")
Back to Journals » Open Access Journal of Contraception » Volume 12
Resilient and Accelerated Scale-Up of Subcutaneously Administered Depot–Medroxyprogesterone Acetate in Nigeria (RASuDiN): A Mid-Line Study in COVID-19 Era
Authors Osinowo K , Sambo-Donga F, Ojomo O , Ibitoye SE , Oluwayemi P, Okunfulure M, Ladipo OA, Ekholuenetale M
Received 23 June 2021
Accepted for publication 11 November 2021
Published 2 December 2021 Volume 2021:12 Pages 187—199
DOI https://doi.org/10.2147/OAJC.S326106
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Igal Wolman
Kehinde Osinowo,1 Fintirimam Sambo-Donga,1 Oluwaseun Ojomo,1 Segun Emmanuel Ibitoye,1 Philip Oluwayemi,1 Morounfola Okunfulure,1 Oladapo Alabi Ladipo,1 Michael Ekholuenetale1,2
1Association for Reproductive and Family Health, Trade and Convention Center, Abuja, Nigeria; 2Department of Epidemiology and Medical Statistics, Faculty of Public Health, College of Medicine, University of Ibadan, Ibadan, Nigeria
Correspondence: Kehinde Osinowo Email [email protected]
Background: Injectable contraceptives are fast becoming the method of choice among women in sub-Saharan Africa (SSA). Specifically, the subcutaneously administered depot–medroxyprogesterone acetate (DMPA-SC) is gaining traction as a convenient, private and effective method to address unmet need for family planning (FP). The objective of this study was to determine the trend in DMPA-SC use in Nigeria.
Methods: Data was extracted from the National Health Management Information System (NHMIS) FP register on DMPA-SC uptake in public health facilities and through community-oriented resource providers (CORPS) in 10 Nigerian states. The linear trend model was adopted in data analysis based on lowest measure of dispersion and/or highest adjusted coefficient of determination (R2). The statistical significance was determined at 5%.
Results: There was an upward trend in the use of DMPA-SC among clients who received the service through health providers, CORPS and self-injection in the 10 project states over a period of 12 months (August 2019–July 2020). In addition, the linear trend model showed that for every unit increase in months, the average number of women expected to use DMPA-SC through health providers, CORPS and self-injection will increase by 1308.3 (Yt = 3799.7 +1308.3*t), 756.73 (Yt = − 1030.8 +756.73*t) and 77.864 (Yt = − 159.7 +77.864*t) respectively. In all models, the adjusted coefficient of determination was 99.9% which showed good model fitness. The results also showed that the number of DMPA-SC clients varied across the project states with Niger (32,988) and Oyo (31,511) states reporting the highest number of clients over the period of 12 months.
Conclusion: There was an increasing use of DMPA-SC and self–injection among clients over time. Health facility and community-based FP programs should be strengthened to ensure improved access to FP services.
Keywords: family planning, contraceptive, Nigeria, DMPA-SC, self-injection, birth control
Introduction
Family planning (FP) has age-long benefits in maternal and infant mortality reduction.1 In resource-poor settings, 214 million women of childbearing age had an unmet need for FP.2 Though the FP2020 global partnership set an ambitious goal to reach more than half of these women with voluntary FP,3 yet achieving this goal was practically impossible. Many factors have continued to hamper contraceptive use, such as: experiences of side effects, cost, method dissatisfaction, convenience, limited method options and intimate partner disapproval.4,5 In addition, home, community and health institutions structure have placed limits on women’s ability to take fertility control decision. For example, cultural, normative, societal and financial concerns as well as the requirement for partner’s permission to access services, religious leaders’ subtle and overt pushes to employ traditional FP methods, and out-of-pocket costs are major barriers.5
In Nigeria, the prevalence of modern contraceptive use was 14.2%.6 According to Nigeria Demographic and Health Survey (NDHS), the use of modern contraceptive method was higher among sexually active unmarried women (28%) than among married women (12%). Among currently married women, the prevalence of contraception, regardless of method, was 17%.7 In the five years prior to the survey, two out of every five women (41%) who started using a contraceptive method stopped within a year, indicating large discontinuation rate. While the desire to become pregnant was the most common reason for discontinuance (35%). Sexually active unmarried women had a larger unmet need for FP (48%) than currently married women (19%).7
Considering the challenges in achieving global, regional, national and sub-national contraceptive use targets, adding another voluntary contraceptive option to the method mix will help women to properly time and space their pregnancies for the healthiest and safest outcomes. Subcutaneously administered depot-medroxyprogesterone acetate (DMPA-SC) is a contraceptive injectable formulation that provides women with another voluntary FP option.8 It offers favourable characteristics such as cost and time savings. It has the potential not only to be administered by a range of health care cadres, but can be self-injected.
The Government of Nigeria pledged to achieve modern contraceptive prevalence rate (mCPR) target of 27% by 2020.9 To accelerate the progress toward that goal, DMPA-SC (brand name Sayana Press) was introduced to the contraceptive method mix in 2015.10 DMPA-SC is seen as a valuable innovation in FP. Compared with other contraceptive methods, the benefits of DMPA-SC include ease of use, few side effects, quick administration, less pain and greater effectiveness.10–13 Injectable contraceptives are increasingly popular in Nigeria (as many other African countries) due to their effectiveness, privacy and convenience.14 DMPA-SC has been paired with an all-in-one syringe (Uniject),13 creating a single, easy-to-use and acceptable product.15,16 It has been heralded as a possible “game changer” for FP, due to its easy administration by paraprofessionals like junior community health extension workers, community-based distributors, proprietary and patent medical vendors (PPMVs), or by self-injection.13
This study is being conducted in coronavirus disease 2019 (COVID-19) era. The first case of COVID-19 was reported in Wuhan, China, on December 8, 2019.17 On December 31, 2019, Chinese health authorities contacted the World Health Organization (WHO), which declared the outbreak a Public Health Emergency of International Concern by January 30, 2020.18 Due to its high spread and mortality across many countries, COVID-19 was declared a pandemic on March 11, 2020.19 The impact of COVID-19 on sexual and reproductive health was worrisome.20 The lack of contraceptive drugs and devices as a result of supply chain disruption was one of the most significant impediments to access.21 In Nigeria, clients were hesitant to visit health facilities for FP commodity uptake. Interestingly, the implementation of resilient and accelerated scale-up of DMPA-SC in Nigeria (RASuDiN) coincided within the COVID-19 era. The project has a community component used to reach clients who are unwilling or unable to visit health facilities due to COVID-19. Also, it was crucial in expanding FP method choice, an indication of the potential for contraceptive use and scale-up in Nigeria. The objective of this study was to examine the trend in DMPA-SC use across selected Nigerian states.
Methods
Study Context
The study location is Nigeria, the most populous country in Africa with a population of 191 million.22 Nigeria has a weak health delivery system that contributes to adverse maternal health outcomes,23,24 including failure in birth control programs. Moreover, the health delivery system in Nigeria is grossly underfunded.25 The national indices of maternal health, particularly in the use of vital healthcare services is among the poorest in the world.26 In the 5 years preceding the 2018 Nigeria Demographic and Health Survey (NDHS), modern contraceptive use was about 28% among sexually active unmarried women and 12% among currently married women. The unmet need for FP was 48% among sexually active unmarried women and 19% among currently married women.7 These show that the use of contraceptive methods was low, worrisome and needs improvement.
To achieve the 27% mCPR, the Nigerian government developed; a) National Communication Plan (2017–2020); b) national guideline and training manuals for the introduction and scale-up of DMPA-SC self-injection (2019); c) manual for the Training of Doctors, Nurse/Midwives and Community Health Extension Workers on Postpartum Family Planning (2016); and d) task shifting/task sharing policy for essential health care services in Nigeria as well as the standard of practice (SOP). The implementation of these programs could in no small measure enhance contraceptive use in Nigeria. In 2017, the Federal Ministry of Health led the development of the Strategic Plan for DMPA-SC introduction and scale-up, a roadmap for expanding access and accelerating progress toward Nigeria’s National FP blueprint (scale-up plan). As part of the strategic plan development process, the ministry – with technical support from the Health Policy Plus project (funded by the US Agency for International Development) and the Technical Support Unit project (funded by the Bill & Melinda Gates Foundation) – applied a new DMPA-SC Impact Model to quantify the potential FP programmatic impact and cost implications of DMPA-SC introduction and scale-up in Nigeria by 2021.
Study Design
We used time series data collected retrospectively from health clinic encounter between August 2019 and July 2020 across the RASuDiN project states. The National Health Management Information System (NHMIS) FP Register was used to capture client information at the health facilities. The data was extracted over a period of 12 months to determine the trend of DMPA-SC uptake in public health facilities in Anambra, Delta, Enugu, Kwara, Lagos, Niger, Ogun, Oyo, Plateau and Rivers states. Association of Reproductive and Family Health (ARFH) is the principal recipient of the grant and manages the project data.
Project Description
In 2016, the Federal Ministry of Health, Nigeria authorized the introduction of DMPA-SC in health facilities. Nurses and midwives administered DMPA-SC at health facilities, adding to their routine FP service provision. In the commencement of the RASuDiN project in 2018, healthcare service providers and community-oriented resource providers (CORPS) were trained on DMPA-SC. This was similar to a previous approach where community health workers and facility-based health care providers in Benin were trained to administer DMPA-SC safely and effectively in 10 health zones.27 Community-based DMPA-SC service delivery is becoming popular, particularly among new users of contraception and could help the country achieve its FP goals. Table 1 has the details of the project Nigerian states, number of Local Government Areas (LGAs) per state and the number of public health facilities (primary, secondary and tertiary) in each state.
 |
Table 1 Study Sites of RASuDiN Project |
Data Collection and Reporting Approach
The data was collected across all intervention health facilities in the 10 RASuDiN project states (Anambra, Delta, Enugu, Kwara, Lagos, Niger, Ogun, Oyo, Plateau and Rivers). These include both those reporting on District Health Information System (DHIS) or otherwise. At community level, each CORPs on the RASuDiN project was attached to a health facility where their service delivery data are entered into the NHMIS FP register. The facility FP providers in turn collates the entire data (both health facility and CORPs contributions) and transmit it to the Local Government Area (LGA) Reproductive Health (RH)/FP supervisor who in turn sends it to the LGA Monitoring and Evaluation (M&E) officer for upload on the National DHIS2 platform after quality control checks. Data is transmitted by the facility FP provider to the LGA RH/FP coordinator every month.
Health facilities from each state conduct data collation and validation review meetings before reporting on the DHIS instance. Similarly, the LGA RH/FP supervisors conduct monthly review meetings with CORPs to collate and validate community-level service delivery at the health facilities where they are linked before transmission to the LGA M&E officers. Data recorded in the NHMIS FP register is verified against data recorded in the Monthly Summary Form, Referral Forms and the CORPs Data Entry Form. The LGA M&E Officers transmit the data to the National DHIS system. The LGA RH/FP supervisors conduct monthly review meetings with CORPs in all the 217 LGAs in the 10 implementing project states. The supervisors also ensure completeness and timely submission of monthly reports.
Outcome Variable
The new acceptors and revisits for DMPA-SC (health facility provider-administered, CORPS-administered and self-injection) were measured in the 10 RASuDiN project states (Anambra, Delta, Enugu, Kwara, Lagos, Niger, Ogun, Oyo, Plateau and Rivers). In addition, the number of health clinics providing DMPA-SC for each month was determined across the project states.
Ethical Approval
Ethical approval was obtained from National Health Research Ethics Committee (NHREC) of Nigeria – Protocol approval number: NHREC/01/01/2007-17/10/2018. In addition, permission was obtained from individual State Ministry of Health to conduct the research.
Statistical Analysis
The total number of clients who received DMPA-SC through health facility staff, CORPS and self-injection were summarized in counts. Time series analysis approach was used to determine the trend of DMPA-SC uptake over a 12-month period; August 2019 through July 2020. The linear trend model was adopted due to lowest measure of dispersion and/or highest adjusted coefficient of determination (R2). This approach follows the method adopted by previous authors.28 Statistical significance was determined at 5%. Data analysis was conducted using Minitab version 17.0. Minitab provides user-friendly approach for time series modeling and forecasting. It provides several statistical models, and graphical tools that make results on time series analysis simpler.
Results
Trend Analysis for Health Facility Providers’, CORPS-Administered and Self-Injection DMPA-SC Clients
In Figure 1, the use of DMPA-SC showed an upward trend among clients who received the service through health facility staff in the 10 RASuDiN project states over a period of 12 months (August 2019 – July 2020). See Figure 1 below for the details.
 |
Figure 1 Count of DMPA-SC clients who received the method through health facility providers. |
Table 2 showed the reported number of facility clients, the predicted number of facility clients and the residual. Based on the linear trend model (Yt = 3799.7 +1308.3*t), for every unit increase in months, the average number of women expected to receive DMPA-SC will increase by 1308.3. The adjusted coefficient of determination was 99.9% which showed very good model fitness.
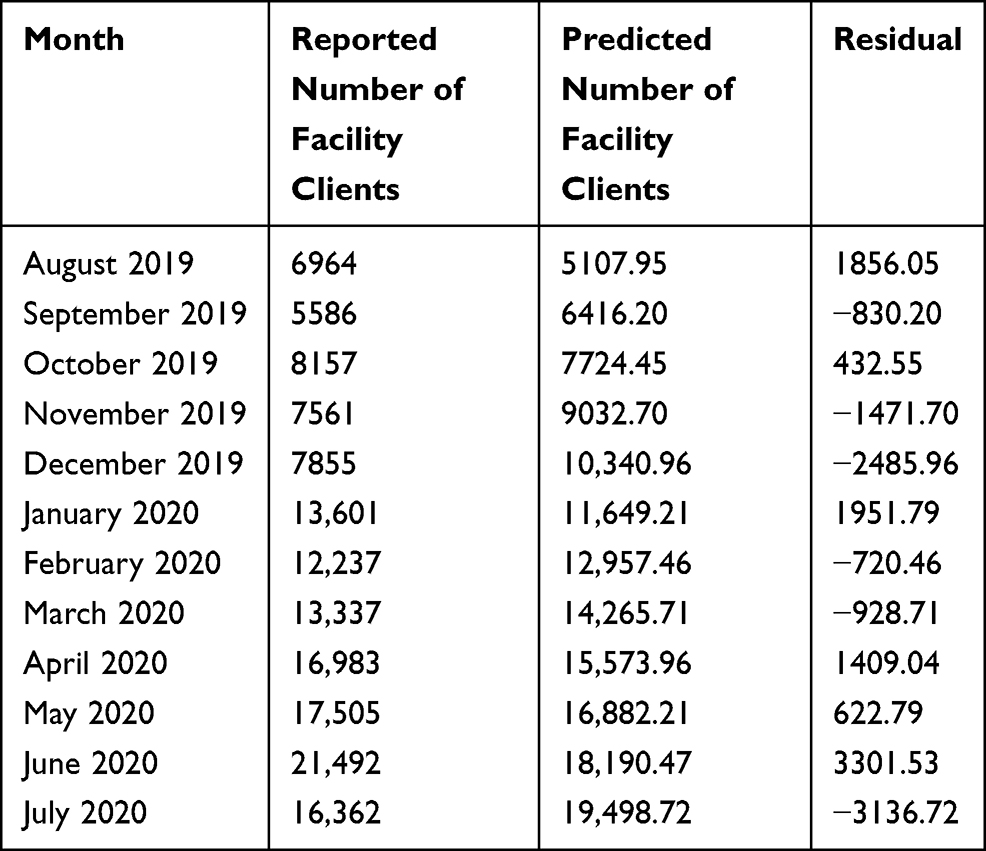 |
Table 2 Time Series Analysis of DMPA-SC Clients Who Received the Method Through Health Facility Providers |
Linear Trend Equation: Yt = 3799.7 +1308.3*t.
Adjusted R2= 99.9%.
Based on Figure 2 results, there was an upward trend in the use of DMPA-SC among clients who received the service through CORPS in the 10 RASuDiN project states over a period of 12 months (August 2019 – July 2020). See Figure 2 for the details.
 |
Figure 2 Count of DMPA-SC clients who received the method through CORPS. |
The results showed reported number of CORPS clients, the predicted number of CORPS clients and the residual. Based on the linear trend model (Yt = −1030.8 +756.73*t), for every unit increase in months, the average number of women expected to received DMPA-SC through CORPS will increase by 756.73. The adjusted coefficient of determination was 99.9% which showed very good model fitness. See Table 3 for the details.
 |
Table 3 Time Series Analysis of DMPA-SC Clients Who Received the Method Through CORPS |
Linear Trend Equation: Yt = −1030.8 +756.73*t.
Adjusted R2= 99.9%.
Figure 3 showed the use of DMPA-SC had an upward trend among clients who self-injected in the 10 RASuDiN project states over a period of 12 months (August 2019 – July 2020). See Figure 3 below for the details.
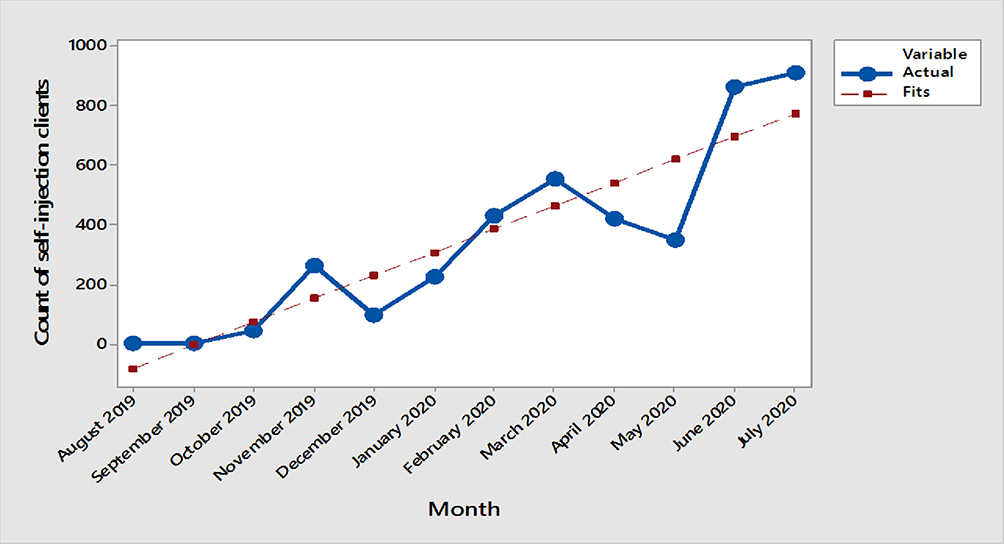 |
Figure 3 Count of DMPA-SC clients who can self-inject. |
In Table 4, we presented the reported number of self-injection clients, the predicted number of self-injection clients and the residual. Based on the linear trend model (Yt = −159.7 +77.864*t), for every unit increase in months, the average number of women expected to receive DMPA-SC will increase by 77.864. The adjusted coefficient of determination was 99.9% which showed very good model fitness.
 |
Table 4 Time Series Analysis of DMPA-SC Self-Injection Clients |
Linear Trend Equation: Yt = −159.7 +77.864*t.
Adjusted R2= 99.9%.
Service Delivery Points Providing DMPA-SC in RASuDiN Project States; August 2019–July 2020
In Table 5, the number of DMPA-SC delivery points were summarized in counts across project states and over time (August 2019 through July 2020). The total number of service delivery points was highest in Delta State (n= 4583), followed by Enugu State (n= 4086) and Oyo State (n= 4006). However, Plateau State had the least service delivery points (n= 864). The total number of service delivery points across the ten project states was 30,797. Notably, the number of DMPA-SC delivery points which reported data increased over time from August 2019 to July 2020. See Table 5 for the details.
 |
Table 5 Number of Service Delivery Points Providing DMPA-SC in RASuDiN Project States, Nigeria; August 2019–July 2020 |
Utilization of DMPA-SC in Nigeria Across Project States for 12 Months
In Table 6, we showed the number of new acceptors and revisits of DMPA-SC clients who received the method through health facility staff and CORPS respectively, across RASuDiN project states and over a period of 12 months (August 2019 – July 2020). In addition, we presented the total number of clients (new acceptors and revisits) who received DMPA-SC across RASuDiN project states and over 12 months. In sum, the number of clients who received DMPA-SC increased as time increases. The results also showed that the number of DMPA-SC clients varied across the project states with Niger (32,988) and Oyo (31,511) states reporting the highest number of clients. See Table 6 for the details.
 |
Table 6 Utilization of DMPA-SC in RASuDiN Project States, Nigeria; August 2019–July 2020 |
Discussion
To the best of our knowledge, this is the foremost study to measure the trend of provider-administered and self-injection of DMPA-SC in Nigeria. The results showed an upward trend in the use of DMPA-SC across the project states. This initial success of the RASuDiN project shows promise to help in the contribution to meet the country’s FP commitment. After 12 months of implementation, the RASuDiN project seems to hold a greater promise by reaching about 194,295 women in 10 Nigerian states. In previous studies, all countries experienced a sizeable increase in the use of DMPA. About 7,997 women chose DMPA-SC after 13 months of implementation in the Republic of Benin.27 Approximately 14,273 units of DMPA-SC provided by Reproductive Health Uganda clinics, mobile outreach teams and village health teams over a period of 12 months were utilized.8 Furthermore, in the results from pilot introduction of DMPA-SC in 4 African countries to expand the range of contraceptive methods available to women, Niger reported 43,801, Senegal reported 120,861, Uganda reported 130,673 and Burkina Faso reported 194,695 DMPA-SC users over a period of 12 months.29 The increased uptake of DMPA has been consistent in various African countries.
The findings of this study is evidence that the Strategic Plan for the introduction and scale-up of DMPA-SC by the Federal Ministry of Health to fully scale-up DMPA-SC across all 36 Nigerian states and the Federal Capital Territory by 2021 may have already been operationalized in the study locations. The plan was to ensure that all eligible providers across public and private sectors are trained on DMPA-SC service provision, counselling and self-injection. Moreover, the village health workers are to serve as public sector community-level providers of DMPA-SC, pharmacies and Patent and Proprietary Medicine Vendors (PPMVs) would be able to legally stock and administer DMPA-SC and the junior community health extension workers would provide the service too.30 The findings are consistent with the results of previous studies which found an upward trend in modern contraceptive use over time especially among young women.31,32
The upward trend could be due to changes in contraceptive use behaviour through increased awareness creation. In a previous study, about two-thirds of the increase in modern contraceptive use was due to change in contraceptive use behaviour.33 Most importantly, the increased number of clients over time could be due to the changes in contraceptive use behaviour among the rural population and among religious women as a result of gatekeepers’ buy-in for the project.31 Decision makers or gatekeepers involvement in FP could be a major motivator for women’s uptake of contraceptive.33 In our project, DMPA-SC is only a method mix to other FP commodities and clients are able to make their choice. A previous study on DMPA-SC in Nigeria reported many users choose DMPA-SC due to recommendations from providers and friends, and the experience of less side effects.34 Proper counselling is a determining factor for contraceptive methods use in general and DMPA-SC uptake in particular.10 In RASuDiN project, clinicians/nurses and CORPS conduct counselling at health facilities and at communities as directed in national guideline.
Another possible reason for the upward trend could be the availability of commodities across the project states. Since the DMPA-SC introductory program in Nigeria, distribution of commodity has been amplified especially to high volume providers and high demand settings.34 Moreover, community-based distribution has been an effective service delivery model for the hard-to-reach, most-at-risk of unmet need for FP and the key population such as the young and unmarried users. Women who are motivated to uptake contraceptive use for reasons such as benefits of a method, economic situation, suitability of a methods and fear of unwanted pregnancy, now have DMPA-SC available, assessable and without fee.33 No doubt, the availability, accessibility and free commodity/service for DMPA-SC may have contributed to the upward trend.
There are many unintended pregnancies in Nigeria,35 which seems to indicate a large unmet need for contraceptive use.36 However, the myth and misconception about the side effects of modern contraceptives,37 may have contributed to low contraceptive use. Moreover, what was lacking was the political will to implement FP programs on a much larger scale, using community-oriented approaches and communication programs, to help change the myth about the side effects of modern contraceptives. But it seems the Nigerian government has arisen to her responsibility recently. This is why DMPA-SC is becoming the game changer in the FP method mix. DMPA-SC is safe with minimal side-effects. In a longitudinal study in Nigeria, 810 clients who used DMPA as a contraceptive method were followed over a period of 11 years. In the end, amenorrhea, weight gain, weight loss, metrorrhagia and menorrhagia were the reasons for discontinuation of DMPA in only 11% of the patients.38
Strengths and Limitations
The total saturation approach in the implementation of RASuDiN project makes a plausible representation of the project states. The participation of key stakeholders during the monthly data validation meetings and the measures of data validation, make the results of this study very dependable. However, our sample of DMPA-SC users in 10 out of 36 states + Federal Capital Territory in Nigeria is unlikely to be representative of the Nigerian population of reproductive age women. These data would not be considered representative, as there is no denominator to determine the rate. The data consist of counts of patient encounters. Further, because this analysis is restricted to service data, client motivations for using family planning for the first time or choosing to switch to DMPA-SC from another method cannot be determined. It is possible that increase in the use of DMPA-SC may have been overestimated due to the use of absolute count rather than a rate.
Conclusion
We have found an increasing number of women adopting and continuing to utilize DMPA-SC as a form of birth control in Nigeria. While there is a large focus on the uptake and continuation of DMPA-SC, more concerted efforts are needed to scale-up the intervention to other parts of Nigeria. More women can be encouraged to uptake or continue contraceptive use. We recommend that attention should be paid to improving the quality of counseling about side effects of contraceptive use, and particularly those related to amenorrhea, weight gain, weight loss, metrorrhagia, menorrhagia and bleeding as to enhance universal acceptability of contraceptive use in Nigeria.
Abbreviations
AIDS, Acquired Immunodeficiency Syndrome; ARFH, Association for Reproductive and Family Health; CORPS, Community Oriented Resource Persons; COVID-19, Coronavirus disease 2019; DHIS, District Health Information System; DMPA-SC, Subcutaneously-administered Depot-medroxyprogesterone acetate; FP, Family Planning; LGA, Local Government Area; M&E, Monitoring and Evaluation; MMR, Maternal Mortality Ratio; NDHS, Nigeria Demographic and Health Survey; NHREC, National Health Research Ethics Committee; PPMVs, Patent and Proprietary Medicine Vendor; RASUDIN, Resilient and Accelerated Scale Up of Subcutaneously-administered Depot-medroxyprogesterone Acetate in Nigeria; RH, Reproductive Health; SBC, Social and Behaviour Change; SDG, Sustainable Development Goal; WHO, World Health Organization.
Data Sharing Statement
Data is available strictly on request.
Ethics Approval and Consent to Participate
Ethical clearance was obtained from the National Health Research Ethics Committee, Nigeria for research in the RASuDiN project.
Consent for Publication
No consent to publish was needed for this study as the authors did not use any details, images or videos related to individual participants.
Acknowledgments
The authors appreciate Bill and Melinda Gates Foundation and Children’s Investment Fund Foundation for the grant.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received a grant from Bill and Melinda Gates Foundation and Children’s Investment Fund Foundation. However, the manuscript is strictly the views of the authors.
Disclosure
The Association of Reproductive and Family Health (ARFH) is the principal recipient of the grant while the Center for Communication and Social Impact is a sub-recipient of the grant and responsible for demand generation component of the grant to promote DMPA-SC. The authors report no other potential conflicts of interest for this work.
References
1. Ahmed S, Li Q, Liu L, Tsui AO. Maternal deaths averted by contraceptive use: an analysis of 172 countries. Lancet Lond Engl. 2012;380(9837):111–125. doi:10.1016/S0140-6736(12)60478-4
2. Darroch JE Adding It Up: investing in Contraception and Maternal and Newborn Health, 2017—Estimation Methodology, New York: Guttmacher Institute; 2018. Available from: https://www.guttmacher.org/report/adding-it-up-investing-in-contraception-maternalnewborn-health-2017-methodology.
3. Family Planning 2020 (FP2020). Measurement. In: FP2020: the Way Ahead, 2016–2017. Washington, DC; 2020. Available from: http://progress.familyplanning2020.org/sites/all/themes/custom/progressreport/pdf/FP2020_2019Report_WEB.pdf.
4. Ali MM, Cleland J, Shah IH Causes and consequences of contraceptive discontinuation: evidence from 60 demographic and health surveys. World Health Organization; 2012. Available from: https://apps.who.int/iris/bitstream/handle/10665/75429/9789241504058_eng.pdf?sequence=1&isAllowed=y.
5. Sinai I, Omoluabi E, Jimoh A, Jurczynska K. Unmet need for family planning and barriers to contraceptive use in Kaduna, Nigeria: culture, myths and perceptions. Cult Health Sex. 2020;22(11):1253–1268. doi:10.1080/13691058.2019.1672894
6. Ekholuenetale M, Olorunju S, Fowobaje KR, Onikan A, Tudeme G, Barrow A. When Do Nigerian Women of Reproductive Age Initiate and What Factors Influence Their Contraceptive Use? A Contextual Analysis. Open Access J Contracept. 2021;12:133–147. doi:10.2147/OAJC.S316009
7. National Population Commission (NPC) [Nigeria] and ICF. Nigeria Demographic and Health Survey 2018. Abuja, Nigeria, and Rockville, Maryland, USA: NPC and ICF; 2019. Available from: https://www.dhsprogram.com/pubs/pdf/FR359/FR359.pdf.
8. Odwe G, Gray K, Kyarimpa A, Obare F, Nagendi G. Introduction of Subcutaneous Depot Medroxyprogesterone Acetate (DMPA-SC) Injectable Contraception at Facility and Community Levels: pilot Results From 4 Districts of Uganda. Glob Health Sci Pract. 2018;6(4):711–722. doi:10.9745/GHSP-D-18-00117
9. Nigeria FP2020. Family Planning Commitment. Available from: https://www.familyplanning2020.org/sites/default/files/Nigeria_FP2020_Commitment_2017.pdf.
10. Liu J, Shen J, Diamond-Smith N. Predictors of DMPA-SC continuation among urban Nigerian women: the influence of counseling quality and side effects. Contraception. 2018;98(5):430–437. doi:10.1016/j.contraception.2018.04.015
11. Burke HM, Mueller MP, Packer C, et al. Provider acceptability of Sayana® Press: results from community health workers and clinic-based providers in Uganda and Senegal. Contraception. 2014;89(5):368–373. doi:10.1016/j.contraception.2014.01.009
12. Cole K, Saad A. The Coming-of-Age of Subcutaneous Injectable Contraception. Glob Health Sci Pract. 2018;6(1):1–5. doi:10.9745/GHSP-D-18-00050
13. Spieler J. Sayana® Press: can it be a “game changer” for reducing unmet need for family planning? Contraception. 2014;89(5):335–338. doi:10.1016/j.contraception.2014.02.010
14. Adetunji JA. Rising popularity of injectable contraceptives in sub-Saharan Africa. Afr Popul Stud. 2011;25:2. doi:10.11564/25-2-247
15. Burke HM, Mueller MP, Perry B, et al. Observational study of the acceptability of Sayana® Press among intramuscular DMPA users in Uganda and Senegal. Contraception. 2014;89(5):361–367. doi:10.1016/j.contraception.2014.01.022
16. Polis CB, Nakigozi GF, Nakawooya H, et al. Preference for Sayana® Press versus intramuscular Depo-Provera among HIV-positive women in Rakai, Uganda: a randomized crossover trial. Contraception. 2014;89(5):385–395. doi:10.1016/j.contraception.2013.11.008
17. Chen X, Yu B. First two months of the 2019 Coronavirus Disease (COVID-19) epidemic in China: real-time surveillance and evaluation with a second derivative model. Glob Health Res Policy. 2020;5(1):7. doi:10.1186/s41256-020-00137-4
18. Patel A, Jernigan DB, Abdirizak F, et al. Initial Public Health Response and Interim Clinical Guidance for the 2019 Novel Coronavirus Outbreak — United States, December 31, 2019–February 4, 2020. Morb Mortal Wkly Rep. 2020;69(5):140–146. doi:10.15585/mmwr.mm6905e1
19. WHO Director-General’s opening remarks at the media briefing on COVID-19-11 March 2020. Available from: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19—11-march-2020.
20. Aly J, Haeger KO, Christy AY, Johnson AM. Contraception access during the COVID-19 pandemic. Contracept Reprod Med. 2020;5(1):17. doi:10.1186/s40834-020-00114-9
21. Riley T, Sully E, Ahmed Z, Biddlecom A. Estimates of the Potential Impact of the COVID-19 Pandemic on Sexual and Reproductive Health In Low- and Middle-Income Countries. Int Perspect Sex Reprod Health. 2020;46:73–76. doi:10.1363/46e9020
22. Population Reference Bureau. 2017 World Population Data Sheet with a special focus on Youth. Available from: https://www.prb.org/wp-content/uploads/2017/08/2017_World_Population.pdf.
23. Nkwo PO, Lawani LO, Ezugwu EC, Iyoke CA, Ubesie AC, Onoh RC. Correlates of poor perinatal outcomes in non-hospital births in the context of weak health system: the Nigerian experience. BMC Pregnancy Childbirth. 2014;14(1):341. doi:10.1186/1471-2393-14-341
24. Yaya S, Bishwajit G, Uthman OA, Amouzou A. Why some women fail to give birth at health facilities: a comparative study between Ethiopia and Nigeria. PLoS One. 2018;13(5):e0196896. doi:10.1371/journal.pone.0196896
25. Adinma ED, Brian-d adinma JI, Obionu CC, Asuzu MC. Effect of government-community healthcare co-financing on maternal and child healthcare in Nigeria. West Afr J Med. 2011;30(1):35–41. doi:10.4314/wajm.v30i1.69882
26. Federal Ministry of Health. Saving Newborn Lives in Nigeria: NEWBORN HEALTH in the Context of the Integrated Maternal, Newborn and Child Health Strategy.
27. Okegbe T, Affo J, Djihoun F, et al. Introduction of Community-Based Provision of Subcutaneous Depot Medroxyprogesterone Acetate (DMPA-SC) in Benin: programmatic Results. Glob Health Sci Pract. 2019;7(2):228–239. doi:10.9745/GHSP-D-19-00002
28. Hellwig F, Coll CV, Ewerling F, Barros AJ. Time trends in demand for family planning satisfied: analysis of 73 countries using national health surveys over a 24-year period. J Glob Health. 2019;9(2). doi:10.7189/jogh.09.020423
29. Stout A, Wood S, Barigye G, Kaboré A, Siddo D, Ndione I. Expanding Access to Injectable Contraception: results From Pilot Introduction of Subcutaneous Depot Medroxyprogesterone Acetate (DMPA-SC) in 4 African Countries. Glob Health Sci Pract. 2018;6(1):55–72. doi:10.9745/GHSP-D-17-00250
30. Health Policy Plus. DMPA-SC Introduction and Scale-Up in Nigeria: future Benefits for Contraceptive Use and Savings. Washington, DC: Palladium. 4; 2018. Available from: http://www.healthpolicyplus.com/ns/pub/8197-8351_DMPASCIntroductionandScaeUpinNigeria.pdf.
31. Worku AG, Tessema GA, Zeleke AA. Trends of Modern Contraceptive Use among Young Married Women Based on the 2000, 2005, and 2011 Ethiopian Demographic and Health Surveys: a Multivariate Decomposition Analysis. PLoS One. 2015;10(1):e0116525. doi:10.1371/journal.pone.0116525
32. Adedini SA, Omisakin OA, Somefun OD. Trends, patterns and determinants of long-acting reversible methods of contraception among women in sub-Saharan Africa. PLoS One. 2019;14(6):e0217574. doi:10.1371/journal.pone.0217574
33. Osinowo K, Ekholuenetale M, Ojomo O, Hassan A, Ladipo OA. Patterns of triggers, ideation and motivational factors of contraceptive utilization among women and gate-keepers in Nigeria: a scoping study on the resilient and accelerated scale up of DMPA-SC in Nigeria (RASUDIN). Contracept Reprod Med. 2020;5(1):38. doi:10.1186/s40834-020-00141-6
34. Liu J, Schatzkin E, Omoluabi E, et al. Introducing the subcutaneous depot medroxyprogesterone acetate injectable contraceptive via social marketing: lessons learned from Nigeria’s private sector. Contraception. 2018;98(5):438–448. doi:10.1016/j.contraception.2018.07.005
35. Yaya S, Amouzou A, Uthman OA, et al. Prevalence and determinants of terminated and unintended pregnancies among married women: analysis of pooled cross-sectional surveys in Nigeria. BMJ Glob Health. 2018;3(2):e000707. doi:10.1136/bmjgh-2018-000707
36. Wang C, Cao H. Persisting Regional Disparities in Modern Contraceptive Use and Unmet Need for Contraception among Nigerian Women. BioMed Res Int. 2019;2019:1–9. doi:10.1155/2019/9103928
37. Monjok E. Contraceptive practices in Nigeria: literature review and recommendation for future policy decisions. Open Access J Contracept. 2010;9. doi:10.2147/OAJC.S9281
38. Falase EA, Otolorin EO, Ladipo OA. Experience with the use of depo-medroxyprogesterone acetate in a Nigerian population. Afr J Med Med Sci. 1988;17(4):209–213.
 © 2021 The Author(s). This work is published by Dove Medical Press Limited, and licensed under a Creative Commons Attribution License.
The full terms of the License are available at http://creativecommons.org/licenses/by/4.0/.
The license permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
© 2021 The Author(s). This work is published by Dove Medical Press Limited, and licensed under a Creative Commons Attribution License.
The full terms of the License are available at http://creativecommons.org/licenses/by/4.0/.
The license permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.