of a shock wave with manual therapy of trigger points in the spinal muscles and region of the quadratus lumborum muscle allows the achievement of the highest therapeutic efficacy in LBP.
Han et al19 included 30 patients (nine men and 21 women) in their study. The participants were divided into two comparative groups. The first group consisted of 15 patients (age 46 years, body height 163.7 cm, body weight 61.9 kg) who underwent standard physical therapy—therapeutic heat compresses on the quadrilateral lumbar region (20 mins), ultrasound therapy (five minutes), and electrotherapy for pain (15 mins). The second group consisted of 15 patients (age 49.7 years, body height 161.3 cm, body weight 62.2 kg) who underwent shock wave procedures (1000 pulses, frequency 2.5 Hz, dose 0.01–0.16 mJ/mm2). All treatments in both groups were performed twice a week for 1.5 months. The evaluation of the therapeutic effects was based on the VAS for pain and the ODI for functional status. At the end of the study, the pain decreased from 7.0 to 3.6 points in the shock wave group (in our project, the decrease was from 4.7 to only 4.4 points, but at one month after the end of treatment it was 2.7 points, and at three months it was 2.0 points). This result was significantly better than in the control group (p<0.01). For functional status, the score decreased from 30.1 to 17.5 (in our study, we recorded results of 16.1, 13.6, 9.3, and 9.3).
It is clear from the research conducted by scientists from South Korea that ESWT allows for very effective pain reduction and improvement of the functionality of patients with LBP. In our work, the patients were much less advanced in exacerbation of the disease—as evidenced by the initial results from before the therapy—than in the study by Han et al,19 but remission and advantage over the control group were observed, and, most importantly, the clinical effect was long-lasting, which was not found in the group undergoing only physical therapy and rehabilitation with sham procedures.
The aim of our study was to assess the influence of rESWT in the treatment of patients with LBP. The rESWT appeared particularly effective in the long term and achieves a stable beneficial effect compared to standard management without sudden relapse. According to follow-up analysis the use of this therapy had a significant influence on the reduction of pain and the improvement of the general functional state in relation to the conventional motor improvement program. However, in short-term the pain reduction after rESWT was not efficient immediately after treatment and results were worse than in a compared group.
Initially, the control group had a statistically significant advantage over the shock wave group (4.4 vs. 3.1 points on the VAS; p=0.039). However, in long-term observations, group A gradually experienced more pain relief than group B (2.7 vs. 3.5 points, p>0.05, at one month after treatment and 2.0 vs. 4.4 points, p<0.0001, at three months after treatment). Similar findings can be seen in the analysis of changes in pain sensations measured with the LPS. After treatment, the pain was higher in group A (5.7 vs. 4.3 points). Again, the situation completely changes in the analysis of later results. Patients with rESWT compared with the group with sham treatments, saw a significant analgesic effect (p=0.043 at one month and p<0.0001 at three months after the end of therapy). The functional state (ODI) was better in rESWT group, especially in follow-up observation (9.3 vs. 14.6 points, p=0.033, at one month and 9.3 vs. 17.8 points, p=0.004, at three months after cessation of active treatment).
Clinical Implications
This RCT provides some suggestions for the use of rESWT in clinical practice of LBP. At the moment, no recommendation can be given as to which of the two types (radial vs. focused) is more efficient. When rESWT is used to treat LBP, it seems that the best effect appears in the long term. This therapy achieves a stable, beneficial effect compared to standard management without sudden relapse. However, in short-term the pain reduction after rESWT is not effective immediately after treatment and results are usually worse than in standard program. This may mean that rESWT, as a relatively invasive physical treatment, does not show significant pain relief effects immediately after the end of the treatment period. We recommend in LBP the rESWT with 2000 pulses; 2.5 bars; 5 Hz, 7 mins; performed twice a week for five weeks.
Study Limitations
As the review of the above articles shows, a study of rESWT with selected parameters, randomization, consistent research material, sample blinding, strict inclusion and exclusion criteria, and analysis of early and later results was justified. However, the material collected should be verified by other research centers to confirm or refute the results obtained in this study. So far, there are too few studies of a sufficient scientific standard to determine the clinical value of rESWT in the treatment of LBP. The results of previous studies are promising but require further verification. In future, the performance of radial shock waves should be checked using more precise measuring tools (e.g., surface electromyography, isokinetic systems, and posturographic platforms). It is also worthwhile conducting a randomized clinical trial with a comparison of rESWT and fESWT during one experiment. The small number of patients in both groups in the current study was also a weakness of the work. The effectiveness of ESWT should certainly be verified with a larger sample.
Conclusion
The rESWT method seems to be effective for patients with LBP, both in the short- and in particular in the long-term, and has a significant advantage over the placebo effect (within the study’s scope). The use of this therapy has a significant influence on the reduction of pain and the improvement of the general functional state in relation to the conventional motor improvement program.
Abbreviations
BMP-2, bone morphogenic protein-2; BMSCs, bone marrow stromal cells; eNOS, nitric oxide synthase; ESWT, extracorporeal shock wave therapy; LBP, low back pain; LPS, Laitinen Pain Scale; MRI, magnetic resonance imaging; OA, osteoarthritis; ODI, Oswestry Disability Index; PCNA, proliferating cell nuclear antigen; rESWT, radial extracorporeal shock wave therapy; RUNX2, runt-related transcription factor 2; TENS, transcutaneous electrical nerve stimulation; VAS, Visual Analog Scale; VEGF, vessel endothelial growth factor.
Acknowledgment
The certificated English language services were provided by an academic highly qualified native speaker.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Hawthorne G, de Morton N, Kent P. Back pain and social isolation: cross-sectional validation of the friendship scale for use in studies on low back pain. Clin J Pain. 2013;29(3):245–252. doi:10.1097/AJP.0b013e31824b3aed
2. Kent P, Mirkhil S, Keating J, Buchbinder R, Manniche C, Albert HB. The concurrent validity of brief screening questions for anxiety, depression, social isolation, catastrophization, and fear of movement in people with low back pain. Clin J Pain. 2014;30(6):479–489. doi:10.1097/AJP.0000000000000010
3. Finco G, Mura P, Musu M, et al. Long-term, prolonged-release oral tapentadol for the treatment of refractory chronic low back pain: a single-center, observational study. Minerva Med. 2018;109(4):259–265. doi:10.23736/S0026-4806.18.05641-0
4. Miller SM. Low back pain: pharmacologic management. Prim Care. 2012;39(3):499–510. doi:10.1016/j.pop.2012.06.005
5. Oliveira CB, Maher CG, Pinto RZ, et al. Clinical practice guidelines for the management of non-specific low back pain in primary care: an updated overview. Eur Spine J. 2018;27(11):2791–2803. doi:10.1007/s00586-018-5673-2
6. Akodu AK, Akindutire OM. The effect of stabilization exercise on pain-related disability, sleep disturbance, and psychological status of patients with non-specific chronic low back pain. Korean J Pain. 2018;31(3):199–205. doi:10.3344/kjp.2018.31.3.199
7. Byrnes K, Wu P-J, Whillier S. Is Pilates an effective rehabilitation tool? A systematic review. J Bodyw Mov Ther. 2018;22(1):192–202. doi:10.1016/j.jbmt.2017.04.008
8. Gomes-Neto M, Lopes JM, Conceição CS, et al. Stabilization exercise compared to general exercises or manual therapy for the management of low back pain: a systematic review and meta-analysis. Phys Ther Sport. 2017;23:136–142. doi:10.1016/j.ptsp.2016.08.004
9. Rajfur J, Pasternok M, Rajfur K, et al. Efficacy of selected electrical therapies on chronic low back pain: a comparative clinical pilot study. Med Sci Monit. 2017;23:85–100. doi:10.12659/MSM.899461
10. Jauregui JJ, Cherian JJ, Gwam CU, et al. A meta-analysis of transcutaneous electrical nerve stimulation for chronic low back pain. Surg Technol Int. 2016;28:296–302.
11. Foldager CB, Kearney C, Spector M. Clinical application of extracorporeal shock wave therapy in orthopedics: focused versus unfocused shock waves. Ultrasound Med Biol. 2012;38(10):1673–1680. doi:10.1016/j.ultrasmedbio.2012.06.004
12. Dymarek R, Halski T, Ptaszkowski K, Slupska L, Rosinczuk J, Taradaj J. Extracorporeal shock wave therapy as an adjunct wound treatment: a systematic review of the literature. Ostomy Wound Manage. 2014;60(7):26–39.
13. Wang C-J, Wang F-S, Yang KD, et al. Shock wave therapy induces neovascularization at the tendon-bone junction. A study in rabbits. J Orthop Res. 2003;21(6):984–989. doi:10.1016/S0736-0266(03)00104-9
14. Yin T-C, Wang C-J, Yang KD, Wang F-S, Sun Y-C. Shockwaves enhance the osteogenetic gene expression in marrow stromal cells from hips with osteonecrosis. Chang Gung Med J. 2011;34(4):367–374.
15. Wang C-J, Sun Y-C, Wong T, Hsu S-L, Chou W-Y, Chang H-W. Extracorporeal shockwave therapy shows time-dependent chondroprotective effects in osteoarthritis of the knee in rats. J Surg Res. 2012;178(1):196–205. doi:10.1016/j.jss.2012.01.010
16. Santamato A, Beatrice R, Micello MF, et al. Power doppler ultrasound findings before and after focused extracorporeal shock wave therapy for achilles tendinopathy: a pilot study on pain reduction and neovascularization effect. Ultrasound Med Biol. 2019;45(5):1316–1323. doi:10.1016/j.ultrasmedbio.2018.12.009
17. Tomska N, Turoń-Skrzypińska A, Szylińska A, et al. Deep electromagnetic stimulation and radial shock wave therapy in back pain. Ortop Traumatol Rehabil. 2018;20(3):189–195. doi:10.5604/01.3001.0012.0943
18. Lin S-F, Chen Y-J, Tu H-P, et al. The effects of extracorporeal shock wave therapy in patients with coccydynia: a randomized controlled trial. PLoS One. 2015;10(11):e0142475. doi:10.1371/journal.pone.0142475
19. Han H, Lee D, Lee S, Jeon C, Kim T. The effects of extracorporeal shock wave therapy on pain, disability, and depression of chronic low back pain patients. J Phys Ther Sci. 2015;27(2):397–399. doi:10.1589/jpts.27.397
20. Lee S, Lee D, Park J. Effects of extracorporeal shockwave therapy on patients with chronic low back pain and their dynamic balance ability. J Phys Ther Sci. 2014;26(1):7–10. doi:10.1589/jpts.26.7
21. Notarnicola A, Maccagnano G, Gallone MF, et al. Extracorporeal shockwave therapy versus exercise program in patients with low back pain: short-term results of a randomised controlled trial. J Biol Regul Homeost Agents. 2018;32(2):385–389.
22. Moon YE, Seok H, Kim S-H, Lee SY, Yeo JH. Extracorporeal shock wave therapy for sacroiliac joint pain: A prospective, randomized, sham-controlled short-term trial. J Back Musculoskelet Rehabil. 2017;30(4):779–784. doi:10.3233/BMR-150405
23. Schneider R. Effectiveness of myofascial trigger point therapy in chronic back pain patients is considerably increased when combined with a new, integrated, low-frequency shock wave vibrotherapy (Cellconnect Impulse): a two-armed, measurement repeated, randomized, controlled pragmatic trial. J Back Musculoskelet Rehabil. 2018;31(1):57–64. doi:10.3233/BMR-169662
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.