")
Back to Journals » Clinical Interventions in Aging » Volume 9
Silent and suffering: a pilot study exploring gaps between theory and practice in pain management for people with severe dementia in residential aged care facilities
Authors Peisah C, Weaver J, Wong L, Strukovski J
Received 21 March 2014
Accepted for publication 11 June 2014
Published 15 October 2014 Volume 2014:9 Pages 1767—1774
DOI https://doi.org/10.2147/CIA.S64598
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Carmelle Peisah,1–3 Judith Weaver,1 Lisa Wong,1 Julie-Anne Strukovski1
1Behaviour Assessment Management Service, Specialist Mental Health Services for Older People, Mental Health Drug and Alcohol, Northern Sydney Local Health District, 2University of Sydney, 3University of NSW, Sydney, NSW, Australia
Background: Pain is common in older people, particularly those in residential aged care facilities (RACF) and those with dementia. However, despite 20 years of discourse on pain and dementia, pain is still undetected or misinterpreted in people with dementia in residential aged care facilities, particularly those with communication difficulties.
Methods: A topical survey typology with semistructured interviews was used to gather attitudes and experiences of staff from 15 RACF across Northern Sydney Local Health District.
Results: While pain is proactively assessed and pain charts are used in RACF, this is more often regulatory-driven than patient-driven (eg, prior to accreditation). Identification of pain and need for pain relief was ill defined and poorly understood. Both pharmacological and nonpharmacological regimes were used, but in an ad hoc, variable and unsystematic manner, with patient, staff, and attitudinal obstacles between the experience of pain and its relief.
Conclusion: A laborious “pain communication chain” exists between the experience of pain and its relief for people with severe dementia within RACF. Given the salience of pain for older people with dementia, we recommend early, proactive consideration and management of pain in the approach to behaviors of concern. Individualized pain measures for such residents; empowerment of nursing staff as “needs interpreters”; collaborative partnerships with common care goals between patients where possible; RACF staff, doctors, and family carers; and more meaningful use of pain charts to map response to stepped pain protocols may be useful strategies to explore in clinical settings.
Keywords: pain, dementia, severe, residential aged care, facilities
Introduction
Pain is common in older people,1 particularly those in residential aged care facilities2,3 and those with dementia.4 People with severe dementia have multiple potential sources of pain, such as genitourinary infection, fall-related injuries, pressure ulcers, contractures, and gastrointestinal and cardiac pain, compounding the generic musculoskeletal and cancer-related pain associated with ageing per se.1,4 This has been known for some time, yet pain is still undetected, misinterpreted, or inaccurately assessed in older adults with dementia.3–6 It is unclear why this still occurs when problems of pain and its detection among older adults with cognitive impairment were recognized some 20 years ago,7 have been discussed at length since,4 and access to pain management is recognized as a fundamental human right.8 The Australian Commonwealth Department of Health and Aged Care Accreditation Standard 2.8 mandates that “all residents are as free as possible from pain” and requires documented evidence of identification, assessment, and review of pain and appropriate programs for managing symptoms.9
Pain and dementia are complex partners. We know that persons with dementia still experience sensation of pain, although interpretation of pain stimulus and the affective and behavioral responses to that sensation may be different.10,11 Perhaps the most crucial factor distinguishing those with and without cognitive impairment in regards to pain is the problem with communication, hindering verbal and other expression of pain, and its interpretation by those who might assist in its relief. Most importantly, there is wide acceptance of a relationship between pain and behaviors of concern in dementia, which may be the only indication of pain in some patients, although the relationship between pain and behavior varies from person to person.12,13
Acknowledging these difficulties in detecting pain in people with dementia, there has been a concerted effort to develop pain assessment tools specifically for people with dementia, of which there are over 35 available.4,14 However, a number of limitations have been associated with these instruments including: lack of user friendliness with intensive observation required; nonspecificity for pain; unusual anchor points; failure to detect pain in some individuals due to individual variability in pain expression; and lack of guidelines as to when to action pain relief. Evaluation of these tools has been restricted to narrow samples or settings, and there is no tool with strong reliability and validity applicable across a range of settings.14,15 As a result, although these tools possibly exist in filing cabinets, we suspect that they are often not used in everyday practice “on the floor” in residential aged care facilities.
In terms of treatment, in a review of pain treatments in dementia, Corbett et al4 identified nine randomized prospective treatment studies with a comparison group or open studies with more than ten participants. A double-blind, randomized controlled trial, stepped treatment using person-centered nonpharmacological treatment, analgesia or antipsychotics reduced discomfort and behavioral symptoms16 as did a cluster randomized controlled trial using paracetamol (acetaminophen), morphine, buprenorphine transdermal patch, or pregabalin.17 In contrast, a small double-blind, placebo-controlled trial of opioids showed no difference in agitation except in a subgroup of older patients;18 and two studies of paracetamol showed an improvement in function and social interaction, but neither agitation nor well-being19 nor pain,20 although the dose in the latter study was only 2,600 mg/day. In regards to nonpharmacological treatment regimes, access to which is mandated by commonwealth standards, there is only limited evidence supporting reflexology, music, or combinations of nonpharmacological and pharmacological therapy using stepped treatment approaches.4
There is no shortage of obligations to treat pain, scales to identify pain, nor potential treatment regimes, with the exception of empirically tested nonpharmacological strategies. Yet, our experience in working with people with severe dementia, particularly those with complex behaviors, is that lip service is paid to meeting the commonwealth standards in regards to pain detection and management and that pain is often not “on the radar” in residential aged care facilities. Our clinical observations are that patients with cognitive impairment, whose communication difficulties or abulia conspire to render them silent sufferers, fare poorly; and those whose pain manifests as screaming or agitation, noisy but also undetected sufferers, fare even worse.
Earlier work has identified barriers to pain assessment in dementia, such as lack of recognition and misdiagnosis/late diagnosis of pain, poor staff education, and nonuse of assessment tools.5 However, staff attitudes and practices in regards to these barriers, and the use of stepped management approaches and the systems relationships upon which they rely, have not been explored.
Our objectives were to explore attitudes and processes relating to pain assessment and management for people with severe dementia in residential aged care facilities. We hypothesized that: pain in older people with severe dementia in residential aged care facilities is not proactively assessed; pain tools exist in the facility but are not used or found useful; both pharmacological and nonpharmacological analgesic regimes are infrequently used, and frequently ceased without structured review; pain is not managed effectively due to a lack of knowledge amongst staff within and amongst those providing input to residential aged care facilities (RACF); there is a need to improve partnerships between medical prescribers and frontline nursing staff in regards to pain management.
Materials and methods
We surveyed staff from 15 residential aged care facilities across the Northern Sydney Local Health District, Australia, that were former or current referrers to our Behaviour Assessment Management Service (formerly Dementia Behaviour Management Advisory Service and Behaviour Assessment Specialist Intervention Service clinicians). The Behaviour Assessment Management Service is a highly specialized nurse-led service with old age psychiatry input that provides consultation, assessment, advice and guidance on management of behavioral and psychological symptoms of dementia and/or mental illness, to inpatients, community-dwelling ambulatory patients, and nursing home residents within the Northern Sydney Local Health District.
Senior and junior staff at these facilities were approached by Behaviour Assessment Management Service clinicians to participate in the survey, which was conducted face to face or by telephone. Topical survey typology21 was used with semistructured interviews using structured open-ended questions on topics such as how pain was assessed, what pain management strategies were used, and when they were used/not used, as well as questions regarding access to and relationship with medical staff and provision of pain education to staff.
The data were immediately transcribed and subject to a manifest content analysis, and then summarized, the intent of data collection being to gather information about a range of responses in regards to pain identification and management for people with severe dementia in RACF. There was some minimal transformation of data such as the obstacles to pain relief. This methodology, being a priori, hypothesis-driven, and with only minimal transformation of data, does not constitute qualitative methodology, but rather a descriptive, topical survey research methodology.21 The study was approved by the Northern Sydney Local Health District human research ethics committee.
Results
Respondents
The facilities included one low care facility, six high care facilities, and eight mixed “ageing in place” facilities with 44–100 beds. Twenty staff members across the facilities comprising four care managers or directors of nursing, ten registered nurses, and six Personal Care Worker ie, Assistants in Nursing/Personal Care Workers (Certificate III or IV). All respondents had recent direct experience with using pain charts and working with residents in pain.
Frequency and nature of pain assessment
All respondents had access to pain charts, all used Abbey Pain Charts, and two facilities used the Pain Assessment in Advanced Dementia scale additionally for patients with impaired communication skills. Timing and frequency of pain assessment was more often regulatory-driven, ie, “on admission” “using the ACFI [Aged Care Funding Instrument]”, or “in the run up to accreditation”, than patient-driven, ie, “when the person appears to be in pain”. Frequency of chart use was every 3, 6, or 12 months, and rarely “as often as required”. One respondent reported using a pain chart to convince a general practitioner who was “against the use of S8 drugs” (controlled drugs with high potential for abuse and addiction) to use analgesia. Pain charts were not used to monitor the efficacy of pain management.
Recognition of pain
Most commonly, staff looked for “calling out in pain”, “facial expression”, “grimacing”, “wincing”, “moaning”, and “frowning”. Thirty-five percent of respondents (7/20) reported behavior changes as a trigger for pain assessment, usually unspecified “behavior changes”, although pacing and restlessness were mentioned (n=2). Neither screaming nor aggression was mentioned at all. Some managers had insight into pain recognition and called for better identification by other staff: “Familiarity with residents guides staff to pick up a distinct indicator with each resident.” Another respondent noted:
I strongly suspect pain is not being assessed in patients with dementia, I do not understand why pain is not considered early when there are behavioral changes, people do not think having personal hygiene attended to is painful, even arthritis is not treated well, when you add a layer of cognitive impairment it’s even worse.
When is pharmacological management given or not given?
We were interested in the prompts for analgesia and when analgesia was not given. Paracetamol was used variably in 10%–100% of patients, most often as needed. It was used invariably (20/20) when “pain was observed”, eg, “when client voices pain, yells out or screams, facial expression or body language”, or occasionally (7/20) with changes in behavior. In terms of roles, certificate III care Worker/assistants in nursing detect pain, while registered nurses initiate treatment. One staff manager described the failure to give prescribed oxycodone as needed for a nocturnally restless patient due to the reluctance of the registered nurse on duty to use the drug. Pain medications were rarely prioritized when patients were refusing medications (only 3/20 respondents prioritized pain management over psychotropics or other physical care medications, a typical reason for not prioritizing being: “we think safety first”).
We found the reasons for not giving analgesia to be diverse. Circumstances under which pain medications are not given can be classified according to patient factors, staff and system factors, and attitudinal factors. Respondents’ statements illustrating these categories include:
Patient factors
- “When patient is unable to tolerate oral medications”
- “Patient no longer says they are in pain”
- “When patient resists, refuses, or is aggressive”
- “When the patient is asleep”
- “Constipation or side effects”
- “Patient says they are fine ‐ they think they have to be stoic”.
Staff and system factors
- “When facility cannot accommodate staffing requirements; when there is no registered nurse on call, eg, can only give S8 between 10 am and 6 pm, sometimes we have to transfer the patient”
- “Junior staff are not clear regarding the evidence for pain”
- “We do not give nurse-initiated medications, we need the certificate III care worker to liaise with the registered nurse”.
Attitudinal factors
- “Reluctance regarding the use of opioids; resistance by nursing/care staff, family members, or general practitioner ”
- “Some nurses/care workers are reluctant even when it is prescribed”
- “Every now and again the general practitioner will not listen to us ‐ often it is difficult because we do not want them ‘zonked out’ and a falls risk but we also feel they need more”
- “Only for palliative care”.
Education and understanding of pain in dementia
All but one facility provided education in pain once or twice a year, and from a variety of sources, including pharmacists, drug companies, Meditrax system, Aged Care Channel, and our own Behaviour Assessment Management Service. Education sessions were attended by all staff, from registered nurses to assistants in nursing/certificate III care workers. One respondent described education about pain occurring “at every handover meeting”.
Nonpharmacological management
Although a range of nonpharmacological measures were used sporadically and nonsystematically, such as massage, repositioning, physiotherapy “pain clinic” (n=1), transcutaneous electrical nerve stimulation (n=2), and music (n=1), the most common and often only strategy described was heat packs (although banned in some facilities). Inconsistency and variability was also evident: “some get pain clinics”, “some get occupational therapy”, and “some get TENS [transcutaneous electrical nerve stimulation]”. Notable were the comments about what staff did not and could not achieve for pain: “we could do more”, “we are not good with therapeutic touch”, and “the ACFI-funded pain physiotherapy resource was stopped”.
Interactions between nursing and medical staff
Interactions with medical staff were very variable, although problems were noted in communication between junior staff, assistants in nursing/certificate III care workers, and medical staff, which usually involved the registered nurse as a conduit. In particular, problems were identified in alerting medical staff that a resident was in pain: “Every now and again the GP does not want to listen when we really do believe the person is in pain”, “it’s variable, some listen, others discount us”, and “staff need to do more to pick the pain and suffering of residents”.
Discussion
In this preliminary investigation of attitudes and processes relating to pain assessment and management for people with severe dementia in RACF, we found that, contrary to our hypotheses and earlier studies,22 pain is proactively assessed and pain tools are used routinely. The Abbey Pain Scale23 was used universally and supplemented with the PAIN-AD tool.24 However, most often this practice was regulatory-driven, in response to pending accreditation, assessment mandated by funding instruments, or routine 3–12-monthly review, rather than patient needs-driven, which although a trigger for pain chart use, was ill-defined. Identifying patient pain was most often based on traditional, overt verbal demonstrations of pain or changed facial expressions which, although still valid in dementia,25 are known to be not always present. In some cases, nonspecific behavior change was a prompt for pain assessment, although staff could not identify any particular behaviors associated with pain.
There is no current evidence of a specific sign or behavior that distinguishes pain from other causes of distress in people with severe communication difficulties,26 although aggression, complaining, negativism, repetitious sentences and questions, constant requests for attention, and cursing or verbal aggression respond to pain treatment.27 Importantly, the lack of specificity of pain assessment tools means that they are only detecting the presence of distress, which could be the result of pain or indeed “psychic distress” caused by various psychosocial or emotional factors. For example, a study of pain assessment in older adults using the Doloplus-II (an established pain assessment tool for people with dementia) found that many of the items were also predictive of the severity of delirium, depression, and dementia.28 Finally, the reference by one staff member to “distinct indicators” is entirely concordant with the concept of a distinct pattern of distress cues, as described by Regnard et al26 and the importance placed on “knowing the person” for pain assessment and understanding each person’s pain cues to overcome barriers to successful pain management.5
In terms of management, both pharmacological and nonpharmacological analgesic regimes were used but in an ad hoc, variable, and unsystematic manner, with patient, staff, and attitudinal obstacles operating between pain experience and relief (see Table 1). There was no evidence that structured stepped protocols were used despite evidence supporting these.6,29 Typically, paracetamol is given on an as needed basis, consistent with previous work,20 which begs the question of how is “need” assessed in nonverbal, abulic patients? It is accepted that analgesics should be given on a regular basis not on an as required basis in the management of chronic pain. Moreover, analgesia is used without any structured review and pain charts are not used to gauge treatment efficacy, previously identified as essential.5,29,30 The unsystematic use of nonpharmacological measures merely reflects the paucity of empirical evidence supporting such,4 prompting an urgent call for more work in this area.
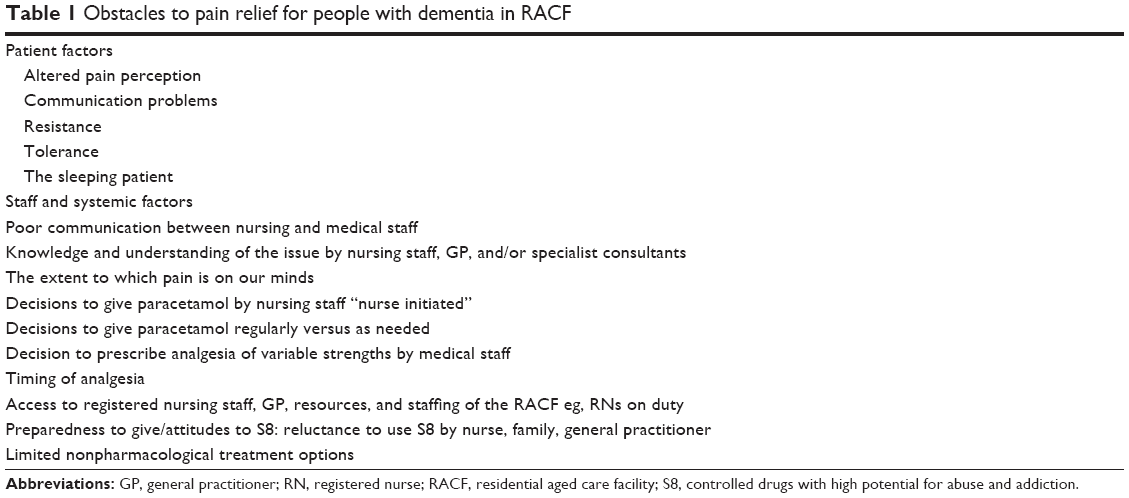 | Table 1 Obstacles to pain relief for people with dementia in RACF |
Contrary to our hypothesis, education was provided for staff in almost all facilities, and across the board for staff at all levels of seniority, indicating an improvement from previous studies that have demonstrated pain education in 34%–44% of nursing homes and mostly to senior staff.22 We were unable to assess the knowledge of staff and thus the efficacy of the education provided, but regardless of how experienced nursing staff are, or their exposure to pain education, there appears to be a thirst for more education and training, particularly in the assessment and recognition of pain in people with dementia.5
Importantly, education needs to be embedded within practice change principles. In Australia, a training module inservice package on pain and dementia was developed for RACFs in 2011 and implemented by the Dementia Behaviour Management Advisory Service and supported by resource materials, the sustainability and uptake of which remains dependent on several implementation strategies.29
Consistent with our hypothesis, there is a need to improve partnerships between medical prescribers and frontline nursing staff in regards to pain management. We have replicated previous findings regarding communication problems between nursing staff (those charged with identifying pain) and medical staff (those charged with prescribing analgesia). Using participatory action research methodology by surveying acute care staff, nursing staff, and physiotherapists, Gregory31 found that a major issue for staff in treating patients with cognitive impairment was getting doctors to recognize that patients were in pain.
Our findings suggest that for patients with severe dementia, there is a laborious “pain communication chain” that must be traversed to the point of pain relief. This starts off at the tissue level, progresses through pain pathways, then manifests in a myriad ways that are probably idiosyncratic to each person, to be picked up by the personal care Worker/Assistant in Nursing (certificate III or IV) or the family, who may (or may not) inform the registered nurse, who may (or may not) inform the physiotherapist or the general practitioner, who may (or may not) act on this information. This extends the multidimensional model of pain assessment devised by Snow et al32 which uses structural equation modelling to elucidate the relationships between pain components from the nociceptive stimulus and the external rater’s pain assessment. In particular, the model elaborates on some of the factors that influence the latter, including the rater’s knowledge of and beliefs about pain and dementia (which will influence their sensitivity to distress) and their relationship and time spent with the patient.32 Our findings extend this model to include the next steps, ie, the response of the external rater and their interactions with higher order “pain actioners”. Both education and partnerships need to target this pain communication chain.
If up to 80% of patients in RACF are in acute or chronic pain,4 we need to be thinking about pain at least 80% of the time, not only at admission, during the lead-up to accreditation, or at 12-monthly review. We need, as Thompsell and Hockley33 suggested, to increase the salience of pain in care goals by raising awareness and “embedding the issue into RACF practice”. As described by one respondent, pain needs to be regularly referred to in handovers and rounds. Although our charts are out of filing cabinets, with our finding of 100% use compared with 25% some 12 years ago,22 they need to be used more meaningfully, or replaced or supplemented by personalized pain measures empowering the intuition and observation5 of nursing staff as “pain interpreters” or “needs interpreters”. It is a frequent observation that frontline staff, especially assistants in nursing/Certificate III Care staff, “lack confidence or certainty in what they observe, making it difficult for them to advocate for the person with the communication difficulty when faced with a challenge to their observation”.34 Another important step in needs assessment by staff might be to establish the resident’s history of pain, ie, the second step in the Assessment of Discomfort in Dementia protocol, a clinical intervention protocol demonstrated to have value in assessment and management of unmet needs in people with dementia.16
This is compounded by the occasional resistance of senior nursing and medical staff, suggesting we may need to change our threshold for acting on presumed pain, or at least change our need for “evidence”.5 To that end, some have advocated for anticipatory prescribing or proactive treatment,33 but this needs to be both pharmacological and nonpharmacological. Finally, and perhaps most importantly, partnership with involved family members is mandatory for both needs assessment and for consent to the use of narcotic analgesics for those unable to give their own consent. Who better to assist us in “interpreting” possible pain or distress in those who cannot express such?
We recommend therefore a systematic, individualized approach to pain assessment and management that relies on a comprehensive history and examination to identify individualized pain patterns, possible etiologies, and management strategies that are based on mutual agreed upon care goals, and assessed using individualized outcome measures (see Table 2).
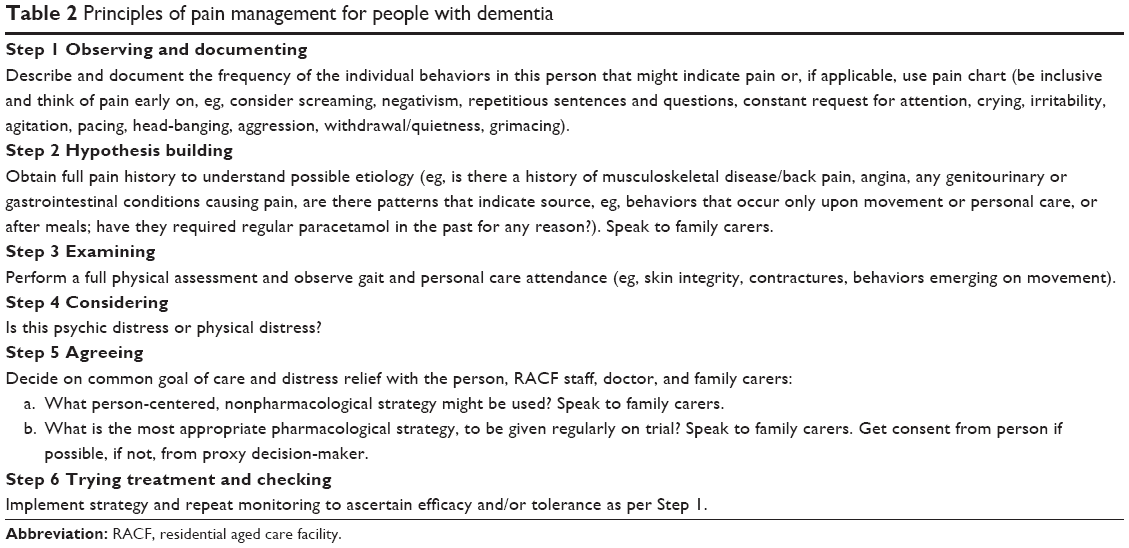 | Table 2 Principles of pain management for people with dementia |
We concede a number of limitations to this exploratory study, which predominantly served to inform our own work with RACFs and to promote further discussion. The sample was very small and contaminated by subjects being former or current clients of our dementia behavior assessment service, having received both intensive support regarding individual patients (many of whom we identified as having been in pain) and group education sessions (some specifically on pain). Clearly, our findings are not generalizable, although given the consistency with other work, we suspect it might be the “tip of the iceberg”. There remain many gaps. We know nothing about the prevalence of actual analgesic use or dosages and the indications for or tolerance of such. We did not measure knowledge about pain among either nursing or medical staff nor seek input from pain specialist staff, although we suspect the latter to be minimal, indicating an access issue which we plan to explore in future studies of service models for pain clinics in RACF. Notwithstanding the limitations of our work, our intent was to provide exploratory pilot data to facilitate raising of awareness and to serve the development of future study protocols.
Dementia may be painful, or at least distressing, particularly towards the end. It may be difficult to “see” pain, or “prove” that it exists to those empowered to relieve it. The experience of pain and distress in severe dementia is the ultimate dependency experience. The person must rely on an impaired mind and body to communicate to a range of people responsible for doing something about the pain, who in turn need to find individualized management options amongst the limited repertoire of empirically proven treatments for pain in dementia. This is what we are working towards.
Acknowledgments
The authors would like to thank Laura Hill and Giselle Bygraves for their assistance with the data collection.
Disclosure
The authors report no conflicts of interest in this work.
References
Blyth FM, March LM, Brnabic AJ, Jorm LR, Williamson M, Cousins MJ. Chronic pain in Australia: a prevalence study. Pain. 2001; 89:127-134. | ||
McClean WJ, Higginbotham HN. Prevalence of pain among nursing home residents in rural New South Wales. Med J Aust. 2002; 177:17-20. | ||
Takai Y, Yamamoto-Mitani N, Okamoto Y, Koyama K, Honda A. Literature review of pain prevalence among older residents of nursing homes. Pain Manag Nurs. 2010;11:209-223. | ||
Corbett A, Husebo B, Malcangio M, et al. Assessment and treatment of pain in people with dementia. Nat Rev Neurol. 2012;8:264-274. | ||
McAuliffe L, Nay R, O’Donnell M, Fetherstonhaugh D. Pain assessment with older people with dementia: literature review. J Adv Nurs. 2009;65:2-10. | ||
Achterberg WP, Pieper MJ, van Dalen-Kok AH, et al. Pain management in patients with dementia. Clin Interv Aging. 2013;8:1471–1482. | ||
Sengstaken EA, King SA. The problems of pain and its detection among geriatric nursing home residents. J Am Geriatr Soc. 1993;41:541–544. | ||
International Pain Summit of The International Association for The Study of Pain. Declaration of Montréal: declaration that access to pain management is a fundamental human right. J Pain Palliat Care Pharmacother. 2011;25:29-31. | ||
Aged Care Standards and Accreditation Agency Ltd. Accreditation Standards. Available from: http://www.accreditation.org.au/site/uploads/files/30985_AgedCare_ASENGLISHbro_cah_0011%20V1_3.pdf. Accessed July 26, 2014. | ||
Cole LJ, Gavrilescu M, Johnston LA, Gibson SJ, Farrell MJ, Egan GF. The impact of Alzheimer’s disease on the functional connectivity between brain regions underlying pain perception. Eur J Pain. 2011;15: e1-e11. | ||
Scherder EJ, Oosterman J, Swaab DF, et al. Recent developments in pain in dementia. BMJ. 2005;330:461-464. | ||
Ahn H, Horgas A. The relationship between pain and disruptive behaviours in nursing home residents with dementia. BMC Geriatr. 2013; 13:14. | ||
Bradford A, Shrestha S, Snow AL, et al. Managing pain to prevent aggression in people with dementia. Am J Alzheimers Dis Other Demen. 2012;27:41-47. | ||
Zwakhalen SM, Hamers JP, Abu-Saad HH, Berger MP. Pain in elderly people with severe dementia: a systematic review of behavioural pain assessment tools. BMC Geriatr. 2006;27:6:3. | ||
Herr K, Bjoro K, Decker S. Tools for assessment of pain in nonverbal older adults with dementia: a state-of-the-science review. J Pain Symptom Manage. 2006;31:170-192. | ||
Kovach CR, Logan BR, Noonan PE, et al. Effects of the Serial Trial Intervention on discomfort and behaviour of nursing home residents with dementia. Am J Alzheimers Dis Other Demen. 2006;21:147-155. | ||
Husebo BS, Ballard C, Sandvik R, Nilsen OB, Aarsland D. Efficacy of treating pain to reduce behavioural disturbances in residents of nursing homes with dementia: cluster randomised clinical trial. BMJ. 2011;343:d4064. | ||
Manfredi PL, Breuer B, Wallenstein S, Stegmann M, Bottomley G, Libow L. Opioid treatment for agitation in patients with advanced dementia. Int J Geriatr Psychiatry. 2003;18:700-705. | ||
Chibnall JT, Tait RC, Harman B, Luebbert RA. Effect of acetaminophen on behavior, well-being, and psychotropic medication use in nursing home residents with moderate-to-severe dementia. J Am Geriatr Soc. 2005;53:1921-1929. | ||
Buffum MD, Sands L, Miaskowski C, Brod M, Washburn A. A clinical trial of the effectiveness of regularly scheduled versus as-needed administration of acetaminophen in the management of discomfort in older adults with dementia. J Am Geriatr Soc. 2004;52:1093-1097. | ||
Sandelowski MJ, Barroso J. Classifying findings in qualitative studies. Qual Health Res. 2003;13:905-923. | ||
Allcock N, McGarry J, Elkan R. Management of pain in older people within the nursing home: a preliminary study. Health Soc Care Community. 2002;10:464-471. | ||
Abbey J, Piller N, De Bellis A, et al. The Abbey pain scale: a 1-minute numerical indicator for people with end-stage dementia. Int J Palliat Nurs. 2004;10:6–13. | ||
Warden V, Hurley AC, Volicer L. Development and psychometric evaluation of the Pain Assessment in Advanced Dementia (PAINAD) scale. J Am Med Dir Assoc. 2003;4:9-15. | ||
Kunz M, Scharmann S, Hemmeter U, Schepelmann K, Lautenbacher S. The facial expression of pain in patients with dementia. Pain. 2007;133:221-228. | ||
Regnard C, Reynolds J, Watson B, Matthews D, Gibson L, Clarke C. Understanding distress in people with severe communication difficulties: developing and assessing the Disability Distress Assessment Tool (DisDAT). J Intellect Disabil Res. 2007;51:277-292. | ||
Husebo BS, Ballard C, Cohen-Mansfield J, Seifert R, Aarsland D. The response of agitated behaviour to pain management in persons with dementia. Am J Geriatr Psychiatry. 2014;22:708-717. | ||
Hadjistavropoulos T, Voyer P, Sharpe D, Verreault R, Aubin M. Assessing pain in dementia patients with comorbid delirium and/or depression. Pain Manag Nurs. 2008;9:48-54. | ||
Wall S, White T. Pain and dementia – an application to practice: an example. Int J Older People Nurs. 2012;7:227-232. | ||
Pieper MJ, Achterberg WP, Francke AL, van der Steen JT, Scherder EJ, Kovach CR. The implementation of the serial trial intervention for pain and challenging behaviour in advanced dementia patients (STA OP!): a clustered randomized controlled trial. BMC Geriatr. 2011;11:12. | ||
Gregory J. Foundation of Nursing Studies. Identifying a pain assessment tool for patient with cognitive impairment Royal Bolton Hospital NHS Foundation Trust, 2011. Available from: http://www.fons.org/library/report-details.aspx?nstid=13188. Accessed July 16, 2014. | ||
Snow AL, O’Malley KJ, Cody M, et al. A conceptual model of pain assessment for noncommunicative persons with dementia. Gerontologist. 2004;44:807-817. | ||
Thompsell A, Hockley J. Achieving good end of life care for people with advanced dementia in care homes. Available from: http://www.bgs.org.uk/powerpoint/spr11/spr11thompsell_eolc.pdf. Accessed January 15, 2014. | ||
Treloar A. Assessing and managing distress and pain in severe dementia. Oxleas NHS Foundation Trust. Available from: http://www.dovehouse.org.uk/document.doc?id=805. Accessed May 7, 2013. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.