")
Back to Journals » Drug Design, Development and Therapy » Volume 12
Review of deutetrabenazine: a novel treatment for chorea associated with Huntington's disease
Received 6 December 2017
Accepted for publication 22 January 2018
Published 15 February 2018 Volume 2018:12 Pages 313—319
DOI https://doi.org/10.2147/DDDT.S138828
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Anastasios Lymperopoulos
Marissa Dean, Victor W Sung
Department of Neurology, Division of Movement Disorders, University of Alabama at Birmingham, Birmingham, AL, USA
Abstract: Deutetrabenazine was recently approved for the treatment of chorea in Huntington’s disease (HD) and is the first deuterated medication that has been US Food and Drug Administration (FDA)-approved for therapeutic use. In this article, we review deutetrabenazine’s drug design, pharmacokinetics, drug interactions, efficacy, adverse events, comparison with tetrabenazine, dosage, and administration. Deutetrabenazine is a deuterated form of tetrabenazine and is a vesicular monoamine transporter 2 (VMAT2) inhibitor. The substitution of deuterium for hydrogen at key positions in the tetrabenazine molecule allows a longer drug half-life and less frequent daily dosing. Deutetrabenazine is administered twice daily up to a maximum daily dose of 48 mg, which corresponds to a similar daily dose of 100 mg of tetrabenazine. In a Phase III clinical trial (First-HD), there was a statistically significant improvement of chorea in HD subjects, as well as improvements in global impression of change as assessed by both patients and clinicians. This improvement was seen without significant adverse effects as the overall tolerability profile of deutetrabenazine was similar to placebo. Somnolence was the most commonly reported symptom in the deutetrabenazine group. In a study where subjects converted from tetrabenazine to deutetrabenazine in an open-label fashion (ARC-HD) and indirect comparison studies between tetrabenazine and deutetrabenazine, there is a suggestion that while efficacy for chorea is similar, the data may slightly favor tetrabenazine, but adverse effects and tolerability strongly favor deutetrabenazine. These data have not been replicated in true head-to-head studies. Current evidence supports that deutetrabenazine is an effective therapeutic treatment option for chorea in HD and may provide a more favorable adverse effect profile than tetrabenazine. However, more data are needed, particularly in the form of head-to-head studies between deutetrabenazine and other treatment options as well as longer term clinical experience with deutetrabenazine.
Keywords: deutetrabenazine, tetrabenazine, Huntington’s disease, chorea
Introduction
Huntington’s disease (HD) is a hereditary neurodegenerative disorder that is caused by a trinucleotide CAG repeat expansion on chromosome 4 in the HTT gene, which encodes for the huntingtin protein.1 HD is characterized by motor disturbances, behavioral disturbances, and cognitive dysfunction, with the most common motor symptom being chorea.2 Up to 90% of patients with HD suffer from chorea that can interfere with daily function and may cause injury.3 For many years, there was no US Food and Drug Administration (FDA)-approved medication for the treatment of chorea, but in 2008, the FDA approved tetrabenazine for HD-associated chorea. Tetrabenazine is a vesicular monoamine transporter 2 (VMAT2) inhibitor and thus lowers the amount of monoamines at the synapse.4 In the clinical trial TETRA-HD, tetrabenazine was found to be effective for the treatment of chorea in HD; however, the side effect profile has limited its use in the HD population.3,4 Despite its effectiveness, controlled trials have found an increased risk of depression, suicidality, anxiety, akathisia, and parkinsonism in patients treated with tetrabenazine, among other tolerability issues.5
In April 2017, the FDA approved a second medication to treat chorea in HD, deutetrabenazine, which is a VMAT2 inhibitor structurally similar to tetrabenazine.6 Deutetrabenazine contains deuterium, which replaces hydrogen at key positions within the tetrabenazine molecule and prolongs plasma half-life, thus reducing fluctuations of drug levels in the plasma without altering protein-binding interactions.6 This allows less frequent and lower drug dosing, which results in a more favorable side effect profile. In First-HD, the adverse events were similar between the placebo and deutetrabenazine groups, further supporting this conclusion of minimal side effect risks.6 In separate clinical trials, both tetrabenazine and deutetrabenazine improved chorea associated with HD; however, there has been no head-to-head randomized controlled trial that has compared the effectiveness of these drugs against one another.4,6 In a recent article by Claassen et al,7 the authors indirectly compared the tolerability of tetrabenazine vs deutetrabenazine and concluded that deutetrabenazine had a more favorable adverse event profile. In the remainder of this article, we review deutetrabenazine drug development through clinical trials with discussion on drug design and pharmacokinetics, drug interactions, and the application of deutetrabenazine in treating chorea in HD.
Drug design and pharmacokinetics
Deuterium is a nontoxic form of hydrogen and has been incorporated into therapeutic drugs to slow liver metabolism for more than 50 years.8 The substitution of deuterium leads to a stronger carbon bond that is more difficult to cleave and increases the drug half-life without affecting protein-binding interactions of the drug.8 An increased drug half-life may result in a clinical benefit of decreased frequency of drug dosing, which may further improve patient adherence to medication administration. Despite the desirable properties of deuterium, deutetrabenazine is the first therapeutic deuterium-based drug to reach a Phase III study.9 Given the effectiveness of tetrabenazine on treating chorea in HD, it was postulated that the addition of deuterium would maintain this clinical benefit, while at the same time improving daily drug dosing, pharmacokinetics, and the side effect profile.
Deutetrabenazine is a reversible VMAT2 inhibitor, which preferentially depletes dopamine by inhibiting uptake into presynaptic vesicles.10,11 Densities of VMAT2 are highest in the caudate, putamen, and nucleus accumbens.12 Although the exact mechanism of how deutetrabenazine improves chorea through VMAT2 inhibition is not known, it is logical to suspect that the interaction within the caudate and putamen is directly related to the clinical effect.
Deutetrabenazine is extensively metabolized by the liver into two active metabolites, alpha-dihydrotetrabenazine (alpha-HTBZ) and beta-dihydrotetrabenazine (beta-HTBZ). When administered orally, at least 80% of deutetrabenazine is absorbed and the peak plasma concentrations (Cmax) of deuterated active metabolites are reached in 3–4 hours.13 When taken with food, there is a 50% increase in Cmax and, for this reason, it is recommended that deutetrabenazine should be administered with food. The half-life of deutetrabenazine is 9–10 hours, and the active metabolites are metabolized primarily by CYP2D6 before they are renally excreted. When compared with an equal oral dose of tetrabenazine, the half-life of deutetrabenazine was increased twofold (measured by active metabolites alpha- and beta-HTBZ concentrations in plasma).13 For patients with hepatic impairment or who are known poor CYP2D6 metabolizers, the effect of deutetrabenazine has not been specifically studied. However, in a clinical study evaluating the effects of hepatic impairment when taking tetrabenazine (which is a structurally similar VMAT inhibitor), there was up to 190-fold higher Cmax when compared with healthy controls. Therefore, it would be expected that a patient with hepatic impairment taking deutetrabenazine may have a similar increase in Cmax and require lower dosing when compared with healthy controls. In addition, although poor CYP2D6 metabolizers were not specifically studied, we would suspect that levels of alpha- and beta-HTBZ would increase in a similar manner that is seen while simultaneously taking strong CYP2D6 inhibitor drugs. Finally, after alpha- and beta-HTBZ are metabolized by CYP2D6, the metabolites are secreted renally; however, clinical studies have not evaluated the pharmacokinetic effect of deutetrabenazine in patients with renal impairment.
Drug interactions
The active metabolites of deutetrabenazine are substrates for CYP2D6; therefore, strong CYP2D6 inhibitors can affect drug levels of alpha- and beta-HTBZ. This effect was studied in 24 healthy subjects who took paroxetine (a strong CYP2D6 inhibitor) 8 days prior to deutetrabenazine. Systemic exposure (AUC) of alpha-HTBZ was increased by 1.9-fold and that of beta-HTBZ was increased by 6.5-fold in subjects taking paroxetine and deutetrabenazine, resulting in a total threefold increase of AUC for alpha- and beta-HTBZ. Half-life and Cmax were also increased for the active metabolites of deutetrabenazine. In summary, medications that are strong CYP2D6 inhibitors should be used with caution when taking deutetrabenazine, as the levels of alpha- and beta-HTBZ can be increased significantly. The effect of weak CYP2D6 inhibitors was not studied, so the potential drug interactions are not known, and caution should be taken when administering these drugs in combination with deutetrabenazine.
Efficacy and adverse events
The effectiveness of deutetrabenazine on treating HD-associated chorea was evaluated in a randomized, double-blind placebo-controlled, multicenter clinical trial, known as First-HD.6 Ninety ambulatory adults with manifest HD were enrolled in Huntington Study Group investigational sites in the USA and Canada. The diagnosis of manifest HD was made based on characteristic motor features and an expanded CAG repeat ≥36 in HTT. Patients were included if they had a Unified Huntington’s Disease Rating Scale (UHDRS) total maximal chorea score of ≥8 and a total functional capacity score of ≥5.15 Patients were excluded if they had a prolonged QTc interval, left bundle-branch block, hepatic impairment, renal impairment, serious untreated psychiatric illness, or significant impairment in speech or were taking drugs that prolong QT intervals (other than escitalopram or citalopram). Prior use of tetrabenazine was permitted, as long as it was not administered within the previous 6 months. Patients were randomized 1:1 to drug (deutetrabenazine) vs placebo and received a drug titration period of 8 weeks. They were maintained on the optimal dose for another 4 weeks, which was followed by a 1-week washout period.
The primary endpoint was the total change in maximal chorea, which was measured by the UHDRS. The maximal chorea score ranges from 0 to 28 and assesses seven different body regions. Each body region is rated from 0 (no chorea) to 4 (marked and prolonged), and the score for each body region is added up to form the maximal chorea score. At the starting of the study, each patient had a maximal chorea score of ≥8. The total maximal chorea score at the baseline visit was compared with the score during maintenance therapy (average of score from weeks 9 and 12 visits) to determine the change in total chorea score.
The study was powered for a treatment effect of −2.7 points on the UHDRS maximal chorea score, which was shown to be significant in the previous clinical trial with tetrabenazine.4 A sample size of 80 patients was predicted to give 90% power to detect a change of −2.7 points, and a total of 90 patients were included in this study. The primary outcome measure was met, as patients in the deutetrabenazine group had an average improvement of maximal chorea of −4.4 points, as compared to −1.9 points in placebo. This corresponded to a treatment difference of −2.5, which was statistically significant (95% CI, −3.7 to −1.3; P<0.001). However, the −2.7 point difference between groups that the study was powered to detect was not met and it is unclear whether the difference of −2.5 points is a clinically important difference in maximal chorea score, as there is no well-accepted guideline for this value. After the 1-week washout period, maximal chorea scores returned to baseline in the deutetrabenazine group, reinforcing that the improvement in chorea was due to drug effect.
There were four secondary endpoints in the study to assess the global impression of change, physical functioning, and change in balance. The Patient Global Impression of Change (PGIC) and the Clinical Global Impression of Change (CGIC) were considered successful if the response was “much” or “very much” improved. The 36-Item Short Form Health Survey (SF-36) physical functioning subscale score and Berg Balance Test were used to assess physical functioning and balance, respectively. It is important to note that anosognosia (unawareness of symptoms) is commonly seen in patients with HD, and this may affect the ability of patients to accurately report their symptoms.16 It is often suggested that due to anosognosia, HD patients are less aware of and therefore less bothered by their chorea than outside observers might imagine. For this reason, PGIC, in particular, would be a strong indicator of whether the −2.5 point change in maximal chorea seen in the study is truly clinically significant in the eyes of the patient. In First-HD, treatment success measured by both the PGIC and CGIC favored treatment with deutetrabenazine, which was statistically significant (P=0.002 in both). Therefore, both blinded clinicians and the blinded patients felt that those subjects taking deutetrabenazine were globally improved. In addition to support the clinical significance of the improvement in chorea score seen with deutetrabenazine, this may suggest that in spite of anosognosia, chorea in HD patients may have a greater impact on their daily life than previously thought. There was an improvement of physical functioning by SF-36 (P=0.03), but despite a trend toward improvement in the Berg Balance Test was not statistically significant (P=0.14) when comparing deutetrabenazine with placebo. This is likely explained by the fact that chorea, particularly when present in the legs and trunk, may interfere to some degree with gait, but other aspects of gait affected by HD (balance, coordination, dystonia, and so on) are not improved by deutetrabenazine to the same degree as chorea.
A number of other outcomes were evaluated, including other subscales of the UHDRS. Since worsening parkinsonism was reported as a side effect in tetrabenazine, the UHDRS subscale for parkinsonism was also evaluated. Interestingly, despite the shared VMAT2 inhibition primary mechanism of action of both deutetrabenazine and tetrabenazine, unlike what was seen in TETRA-HD, there was no significant difference between parkinsonism seen in the deutetrabenazine and placebo groups in First-HD. The total maximal dystonia score of the UHDRS was also evaluated and demonstrated a trend toward improvement in the deutetrabenazine group that did not meet statistical significance (P=0.02). The effect size of the improvement seen in the UHDRS total motor score was greater than the improvement of the total maximal chorea score, and some of that difference may be attributed to these subtle improvements in dystonia. The suggestion that deutetrabenazine may lead to the improvement of dystonia as well as chorea, without a worsening of parkinsonism in HD patients is extremely interesting and should be further investigated and validated in future studies.
Adverse effects overall were fairly similar between deutetrabenazine and placebo. The most commonly reported adverse event in the deutetrabenazine group was somnolence (five patients, or 11% of the treatment group vs 4% of the placebo group), which did improve with dose reduction. Given a central nervous system (CNS) active drug, the adverse events of somnolence are not surprising; however, this was the only individual neuropsychiatric adverse event that occurred with >7% of patients taking deutetrabenazine and there was no significant difference between deutetrabenazine and placebo on any individual neuropsychiatric adverse events. Harder to explain from a mechanism of action standpoint is the adverse effect of diarrhea, which was seen in four patients on deutetrabenazine but none in placebo patients. There was also an increase in weight in the deutetrabenazine group, with an average increase in the BMI of 0.6 (compared to −0.1 average weight loss in the placebo group). A likely explanation for this weight gain is the improvement of chorea and swallowing function, which can lead to decreased energy expenditure and increased calorie consumption.
There was one patient with serious adverse events who experienced both cholecystitis and agitated depression. Despite this one episode of agitated depression, there was no significant worsening of depression in the deutetrabenazine group when compared with the placebo group. Suicidal ideation was reported by one person in each group, and the significance of this is unclear, as suicidal ideation can occur as a behavioral manifestation of HD itself. That neither depression nor suicidal ideation was worse than in the placebo group is important, given that both of those are already problematic in HD patients. Having a treatment option in HD with no statistical risk of worsening depression or suicidality (and with an overall safety profile that is similar to placebo) is a valuable addition to the treatment armamentarium. It is important to note that despite the lack of statistical worsening of depression and suicidality, deutetrabenazine still has a boxed warning for depression and suicidality. These are critical issues in the treatment of HD patients, and deutetrabenazine is still a VMAT2 inhibitor. VMAT2 inhibitors in the past have a record of causing worsening depression and suicidality. Given the VMAT2 inhibition mechanism, an adverse effect that is conspicuously absent is parkinsonism, which was not seen with deutetrabenazine in First-HD. It will be interesting to watch for the future publication of open-label extension data as well as real-world data of commercial use of deutetrabenazine to know whether the low adverse effect profile, particularly as regards depression and suicidality, remains so favorable with time.
In conclusion, First-HD demonstrates statistically significant improvement of chorea in HD that helped both patients and clinicians to feel that patients were globally improved with the administration of deutetrabenazine. The drug also showed a favorable side effect profile that is overall similar to placebo and specifically has no statistical worsening of depression/suicidality, though deutetrabenazine maintains a boxed warning for both. The maximal efficacy and improved safety profile was attributed to the unique pharmacokinetic profile of deutetrabenazine, which enables comparable systemic exposure at lower doses, lower peak concentrations, and reduced plasma fluctuations.14 Future studies will need to assess whether there is a sustained improvement of chorea for >12 weeks and if the side effect profile changes with continued exposure to deutetrabenazine.
Deutetrabenazine vs tetrabenazine
As stated previously, there has been no head-to-head evaluation of deutetrabenazine vs tetrabenazine for the treatment of chorea in HD. However, there are similarities between the Phase III clinical trials that evaluated either tetrabenazine (TETRA-HD)or deutetrabenazine (First-HD) vs placebo for the treatment of HD-associated chorea, so it may be reasonable to compare the results of these studies. Both TETRA-HD4 and First-HD6 studies were designed by the same study consortium (the Huntington Study Group), and the methods were very similar. The inclusion criteria for TETRA-HD required slightly worse maximal chorea scores on the UHDRS (≥10) when compared with First-HD (≥8), but otherwise, the inclusion and exclusion criteria were very similar between the two studies. The randomization also differed between the two groups, with a 2:1 randomization in TETRA-HD and a 1:1 randomization in First-HD. In TETRA-HD, this allowed more patients to be placed on the study drug and, therefore, led to an assessment of more patients taking tetrabenazine. The titration phase (8 weeks), maintenance phase (4 weeks), and 1-week washout period were the same in both trials.
The efficacy of deutetrabenazine vs tetrabenazine in treating HD-associated chorea was recently evaluated by comparing First-HD and TETRA-HD trials.17 In this comparison, deutetrabenazine and tetrabenazine had mild effects on chorea when compared with placebo, but neither differed significantly when compared with each other. The actual UHDRS point reduction was higher in TETRA-HD (5 points) than in First-HD (4.4 points), but the amount of change that occurred when compared with placebo was not different when comparing the two studies. In addition, there was no significant difference in the UHDRS total motor score when comparing TETRA-HD with First-HD. Overall, based on this indirect comparison, tetrabenazine may have a slightly higher impact on the improvement of chorea, but both deutetrabenazine and tetrabenazine show an improvement of chorea when compared with placebo.
Additionally, the authors of First-HD performed a study titled ARC-HD, and in one portion of the study, patients were entered to the study on a stable dose of tetrabenazine and were allowed to switch to deutetrabenazine in an open-label fashion.18 Though the goal of this study was to show that patients could switch from tetrabenazine to deutetrabenazine safely without loss of efficacy from a chorea standpoint, the efficacy and safety data could also be used as an indirect comparison between the two drugs as the same patients will have taken both drugs. There were 37 patients enrolled in this study, and each patient switched overnight from tetrabenazine to deutetrabenazine in ~2:1 conversion. There was no reported worsening of chorea after the switch was made, and after 1 week, the investigator was given the option to increase deutetrabenazine further if chorea was still present. The maximum dose of deutetrabenazine that was permitted was 72 mg/day. Prior to entry to the study, patients were to be on a stable dose of tetrabenazine with relative chorea control and the average tetrabenazine dose at study entry was 37.5 mg/day. At the initial overnight switch, the average deutetrabenazine daily dose was 18 mg (approximately half of 37.5 mg); however, after 4 weeks, the average daily dose was 30 mg and after 8 weeks, the average dose was 36 mg. This raises a further question as to why patients required much higher doses of deutetrabenazine when compared with tetrabenazine (~1:1 ratio at 8 weeks following the overnight switch). Since the UHDRS total maximal chorea score improved from weeks 1 to 8 by an average of 1.4 points, this suggests that there was further improvement of chorea with dose adjustments. One interpretation of this finding is that patients entering the study did not have quite the chorea control that they could have had due to dose-limiting side effects of tetrabenazine and that the favorable tolerability of deutetrabenazine allowed further titration to better chorea control. However, the UHDRS total motor score was not significantly different from weeks 1 to 8, with an average improvement of 0.3 points. Though not discussed in the article, something to be explored further would be whether the suggested 2:1 ratio switch from tetrabenazine to deutetrabenazine may be underdosing a bit as patients seemed to require much higher doses of deutetrabenazine than would be predicted by the 2:1 conversion ratio.
Drug adherence was high in ARC-HD, and the authors attributed this to the twice daily dosing of deutetrabenazine compared to the three times daily dosing of tetrabenazine. Adverse events were also evaluated in this study, and similar results were found as were previously reported in First-HD. Somnolence was the most common adverse event (nine patients), and there were two patients who reported mild depression. As in First-HD, there was no parkinsonism or suicidality seen in this study. This study was not blinded, so the results are to be interpreted with caution, but it at least serves as some confirmation of the favorable safety profile of deutetrabenazine seen in First-HD. Important to note is that in ARC-HD, this favorable safety profile was maintained up to the allowed 72 mg/day, which is above the FDA-recommended maximum of 48 mg/day.
Recently, there was also an indirect tolerability comparison between deutetrabenazine and tetrabenazine that specifically compared patient outcomes and adverse events in the TETRA-HD and First-HD clinical trials.7 Indirect analysis demonstrated statistically significant overall lower adverse event incidence (as well as lower moderate and severe adverse event incidence) with deutetrabenazine when compared with tetrabenazine. There was a slightly increased risk of mild adverse events with deutetrabenazine, but this was not statistically significant. Overall dose reductions and suspensions due to an adverse event were lower in deutetrabenazine when compared with tetrabenazine in all comparisons (P<0.001). These results support the conclusion that deutetrabenazine has a more favorable benefit–risk ratio when compared with tetrabenazine. This may be related to the unique properties of deuterium that allows a longer half-life with modest change in Cmax and, thus, less daily fluctuations in drug levels. It should be noted, however, that TETRA-HD and First-HD were short clinical trial studies and further analysis of the side effect profile for deutetrabenazine needs to be evaluated in longer clinical trials.
Dosage and administration
Deutetrabenazine is administered twice daily, once in the morning and once in the evening. Twice daily dosing is more favorable than three times a day dosing, which is often required for tetrabenazine, and this may lead to improved patient adherence. Each dose is given with food, as there is an associated increase in Cmax of the active metabolites of deutetrabenazine when administered with food. Deutetrabenazine is dispensed as tablets that come in the following three strengths: 6, 9, and 12 mg. Each patient starts with 6 mg daily and titrates upward by 6 mg/week until either chorea has improved or the total dose reaches 96 mg/day (48 mg twice daily). If the patient is also taking a strong CYP2D6 inhibitor or is a poor CYP2D6 metabolizer, the daily dose should not exceed 36 mg and the maximum single dose is 18 mg. If the patient is switching from tetrabenazine to deutetrabenazine, the change can be made the following day (specific instructions are provided in the Austedo package insert). The dose of deutetrabenazine will be approximately half the dose of tetrabenazine. This dose conversion was supported by the observation that an equal dose of tetrabenazine and deutetrabenazine resulted in a near doubling of the half-life in deutetrabenazine.14 However, as earlier, results from ARC-HD suggest that a higher ratio may be needed when converting from tetrabenazine to deutetrabenazine. A higher overnight switch ratio was not evaluated in this study, and a study with a higher deutetrabenazine-to-tetrabenazine ratio would be interesting from a safety and efficacy standpoint to know whether efficacy is further improved without sacrificing the favorable safety profile that has been seen in studies thus far.18
Conclusion
Deutetrabenazine is the first FDA-approved deuterated medication, and the benefits of deuterium can be seen with less frequent daily dosing and a more favorable side effect profile. Current evidence supports that deutetrabenazine is an effective therapeutic treatment option for chorea in HD with a side effect profile similar to placebo (Table 1). Real-world studies with deutetrabenazine validating the favorable adverse effect profile seen in clinical trials would be valuable to further support the utility of this medication for the treatment of chorea in HD. In limited data available so far, both tetrabenazine and deutetrabenazine produce a statistically significant improvement in chorea compared to placebo, with perhaps a slightly greater magnitude of effect in tetrabenazine. Adverse effect profile strongly favors deutetrabenazine over tetrabenazine, though none of this has been validated by true head-to-head studies, which will be needed to truly compare deutetrabenazine to other treatment options for chorea in HD.
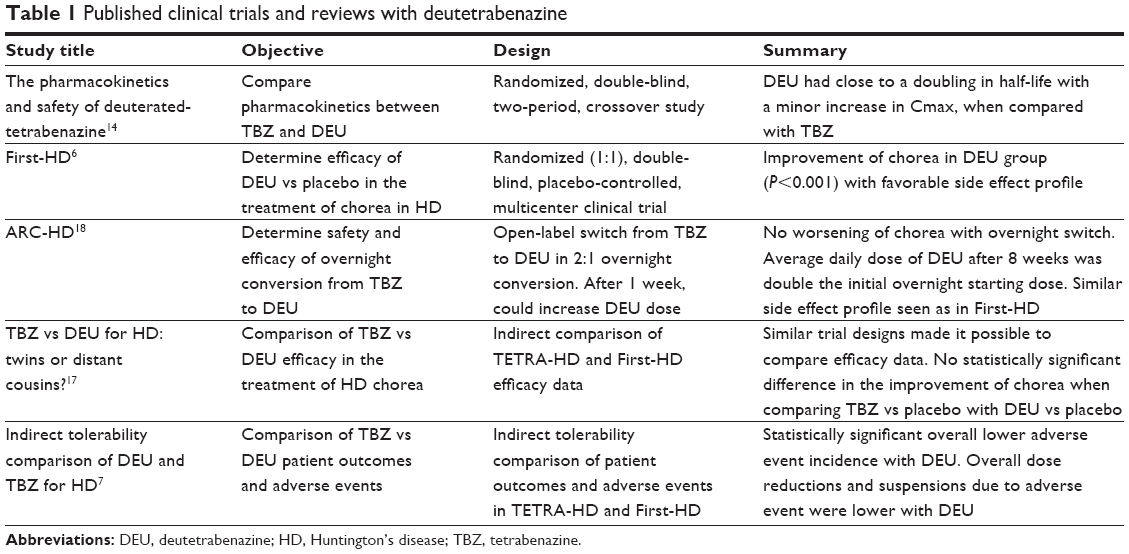 | Table 1 Published clinical trials and reviews with deutetrabenazine |
Author contributions
MD drafted and revised the manuscript and analyzed and interpreted the data, study concept, and design. VWS revised the manuscript and analyzed and interpreted the data, and participated in study concept and design. Both authors contributed toward data analysis, drafting and revising the paper and agree to be accountable for all aspects of the work.
Disclosure
VWS has served as a consultant to Lundbeck and Teva. MD reports no conflicts of interest in this work.
References
[No authors listed] A novel gene containing a trinucleotide repeat that is expanded and unstable on Huntington’s disease chromosomes. The Huntington’s Disease Collaborative Research Group. Cell. 1993;72(6):971–983. | ||
Huntington G. On chorea. George Huntington, M.D. J Neuropsychiatry Clin Neurosci. 2003;15(1):109–112. | ||
Jankovic J, Roos RA. Chorea associated with Huntington’s disease: to treat or not to treat? Mov Disord. 2014;29:1414–1418. | ||
Huntington Study Group. Tetrabenazine as antichorea therapy in Huntington disease: a randomized controlled trial. Neurology. 2006;66(3):366–372. | ||
Yero T, Rey JA. Tetrabenazine (Xenazine), an FDA-approved treatment option for Huntington’s disease-related chorea. P T. 2008;33:690–694. | ||
Huntington Study Group, Frank S, Testa CM, et al. Effect of deutetrabenazine on chorea among patients with Huntington disease: a randomized clinical trial. JAMA. 2016;316:40–50. | ||
Claassen DO, Carroll B, De Boer LM, et al. Indirect tolerability comparison of deutetrabenazine and tetrabenazine for Huntington disease. J Clin Mov Disord. 2017;4:3. | ||
Shao L, Hewitt MC. The kinetic isotope effect in the search for deuterated drugs. Drug News Perspect. 2010;23:398–404. | ||
Gant TG. Using deuterium in drug discovery: leaving the label in the drug. J Med Chem. 2014;57:3595–3611. | ||
Scherman D, Jaudon P, Henry JP. Characterization of the monoamine carrier of chromaffin granule membrane by binding of [2-3H]dihydrotetrabenazine. Proc Natl Acad Sci U S A. 1983;80:584–588. | ||
Bagchi SP. Differential interactions of phencyclidine with tetrabenazine and reserpine affecting intraneuronal dopamine. Biochem Pharmacol. 1983;32:2851–2856. | ||
Scherman D, Raisman R, Ploska A, Agid Y. [3H]dihydrotetrabenazine, a new in vitro monoaminergic probe for human brain. J Neurochem. 1988;50:1131–1136. | ||
Austedo (TM) (deutetrabenazine) [package insert] North Wales, PA, Teva Pharmaceuticals, USA, Inc.; 2017. | ||
Stamler D, Bradbury M, Brown F. The pharmacokinetics and safety of deuterated-tetrabenazine (P07.210). Neurology. 2013;80(7 suppl):765. | ||
Unified Huntington’s Disease Rating Scale: reliability and consistency. Huntington Study Group. Mov Disord. 1996;11(2):136–142. | ||
McCusker E, Loy CT. The many facets of unawareness in Huntington Disease. Tremor Other Hyperkinet Mov (N Y). 2014;4:257. | ||
Rodrigues FB, Duarte GS, Costa J, Ferreira JJ, Wild EJ. Tetrabenazine versus deutetrabenazine for Huntington’s disease: twins or distant cousins? Mov Disord Clin Pract. 2017;4(4):582–585. | ||
Frank S, Stamler D, Kayson E, et al. Safety of converting from tetrabenazine to deutetrabenazine for the treatment of chorea. JAMA Neurol. 2017;74(8):977–982. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.