")
Back to Journals » Drug Design, Development and Therapy » Volume 10
Spotlight on fluticasone furoate/vilanterol trifenatate for the once-daily treatment of asthma: design, development and place in therapy
Authors Albertson TE, Bullick SW, Schivo M, Sutter ME
Received 17 September 2016
Accepted for publication 16 November 2016
Published 14 December 2016 Volume 2016:10 Pages 4047—4060
DOI https://doi.org/10.2147/DDDT.S113573
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr James Janetka
Timothy E Albertson,1–3 Samuel W Bullick,1,3 Michael Schivo,1 Mark E Sutter2,3
1Division of Pulmonary, Critical Care and Sleep Medicine, Department of Internal Medicine, 2Department of Emergency Medicine, School of Medicine, UC Davis, Sacramento, 3Department of Medicine, Veterans Administration Northern California Health Care System, Mather, CA, USA
Abstract: The use of inhaled corticosteroids (ICSs) plays a key role in the treatment of asthmatic patients, and international guidelines have designated ICSs as an early maintenance therapy in controlling asthma symptoms. When asthmatic patients remain symptomatic on ICSs, one common option is to add a long-acting beta2 agonist (LABA) to the maintenance treatment. Fixed combination inhalers that contain both an ICS and a LABA have been popular for both chronic obstructive pulmonary disease (COPD) and asthma. Historically, these inhalers have been dosed twice daily. However, currently, there is a once-daily combination therapy with the ICS fluticasone furoate (FF) and the LABA vilanterol trifenatate (VI) with indications for use in both COPD and asthma. This dry powder inhaler (DPI) comes in two doses of FF (100 or 200 µg) both combined with VI (25 µg). This article reviews the clinical trial data for FF, VI and FF/VI combination inhalers and documents the efficacy and safety of once-daily inhaled maintenance therapy by DPI in asthmatic patients.
Keywords: fluticasone furoate/vilanterol trifenatate, asthma, long-acting beta2 agonist, inhaled corticosteroid, combined inhaler, persistent asthma, dry powder inhaler
Introduction
Asthma is an airway disease of inflammation and bronchoconstriction. Genetics and environmental factors combine to produce different asthma phenotypes and various responses to controller medications. The Global Initiative for Asthma (GINA) updated in 20161 is an ongoing international effort to provide a unified approach to the diagnosis and treatment of asthma. Table 1 summarizes the GINA general treatment approach to asthma that uses a stepwise function based on the severity of asthma symptoms. The table shows that inhaled corticosteroids (ICSs) play a major role as maintenance or preventative treatments in this stepwise approach to asthma. Table 2 summarizes the currently available and approved handheld inhalers by the US Food and Drug Administration (FDA) and several others not available in the USA. Fluticasone furoate (FF) is a potent corticosteroid that is dosed once daily due to its long half-life when inhaled. It was approved by the FDA as a once-daily ICS for the maintenance treatment of asthma as a dry powder inhaler (DPI) in August 2014 with the brand name Arnuity™ Ellipta® (GSK, USA).2
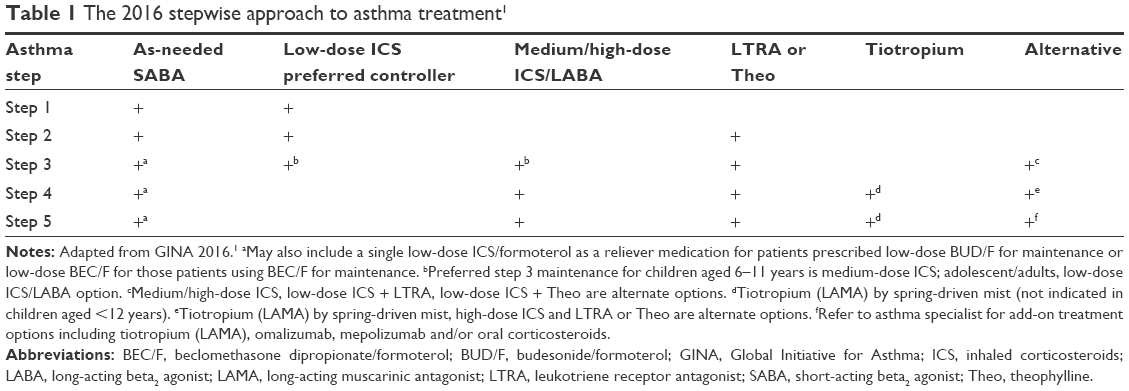 | Table 1 The 2016 stepwise approach to asthma treatment1 |
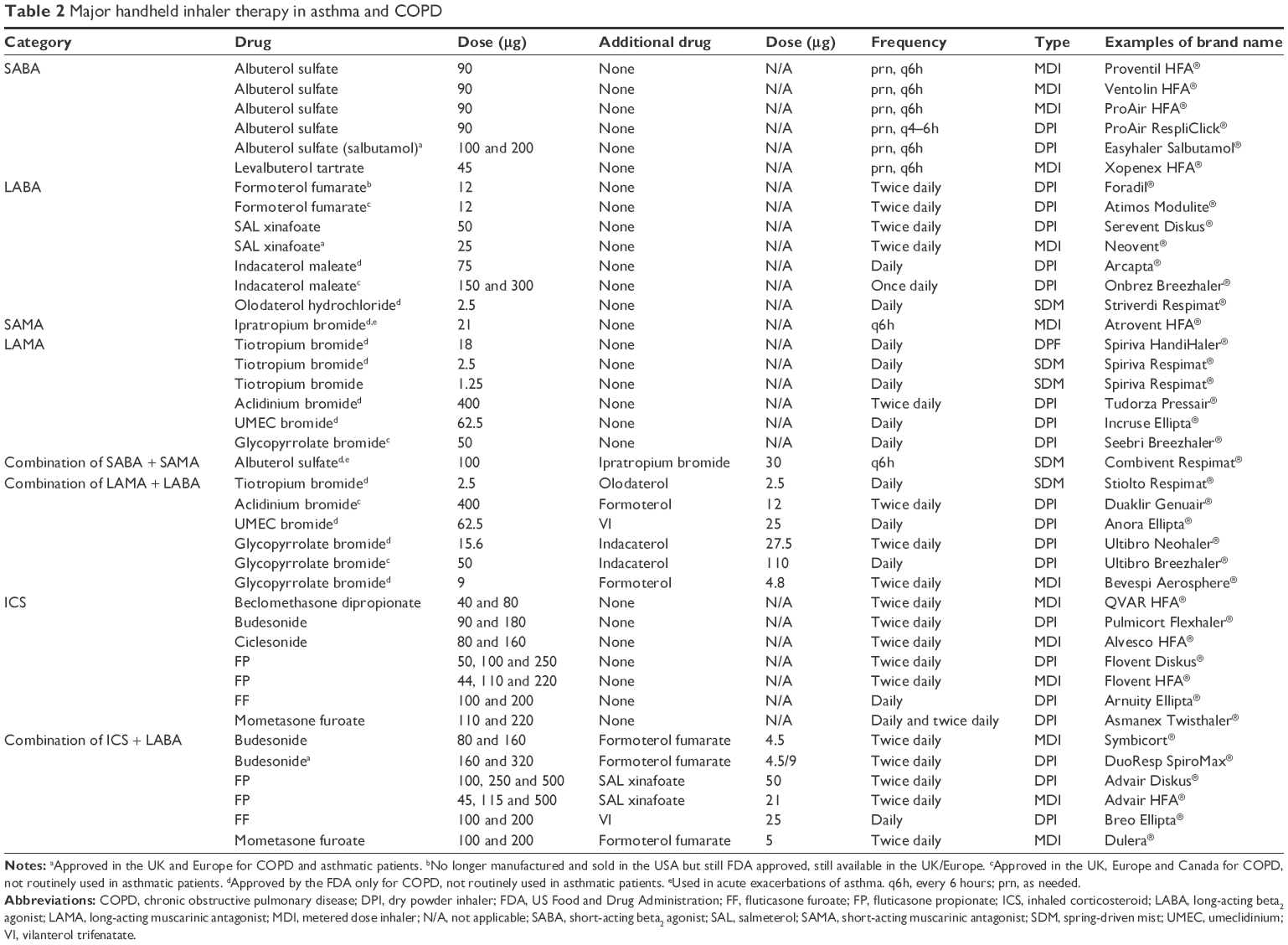 | Table 2 Major handheld inhaler therapy in asthma and COPD |
Controversy exists as to the role of long-acting beta2 agonists (LABAs) in the maintenance treatment of moderate to severe asthmatics. Early clinical trials of the LABA salmeterol (SAL) noted a nonstatistically significant increase in all-cause mortality in asthmatic patients treated over 16 weeks when compared to those using the short-acting beta2 agonist (SABA), albuterol.3 A large 2006 clinical trial of 26,355 asthmatics named the Salmeterol Multicenter Asthma Research Trial (SMART) evaluated SAL by metered dose inhaler (MDI) compared to placebo MDI over 28 weeks.4 The use of ICS and leukotriene modifiers was equal in both groups (47% and 11%, respectively). The primary outcome included respiratory-related deaths or life-threatening events, and both were infrequent for the SAL group (50 patients) and placebo group (36 patients). This difference did not reach statistical significance (relative risk [RR] =1.40, 95% confidence interval [CI] =0.91–2.14). When secondary outcomes were explored, a small but significant increase in respiratory-related deaths was found in the SAL group (SAL 24 vs placebo 11; RR =2.16, 95% CI =1.06–4.41) along with specific asthma-related deaths (SAL 13 vs placebo 3; RR =4.37, 95% CI =1.25–15.4). The secondary outcome imbalances were largely related to the effects on the African-American subpopulation (20 SAL vs 5 placebo; RR =4.92, 95% CI =1.54–10.90).4 This study and a few others resulted in the FDA requiring a “black box” warning for all inhaled LABA agents based on the “risk” of their use in asthma.
Recent studies have called into question if there is an increase in risk to asthmatic patients treated with a combination ICS/LABA inhaler. In 2016, Peters et al5 studied 11,693 adult and adolescent asthmatic patients ≥12 years of age for 26 weeks. They were randomized to the ICS budesonide alone or a fixed-dose combination of budesonide and the LABA formoterol given twice daily by MDI. The budesonide/formoterol (BUD/F) combination was found to be noninferior to budesonide alone with 43 patients having a serious asthma-related event in the BUD/F group and 40 patients in the budesonide-alone-treated group (hazard ratio [HR] =1.07, 95% CI =0.70–1.65). The risk of an asthma exacerbation was 16.5% lower in the BUD/F-treated group compared to the budesonide-alone-treated group (HR =0.84, 95% CI =0.74–0.94).5 A similarly designed study in 11,679 asthmatic patients ≥12 years of age treated for 26 weeks also found that the combined fixed-dose fluticasone propionate (FP)/SAL did not have a significantly higher risk of serious asthma-related events and did have a 21% reduction in severe asthma exacerbations than those treated with fluticasone alone.6 Similarly, when a fixed combination inhaler of SAL and FP was compared to inhaled FP alone in 6,208 asthmatic children aged 4–11 years, non-inferiority for serious asthma-related events was seen (HR =1.28, 95% CI =0.73–2.27).7 These and other data suggest that the combination of an ICS with LABA is a safe and an effective treatment for asthma. Furthermore, the use of both an ICS and a LABA is an integral part of the GINA guidelines (Table 1) for the asthma patient at the step 3–step 5 levels.1 Table 2 summarizes the multiple handheld inhalers available in the USA. At this time, LABA monotherapy without the simultaneous use of an ICS is still discouraged and has recently been described as “medical negligence” in children with asthma.8
The fixed combination of FF (100 or 200 μg) combined with the LABA vilanterol trifenatate (VI; 25 μg) was approved in the USA in May 2013 for the maintenance treatment of chronic obstructive pulmonary disease (COPD) as the once-daily DPI Breo Ellipta® (GSK, USA). The same year, the same combination of drugs, doses and delivery system (Relvar Ellipta®; GSK, UK) was approved in Japan and the European Union for the treatment of asthma.9 Breo Ellipta (FF [100 or 200 μg]/VI [25 μg]) was approved by the FDA for the maintenance treatment of asthma in April 2015.2 This article reviews the data that support the use of the fixed-dose combination of DPI FF with VI as a once-daily asthma maintenance treatment.
FF in asthma
The inhaled use of FF in asthma is in part based on its long half-life in the lung that allows once-daily dosing for asthma maintenance therapy.10 As given in Table 1, ICS therapy plays a major role in the current GINA guidelines. When as-needed SABAs become inadequate to control asthma symptoms, the use of low-dose ICS should be considered as early as step 1 and used through step 2 into step 3 as medium- to high-dose ICS. The 100 μg daily DPI dose of FF is considered low-dose ICS therapy for asthmatics aged 12 years and older.1 After the addition of a LABA to low-dose ICS therapy at step 3, higher medium- or high-dose ICS therapy is recommended by the GINA guidelines for asthmatic patients that remain symptomatic. The 200 μg daily DPI dose of FF is considered a “high-dose” ICS and can be used for symptomatic step 3–5 asthmatic patients.1
Table 3 summarizes the major clinical trials that have examined the use of FF as an ICS maintenance asthma therapy. Efficacy and safety have been verified with once-daily FF dosing in asthmatic patients in several studies. An 8-week study of 545 adolescent and adult asthmatic patients demonstrated significant (all P≤0.033) improvements with FF in pre-dose and placebo-adjusted forced expiratory volume at 1 second (FEV1). Once-daily evening-dosed FF (400 μg) was also as effective as twice-daily dosing (200 μg) of the same total daily FF dose in improving placebo-adjusted FEV1 (≥200 mL).11 In this study, the morning-dosed FF (400 μg) was found to be less effective than an equal dose of FF (200 μg) given twice daily (202 mL improvement, 95% CI =96–307 vs 315 mL improvement, 95% CI =208–421 mL).11 A randomized, double-blind, double-dummy and placebo-controlled study further evaluated once-daily FF (100 μg) given in the morning compared to the evening over a 2-week trial in asthmatics aged 18–70 years who required an ICS to control symptoms.12 Inhaled FF (100 μg) daily increased 24-hour weighted mean FEV1 relative to placebo (for AM dosing, 77 mL; 90% CI =1–152 mL and for PM dosing, 105 mL; 90% CI =29–180 mL)13 and found that the difference in the increase when FF was given in the morning or evening was negligible (adjusted differences, 28 mL; 90% CI =−102–45 mL).12 A longer 24-week multicenter, double-blind, parallel-group study compared once-daily evening doses of FF (100 μg) to FF (200 μg).13 Both FF doses improved least-squares mean trough FEV1 from baseline by 208 mL in the FF (100 μg) group and 284 mL in the FF (200 μg) group (treatment difference, 77 mL; 95% CI =−39–192 mL).13 Similar improvements were seen in rescue- and symptom-free days, morning and evening peak expiratory flow (PEF) and reported adverse events with the two FF doses. The 200 μg FF-treated group was 42% more likely to have well-controlled symptoms than the 100 μg FF-treated group. There were no safety concerns, and no clinically relevant effects on 24-hour urinary cortisol levels with either of the doses of inhaled FF were found.13
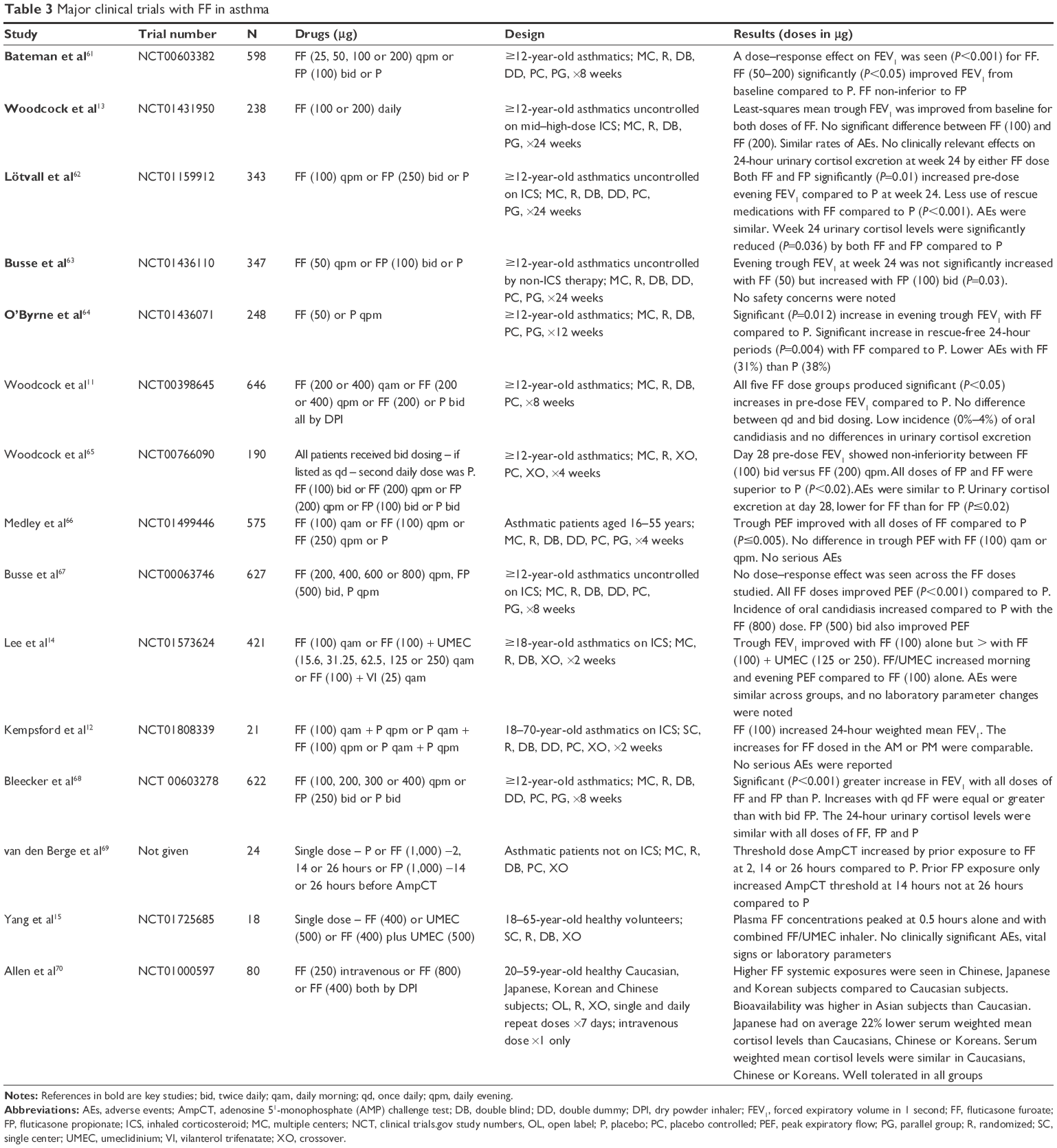 | Table 3 Major clinical trials with FF in asthma |
When inhaled FF (100 μg) daily for 2 weeks was compared to FF (100 μg) combined with the long-acting muscarinic antagonist (LAMA), umeclidinium (UMEC; 15.6, 31.25, 62.5, 125 or 250 μg), in adult asthmatics, trough FEV1 was improved with FF (100 μg) alone (by 87 mL) compared to baseline, but they increased even more when FF (100 μg) was combined with UMEC doses (141–214 mL).14 When least-squares mean change in trough FEV1 was evaluated, statistically significant differences were seen with FF (100 μg)/UMEC (125 and 250 μg; both 55 mL, P=0.018) compared to FF (100 μg) alone.14 In addition, both morning and evening PEF improved more with the combination of FF with UMEC daily inhalation compared to FF alone. The FF serum concentrations peaked at half an hour when given alone, and this did not change when combined with UMEC.15 The use of daily FF given by DPI has a proven efficacy in asthmatic patients requiring an ICS for symptom control. The combination of FF with LAMA appears to increase the efficacy compared to FF alone in asthmatic patients.
The use of VI in asthma
Several new LABA agents designed for once-daily dosing are available or under study including indacaterol, olodaterol, abediterol and VI.16 Appropriate concern for the use of LABA agents alone as maintenance therapy has mandated that asthmatic subjects in most clinical studies evaluating the use of the inhaled LABA VI be currently on an ICS (Table 4). An exception is the study by Kempsford et al.17 Inhaled VI was given once daily (25–100 μg) for 14 days to healthy volunteers and once to patients with either asthma or COPD. Inhaled VI was rapidly absorbed with a median time to maximal serum concentrations of 5 minutes in healthy subjects and 10 minutes for asthma and COPD patients. All VI doses improved FEV1 by 5 minutes and maintained increased FEV1 up to 24 hours after inhalation in patients with asthma or COPD.17 No clinically significant adverse effects were found including evaluations of vital signs, 12-lead electrocardiogram (ECG), Holter ECG, blood glucose or potassium levels. Table 4 summarizes five placebo-controlled clinical trials in asthmatics on an ICS that evaluated inhaled VI using a DPI device lasting between 1 and 12 weeks. Doses between 3 and 50 μg daily of inhaled VI were tried, and the bronchodilator effect lasted at least 24 hours for VI doses 12.5–50 μg.18 The efficacy and safety of once-daily VI dosing in asthmatics were established by Sterling et al19 who evaluated 72 adult (≥18 years old) asthmatics on an ICS with a 7-day treatment of daily inhaled VI (6.25, 12.5 and 25 μg), twice-daily inhaled VI (6.25 μg) or placebo using a DPI. The VI treatment in asthmatics resulted in a statistically significant (P<0.001 for all doses) increase on day 7 in trough FEV1 and weighted mean 24-hour FEV1 versus placebo. The differences from placebo for trough FEV1 with once-daily VI were 94 mL (95% CI =49–140 mL), 102 mL (95% CI =57–147 mL) and 125 mL (95% CI =80–170 mL) for 6.25, 12.5 and 25 μg doses, respectively. The 6.25 μg VI twice-daily dose resulted in 140 mL (95% CI =95–185 mL) improvement in trough FEV1 compared to placebo.19 Non-inferiority between once-daily versus twice-daily VI dosing was also shown.19
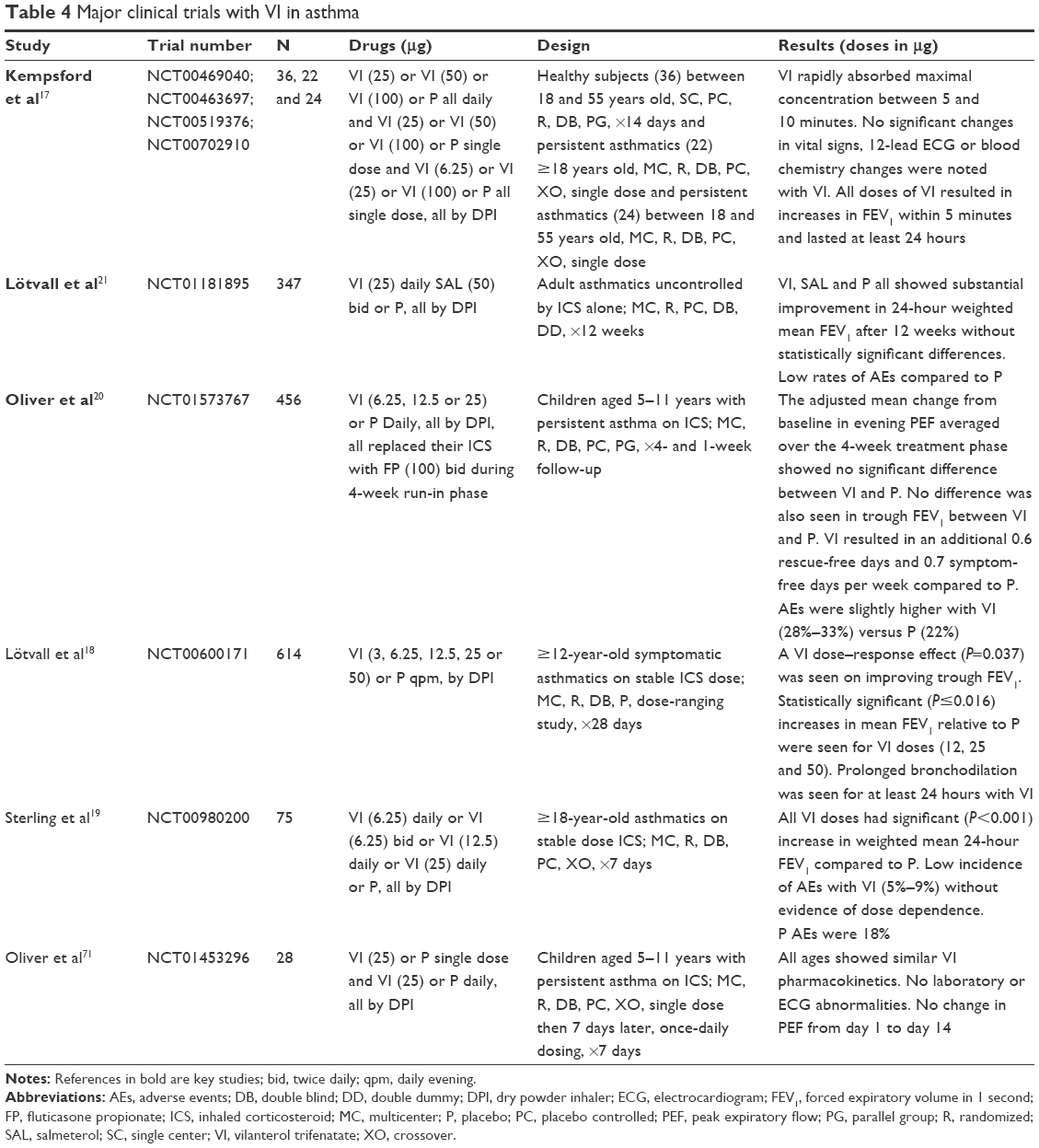 | Table 4 Major clinical trials with VI in asthma |
A recent large trial children aged 5–11 years (N=456) with persistent asthma symptoms inadequately controlled on an ICS were randomized to once-daily inhaled VI (6.25, 12.5 or 25 μg), and this was compared to placebo over 4 weeks. It demonstrated safety but failed to show an improvement from baseline in trough FEV1 for any of the VI doses tested.20 Adult asthmatic patients uncontrolled on an ICS (N=347) were given once-daily VI (25 μg) for 12 weeks and were compared to those given twice-daily SAL or placebo. Researchers noted the improvement in FEV1 of 359±42.9 mL with VI, 283±41.9 mL with SAL and 289±42.9 mL for placebo.21 The increase in FEV1 was not statistically significantly different between VI and placebo. Overall, these data suggest that there is a variable response to inhaled VI in adult patients with persistent symptoms already on an ICS and even less efficacy of VI in asthmatic children on an ICS.
The use of FF and VI in asthma
Pharmacodynamic, pharmacokinetic and safety data have been tested with inhaled FF/VI in several populations, including healthy Chinese and Japanese, in patients simultaneously on ketoconazole and in patients with renal and hepatic impairment.22–25 Stable pharmacokinetics and pharmacodynamics and no safety concerns over the use of inhaled FF/VI were found in these studies. Allergen and methacholine challenge tests were used in 27 patients randomized to inhaled FF (100 μg), VI (25 μg), FF (100 μg)/VI (25 μg) or placebo.26 Using the allergen challenge to test early asthmatic response (EAR) and airway hyperresponsiveness (AHR), researchers found a decrease in FEV1. Using the mean 0–2 hours post allergen challenge FEV1, the least decrease was reported with the pre-challenge dosing of the combination FF/VI inhaler (−0.614 L, 95% CI =−0.858 to −0.370) and the greatest decrease was after placebo inhaler (−1.091 L, 95% CI =−1.344 to −0.837). The methacholine challenge test was used in these patients to model late asthmatic response (LAR) and AHR at 24 hours. Weighted mean FEV1 4–10 hours post challenge was reduced after placebo (−466 mL, 95% CI =−589 to −343) but actually increased with FF (100 μg; 18 mL, 95% CI =−89 to 125) and with FF (100 μg)/VI (25 μg; 18 mL, 95% CI =−89 to 124). It was also improved compared to placebo with VI (25 μg; −298 mL, 95% CI =−415 to −181).26 The use of the combined FF/VI provided statistically significant protection against the EAR of AHR compared to its components alone and to placebo. There was also statistically significant protection with combination FF/VI therapy when compared to placebo and VI alone against the LAR of AHR.
Cytochrome P450 3A4 (CYP3A4) is the major hepatic enzyme responsible for metabolizing FF by ester hydrolysis with the formation of the 17 beta-carboxylic acid and loss of the S-fluoro-methyl-carbothioate.24,27 FF is also believed to be a substrate for the P-glycoprotein (PgP) efflux transporter, and enterocytes may have a major metabolic effect on FF in the gastrointestinal track.27 The hepatic enzyme CYP3A4 also plays a major role in the metabolism of VI by O-dealkylation.28 It is also believed to be a substrate for PgP when in the gastrointestinal system.24 Ketoconazole is a probe used to assess the potential effect of CYP3A4 metabolic inhibition, and it also has inhibitory effects on PgP.24 Coadministration of repeat doses of ketoconazole 400 mg daily and inhaled VI (25 μg) alone had no pharmacodynamic or pharmacokinetic effect on VI. When 11 days of 400 mg oral ketoconazole daily was coadministered with inhaled FF (200 μg)/VI (25 μg) from days 5 to 11, no statistical or clinical effect was seen on heart rate or minimal potassium levels.24 There was a 27% decrease in 24-hour weighted mean serum cortisol levels (treatment ratio =0.73, 90% CI =0.62–0.86). An increase in the FF area under the plasma concentration 0–24-hour curve by 36% with ketoconazole (90% CI =16%–59%) was reported. The area under the plasma concentration 0–24-hour VI curve increased by 65% (90% CI =38%–97%).24 Table 5 summarizes the major pharmacokinetic parameters of FF and VI that allow once-daily dosing for this inhaled fixed combination medication.
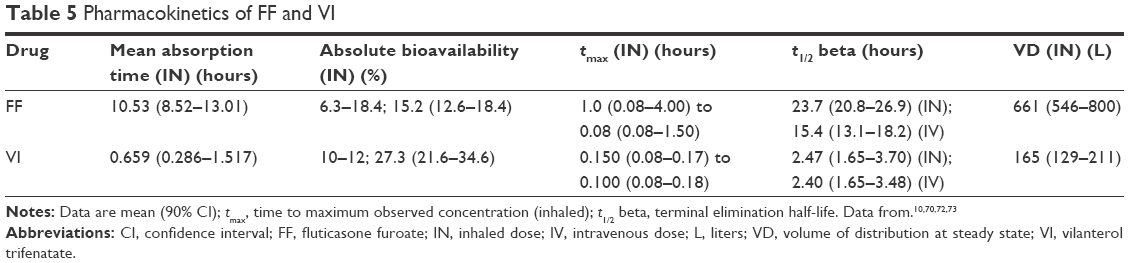 | Table 5 Pharmacokinetics of FF and VI |
Table 6 summarizes the major clinical trials evaluating pharmacokinetics, safety and efficacy of FF/VI given by DPI in asthmatic patients. Large randomized double-blind clinical trials have shown improved FEV1 and PEF measures by treatment with FF/VI compared to placebo or the same or better measures with active control agents such as inhaled FP and FP with the LABA SAL twice daily.29–36 These clinical trials lasted from 2 to 52 weeks and evaluated efficacy and safety. Two trials each of 12-week duration have confirmed the efficacy of FF (100–200 μg)/VI (25 μg) given daily by DPI in Asian asthmatic patients compared to placebo37 and compared to the active comparator FP using PEF measures of efficacy.38
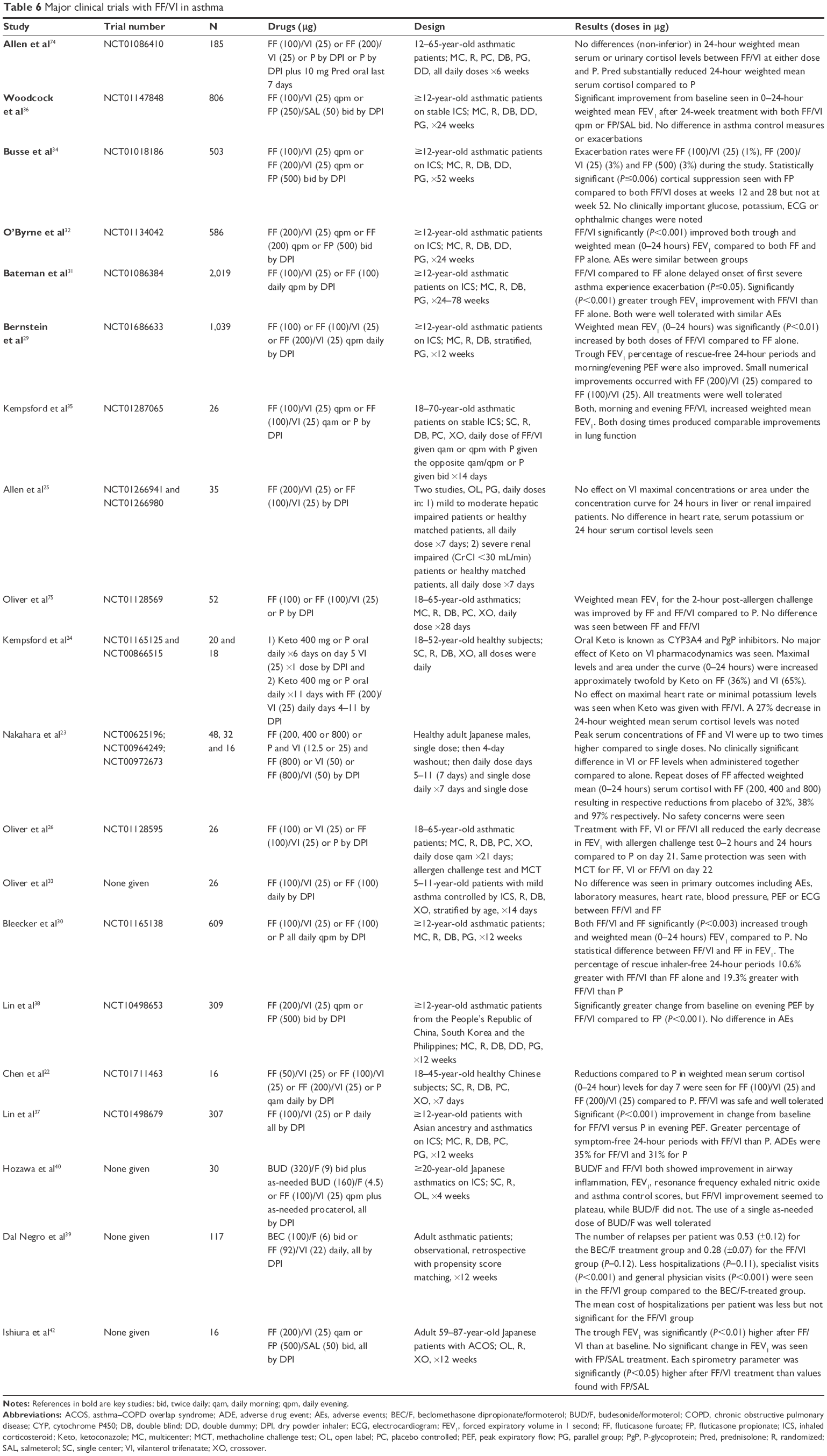 | Table 6 Major clinical trials with FF/VI in asthma |
An observational study from Italian National Health Service data used propensity score matching on baseline covariates of gender, age, FEV1 and comorbidities on 40 adult asthmatic patients. They were treated with FF (100 μg)/VI (25 μg) by DPI once daily or beclomethasone dipropionate/formoterol (BEC/F) inhalation twice daily.39 The BEC/F-treated group had 0.28 (±0.12) days of hospitalization, and those treated with FF/VI had 0.08 (±0.04) days of hospitalization (P=0.09) during the 12-week analysis period. Both the number of physician visits and the number of specialist visits were statistically reduced in the FF/VI-treated group compared to the BEC/F-treated group.39 Another small comparison study (N=30) in Japan evaluated BUD (160 μg)/F (4.5 μg) two puffs twice daily and one additional inhalation as needed of BUD/F each day versus FF (100 μg)/VI (25 μg) by DPI daily over 4 weeks in asthmatics ≥20 years who required an ICS.40 Both drug combinations showed statistically significant (P<0.001) improvement in the asthma control questionnaire during the 4 weeks with greater improvement in the scores with the BUD/F-treated group. Both groups also showed decreases (P<0.001) in fractional exhaled nitric oxide (FeNO) from baseline to week 4 with the levels in the BUD/F group reduced greater (P<0.001) than the FF/VI-treated group. The use of a fixed-dose ICS/LABA as a rescue medication in this study goes against historical dogma of using SABA agents as rescue medication in asthma but is in the GINA guidelines (Table 1). In addition, direct comparisons between different combinations of ICS/LABA beg the question of dosage equivalence. In this study, perhaps the comparator should have been FF (200 μg)/VI (25 μg) as a high-dose ICS as opposed to the low-dose FF (100 μg)/VI (25 μg) combination.
The asthma–COPD overlap syndrome (ACOS) is an asthma phenotype that shares features of both asthma and traditional COPD.1,41 A small (N=16) open-label, randomized, crossover study of patients with ACOS in Japan compared once-daily FF (200 μg)/VI (25 μg) versus FP (500 μg)/SAL (50 μg) twice daily for 4-week treatment periods.42 The mean value of FEV1 was 1.33 L (±1.29) during the run-in period, 138 L (±0.39) after the FP/SAL treatment and 1.47 (±0.38) L after the FF/VI treatment. The mean value of FEV1 was significantly (P<0.01) greater in the FF/VI treatment group compared to the run-in period in these patients with ACOS. Although a small trial of short duration, it is one of the few pharmacological trials in patients with ACOS and the only randomized trial evaluating the FF/VI combination inhaler in patients with ACOS phenotype.
A large pragmatic study evaluating FF (100 or 200 μg)/VI (25 μg) inhaler use versus existing asthma maintenance therapies is ongoing. The Salford Lung Study is a randomized and controlled trial started before FF/VI inhalers were approved for asthma treatment. It utilizes the Salford electronic medical record to give near real-time data collection and monitoring of safety data at 66 primary care sites in and around Salford and South Manchester, England.43 The data from this study when available will complement the more standard double-blind, randomized, controlled trials evaluating real-world efficacy and obtaining risk/benefit information on inhaled FF/VI.
When East Asian patients were compared to non-East Asian patients from the large randomized, double-blind, multicenter clinical trials in a prespecified subgroup analysis, both FF (100 or 200 μg)/VI (25 μg) dose combinations were as effective in improving FEV1 compared to placebo as in non-East Asian patients.44 A systematic review with meta-analysis of seven published trials (N=5,668) evaluating inhaled FF/VI in asthmatic patients was recently performed.45 The combination therapy of FF (100 or 200 μg)/VI (25 μg) daily increased trough FEV1 in asthmatics treated longer than 8 weeks compared to either FP twice daily or FF daily alone. Three of the seven trials compared FF (100 or 200 μg)/VI (25 μg) doses to FF (100 μg) once daily and showed a significant (P≤0.001) increase in trough FEV1 of 90 mL (95% CI =60–120 mL) with the combination inhaler compared to FF alone.45
Medication adherence with inhalers
Medication adherence or following the medication plan is a significant problem and factor in the treatment of chronic diseases.46 Dosing frequency has a major effect on the rate of nonadherence of medication in chronic diseases.47 When medications are given twice daily compared to once daily, the adherence rates were significantly lower, with regimen adherence reduced by 13.1% and timing adherence reduced by 26.7% compared to once daily.47 The adherence rates fall 23.1% for regimen adherence and 54.2% for timing adherence when medications are given four times daily compared to daily dosing. Nonadherence to treatment is associated with poor baseline asthma control.48,49 The nonadherence rates among asthmatic patients range between 30% and 70%, and because of this the assessment of medication adherence is a critical part of evaluating the difficult to treat asthma patient.50,51 Integrated and innovative approaches to patients are needed to improve medication adherence in difficult asthmatic patients.52 Once-daily medications and the combination of an ICS with a LABA in a single inhaler are associated with improved medication adherence compared to that of an ICS alone.53,54 Better medication adherence must be addressed and will improve health outcomes and asthma disease control.55,56
In addition to being a daily combination dosing asthma maintenance medication, Breo Ellipta (GSK) utilizes the Ellipta delivery system. The Ellipta dry powder system (GSK, UK and Japan) has been shown to be easy to use and preferred over the Breezhaler (Novartis Pharma UK, Japan) in device-naive Japanese volunteers.57 When semi-structured, in-depth, qualitative interviews were conducted on asthma and COPD patients after using Ellipta (GSK, Germany) dry powder inhalation systems, the Ellipta device was associated with the highest patient satisfaction and preference.58 Patient preference for the Ellipta device was also demonstrated in 287 COPD patients randomized to the Ellipta or Diskus DPIs.59 The Ellipta device was significantly preferred (P<0.001) over the Diskus device in all categories. Overall inhaler preference was 67% for the Ellipta device and 31% for the Diskus.59 Once-daily dosing with the FF/VI Ellipta device and its high patient preference are also likely to contribute to improved asthma medication adherence.
To date, a large amount of clinical trial data exists supporting the efficacy and safety of the use of inhaled FF/VI by DPI for asthma maintenance treatment. The combination ICS/LABA of FF/VI fits well into the GINA guidelines starting as early as step 3.1 Studies looking at a fixed-dose triple-combination inhaler with FF, VI and the LAMA UMEC are ongoing in healthy volunteers, being developed for COPD indication and could be evaluated in asthmatic patients.60
Conclusion
The DPI inhaler, FF/VI, is a fixed combination of two strengths of FF (100 or 200 μg) both with VI (25 μg) used as a maintenance treatment in asthmatic patients not controlled on just an ICS therapy alone. The doses of FF cover low- and high-dose ICS categories and fit nicely into the current GINA asthma treatment guidelines. Clinical trials have focused on each of the components of the combination inhaler. Efficacy and safety were demonstrated with inhaled FF in asthmatic patients. Similarly, efficacy and safety were demonstrated in clinical trials in adolescent and adult asthmatic patients on an ICS with adding inhaled VI but not in children aged 5–11 years. The data supporting the combined use of FF/VI in asthmatic patients requiring ICS are strong and document its efficacy and safety in long-term, large and randomized clinical trials in adolescents and adults. Pharmacokinetics and pharmacodynamics have been well studied and have demonstrated limited clinically important drug interactions (eg, ketoconazole) and minimal alterations from renal and liver impairments. Limited efficacy data with inhaled FF/VI exist for asthmatic children (<12 years). Further studies on asthmatic children and various asthma phenotypes such as patients with ACOS are needed to better understand the full spectrum of the use of inhaled fixed combination FF/VI in the maintenance treatment of asthma.
Disclosure
The authors report no conflicts of interest in this work.
References
Asthma GINA Guidelines [homepage on the Internet]. Pocket Guide for Asthma Management and Prevention. 2016. Available from: www.ginasthma.org. Accessed September 1, 2016. | ||
US FDA [database on the Internet]. 2016; Available from: https://www.accessdata.fda.gov/scripts/cder/drugsatfda/. Accessed September 1, 2016. | ||
Castle W, Fuller R, Hall J, Palmer J. Serevent nationwide surveillance study: comparison of salmeterol with salbutamol in asthmatic patients who require regular bronchodilator treatment. BMJ. 1993;306(6884):1034–1037. | ||
Nelson HS, Weiss ST, Bleecker ER, Yancey SW, Dorinsky PM, Group SS. The Salmeterol Multicenter Asthma Research Trial: a comparison of usual pharmacotherapy for asthma or usual pharmacotherapy plus salmeterol. Chest. 2006;129(1):15–26. | ||
Peters SP, Bleecker ER, Canonica GW, et al. Serious asthma events with budesonide plus formoterol vs. budesonide alone. N Engl J Med. 2016;375(9):850–860. | ||
Stempel DA, Raphiou IH, Kral KM, et al. Serious asthma events with fluticasone plus salmeterol versus fluticasone alone. N Engl J Med. 2016;374(19):1822–1830. | ||
Stempel DA, Szefler SJ, Pedersen S, et al. Safety of adding salmeterol to fluticasone propionate in children with asthma. N Engl J Med. 2016;375(9):840–849. | ||
Bush A, Frey U. Safety of long-acting beta-agonists in children with asthma. N Engl J Med. 2016;375(9):889–891. | ||
Syed YY. Fluticasone furoate/vilanterol: a review of its use in patients with asthma. Drugs. 2015;75(4):407–418. | ||
Allen A, Bareille PJ, Rousell VM. Fluticasone furoate, a novel inhaled corticosteroid, demonstrates prolonged lung absorption kinetics in man compared with inhaled fluticasone propionate. Clin Pharmacokinet. 2013;52(1):37–42. | ||
Woodcock A, Bateman ED, Busse WW, et al. Efficacy in asthma of once-daily treatment with fluticasone furoate: a randomized, placebo-controlled trial. Respir Res. 2011;12:132. | ||
Kempsford RD, Bal J, Baines A, Renaux J, Ravindranath R, Thomas PS. The efficacy of fluticasone furoate administered in the morning or evening is comparable in patients with persistent asthma. Respir Med. 2016;112:18–24. | ||
Woodcock A, Lotvall J, Busse WW, et al. Efficacy and safety of fluticasone furoate 100 mug and 200 mug once daily in the treatment of moderate-severe asthma in adults and adolescents: a 24-week randomised study. BMC Pulm Med. 2014;14:113. | ||
Lee LA, Yang S, Kerwin E, Trivedi R, Edwards LD, Pascoe S. The effect of fluticasone furoate/umeclidinium in adult patients with asthma: a randomized, dose-ranging study. Respir Med. 2015;109(1):54–62. | ||
Yang S, Lee L, Mallett S, Ayer J, Wolstenholme A, Pascoe S. A randomized, crossover study to investigate the pharmacokinetics and safety of inhaled fluticasone furoate and umeclidinium, administered separately and in combination via dry powder inhaler in healthy adult volunteers. Adv Ther. 2015;32(2):157–171. | ||
Aparici M, Gavalda A, Ramos I, et al. In vitro and in vivo preclinical profile of abediterol (LAS100977), an inhaled long-acting beta2-adrenoceptor agonist, compared with indacaterol, olodaterol and vilanterol. Eur J Pharmacol. 2016;770:61–69. | ||
Kempsford R, Norris V, Siederer S. Vilanterol trifenatate, a novel inhaled long-acting beta2 adrenoceptor agonist, is well tolerated in healthy subjects and demonstrates prolonged bronchodilation in subjects with asthma and COPD. Pulm Pharmacol Ther. 2013;26(2):256–264. | ||
Lötvall J, Bateman ED, Bleecker ER, et al. 24-h duration of the novel LABA vilanterol trifenatate in asthma patients treated with inhaled corticosteroids. Eur Respir J. 2012;40(3):570–579. | ||
Sterling R, Lim J, Frith L, Snowise NG, Jacques L, Haumann B. Efficacy and optimal dosing interval of the long-acting beta(2) agonist, vilanterol, in persistent asthma: a randomised trial. Respir Med. 2012;106(8):1110–1115. | ||
Oliver AJ, Covar RA, Goldfrad CH, et al. Randomised trial of once-daily vilanterol in children with asthma on inhaled corticosteroid therapy. Respir Res. 2016;17:37. | ||
Lötvall J, Bateman ED, Busse WW, et al. Comparison of vilanterol, a novel long-acting beta2 agonist, with placebo and a salmeterol reference arm in asthma uncontrolled by inhaled corticosteroids. J Negat Results Biomed. 2014;13(1):9. | ||
Chen X, Zheng X, Jiang J, et al. Pharmacodynamics and pharmacokinetics of fluticasone furoate/vilanterol in healthy Chinese subjects. Pharmacotherapy. 2015;35(6):586–599. | ||
Nakahara N, Wakamatsu A, Kempsford R, et al. The safety, pharmacokinetics and pharmacodynamics of a combination of fluticasone furoate and vilanterol in healthy Japanese subjects. Int J Clin Pharmacol Ther. 2013;51(8):660–671. | ||
Kempsford R, Allen A, Bal J, Rubin D, Tombs L. The effect of ketoconazole on the pharmacokinetics and pharmacodynamics of inhaled fluticasone furoate and vilanterol trifenatate in healthy subjects. Br J Clin Pharmacol. 2013;75(6):1478–1487. | ||
Allen A, Davis A, Hardes K, Tombs L, Kempsford R. Influence of renal and hepatic impairment on the pharmacokinetic and pharmacodynamic properties and tolerability of fluticasone furoate and vilanterol in combination. Clin Ther. 2012;34(12):2316–2332. | ||
Oliver A, Bjermer L, Quinn D, et al. Modulation of allergen-induced bronchoconstriction by fluticasone furoate and vilanterol alone or in combination. Allergy. 2013;68(9):1136–1142. | ||
Hughes SC, Shardlow PC, Hollis FJ, et al. Metabolism and disposition of fluticasone furoate, an enhanced-affinity glucocorticoid, in humans. Drug Metab Dispos. 2008;36(11):2337–2344. | ||
Harrell AW, Siederer SK, Bal J, et al. Metabolism and disposition of vilanterol, a long-acting beta(2)-adrenoceptor agonist for inhalation use in humans. Drug Metab Dispos. 2013;41(1):89–100. | ||
Bernstein DI, Bateman ED, Woodcock A, et al. Fluticasone furoate (FF)/vilanterol (100/25 mcg or 200/25 mcg) or FF (100 mcg) in persistent asthma. J Asthma. 2015;52(10):1073–1083. | ||
Bleecker ER, Lotvall J, O’Byrne PM, et al. Fluticasone furoate-vilanterol 100-25 mcg compared with fluticasone furoate 100 mcg in asthma: a randomized trial. J Allergy Clin Immunol Pract. 2014;2(5):553–561. | ||
Bateman ED, O’Byrne PM, Busse WW, et al. Once-daily fluticasone furoate (FF)/vilanterol reduces risk of severe exacerbations in asthma versus FF alone. Thorax. 2014;69(4):312–319. | ||
O’Byrne PM, Bleecker ER, Bateman ED, et al. Once-daily fluticasone furoate alone or combined with vilanterol in persistent asthma. Eur Respir J. 2014;43(3):773–782. | ||
Oliver A, VanBuren S, Allen A, et al. Tolerability of fluticasone furoate/vilanterol combination therapy in children aged 5 to 11 years with persistent asthma. Clin Ther. 2014;36(6):928e921–939e921. | ||
Busse WW, O’Byrne PM, Bleecker ER, et al. Safety and tolerability of the novel inhaled corticosteroid fluticasone furoate in combination with the beta2 agonist vilanterol administered once daily for 52 weeks in patients >=12 years old with asthma: a randomised trial. Thorax. 2013;68(6):513–520. | ||
Kempsford RD, Oliver A, Bal J, Tombs L, Quinn D. The efficacy of once-daily fluticasone furoate/vilanterol in asthma is comparable with morning or evening dosing. Respir Med. 2013;107(12):1873–1880. | ||
Woodcock A, Bleecker ER, Lotvall J, et al. Efficacy and safety of fluticasone furoate/vilanterol compared with fluticasone propionate/salmeterol combination in adult and adolescent patients with persistent asthma: a randomized trial. Chest. 2013;144(4):1222–1229. | ||
Lin J, Tang H, Chen P, et al. Efficacy and safety evaluation of once-daily fluticasone furoate/vilanterol in Asian patients with asthma uncontrolled on a low- to mid-strength inhaled corticosteroid or low-dose inhaled corticosteroid/long-acting beta2-agonist. Allergy Asthma Proc. 2016;37(4):302–310. | ||
Lin J, Kang J, Lee SH, et al. Fluticasone furoate/vilanterol 200/25 mcg in Asian asthma patients: a randomized trial. Respir Med. 2015;109(1):44–53. | ||
Dal Negro RW, Distante C, Bonadiman L, Turco P, Iannazzo S. Fluticasone furoate/vilanterol 92/22 mug once-a-day vs beclomethasone dipropionate/formoterol 100/6 mug b.i.d.: a 12-week cost analysis in mild-to-moderate asthma. Multidiscip Respir Med. 2016;11:20. | ||
Hozawa S, Terada M, Haruta Y, Hozawa M. Comparison of early effects of budesonide/formoterol maintenance and reliever therapy with fluticasone furoate/vilanterol for asthma patients requiring step-up from inhaled corticosteroid monotherapy. Pulm Pharmacol Ther. 2016;37:15–23. | ||
Louie S, Zeki AA, Schivo M, et al. The asthma-chronic obstructive pulmonary disease overlap syndrome: pharmacotherapeutic considerations. Expert Rev Clin Pharmacol. 2013;6(2):197–219. | ||
Ishiura Y, Fujimura M, Shiba Y, Ohkura N, Hara J, Kasahara K. A comparison of the efficacy of once-daily fluticasone furoate/vilanterol with twice-daily fluticasone propionate/salmeterol in asthma-COPD overlap syndrome. Pulm Pharmacol Ther. 2015;35:28–33. | ||
Woodcock A, Bakerly ND, New JP, et al. The Salford Lung Study protocol: a pragmatic, randomised phase III real-world effectiveness trial in asthma. BMC Pulm Med. 2015;15:160. | ||
Gross AS, Goldfrad C, Hozawa S, et al. Ethnic sensitivity assessment of fluticasone furoate/vilanterol in East Asian asthma patients from randomized double-blind multicentre phase IIb/III trials. BMC Pulm Med. 2015;15:165. | ||
Rodrigo GJ, Plaza V. Once-daily fluticasone furoate and vilanterol for adolescents and adults with symptomatic asthma: a systematic review with meta-analysis. Ann Allergy Asthma Immunol. 2016;116(6):565–570. | ||
Ingersoll KS, Cohen J. The impact of medication regimen factors on adherence to chronic treatment: a review of literature. J Behav Med. 2008;31(3):213–224. | ||
Coleman CI, Limone B, Sobieraj DM, et al. Dosing frequency and medication adherence in chronic disease. J Manag Care Pharm. 2012;18(7):527–539. | ||
Lindsay JT, Heaney LG. Non-adherence in difficult asthma and advances in detection. Expert Rev Respir Med. 2013;7(6):607–614. | ||
Fischer J, Wimmer A, Mahlich J. [Medication adherence in asthma therapy – a structured review]. Pneumologie. 2013;67(7):406–414. | ||
Lindsay JT, Heaney LG. Nonadherence in difficult asthma – facts, myths, and a time to act. Patient Prefer Adherence. 2013;7:329–336. | ||
Bender B, Milgrom H, Rand C. Nonadherence in asthmatic patients: is there a solution to the problem? Ann Allergy Asthma Immunol. 1997;79(3):177–185; quiz185–176. | ||
Bender B, Milgrom H, Apter A. Adherence intervention research: what have we learned and what do we do next? J Allergy Clin Immunol. 2003;112(3):489–494. | ||
Feehan M, Ranker L, Durante R, et al. Adherence to controller asthma medications: 6-month prevalence across a US community pharmacy chain. J Clin Pharm Ther. Epub 2015 Aug 20. | ||
McNally KA, Rohan J, Schluchter M, et al. Adherence to combined montelukast and fluticasone treatment in economically disadvantaged African American youth with asthma. J Asthma. 2009;46(9):921–927. | ||
Shams MR, Fineman SM. Asthma adherence: how can we help our patients do it better? Ann Allergy Asthma Immunol. 2014;112(1):9–12. | ||
Heaney LG, Horne R. Non-adherence in difficult asthma: time to take it seriously. Thorax. 2012;67(3):268–270. | ||
Komase Y, Asako A, Kobayashi A, Sharma R. Ease-of-use preference for the ELLIPTA(R) dry powder inhaler over a commonly used single-dose capsule dry powder inhaler by inhalation device-naive Japanese volunteers aged 40 years or older. Int J Chron Obstruct Pulmon Dis. 2014;9:1365–1375. | ||
Svedsater H, Dale P, Garrill K, Walker R, Woepse MW. Qualitative assessment of attributes and ease of use of the ELLIPTA dry powder inhaler for delivery of maintenance therapy for asthma and COPD. BMC Pulm Med. 2013;13:72. | ||
Yun Kirby S, Zhu CQ, Kerwin EM, Stanford RH, Georges G. A preference study of two placebo dry powder inhalers in adults with COPD: ELLIPTA(R) dry powder inhaler (DPI) versus DISKUS(R) DPI. COPD. 2016;13(2):167–175. | ||
Brealey N, Gupta A, Renaux J, Mehta R, Allen A, Henderson A. Pharmacokinetics of fluticasone furoate, umeclidinium, and vilanterol as a triple therapy in healthy volunteers. Int J Clin Pharmacol Ther. 2015;53(9):753–764. | ||
Bateman ED, Bleecker ER, Lotvall J, et al. Dose effect of once-daily fluticasone furoate in persistent asthma: a randomized trial. Respir Med. 2012;106(5):642–650. | ||
Lötvall J, Bleecker ER, Busse WW, et al. Efficacy and safety of fluticasone furoate 100 mug once-daily in patients with persistent asthma: a 24-week placebo and active-controlled randomised trial. Respir Med. 2014;108(1):41–49. | ||
Busse WW, Bateman ED, O’Byrne PM, et al. Once-daily fluticasone furoate 50 mcg in mild-to-moderate asthma: a 24-week placebo-controlled randomized trial. Allergy. 2014;69(11):1522–1530. | ||
O’Byrne PM, Woodcock A, Bleecker ER, et al. Efficacy and safety of once-daily fluticasone furoate 50 mcg in adults with persistent asthma: a 12-week randomized trial. Respir Res. 2014;15:88. | ||
Woodcock A, Bleecker ER, Busse WW, et al. Fluticasone furoate: once-daily evening treatment versus twice-daily treatment in moderate asthma. Respir Res. 2011;12:160. | ||
Medley H, Orozco S, Allen A. Efficacy and safety profile of fluticasone furoate administered once daily in the morning or evening: a randomized, double-blind, double-dummy, placebo-controlled trial in adult and adolescent patients with persistent bronchial asthma. Clin Ther. 2012;34(8):1683–1695. | ||
Busse WW, Bleecker ER, Bateman ED, et al. Fluticasone furoate demonstrates efficacy in patients with asthma symptomatic on medium doses of inhaled corticosteroid therapy: an 8-week, randomised, placebo-controlled trial. Thorax. 2012;67(1):35–41. | ||
Bleecker ER, Bateman ED, Busse WW, et al. Once-daily fluticasone furoate is efficacious in patients with symptomatic asthma on low-dose inhaled corticosteroids. Ann Allergy Asthma Immunol. 2012;109(5):353e354–358e354. | ||
van den Berge M, Luijk B, Bareille P, Dallow N, Postma DS, Lammers JW. Prolonged protection of the new inhaled corticosteroid fluticasone furoate against AMP hyperresponsiveness in patients with asthma. Allergy. 2010;65(12):1531–1535. | ||
Allen A, Bal J, Cheesbrough A, Hamilton M, Kempsford R. Pharmacokinetics and pharmacodynamics of intravenous and inhaled fluticasone furoate in healthy Caucasian and East Asian subjects. Br J Clin Pharmacol. 2014;77(5):808–820. | ||
Oliver A, VanBuren S, Allen A, et al. Safety, tolerability, pharmacokinetics, and pharmacodynamics of vilanterol, a novel inhaled long-acting beta-agonist, in children aged 5–11 years with persistent asthma: a randomized trial. Clin Pharmacol Drug Dev. 2014;3(3):215–221. | ||
Allen RA, Wu W, Yao M, et al. Nerve regeneration and elastin formation within poly(glycerol sebacate)-based synthetic arterial grafts one-year post-implantation in a rat model. Biomaterials. 2014;35(1):165–173. | ||
Calzetta L, Rinaldi B, Cazzola M, Matera MG. Pharmacodynamic and pharmacokinetic assessment of fluticasone furoate + vilanterol for the treatment of asthma. Expert Opin Drug Metab Toxicol. 2016;12(7):813–822. | ||
Allen A, Schenkenberger I, Trivedi R, et al. Inhaled fluticasone furoate/vilanterol does not affect hypothalamic-pituitary-adrenal axis function in adolescent and adult asthma: randomised, double-blind, placebo-controlled study. Clin Respir J. 2013;7(4):397–406. | ||
Oliver A, Quinn D, Goldfrad C, van Hecke B, Ayer J, Boyce M. Combined fluticasone furoate/vilanterol reduces decline in lung function following inhaled allergen 23 h after dosing in adult asthma: a randomised, controlled trial. Clin Transl Allergy. 2012;2(1):11. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.