")
Back to Journals » Drug Design, Development and Therapy » Volume 11
Sodium-glucose cotransporter 2 inhibitors combined with dipeptidyl peptidase-4 inhibitors in the management of type 2 diabetes: a review of current clinical evidence and rationale
Received 8 September 2016
Accepted for publication 19 January 2017
Published 21 March 2017 Volume 2017:11 Pages 923—937
DOI https://doi.org/10.2147/DDDT.S121899
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jianbo Sun
Sayf A Yassin,1 Vanita R Aroda2
1MedStar Union Memorial Hospital, Baltimore, 2MedStar Health Research Institute, Hyattsville, MD, USA
Abstract: Type 2 diabetes mellitus (T2DM) is a progressive and multifactorial cardiometabolic disorder. Almost half of adults with diabetes fail to achieve their recommended glucose control target. This has prompted some clinicians to advocate the use of more intensive initial therapy, including the use of combination therapy to target multiple physiologic defects in diabetes with the goal of achieving and sustaining glucose control. Numerous options exist for combining the various classes of glucose-lowering agents in the treatment of T2DM. This report reviews the mechanism, rationale, and evidence from clinical trials for combining two of the newer drug classes, namely, dipeptidyl peptidase-4 inhibitors and sodium-glucose cotransporter 2 inhibitors, and considers the possible role of such dual therapy in the management of T2DM.
Keywords: sodium-glucose cotransporter 2 inhibitors, dipeptidyl peptidase-4 inhibitors, type 2 diabetes mellitus, combination therapy
Introduction
Type 2 diabetes mellitus (T2DM) is a progressive, multifactorial metabolic and cardiovascular disorder characterized by multiple pathophysiologic abnormalities (exemplified by the “Ominous Octet”).1–3 Almost half of adults with diabetes do not achieve the recommended glucose control targets.4 This has prompted some clinicians to consider more aggressive initial therapy, including the initial use of combination therapy.1,5 DeFronzo and colleagues have proposed the early initiation of combination therapy in the treatment of T2DM, using agents that correct the associated pathophysiologic abnormalities to produce a sustained reduction in glycated hemoglobin (HbA1c).1 They further suggested that medications and treatment approaches in T2DM should preserve or improve pancreatic β-cell function, reduce insulin resistance in muscle and liver, have a beneficial effect on cardiovascular risk factors, be weight neutral/promote weight loss, and be safe to use.1 Drug classes selected for use in combination should have complementary mechanisms of action,1,5 which may prevent the occurrence of compensatory mechanisms and may maximize the chances of additive effects in achieving and maintaining HbA1c goals.6 The potential use of initial combination therapy is recognized in the current standards of care for diabetes, but the guidance is directed at those with more severe hyperglycemia.5 The American Diabetes Association/European Association for the Study of Diabetes recommend that initial combination therapy should be considered for patients with baseline HbA1c ≥9%.3,7 The American Association of Clinical Endocrinologists/American College of Endocrinology recommend initial dual therapy for patients with HbA1c ≥7.5%, and dual or triple combination therapy for individuals with HbA1c >9%, if presenting without significant symptoms.8 Nevertheless, both treatment algorithms describe the need to individualize HbA1c targets and the choice of therapies, based on each patient’s clinical attributes and preferences.3,7,8
Numerous options exist for combining the various classes of glucose-lowering agents in the treatment of T2DM. This report examines the mechanism, rationale, and evidence from Phase III clinical trials for combining two of the newer drug classes in the treatment of T2DM, namely, dipeptidyl peptidase-4 (DPP-4) inhibitors and sodium-glucose cotransporter 2 (SGLT2) inhibitors, and considers the possible role of such therapy in the management of T2DM. Of note, the scope of this review does not include examination of the sequence in which the various classes of glucose-lowering medication are used, nor does it compare combination vs stepwise therapy, but rather explores in detail the current evidence and data available for the combination of SGLT2 and DPP-4 inhibitors in the treatment of T2DM.
Summary of mechanisms, efficacy, and safety
DPP-4 inhibitors
DPP-4 inhibitors prevent the enzymatic degradation of endogenous incretin hormones (active glucagon-like peptide [GLP]-1 and glucose-dependent insulinotropic polypeptide [GIP]).9,10 Increased plasma concentrations of GLP-1 and GIP stimulate insulin secretion from pancreatic β-cells and inhibit glucagon secretion from pancreatic α-cells, which causes inhibition of endogenous glucose production and a reduction in plasma glucose concentration.11 DPP-4 inhibitors first gained US regulatory approval for use in T2DM in 2006, with sitagliptin as the first-in-class.12 Other US-approved DPP-4 inhibitors are saxagliptin, linagliptin, and alogliptin, and four additional “gliptins” are available in other parts of the world.13 DPP-4 inhibitors are a heterogeneous group, differing in their chemical structure (not shown) and pharmacokinetic properties (Table 1).12,14–19 As a class, DPP-4 inhibitors have been shown to improve glycemic control in patients with T2DM when given as monotherapy or in combination therapy, with no increased risk of weight gain or hypoglycemia13 (when used without insulin secretagogues or insulin).16–19 DPP-4 inhibitor monotherapy reduced HbA1c by 0.6%–0.7% when compared with placebo in randomized controlled trials (RCTs; Table 2),20–23 and comparable efficacy was observed in RCTs of DPP-4 inhibitors in combination with other glucose-lowering agents.24 DPP-4 inhibitors are virtually weight neutral,12 and exert modest blood pressure (BP)-lowering effects compared with placebo or nontreatment (mean difference in systolic BP −3 mmHg).25 DPP-4 inhibitors are generally safe and well tolerated.26,27 There have been postmarketing reports of acute pancreatitis in patients receiving DPP-4 inhibitors;27 per the labeling information, these agents should be discontinued if pancreatitis is suspected.16–19 Postmarketing cardiovascular outcomes trials in patients receiving saxagliptin,28 alogliptin,29 and sitagliptin30 produced conflicting results regarding the risk of hospitalization for heart failure associated with DPP-4 inhibitors31 (cardiovascular outcomes trials for linagliptin are currently ongoing). A recent systematic review and meta-analysis of 43 randomized trials and 12 observational studies of DPP-4 inhibitors concluded that the effect of these agents on the risk of heart failure was uncertain,32 and there was a small increased risk of hospital admission for heart failure in T2DM patients with existing cardiovascular disease or multiple risk factors for vascular disease who were receiving DPP-4 inhibitors, relative to no use (pooled odds ratio: 1.13; 95% confidence interval [CI] 1.00, 1.26).32 The labels for saxagliptin17 and alogliptin19 contain warning information on the use of these agents in patients at risk of heart failure.
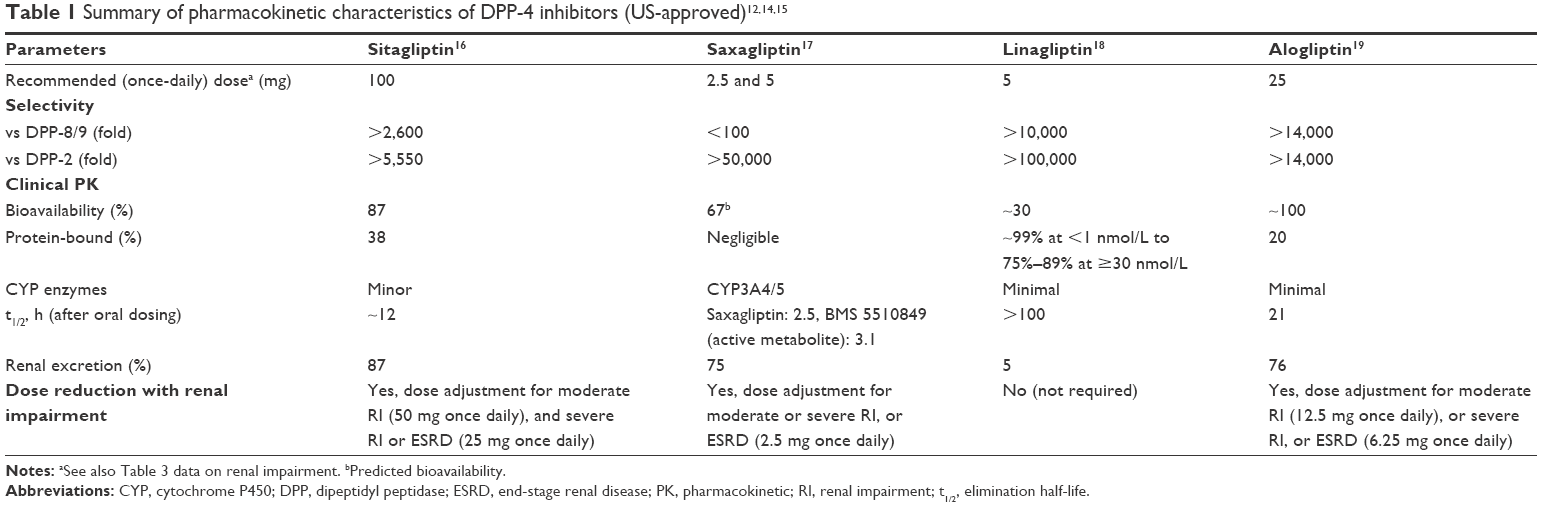 | Table 1 Summary of pharmacokinetic characteristics of DPP-4 inhibitors (US-approved)12,14,15 |
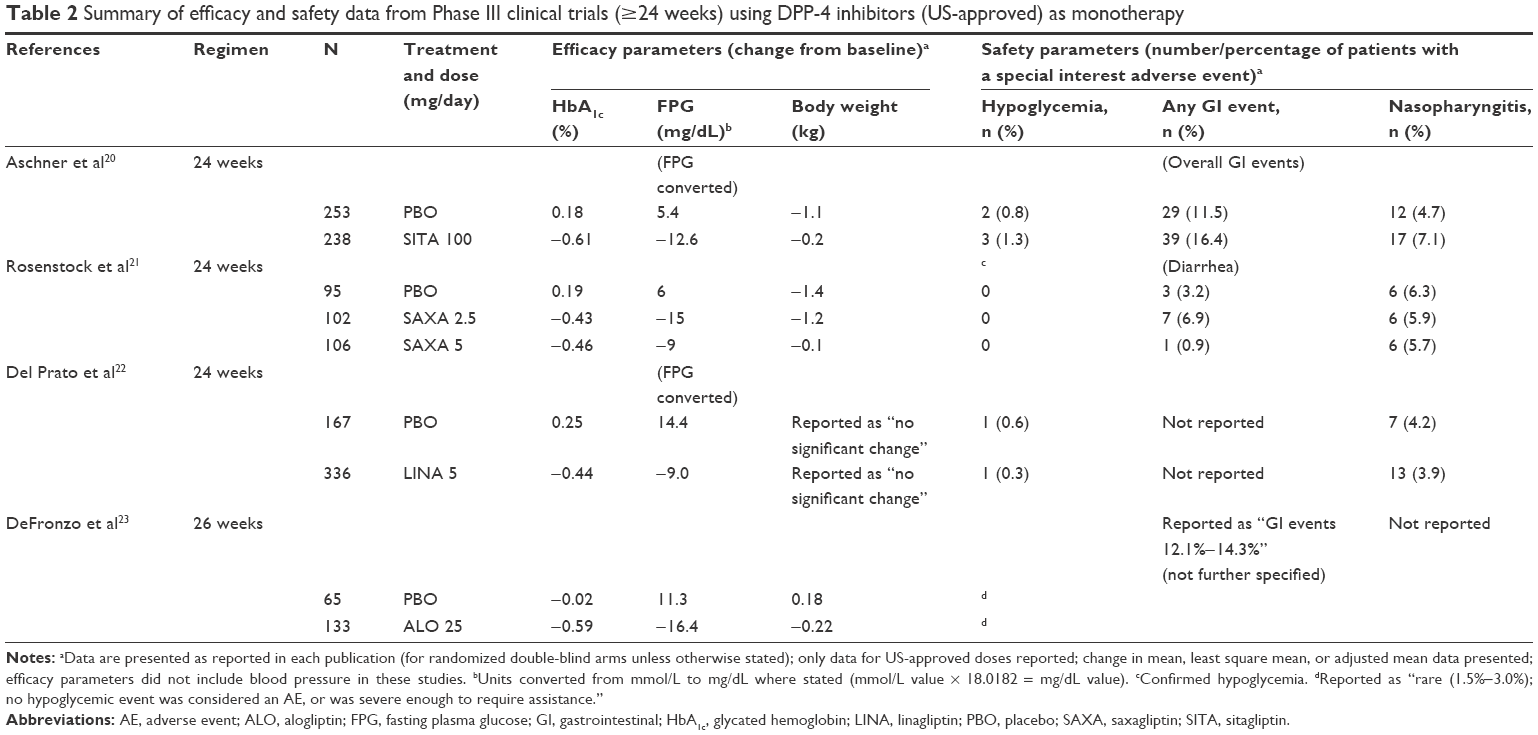 | Table 2 Summary of efficacy and safety data from Phase III clinical trials (≥24 weeks) using DPP-4 inhibitors (US-approved) as monotherapy |
SGLT2 inhibitors
SGLT2 inhibitors suppress renal glucose reabsorption and promote urinary glucose excretion (UGE), which decreases hyperglycemia.33 SGLT2 inhibitors act independently of pancreatic β-cell function and the degree of insulin resistance.33,34 In 2013, canagliflozin became the first SGLT2 inhibitor to receive US regulatory approval for use in T2DM, and was followed by US approvals for dapagliflozin and empagliflozin in 2014.35 Canagliflozin, dapagliflozin, and empagliflozin are based on a C-glucoside structure (not shown),36 and have comparable pharmacokinetic properties in terms of excellent oral bioavailability, a long half-life allowing once-daily administration, and an absence of active metabolites (Table 3).37–44 However, differences are present in their respective selectivity for SGLT2 over SGLT1,44 and regarding dosing recommendations for patients with T2DM and renal impairment (Table 3).38–44 Data from RCTs in patients with T2DM demonstrated that SGLT2 inhibitor monotherapy reduced HbA1c by 0.5%–1.0% compared with placebo, and was associated with reductions in body weight of ~2 kg and in systolic BP of 2–5 mmHg (Table 4).45–50 Greater reductions in HbA1c (2%–3%) were reported in patients with higher baseline levels of HbA1c (ie, >10.0%) receiving SGLT2 inhibitor therapy.48–50 SGLT2 inhibitors have a generally favorable safety profile.45–47 These agents are not associated with an increased risk of hypoglycemia, unless combined with insulin secretagogues or insulin.45–47 However, SGLT2 inhibitors are associated with an increased risk of genital mycotic infections51–54 and urinary tract infection (UTI).51,54–56 Furthermore, the UGE-associated osmotic diuresis observed with SGLT2 inhibitors could potentially increase the risk of volume depletion events (eg, hypotension) in susceptible patients.41–43 More recently, postmarketing cases of urosepsis and pyelonephritis, and diabetic ketoacidosis (DKA) associated with SGLT2 inhibitor therapy have been reported.57 Some cases of DKA in T2DM patients were euglycemic.58–60 Other cases of DKA were associated with off-label use of SGLT2 inhibitors in patients with type 1 diabetes mellitus.58,61,62 SGLT2 inhibitor clinical trials reported low frequencies of DKA in T2DM: canagliflozin events by treatment group were 0.07% (4/5,337), 0.11% (6/5,350), and 0.03% (2/6,909) for 100 mg, 300 mg, and comparator, respectively;63 dapagliflozin events were <0.1% in >18,000 patients (no further details stated);64 and DKA events with empagliflozin by treatment group were 2 events for 10 mg and 1 event for 25 mg, vs 5 events for placebo (N>13,000 T2DM patients; treatment group sizes not stated).64 It has been postulated that euglycemic DKA associated with SGLT2 inhibitor use in T2DM may result from reduced plasma glucose concentrations caused by SGLT2 inhibitor-induced UGE, which predisposes to increased ketogenesis.64
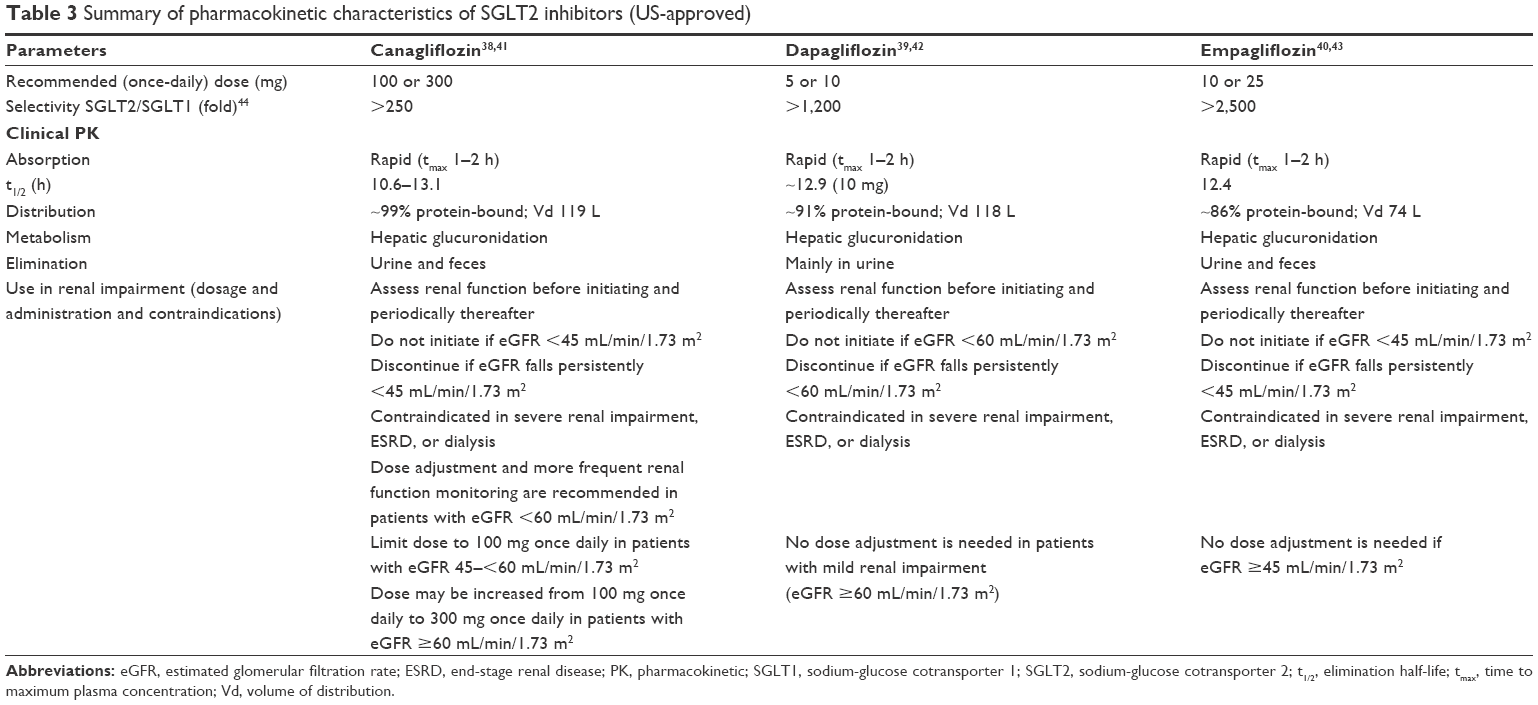 | Table 3 Summary of pharmacokinetic characteristics of SGLT2 inhibitors (US-approved) |
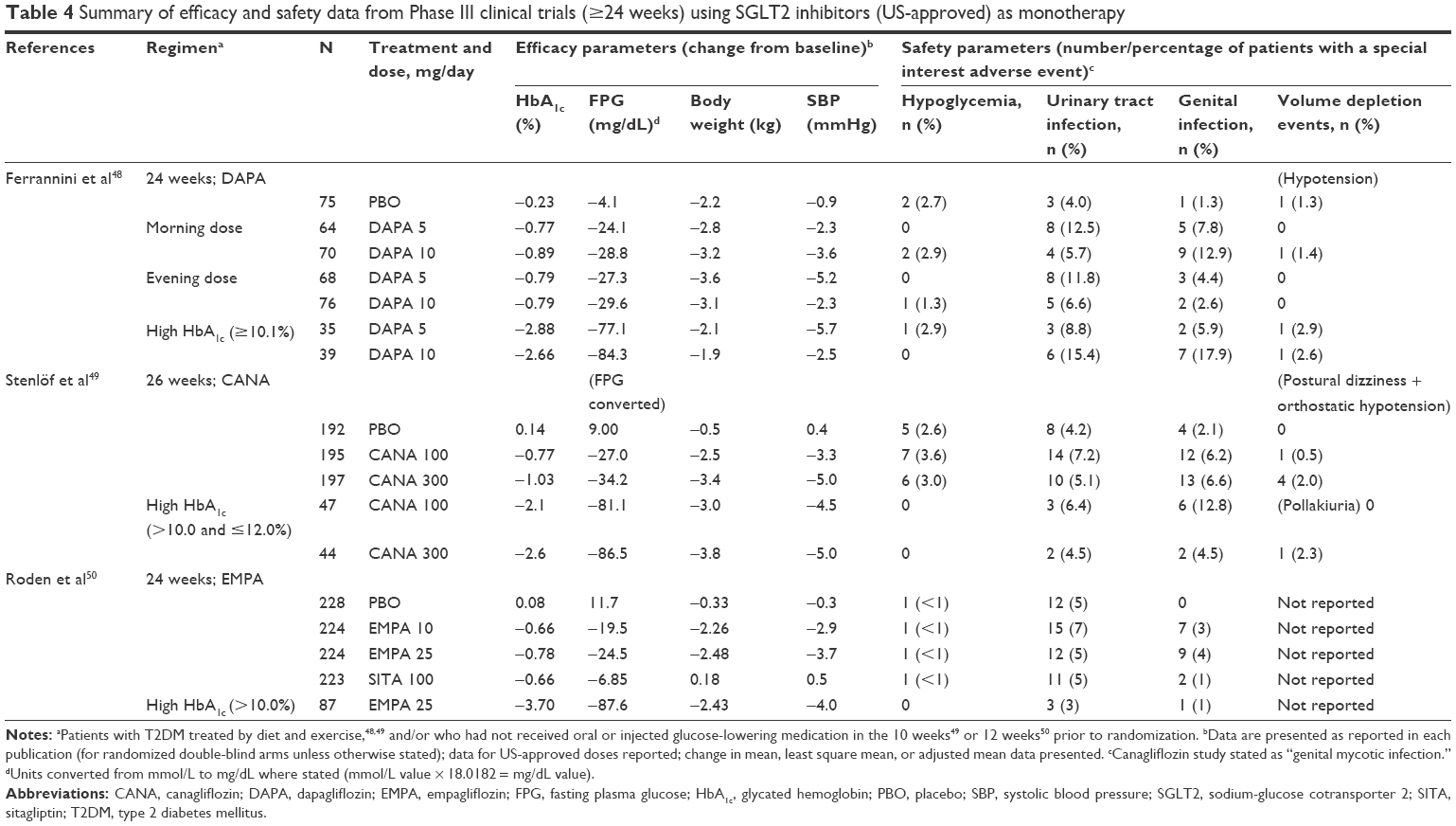 | Table 4 Summary of efficacy and safety data from Phase III clinical trials (≥24 weeks) using SGLT2 inhibitors (US-approved) as monotherapy |
Clinical evidence for combinations of DPP-4 inhibitors and SGLT2 inhibitors
Two combination formulations of DPP-4 inhibitors and SGLT2 inhibitors are currently approved in the treatment of T2DM: fixed-dose formulations of dapagliflozin plus saxagliptin (approved by the European Medicines Agency [EMA] in July 2016), and empagliflozin plus linagliptin (approved by US Food and Drug Administration in January 2015, and by EMA in November 2016). Historical rationale and clinical evidence of the combination of the two classes are now reviewed.
Early drug–drug interaction studies between SGLT2 inhibitors and other glucose-lowering agents, including the DPP-4 inhibitors sitagliptin and linagliptin, did not demonstrate any significant changes in exposure following coadministration, thus indicating that DPP-4 inhibitors and SGLT2 inhibitors could be coadministered without the need for dose adjustments and without any significant drug interaction.65–67 Clinical data from RCTs using DPP-4 inhibitor plus SGLT2 inhibitor combination therapy in patients with T2DM by background therapy and treatment sequence are shown in Table 568–75 and are discussed below. Studies for inclusion were selected on the basis of being Phase III RCTs of at least 24 weeks’ duration; post hoc analyses were excluded.
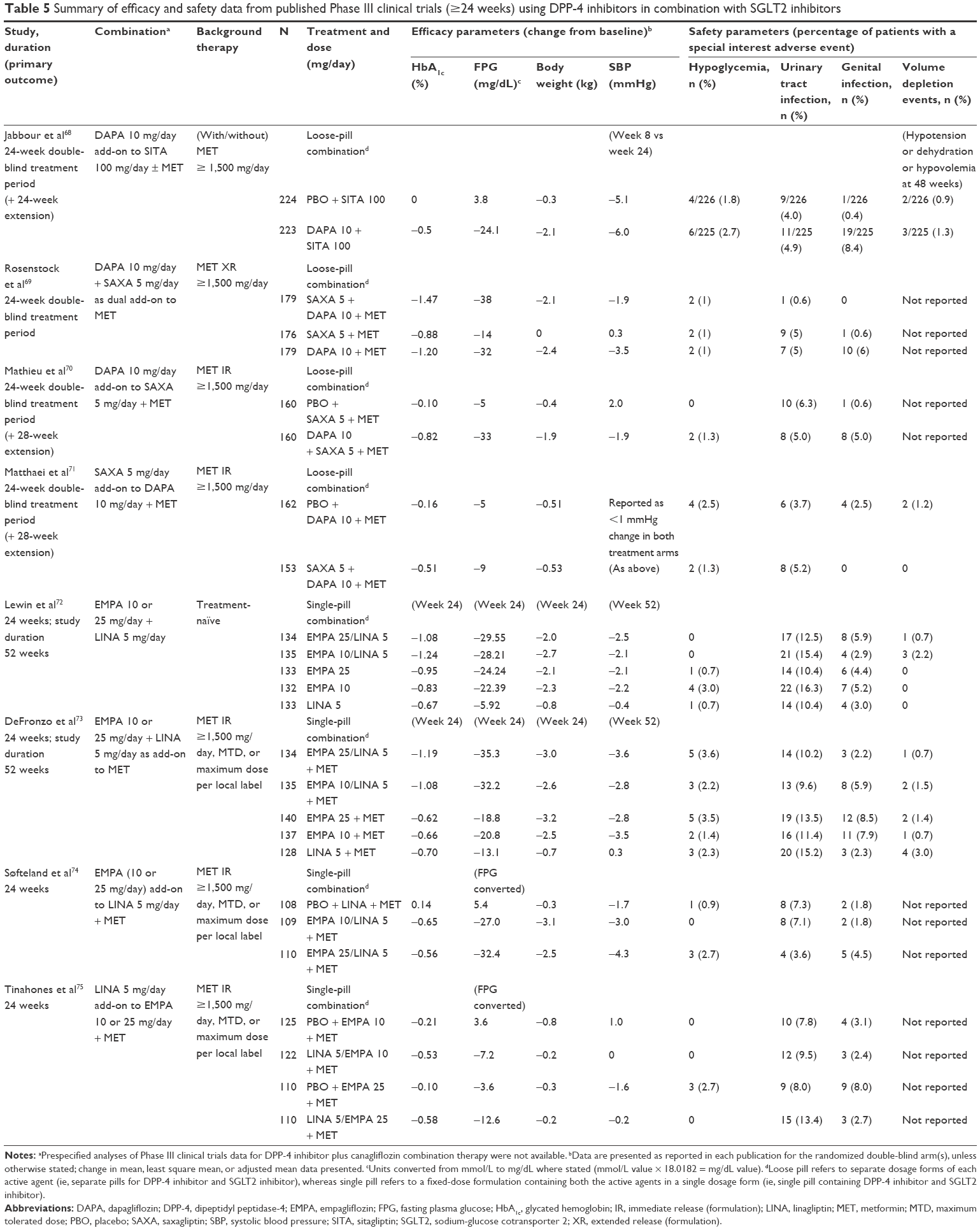 | Table 5 Summary of efficacy and safety data from published Phase III clinical trials (≥24 weeks) using DPP-4 inhibitors in combination with SGLT2 inhibitors |
In a 24-week, randomized, placebo-controlled study (N=432) of dapagliflozin (10 mg/day) or placebo added to sitagliptin (100 mg/day), given with/without metformin (≥1,500 mg/day),68 dapagliflozin significantly reduced mean HbA1c vs placebo (placebo-corrected change from baseline to week 24: −0.5%; 95% CI −0.6, −0.3; P<0.0001).68 The HbA1c reduction was greater in patients with baseline levels ≥8% (placebo-corrected change from baseline to week 24: −0.8%; 95% CI −1.1, −0.6; P<0.0001).68 A similar trend was observed for dapagliflozin vs placebo, respectively, for fasting plasma glucose (FPG) (−24.1 vs +3.8 mg/dL) and body weight (−2.1 vs −0.3 kg); however, changes in systolic BP were not significantly different between groups (−6.0 vs −5.1 mmHg).68 Adverse events were balanced between groups and discontinuation rates were low.68 A similar number of patients in both groups reported hypoglycemic events at week 24 (dapagliflozin: 6/225, 2.7%; placebo 4/226, 1.8%), and none of these events led to treatment discontinuation.68 At week 24, the rate of UTI was balanced between groups (~4%–5%), but genital infection was more common with dapagliflozin vs placebo (8.4% vs 0.4%, respectively), and one patient (dapagliflozin group) discontinued treatment due to vulvovaginal mycotic infection.68 Both UTI and genital infection events occurred more frequently in female patients. Volume depletion events were reported for the 24-week extension period (ie, at week 48), and occurred in low numbers in both treatment groups (dapagliflozin: 3/225, 1.3%; placebo 2/226, 0.9%).68
In a randomized, placebo-controlled study where dapagliflozin (10 mg/day) was added to saxagliptin (5 mg/day) – that is, as dual add-on therapy vs each agent administered alone (N=534), all on a background of metformin therapy (extended-release formulation, 1,500–2,000 mg/day), patients receiving dapagliflozin plus saxagliptin demonstrated greater improvements in glycemic control (ie, HbA1c and FPG) at week 24 than those receiving either dapagliflozin or saxagliptin (Table 5).69 Furthermore, 41% of patients achieved HbA1c <7% with dapagliflozin plus saxagliptin vs 18% and 22% with saxagliptin or dapagliflozin, respectively.69 As noted in a separate report of these study data by Abdul-Ghani,6 when patients were stratified by their baseline HbA1c, for the subgroup of patients with baseline HbA1c ≥9% (n=190; mean HbA1c ~10%), the mean change in HbA1c was similar for the dapagliflozin plus saxagliptin group and the dapagliflozin group (−2.03% and −1.87%, respectively), whereas the contribution of saxagliptin was lower (−1.32%).6,69 In addition, higher baseline HbA1c levels were associated with proportionally larger changes in HbA1c following dapagliflozin therapy (eg, increasing baseline mean HbA1c from ~7.5% to ~10% was associated with the following changes in HbA1c at treatment end: dapagliflozin group, −0.45% vs −1.87% [greater than fourfold change]; dapagliflozin plus saxagliptin group, −0.80% vs −2.03% [greater than twofold change]; saxagliptin group, −0.69% vs −1.32% [less than twofold change]).6,69 Mean reductions in systolic BP and body weight only occurred in the dapagliflozin plus saxagliptin group and the dapagliflozin group (systolic BP: reductions of 1.9 and 3.5 mmHg, respectively; and body weight: reductions of 2.1 and 2.4 kg, respectively), with no reduction in either parameter in the saxagliptin group.69 Thus, an SGLT2 inhibitor given as an add-on to metformin or in combination with saxagliptin plus metformin appears to contribute to both body weight and BP-lowering potential. The proportion of adverse events was similar across treatment groups. Hypoglycemia events occurred in 1% of each group, and there were no major hypoglycemic events.69 UTI occurred in ≤1% of patients receiving dapagliflozin plus saxagliptin vs in 5% of patients receiving dapagliflozin or saxagliptin. However, genital infection events were more common in the dapagliflozin group (6%) vs the saxagliptin group (0.6%) and, interestingly, were not reported in the dapagliflozin plus saxagliptin group (0%).69
Two further RCTs investigated the triple combination therapy of dapagliflozin plus saxagliptin plus metformin. In the first study, patients (N=320) received open-label treatment with saxagliptin (5 mg/day) and metformin (immediate-release formulation, ≥1,500 mg/day) for 16 weeks before being randomized to a 24-week, double-blind treatment period and receive additional treatment with dapagliflozin (10 mg/day) or placebo.70 The second study (N=315) followed a similar design and drug dosing, but with saxagliptin (or placebo) added to dapagliflozin and metformin.71 The results from both studies showed a comparable trend to those reported above in the dual add-on study, with greater reductions in HbA1c and FPG at week 24 occurring in patients receiving dapagliflozin plus saxagliptin plus metformin (Table 5).70,71 Adverse events occurred with a similar frequency across the treatment groups in both studies, and the overall risk of hypoglycemia was low (0%–2.5%).70,71 In the add-on to saxagliptin and metformin study, genital infections occurred in 5.0% of patients receiving dapagliflozin vs 0.6% of those receiving placebo,70 whereas in the add-on to dapagliflozin and metformin study, the proportions were 0% for saxagliptin vs 2.5% for placebo.71
An RCT evaluated single-pill combinations (ie, fixed doses) of empagliflozin plus linagliptin over 52 weeks, with data reported for treatment-naïve patients,72 and for those inadequately controlled on metformin.73 Treatment-naïve patients (N=667) were randomized into five treatment groups (where all study drugs were taken once daily in the morning): empagliflozin 25 mg/linagliptin 5 mg, empagliflozin 10 mg/linagliptin 5 mg, empagliflozin 25 or 10 mg, and linagliptin 5 mg.72 The adjusted mean change from baseline in HbA1c at week 24 was significantly greater for empagliflozin 25 mg/linagliptin 5 mg compared with linagliptin 5 mg (−0.41%; 95% CI −0.61, −0.22; P<0.001) but not compared with empagliflozin 25 mg (−0.14%; 95% CI −0.33, 0.06; P=0.179), and was also significantly greater for empagliflozin 10 mg/linagliptin 5 mg than for either drug individually (−0.41%; 95% CI −0.61, −0.21; and −0.57%; 95% CI −0.76, −0.37 for empagliflozin 10 mg/linagliptin 5 mg vs empagliflozin 10 mg and linagliptin 5 mg, respectively; P<0.001 for each).72 Reductions in HbA1c with the two empagliflozin/linagliptin single-pill combinations were sustained at week 52.72 Reductions from baseline in FPG concentrations at week 24 were significantly greater for the empagliflozin/linagliptin single-pill combination therapies vs linagliptin monotherapy, but not vs empagliflozin monotherapy.72 A similar trend was reported for reductions in body weight from baseline to week 24.72 The overall proportion and intensity of adverse events were similar for all treatment groups.72 No confirmed hypoglycemic adverse events were reported in the two empagliflozin/linagliptin single-pill combination groups; however, hypoglycemia was reported in one subject in each of the empagliflozin 25-mg and linagliptin 5-mg groups, and in four subjects in the empagliflozin 10-mg group.72 UTI events were reported in 12.5%–15.4% of patients receiving empagliflozin/linagliptin single-pill combinations, in 10.4%–16.3% of patients receiving empagliflozin monotherapy, and in 10.4% of patients receiving linagliptin monotherapy, with a greater proportion occurring in female vs male patients in all treatment groups; only one patient reported an event that was severe in intensity (empagliflozin 25-mg group) but this did not lead to discontinuation of the study drug.72 Genital infection events were reported in 2.9%–5.9% of patients overall, and were reported more frequently in female than male patients in all groups except the empagliflozin 25-mg group; however, none of these events was reported to be severe, although two subjects (n=1, empagliflozin 25 mg/linagliptin 5 mg; n=1, empagliflozin 10 mg) discontinued study drug as a result of these events.72
Patients inadequately controlled on metformin (≥1,500 mg/day, maximum tolerated dose, or maximum dose per local label; N=674) were also randomized into the five treatment groups described above.73 At week 24, HbA1c levels were reduced from baseline values to a greater extent with both empagliflozin/linagliptin single-pill combination therapies than with either component alone (−0.58%; 95% CI −0.75, −0.41 for empagliflozin 25 mg/linagliptin 5 mg vs empagliflozin 25 mg; −0.50%; 95% CI −0.67, −0.32 for empagliflozin 25 mg/linagliptin 5 mg vs linagliptin 5 mg; −0.42%; 95% CI −0.59, −0.25 for empagliflozin 10 mg/linagliptin 5 mg vs empagliflozin 10 mg; −0.39%; 95% CI −0.56, −0.21 for empagliflozin 10 mg/linagliptin 5 mg vs linagliptin 5 mg; P<0.001 for each).73 A similar trend occurred for FPG concentrations.73 The significant reductions in HbA1c from baseline were maintained at 52 weeks with both empagliflozin/linagliptin single-pill combinations vs the individual components.73 Reductions in body weight from baseline to week 24 were significantly greater for both empagliflozin/linagliptin single-pill combinations compared with linagliptin alone, but not compared with empagliflozin alone,73 as was observed in the previous study.72 Similarly, the overall proportion and intensity of adverse events were similar for all treatment groups. Confirmed hypoglycemia event rates were low (1.4%–3.6%); no patients discontinued treatment due to hypoglycemia.73 UTI events were reported in 9.6%–10.2% of patients receiving empagliflozin/linagliptin single-pill combinations, in 11.4%–13.5% of patients receiving empagliflozin monotherapy, and in 15.2% of patients receiving linagliptin monotherapy, with a greater proportion of cases reported in female patients in all treatment groups. Most UTI events were mild or moderate in intensity, and only one patient discontinued study drug (empagliflozin 10 mg) due to UTI.73 Genital infection events were reported in 2.2%–8.5% of patients overall, and were more frequent among female patients in three of the treatment groups (not in empagliflozin 25 mg/linagliptin 5 mg, or linagliptin 5-mg groups).73 Two patients (empagliflozin 25-mg group) discontinued due to genital infection events.73 In addition, no patients experienced worsening of heart failure or were hospitalized for heart failure in either of these empagliflozin/linagliptin single-pill combination study populations.72,73
Results from two additional 24-week RCTs to investigate combination therapy with empagliflozin plus linagliptin were published recently; empagliflozin (10 or 25 mg/day) and linagliptin (5 mg/day) combinations were administered as single-pill formulations in both studies.74,75 One study (N=333) evaluated empagliflozin vs placebo as add-on therapy to linagliptin and metformin,74 and the second study (N=709) evaluated linagliptin vs placebo as add-on therapy to empagliflozin and metformin.75 Empagliflozin/linagliptin combination therapy (plus metformin) produced greater reductions in HbA1c and FPG from baseline than that observed with either linagliptin plus placebo (plus metformin) or empagliflozin plus placebo (plus metformin).74,75 Adverse events were more common in the placebo groups in both studies, and the incidence of confirmed hypoglycemic adverse events was low in both studies and across all treatment groups (0%–2.7%).74,75 In the empagliflozin as add-on study, the incidence of events consistent with genital infection was low in all treatment groups, but was higher in patients treated with combination therapy containing empagliflozin 25 mg than in those treated with either combination therapy containing empagliflozin 10 mg or placebo (4.5% vs 1.8% and 1.8%, respectively).74 In the linagliptin as add-on study, events consistent with genital infection were reported in more patients receiving empagliflozin plus placebo (plus metformin) than those receiving combination therapy (plus metformin); 8.0% and 3.1% for empagliflozin 25 and 10 mg, respectively, plus placebo, vs 2.7% and 2.4% for combination therapy with empagliflozin 25 and 10 mg, respectively.75
Discussion
T2DM is a multifactorial, multiorgan, and progressive disease, during which glucose control worsens due to the deterioration of pancreatic β-cell function and increasing insulin resistance.1 In practice, this inevitably requires the intensification of glucose-lowering drug therapy and the use of dual or even triple therapy in the effort to achieve and maintain glucose control,76 per current diabetes management recommendations.7,8 However, many patients with T2DM failing to achieve their glucose targets do not receive intensification of glucose-lowering therapy in a timely manner,77 with delays of ~1–3 years reported for patients with HbA1c ≥7% to receive additional glucose-lowering medication.78,79 A recent retrospective cohort study based on patients with T2DM from the UK (N=105,477) reported that 22% of newly diagnosed patients had poor glucose control over 2 years and 26% did not receive treatment intensification.80 This study further concluded that delaying treatment intensification by 1 year in conjunction with poor glucose control significantly increased the risk of cardiovascular events.80
Clinical inertia, defined as the failure to initiate or intensify treatment in a timely manner to address a progressing medical condition,81 is common in management of T2DM, and is evident by the fact that treatment targets from diabetes guidelines and those attained in reality often differ, such that failure to achieve targets occurs in a large proportion of adults with diabetes.4,81 Deficiencies in communication and engagement between physicians and patients on goals and treatment approaches for diabetes appear to be a key issue,81 and recommendations for improvement include treating patients as active partners, establishing realistic and shared treatment goals, individualizing all aspects of diabetes care, and focusing on good management early in the disease to optimize patient quality of life.81
There are many choices for therapy in patients with T2DM requiring treatment intensification, with the rationale, mechanism, and clinical data on combination therapy with DPP-4 inhibitors and SGLT2 inhibitors being explored in depth in this review. Each choice in the treatment of T2DM carries its own merits and clinical considerations. Clinical considerations that may support the use of combination therapy include the potential for enhancing treatment adherence and the concept of simultaneously addressing several pathophysiologic defects in T2DM. The use of combination drug therapy may improve patient adherence to treatment by facilitating the use of less complex treatment regimens with fewer pills, particularly if single-pill (ie, fixed-dose) combination formulations are used.82 Frequency and timing of dosing can also affect adherence, and once-daily dosing is associated with higher adherence rates.82 Also, by facilitating the use of submaximal doses of each agent, combination therapy may result in fewer side effects,1 which may further improve adherence to treatment by the patient.83
When combination therapy is used for patients with T2DM, the selection of glucose-lowering agents with complementary modes of action may help to protect pancreatic β-cell function and thereby preserve glucose control.1,5 As SGLT2 inhibitors have a unique mechanism of action, and are not dependent on insulin or the degree of insulin resistance, they could be given with any class of glucose-lowering agent, including DPP-4 inhibitors, and at any stage of disease progression in T2DM,33,34 provided the patient has adequate renal function. The other main consideration for any combination drug therapy is to avoid the potential accumulation of adverse effects from the component drugs.5 Medication-related body weight gain and increased risk of hypoglycemia are particularly important to patients with T2DM,83,84 and may affect subsequent adherence to treatment.83 DPP-4 inhibitors are body weight neutral,12 whereas SGLT2 inhibitors produce small reductions in body weight,45–47 and neither of these drug classes is associated with a significantly increased risk of hypoglycemia (unless coadministered with insulin secretagogues, eg, sulfonylureas or insulin).12,45–47 Therefore, as DPP-4 inhibitors and SGLT2 inhibitors have distinct and compatible mechanisms of action, their use as a combination therapy would appear to be a balanced option, providing efficacy with an acceptable safety and tolerability profile.
Although commentators have discussed the potential for additive efficacy in combination therapies, clinical trials data have not currently demonstrated synergistic effects in lowering plasma glucose or HbA1c when DPP-4 inhibitors were combined with SGLT2 inhibitors6,69,72,73 (and Table 5). This is not surprising since it had been postulated that the stimulation of endogenous glucose production observed with SGLT2 inhibitors85,86 may be too strong to be prevented by DPP-4 inhibitors, which reduce plasma glucose primarily by suppressing glucagon secretion and inhibiting production of endogenous glucose;11 thus, reducing the latter’s glucose-lowering ability,6,87 although further studies are required to confirm this.6 However, it should be noted that combination therapy is not necessarily about achieving additive efficacy, rather it may address the incremental benefits of combining different drug classes. There are also potentially beneficial effects beyond glucose lowering to consider. For example, improvements in albuminuria have been observed with both DPP-4 inhibitors and SGLT2 inhibitors, and combination therapy may offer a therapeutic option for patients with chronic kidney disease.88 The lack of increase in body weight associated with DPP-4 inhibitors, or the modest reduction in body weight associated with SGLT2 inhibitors may make combination therapy with these agents suitable for patients who are overweight or obese. Similarly, the BP-lowering effect of the SGLT2 inhibitor component may be useful in patients with hypertension. Also, following the publication of data from the landmark EMPA-REG OUTCOME trial, which showed that patients with T2DM and at high risk of cardiovascular disease who received empagliflozin (in addition to standard of care), as compared with placebo, had a lower rate of cardiovascular mortality and all-cause mortality, and a reduced rate of hospitalization for heart failure,89 SGLT2 inhibitors are likely to be studied in more combinations and in earlier stages of T2DM.
Finally, the limitations of this report must be considered. No systematic review or meta-analysis was conducted, and only data from RCTs were included; however, observational (real world) data on this topic are not yet available. Furthermore, as stated above, the sequence of glucose-lowering medication used in combination therapy was neither discussed, nor was there any comparison of the efficacy and safety of combination vs stepwise therapy. These issues might be topics for future studies, together with investigation of cost issues relating to combination therapy.
Conclusion
With an overall favorable efficacy and safety profile, combination therapy with DPP-4 inhibitors and SGLT2 inhibitors has the potential to play an important role in the management of patients with T2DM. The tolerability of this combination, in particular the absence of body weight gain and the low risk of hypoglycemia, may add to its potential viability as an option for early treatment intensification in T2DM.
Acknowledgments
Writing assistance was provided by Debra Brocksmith, MB ChB, PhD, of Envision Scientific Solutions, which was contracted and funded by Boehringer Ingelheim Pharmaceuticals, Inc. (BIPI). BIPI was given the opportunity to review the manuscript for medical and scientific accuracy as well as intellectual property considerations.
Disclosure
VRA was the MedStar Health Research Institute’s principal clinical trial investigator for studies involving AstraZeneca/BMS, Calibra, Esai, Elcelyx, Janssen, Novo Nordisk, Sanofi, and Theracos; is a consultant for Adocia, the American Diabetes Association, MedScape, and Tufts; and was a consultant for AstraZeneca/BMS, Janssen, Novo Nordisk, and Sanofi. SAY reports no conflicts of interest in this work.
References
DeFronzo RA, Eldor R, Abdul-Ghani M. Pathophysiologic approach to therapy in patients with newly diagnosed type 2 diabetes. Diabetes Care. 2013;36 (Suppl 2):S127–S138. | ||
Defronzo RA. Banting Lecture. From the triumvirate to the ominous octet: a new paradigm for the treatment of type 2 diabetes mellitus. Diabetes. 2009;58(4):773–795. | ||
Inzucchi SE, Bergenstal RM, Buse JB, et al. Management of hyperglycemia in type 2 diabetes, 2015: a patient-centered approach: update to a position statement of the American Diabetes Association and the European Association for the Study of Diabetes. Diabetes Care. 2015;38(1):140–149. | ||
Stark Casagrande S, Fradkin JE, Saydah SH, Rust KF, Cowie CC. The prevalence of meeting A1C, blood bressure, and LDL goals among people with diabetes, 1988–2010. Diabetes Care. 2013;36(8):2271–2279. | ||
Zinman B. Initial combination therapy for type 2 diabetes mellitus: is it ready for prime time? Am J Med. 2011;124(1 Suppl):S19–S34. | ||
Abdul-Ghani M. Where does combination therapy with an SGLT2 inhibitor plus a DPP-4 inhibitor fit in the management of type 2 diabetes? Diabetes Care. 2015;38(3):373–375. | ||
American Diabetes Association. 7. Approaches to glycemic treatment. Diabetes Care. 2016;39 (Suppl 1):S52–S59. | ||
Garber AJ, Abrahamson MJ, Barzilay JI, et al. Consensus statement by the American Association of Clinical Endocrinologists and American College of Endocrinology on the comprehensive type 2 diabetes management algorithm – 2016 executive summary. Endocr Pract. 2016;22(1):84–113. | ||
Ahrén B, Simonsson E, Larsson H, et al. Inhibition of dipeptidyl peptidase IV improves metabolic control over a 4-week study period in type 2 diabetes. Diabetes Care. 2002;25(5):869–875. | ||
Deacon CF. Dipeptidyl peptidase-4 inhibitors in the treatment of type 2 diabetes: a comparative review. Diabetes Obes Metab. 2011;13(1):7–18. | ||
Balas B, Baig MR, Watson C, et al. The dipeptidyl peptidase IV inhibitor vildagliptin suppresses endogenous glucose production and enhances islet function after single-dose administration in type 2 diabetic patients. J Clin Endocrinol Metab. 2007;92(4):1249–1255. | ||
Scheen AJ. A review of gliptins in 2011. Expert Opin Pharmacother. 2012;13(1):81–99. | ||
Scheen AJ. A review of gliptins for 2014. Expert Opin Pharmacother. 2015;16(1):43–62. | ||
Baetta R, Corsini A. Pharmacology of dipeptidyl peptidase-4 inhibitors: similarities and differences. Drugs. 2011;71(11):1441–1467. | ||
Scheen AJ. Pharmacokinetics and clinical use of incretin-based therapies in patients with chronic kidney disease and type 2 diabetes. Clin Pharmacokinet. 2015;54(1):1–21. | ||
Merck & Co. Inc. Prescribing Information (08/2015): JANUVIA® (sitagliptin) Tablets. Available from: http://www.accessdata.fda.gov/drugsatfda_docs/label/2015/021995s034lbl.pdf. Accessed June 20, 2016. | ||
Bristol-Myers Squibb Company. Prescribing Information (04/2016): ONGLYZA (saxagliptin) Tablets, for Oral Use. Available from: http://www.accessdata.fda.gov/drugsatfda_docs/label/2016/022350s014lbl.pdf. Accessed June 20, 2016. | ||
Boehringer Ingelheim Pharmaceuticals, Inc. Prescribing Information (08/2015): Tradjenta® (linagliptin) Tablets. Available from: http://www.accessdata.fda.gov/drugsatfda_docs/label/2015/201280s012lbl.pdf. Accessed June 20, 2016. | ||
Takeda Pharmaceuticals USA, Inc. Prescribing Information (05/2016): NESINA (alogliptin) Tablets. Available from: http://www.accessdata.fda.gov/drugsatfda_docs/label/2016/022271s009lbl.pdf. Accessed June 20, 2016. | ||
Aschner P, Kipnes MS, Lunceford JK, et al. Effect of the dipeptidyl peptidase-4 inhibitor sitagliptin as monotherapy on glycemic control in patients with type 2 diabetes. Diabetes Care. 2006;29(12):2632–2637. | ||
Rosenstock J, Aguilar-Salinas C, Klein E, et al. Effect of saxagliptin monotherapy in treatment-naïve patients with type 2 diabetes. Curr Med Res Opin. 2009;25(10):2401–2411. | ||
Del Prato S, Barnett AH, Huisman H, Neubacher D, Woerle HJ, Dugi KA. Effect of linagliptin monotherapy on glycaemic control and markers of β-cell function in patients with inadequately controlled type 2 diabetes: a randomized controlled trial. Diabetes Obes Metab. 2011;13(3):258–267. | ||
DeFronzo RA, Fleck PR, Wilson CA, Mekki Q; Alogliptin Study 010 Group. Efficacy and safety of the dipeptidyl peptidase-4 inhibitor alogliptin in patients with type 2 diabetes and inadequate glycemic control: a randomized, double-blind, placebo-controlled study. Diabetes Care. 2008;31(12):2315–2317. | ||
Craddy P, Palin HJ, Johnson KI. Comparative effectiveness of dipeptidylpeptidase-4 inhibitors in type 2 diabetes: a systematic review and mixed treatment comparison. Diabetes Ther. 2014;5(1):1–41. | ||
Zhang X, Zhao Q. Effects of dipeptidyl peptidase-4 inhibitors on blood pressure in patients with type 2 diabetes: a systematic review and meta-analysis. J Hypertens. 2016;34(2):167–175. | ||
Scheen AJ. Safety of dipeptidyl peptidase-4 inhibitors for treating type 2 diabetes. Expert Opin Drug Saf. 2015;14(4):505–524. | ||
Karagiannis T, Boura P, Tsapas A. Safety of dipeptidyl peptidase 4 inhibitors: a perspective review. Ther Adv Drug Saf. 2014;5(3):138–146. | ||
Scirica BM, Bhatt DL, Braunwald E, et al. Saxagliptin and cardiovascular outcomes in patients with type 2 diabetes mellitus. N Engl J Med. 2013;369(14):1317–1326. | ||
Zannad F, Cannon CP, Cushman WC, et al. Heart failure and mortality outcomes in patients with type 2 diabetes taking alogliptin versus placebo in EXAMINE: a multicentre, randomised, double-blind trial. Lancet. 2015;385(9982):2067–2076. | ||
Green JB, Bethel MA, Armstrong PW, et al. Effect of sitagliptin on cardiovascular outcomes in type 2 diabetes. N Engl J Med. 2015;373(3):232–242. | ||
Toh S, Hampp C, Reichman ME, et al. Risk for hospitalized heart failure among new users of saxagliptin, sitagliptin, and other antihyperglycemic drugs: a retrospective cohort study. Ann Intern Med. 2016;164(11):705–714. | ||
Li L, Li S, Deng K, et al. Dipeptidyl peptidase-4 inhibitors and risk of heart failure in type 2 diabetes: systematic review and meta-analysis of randomised and observational studies. BMJ. 2016;352:i610. | ||
DeFronzo RA, Davidson JA, Del Prato S. The role of the kidneys in glucose homeostasis: a new path towards normalizing glycaemia. Diabetes Obes Metab. 2012;14(1):5–14. | ||
Zhang L, Feng Y, List J, Kasichayanula S, Pfister M. Dapagliflozin treatment in patients with different stages of type 2 diabetes mellitus: effects on glycaemic control and body weight. Diabetes Obes Metab. 2010;12(6):510–516. | ||
Nauck MA. Update on developments with SGLT2 inhibitors in the management of type 2 diabetes. Drug Des Devel Ther. 2014;8:1335–1380. | ||
Washburn WN, Poucher SM. Differentiating sodium-glucose co-transporter-2 inhibitors in development for the treatment of type 2 diabetes mellitus. Expert Opin Investig Drugs. 2013;22(4):463–486. | ||
Scheen AJ. Evaluating SGLT2 inhibitors for type 2 diabetes: pharmacokinetic and toxicological considerations. Expert Opin Drug Metab Toxicol. 2014;10(5):647–663. | ||
Lamos EM, Younk LM, Davis SN. Canagliflozin, an inhibitor of sodium-glucose cotransporter 2, for the treatment of type 2 diabetes mellitus. Expert Opin Drug Metab Toxicol. 2013;9(6):763–775. | ||
Kasichayanula S, Liu X, Lacreta F, Griffen SC, Boulton DW. Clinical pharmacokinetics and pharmacodynamics of dapagliflozin, a selective inhibitor of sodium-glucose co-transporter type 2. Clin Pharmacokinet. 2014;53(1):17–27. | ||
Scheen AJ. Pharmacokinetic and pharmacodynamic profile of empagliflozin, a sodium glucose co-transporter 2 inhibitor. Clin Pharmacokinet. 2014;53(3):213–225. | ||
Janssen Pharmaceuticals Inc. Prescribing Information (08/2016): INVOKANA (canagliflozin) Tablets, for Oral Use. Available from: http://www.accessdata.fda.gov/drugsatfda_docs/label/2016/204042s022lbl.pdf. Accessed December 20, 2016. | ||
AstraZeneca Pharmaceuticals LP. Prescribing Information (08/2016): FARXIGA® (dapagliflozin) Tablets, for Oral Use. Available from: http://www.accessdata.fda.gov/drugsatfda_docs/label/2016/202293s010lbl.pdf. Accessed December 20, 2016. | ||
Boehringer Ingelheim Pharmaceuticals, Inc. Prescribing Information (12/2016): JARDIANCE® (empagliflozin) Tablets, for Oral Use. Available from: http://www.accessdata.fda.gov/drugsatfda_docs/label/2016/204629s008lbl.pdf. Accessed December 20, 2016. | ||
Grempler R, Thomas L, Eckhardt M, et al. Empagliflozin, a novel selective sodium glucose cotransporter-2 (SGLT-2) inhibitor: characterisation and comparison with other SGLT-2 inhibitors. Diabetes Obes Metab. 2012;14(1):83–90. | ||
Yang XP, Lai D, Zhong XY, Shen HP, Huang YL. Efficacy and safety of canagliflozin in subjects with type 2 diabetes: systematic review and meta-analysis. Eur J Clin Pharmacol. 2014;70(10):1149–1158. | ||
Zhang M, Zhang L, Wu B, Song H, An Z, Li S. Dapagliflozin treatment for type 2 diabetes: a systematic review and meta-analysis of randomized controlled trials. Diabetes Metab Res Rev. 2014;30(3):204–221. | ||
Liakos A, Karagiannis T, Athanasiadou E, et al. Efficacy and safety of empagliflozin for type 2 diabetes: a systematic review and meta-analysis. Diabetes Obes Metab. 2014;16(10):984–993. | ||
Ferrannini E, Ramos SJ, Salsali A, Tang W, List JF. Dapagliflozin monotherapy in type 2 diabetic patients with inadequate glycemic control by diet and exercise: a randomized, double-blind, placebo-controlled, phase 3 trial. Diabetes Care. 2010;33(10):2217–2224. | ||
Stenlöf K, Cefalu WT, Kim KA, et al. Efficacy and safety of canagliflozin monotherapy in subjects with type 2 diabetes mellitus inadequately controlled with diet and exercise. Diabetes Obes Metab. 2013;15(4):372–382. | ||
Roden M, Weng J, Eilbracht J, et al. Empagliflozin monotherapy with sitagliptin as an active comparator in patients with type 2 diabetes: a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Diabetes Endocrinol. 2013;1(3):208–219. | ||
Geerlings S, Fonseca V, Castro-Diaz D, List J, Parikh S. Genital and urinary tract infections in diabetes: impact of pharmacologically-induced glucosuria. Diabetes Res Clin Pract. 2014;103(3):373–381. | ||
Johnsson KM, Ptaszynska A, Schmitz B, Sugg J, Parikh SJ, List JF. Vulvovaginitis and balanitis in patients with diabetes treated with dapagliflozin. J Diabetes Complications. 2013;27(5):479–484. | ||
Nyirjesy P, Sobel JD, Fung A, et al. Genital mycotic infections with canagliflozin, a sodium glucose co-transporter 2 inhibitor, in patients with type 2 diabetes mellitus: a pooled analysis of clinical studies. Curr Med Res Opin. 2014;30(6):1109–1119. | ||
Dailey G. Empagliflozin for the treatment of type 2 diabetes mellitus: an overview of safety and efficacy based on Phase 3 trials. J Diabetes. 2015;7(4):448–461. | ||
Johnsson KM, Ptaszynska A, Schmitz B, Sugg J, Parikh SJ, List JF. Urinary tract infections in patients with diabetes treated with dapagliflozin. J Diabetes Complications. 2013;27(5):473–478. | ||
Nicolle LE, Capuano G, Fung A, Usiskin K. Urinary tract infection in randomized phase III studies of canagliflozin, a sodium glucose co-transporter 2 inhibitor. Postgrad Med. 2014;126(1):7–17. | ||
US Food and Drug Administration. Drug safety communication (December 4, 2015). FDA revises labels of SGLT2 inhibitors for diabetes to include warnings about too much acid in the blood and serious urinary tract infections. Available from: http://www.fda.gov/Drugs/DrugSafety/ucm475463.htm. Accessed February 03, 2016. | ||
Peters AL, Buschur EO, Buse JB, Cohan P, Diner JC, Hirsch IB. Euglycemic diabetic ketoacidosis: a potential complication of treatment with sodium-glucose cotransporter 2 inhibition. Diabetes Care. 2015;38(9):1687–1693. | ||
Roach P, Skierczynski P. Euglycemic diabetic ketoacidosis in a patient with type 2 diabetes after treatment with empagliflozin. Diabetes Care. 2016;39(1):e3. | ||
Hine J, Paterson H, Abrol E, Russell-Jones D, Herring R. SGLT inhibition and euglycaemic diabetic ketoacidosis. Lancet Diabetes Endocrinol. 2015;3(7):503–504. | ||
Harati H, Sharma V, Motazedi A. Sodium-glucose cotransporter 2 inhibitor-associated diabetic ketoacidosis: report of two cases with hyperglycemic ketoacidosis in type 1 diabetes. J Diabetes. 2016;8(1):165. | ||
Gelaye A, Haidar A, Kassab C, Kazmi S, Sinha P. Severe ketoacidosis associated with canagliflozin (Invokana): a safety concern. Case Rep Crit Care. 2016;2016:1656182. | ||
Erondu N, Desai M, Ways K, Meininger G. Diabetic ketoacidosis and related events in the canagliflozin type 2 diabetes clinical program. Diabetes Care. 2015;38(9):1680–1686. | ||
Rosenstock J, Ferrannini E. Euglycemic diabetic ketoacidosis: a predictable, detectable, and preventable safety concern with SGLT2 inhibitors. Diabetes Care. 2015;38(9):1638–1642. | ||
Kasichayanula S, Liu X, Shyu WC, et al. Lack of pharmacokinetic interaction between dapagliflozin, a novel sodium-glucose transporter 2 inhibitor, and metformin, pioglitazone, glimepiride or sitagliptin in healthy subjects. Diabetes Obes Metab. 2011;13(1):47–54. | ||
Brand T, Macha S, Mattheus M, Pinnetti S, Woerle HJ. Pharmacokinetics of empagliflozin, a sodium glucose cotransporter-2 (SGLT-2) inhibitor, coadministered with sitagliptin in healthy volunteers. Adv Ther. 2012;29(10):889–899. | ||
Friedrich C, Metzmann K, Rose P, Mattheus M, Pinnetti S, Woerle HJ. A randomized, open-label, crossover study to evaluate the pharmacokinetics of empagliflozin and linagliptin after coadministration in healthy male volunteers. Clin Ther. 2013;35(1):A33–A42. | ||
Jabbour SA, Hardy E, Sugg J, Parikh S; Study 10 Group. Dapagliflozin is effective as add-on therapy to sitagliptin with or without metformin: a 24-week, multicenter, randomized, double-blind, placebo-controlled study. Diabetes Care. 2014;37(3):740–750. | ||
Rosenstock J, Hansen L, Zee P, et al. Dual add-on therapy in type 2 diabetes poorly controlled with metformin monotherapy: a randomized double-blind trial of saxagliptin plus dapagliflozin addition versus single addition of saxagliptin or dapagliflozin to metformin. Diabetes Care. 2015;38(3):376–383. | ||
Mathieu C, Ranetti AE, Li D, et al. Randomized, double-blind, phase 3 trial of triple therapy with dapagliflozin add-on to saxagliptin plus metformin in type 2 diabetes. Diabetes Care. 2015;38(11):2009–2017. | ||
Matthaei S, Catrinoiu D, Celinski A, et al. Randomized, double-blind trial of triple therapy with saxagliptin add-on to dapagliflozin plus metformin in patients with type 2 diabetes. Diabetes Care. 2015;38(11):2018–2024. | ||
Lewin A, DeFronzo RA, Patel S, et al. Initial combination of empagliflozin and linagliptin in subjects with type 2 diabetes. Diabetes Care. 2015;38(3):394–402. | ||
DeFronzo RA, Lewin A, Patel S, et al. Combination of empagliflozin and linagliptin as second-line therapy in subjects with type 2 diabetes inadequately controlled on metformin. Diabetes Care. 2015;38(3):384–393. | ||
Søfteland E, Meier JJ, Vangen B, Toorawa R, Maldonado-Lutomirsky M, Broedl UC. Empagliflozin as add-on therapy in patients with type 2 diabetes inadequately controlled with linagliptin and metformin: a 24-week randomized, double-blind, parallel-group trial. Diabetes Care. 2017;40(2):201–209. | ||
Tinahones FJ, Gallwitz B, Nordaby M, et al. Linagliptin as add-on to empagliflozin and metformin in patients with type 2 diabetes: two 24-week randomized, double-blind, double-dummy, parallel-group trials. Diabetes Obes Metab. 2017;19(2):266–274. | ||
Neumiller JJ. Efficacy and safety of saxagliptin as add-on therapy in type 2 diabetes. Clin Diabetes. 2014;32(4):170–177. | ||
Engel SS, Seck TL, Golm GT, Meehan AG, Kaufman KD, Goldstein BJ. Assessment of AACE/ACE recommendations for initial dual antihyperglycemic therapy using the fixed-dose combination of sitagliptin and metformin versus metformin. Endocr Pract. 2013;19(5):751–757. | ||
Khunti K, Wolden ML, Thorsted BL, Andersen M, Davies MJ. Clinical inertia in people with type 2 diabetes: a retrospective cohort study of more than 80,000 people. Diabetes Care. 2013;36(11):3411–3417. | ||
Fu AZ, Qiu Y, Davies MJ, Radican L, Engel SS. Treatment intensification in patients with type 2 diabetes who failed metformin monotherapy. Diabetes Obes Metab. 2011;13(8):765–769. | ||
Paul SK, Klein K, Thorsted BL, Wolden ML, Khunti K. Delay in treatment intensification increases the risks of cardiovascular events in patients with type 2 diabetes. Cardiovasc Diabetol. 2015;14:100. | ||
Strain WD, Cos X, Hirst M, et al. Time to do more: addressing clinical inertia in the management of type 2 diabetes mellitus. Diabetes Res Clin Pract. 2014;105(3):302–312. | ||
Nau DP. Recommendations for improving adherence to type 2 diabetes mellitus therapy–focus on optimizing oral and non-insulin therapies. Am J Manag Care. 2012;18(3 Suppl):S49–S54. | ||
Hauber AB, Mohamed AF, Johnson FR, Falvey H. Treatment preferences and medication adherence of people with type 2 diabetes using oral glucose-lowering agents. Diabet Med. 2009;26(4):416–424. | ||
Barendse S, Singh H, Frier BM, Speight J. The impact of hypoglycaemia on quality of life and related patient-reported outcomes in type 2 diabetes: a narrative review. Diabet Med. 2012;29(3):293–302. | ||
Merovci A, Solis-Herrera C, Daniele G, et al. Dapagliflozin improves muscle insulin sensitivity but enhances endogenous glucose production. J Clin Invest. 2014;124(2):509–514. | ||
Ferrannini E, Muscelli E, Frascerra S, et al. Metabolic response to sodium-glucose cotransporter 2 inhibition in type 2 diabetic patients. J Clin Invest. 2014;124(2):499–508. | ||
Schernthaner G, Schernthaner-Reiter MH. How attractive is the combination of a sodium glucose co-transporter 2 inhibitor with a dipeptidyl peptidase 4 inhibitor in the treatment of type 2 diabetes? Diabetes Obes Metab. 2015;17(7):613–615. | ||
Schernthaner G, Mogensen CE, Schernthaner GH. The effects of GLP-1 analogues, DPP-4 inhibitors and SGLT2 inhibitors on the renal system. Diab Vasc Dis Res. 2014;11(5):306–323. | ||
Zinman B, Wanner C, Lachin JM, et al. Empagliflozin, cardiovascular outcomes, and mortality in type 2 diabetes. N Engl J Med. 2015;373(22):2117–2128. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.