")
Back to Journals » Clinical Interventions in Aging » Volume 14
Reference values of gait parameters measured with a plantar pressure platform in community-dwelling older Japanese adults
Authors Kawai H , Taniguchi Y, Seino S, Sakurai R, Osuka Y, Obuchi S , Watanabe Y , Kim H, Inagaki H , Kitamura A, Awata S , Shinkai S
Received 23 April 2019
Accepted for publication 15 June 2019
Published 12 July 2019 Volume 2019:14 Pages 1265—1276
DOI https://doi.org/10.2147/CIA.S213216
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Richard Walker
Hisashi Kawai, Yu Taniguchi, Satoshi Seino, Ryota Sakurai, Yosuke Osuka, Shuichi Obuchi, Yutaka Watanabe, Hunkyung Kim, Hiroki Inagaki, Akihiko Kitamura, Shuichi Awata, Shoji Shinkai
Tokyo Metropolitan Institute of Gerontology, Tokyo 173-0015, Japan
Background: Gait measures such as gait speed, stride length, step width, and stance duration change with advanced age and are associated with adverse health outcomes among older adults. The stride-to-stride variabilities of gait measures are also related to falls and cognitive decline in older adults; however, reference values of these gait parameters in older Japanese adults do not exist. This study aimed to determine the reference values of gait parameters as measured by a plantar pressure platform in community-dwelling older Japanese adults.
Methods: Community-dwelling adults (N=1,212) who were independent in basic activities of daily living and aged 70–96 years (491 men, 721 women) completed the gait performance measurement in a geriatric health assessment. We assessed 10 gait performance measures with a plantar pressure platform system (P-WALK, BTS Bioengineering) and calculated means and coefficient of variations (CVs) of the gait measures as well as quintiles for those gait parameters per age group among men and women.
Results: Mean (SDs) of gait speed, stride length, step width, and stance durations were 1.26 (0.24) meters per second (m/s), 121.9 (19.8) cm, 24.0 (3.2) cm, and 552.4 (60.4) milliseconds (ms), respectively, in men, and 1.27 (0.21) m/s, 115.7 (16.3) cm, 17.9 (2.8) cm, and 517.6 (59.8) ms, respectively, in women. Mean of CVs (SD) of stride length, step width, and single-stance duration were 2.76 (1.35), 12.06 (3.98), and 5.74 (2.66), respectively, in men and 2.69 (1.24), 15.65 (4.53), and 5.77 (2.40), respectively, in women. Gait parameters (except CVs of step width) declined significantly with age regardless of gender (P< 0.01 for trends).
Conclusion: This study determined age group dependent gait parameter reference values, presented as means with quintile ranges, in community-dwelling older Japanese adults. These reference values may be useful metrics for gait assessment in the elderly.
Keywords: gait parameter, variation coefficient, community-dwelling, older adult, reference value
Introduction
Gait speed is an important measure that can predict adverse health outcomes such as disability,1 death,2 and functional dependence3 in older individuals. Gait speed is determined by step length and step frequency, and especially gait speed and step length decrease with advanced age.4,5 Other gait parameters, such as step width, foot angle, stance duration, and double-stance duration, are also suggested to change with age.6,7 Cadence, stride length, and double-stance duration are also correlated with gait speed.8
Gait parameters are associated with falls among older individuals. A systematic review suggested that step length, gait speed, stride length, and stance-time variability were more sensitive than other gait parameters for differentiating fallers from non-fallers among older individuals.9 Gait variability is defined as a variation of stride-to-stride gait parameters, which is usually assessed by SD or coefficient of variation (CV) of the gait parameters in each step.10,11 Many studies have reported that gait parameter variabilities are associated with fall risks and mobility disability.11–13
Moreover, several studies have reported that gait speed and step length predict cognitive decline.14–16 A recent study investigated the association between gait parameter and cognitive status with falls since falls are prevalent in individuals with cognitive decline.17 Gait parameters are also utilized to assess frailty18 and to evaluate effectiveness of physical improvement by exercise.19 Reference values for gait parameters could be utilized by researchers to determine cut-off values when examining the impact of gait parameters on adverse health outcomes as described above. Additionally, these values may provide valuable assistance to clinicians to establish normal value ranges and for assessment of clinical intervention effects.
Several studies proposed reference values of gait parameter, such as gait speed and step length,20–22 spatio-temporal parameters,23 and planter pressure,;24,25 however, no studies have reported data concerning older Japanese adults. Moreover, only a few studies showed the reference value of the variability of such gait parameters.23 This study thus aimed to clarify the gait parameters that decline with advanced age and to determine the reference values of those gait parameters in community-dwelling older Japanese adults.
Methods
Participants
Data were collected as part of a community-wide survey in Itabashi ward, Tokyo, Japan.26 Surveys were mailed to 7,614 adults aged 70 years or older who were listed in the basic resident register of which 5,430 participants responded (response rate of 71.3%). Respondents were provided the opportunity for a preventive health check-up at a survey location. Of the initial survey respondents a total of 1,248 participants underwent a geriatric assessment (response rate of 23.0%). Ultimately, 1,212 participants aged 70–96 years (491 men, 721 women; both mean age =77.1 years), who completed the gait performance measurement without a cane and were independent in any five basic activities of daily living (ADLs; which included bathing, dressing, walking, eating, and continence) were included in the analyses.
Age, body height, body weight, history of chronic disease (which included hypertension, stroke, heart disease, diabetes, or osteoarthritis), hip/knee pain, depression, and Parkinson’s disease were assessed to determine participant characteristics. History of disease and pain were confirmed in face-to-face interviews by physicians or nurses. In addition, cognitive function of participants was assessed using the Mini-Mental State Examination (MMSE), which was administrated by well-trained personnel.
This study was conducted in accordance with the Declaration of Helsinki and all participants provided written, informed consent prior to their participation in the study. The ethics committee of the Tokyo Metropolitan Institute of Gerontology approved this study.
Gait performance measurement
Gait performance was measured by P-WALK (Bioengineering, Milano, Italy) modular platforms system for plantar pressure measurement. Ten sensor plates were placed on a straight 5-m intermediate area of a walkway.26,27 Gait performance was recorded when participants walked at a normal pace in the sensor area of the walkway, with 3-m each at the beginning and the ending of the walkway. Participants walked on the walkway barefoot. Data were sampled at 50 Hz and processed by P-WALK software. Several previous studies have demonstrated the reliability of obtaining gait parameter measurements using a pressure platform device.28–30
Gait performance was measured twice, and the following 10 gait parameters were measured by the software: i) gait speed, ii) stride length, iii) step length, iv) step width, v) average foot pressure, vi) maximum foot pressure, vii) stance duration, viii) double-stance duration, ix) single-stance duration, and x) stride time (Figure 1). Foot angle and step surface were also measured in the P-WALK software. However, since those parameters are affected by individual gait characteristics, rather than age decline, they were excluded from the analysis. Gait speed was measured over the entire walk, while the other parameters were measured at each step. Plantar pressure were also normalized by body weight. Finally, we used the average of all steps between the left and right legs. We also calculated coefficient of variations (CVs) from each step for all parameters (except for gait speed). Although all the data of the complete steps were used for calculating the gait parameters, we excluded a step deemed to be intentionally adjusted when stepping on the first sensor mat from the calculation.
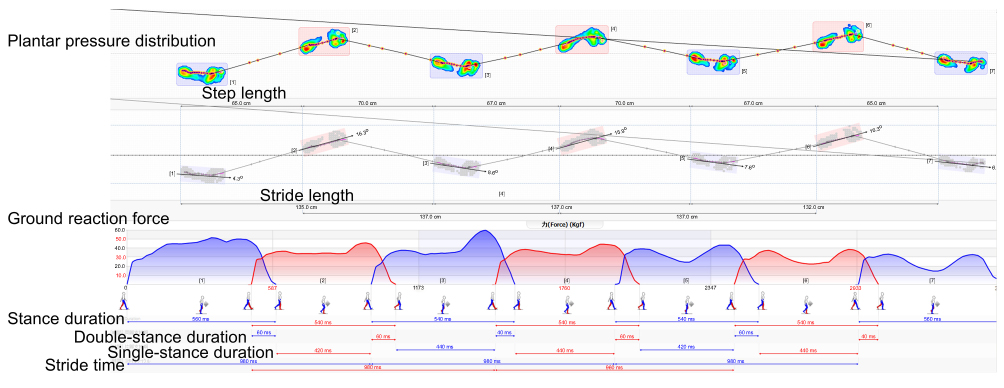 |
Figure 1 Example of gait performance measurement (P-WALK software). Step length and stride length were calculated using the distance between the heel contact and next heel contact. Average foot pressure and maximum foot pressure were determined as the average and maximum values of plantar pressure distribution during whole walk, respectively. Time parameters, including stance duration, double-stance duration, single stance duration, and stride time, were calculated by detection of foot contact based on ground reaction forces. |
Statistical analyses
We used descriptive statistics to analyze participants. Differences in the variables between men and women were analyzed with unpaired t-tests and chi-square tests. The mean and SDs of all gait parameters were tabulated per 5-year age groups (70–74, 75–79, 80–84, and ≥85 years) for each gender. To evaluate linear trends in the means of gait parameters between age groups, we used weighted one-way analyses of variance by age groups. We also calculated quintiles (20th, 40th, 60th, and 80th percentiles) of each gait parameter by gender and each 5-year age group.31
IBM SPSS statistics 25 (IBM Japan, Ltd., Tokyo, Japan) was used for all analyses. Statistical significance was set at 5%.
Results
Descriptive statistics of age, chronic disease status, body height, body weight, body mass index, and gait parameters were shown in Table 1. The mean gait speed (SD) was 1.26 (0.24) meters per second (m/s) for men and 1.27 (0.21) m/s for women. There was a significant difference in the age distribution between genders. The percentage of those aged 70–74 years was significantly greater in men than in women, whereas the percentage of those aged 75–80 years was significantly greater in women than in men (Table 1). The prevalence of stroke, heart disease, and diabetes was significantly greater in men than in women. The prevalence of osteoarthritis and reporting knee pain was significantly greater in women than in men.
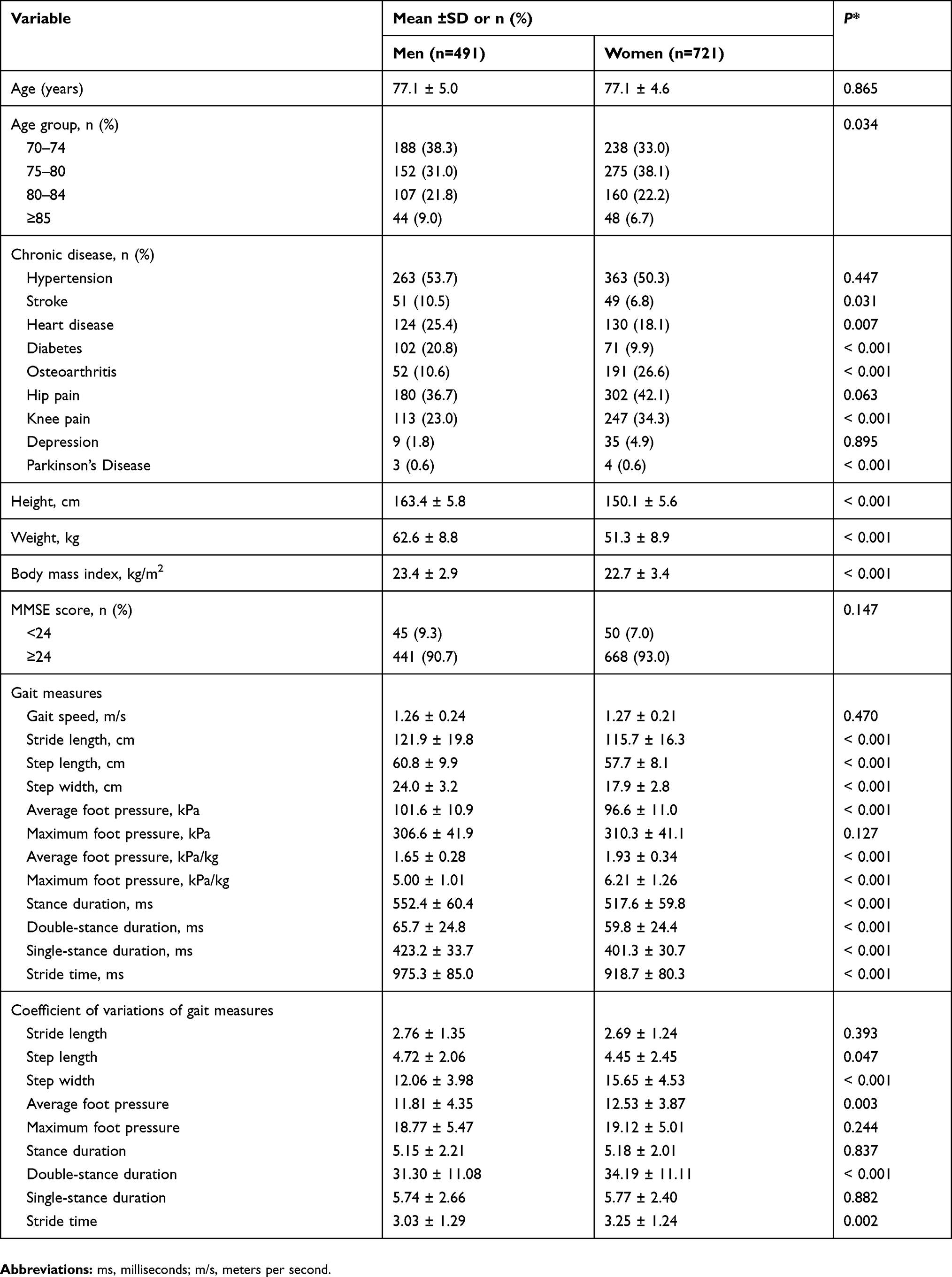 |
Table 1 Participants’ characteristics |
Stride and step length, step width, and average foot pressure were significantly larger in men than in women (Table 1). Temporal parameters included in stride time were significantly longer in men than in women. CVs of step width, average foot pressure, normalized average and maximum foot pressure, double-stance duration, and stride time were significantly greater in women than in men, whereas that of step length was significantly longer in men than in women.
Among men, the gait parameters (except for maximum foot pressure, normalized average foot pressure, single-stance duration, CVs of step width, stance duration, and stride time) showed significant declining trends with advanced age (Table 2). In women, step width, maximum foot pressure, normalized average foot pressure, single-stance duration, CVs of step width, and average foot pressure did not show significant declining trends per age (Table 3).
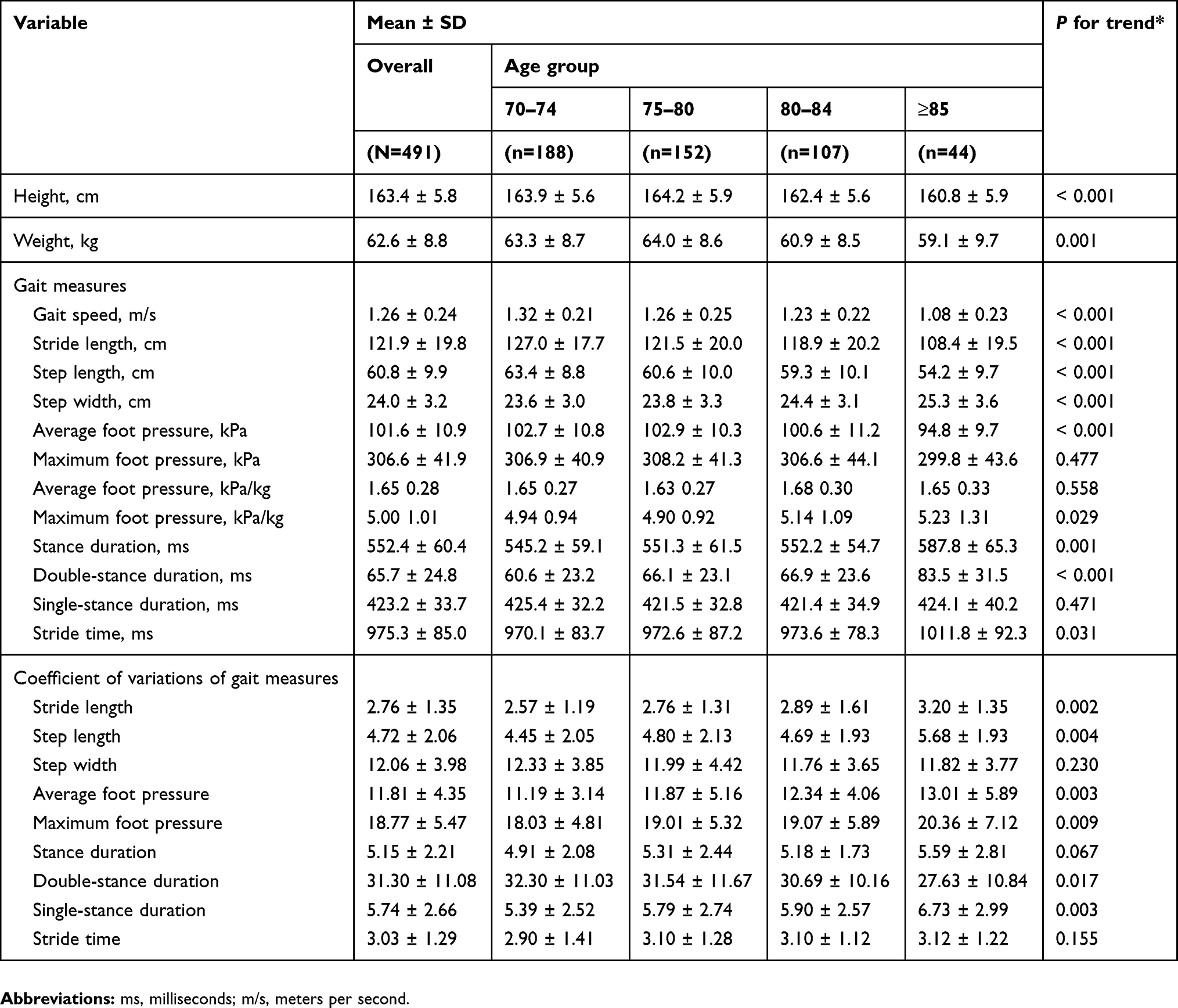 |
Table 2 Mean and SDs for gait parameters per age group among men |
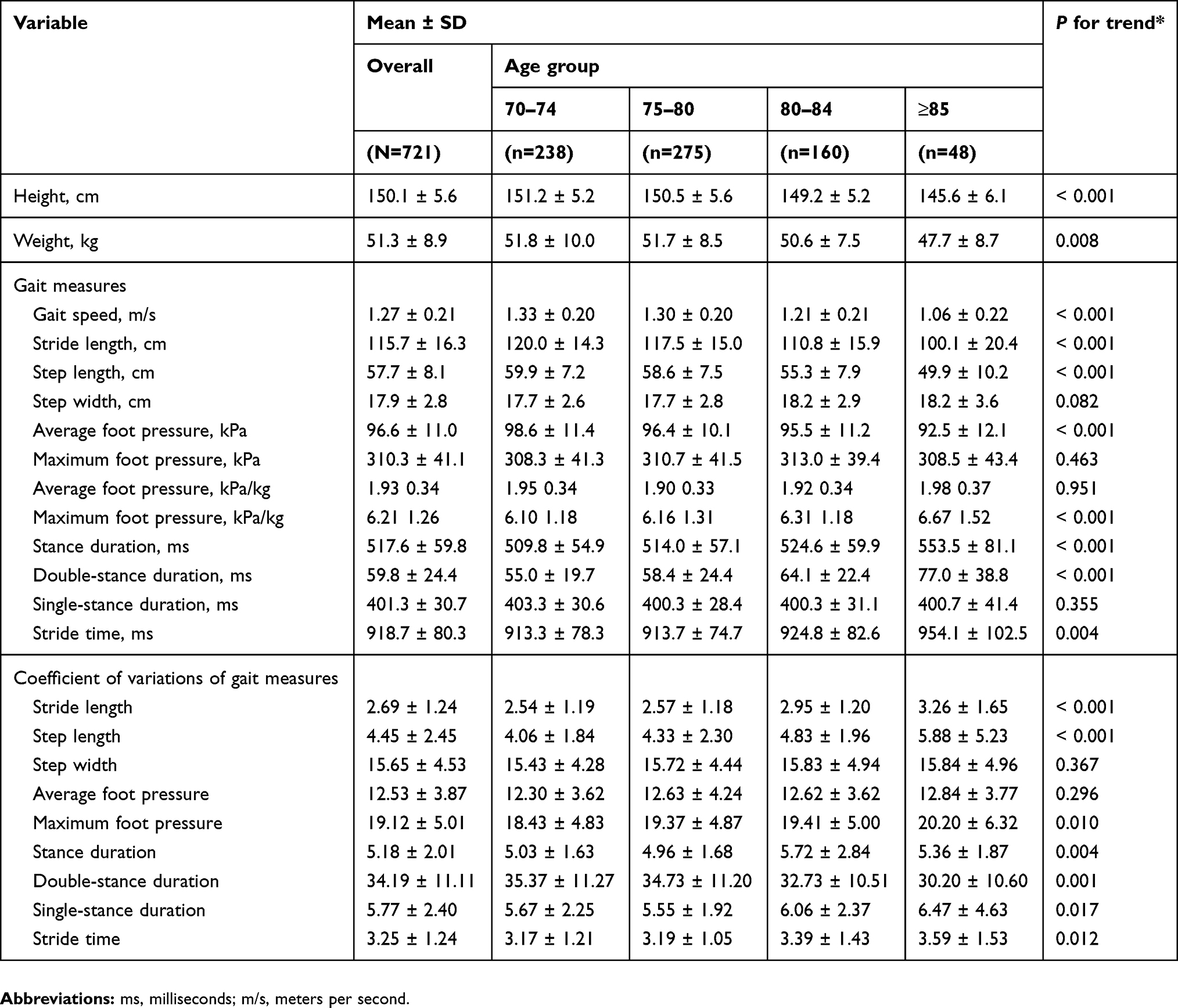 |
Table 3 Mean and SDs for gait parameters per age group among women |
Lastly, quintiles of the gait parameters, which were recognized with declining trends of advanced age among both genders, are shown in Tables 4 and 5.
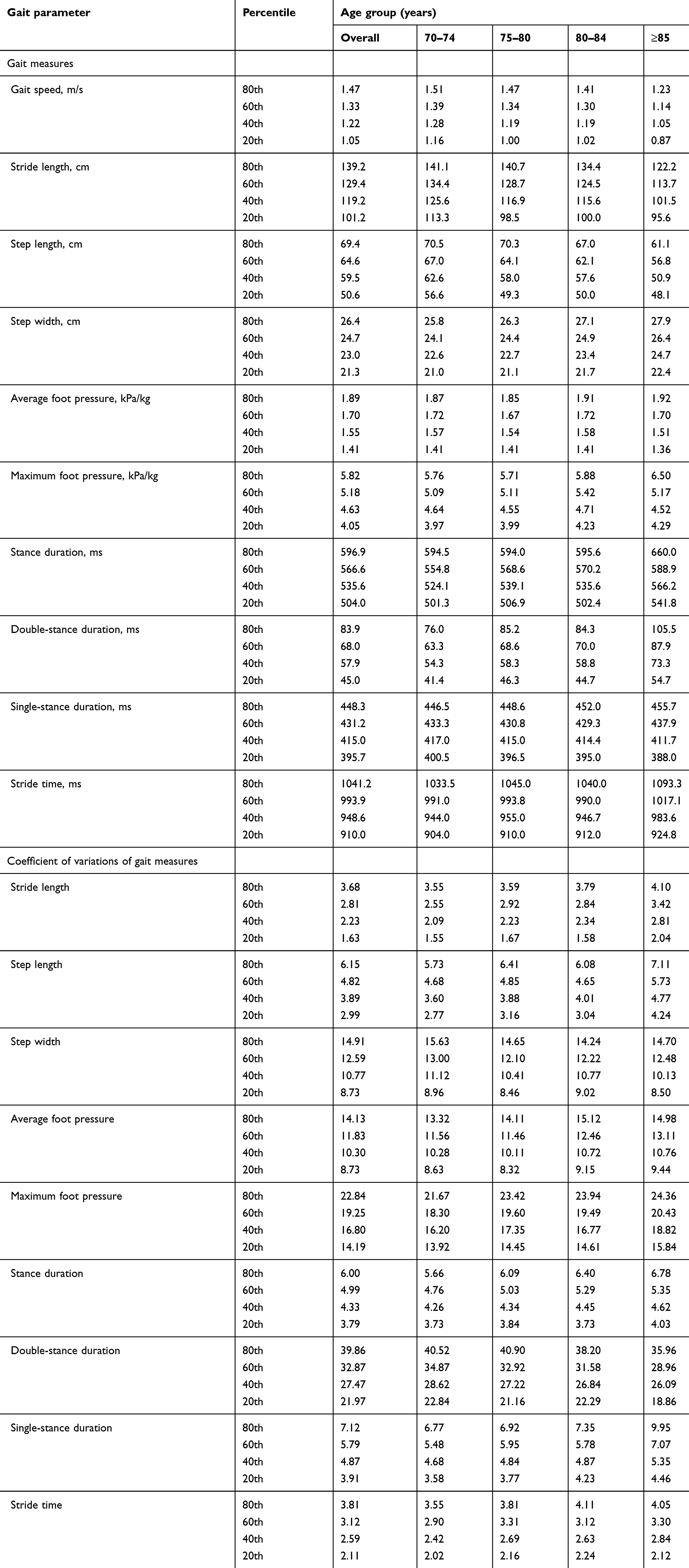 |
Table 4 Quintiles of gait parameters per age group among men |
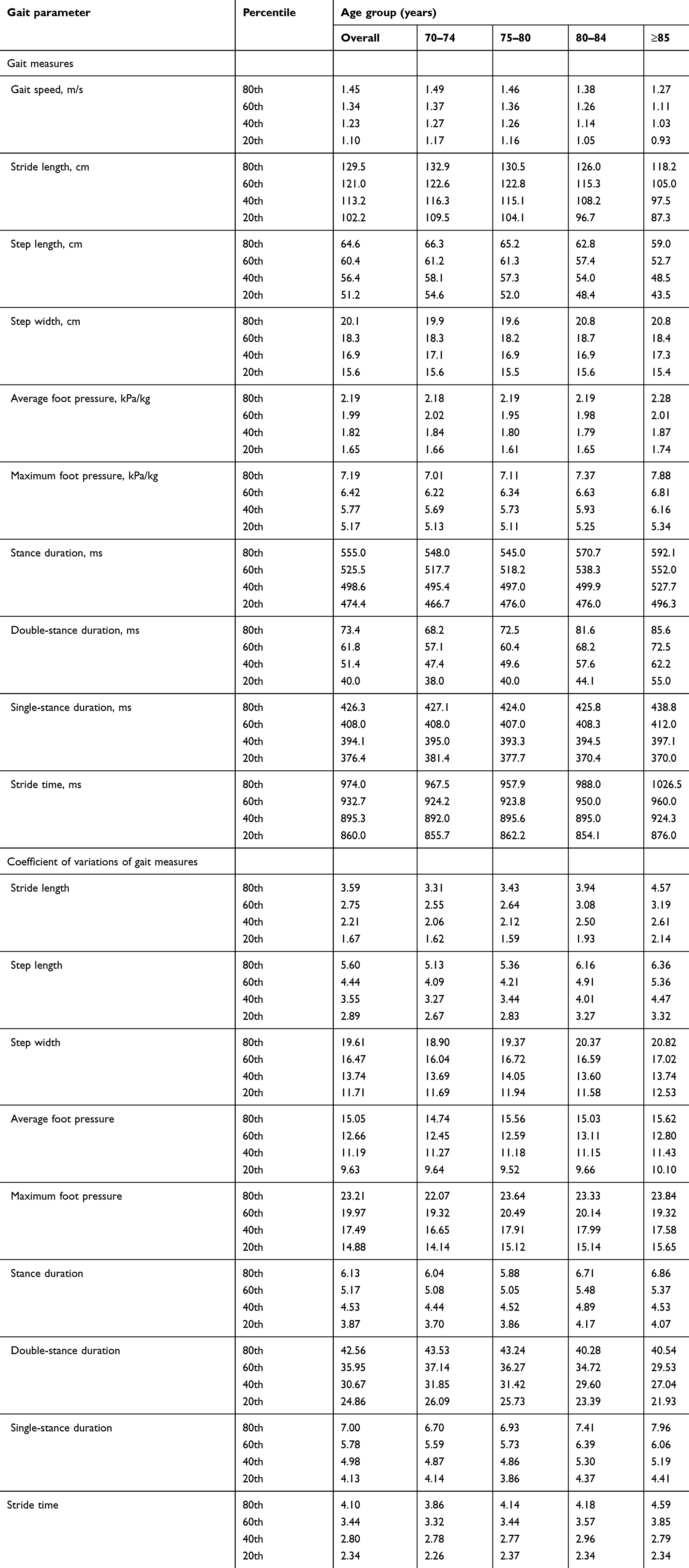 |
Table 5 Quintiles of gait parameters per age group among women |
Discussion
In this study, we obtained reference value data divided across quintiles for ten gait parameters and their associated CVs (except for gait speed) for a large sample set of community-dwelling older Japanese adults. There is ample need for such reference values since there are few studies that have either published reference values for gait parameters or examined stride-to-stride variability present across gait parameters. Although we did not examine the association between each gait parameter and any specific adverse health outcome, many epidemiological studies have demonstrated that gait parameters can predict adverse events in the elderly, including frailty,18 ADL disability,3 and cognitive decline.16 Therefore, the reference values obtained from this study could be used to compare the prevalence of adverse events across values to determine cut-off ranges for adverse event risk screening. Since gait is associated in the elderly with not only adverse health outcomes but also mortality in patients, such as in those with chronic heart disease,32 the gait parameter reference values obtained in this study may also be utilized for patient evaluation and classification. These reference values can be utilized to assess the effectiveness of interventions; determine the relationship between each gait level and the onset of future adverse health outcomes such as frailty, ADL disability, and dementia; and screen for these unfavorable outcomes. The reference values presented in this study would be useful for health assessment of not only Japanese but also Asian older adults.
We first examined the representativeness of the sample—whether the reference values shown in this study can be widely applied to predicting health outcomes and intervention assessments among community-dwelling older adults. The participants in this study were recruited from all residents across a community population, and approximately 16% of the total population participated in this study. Reasons for not participating in the study may have included inability to respond due to cognitive decline, or mobility issues that preventing arrival to the survey site. However, regardless of the reasons for lack of participation, the samples that comprised this study better represent community-dwelling older adults compared with studies where samples were recruited from an applicant pool or through significant extraction. Compared to the pooled data from cohort studies of community-dwelling older Japanese adults,21,31 where participants were recruited from all residents or through random sampling, this study was able to include more participants with age over 85 years old. However, the current participants were recruited from only one urban area. Since it has been suggested that the gait speed is affected by regional differences,33 comparison with other population recruited from other regions remains necessary.
Although some previous studies reported gender differences in gait speed,20–23,31 we did not mirror these results. Moreover, the mean values of gait speed in the younger age groups were faster for men than for women, which was consistent with previous studies. Contrary, in those aged older than 80 years, gait speed was slower in men than in women. Some walking ability will be required for independent daily living; therefore, gender differences may decrease in the older age groups. These findings may have become apparent in this study since the proportion of those older than 80 years was larger compared to previous studies. Thus, the data presented in this study included participants in the independent community population over the age of 80 years old.
Next, we examined which parameter reflected the age change. Gait speed, stride length, and step length declined with age in both men and women, which was again consistent with some previous studies.20,22,23 It has been reported that step width increases with age;6 however, significant age-related change in step width was not recognized among women in the current study. Increased step width in aged groups would be increased gait stability by widening the base of support. The adaptation for stability may have influenced the result for step width.
Average foot pressure decreased for both men and women according to age; however, maximum foot pressure did not change with age in both genders. We posit that decreased average foot pressure was affected by a decrease in ground reaction force during the stance phase, which may be due to body weight loss rather than aging. Conflicting results were shown since normalized maximum foot pressure increased with age; however, peak force did not differ between the older and younger participants, which was shown in a previous study.24 Concerning the lack of age-related change in normalized average foot pressure, it may be not functional decline, but an adaptation to increase gait stability as similar to increased step width. Although single-stance duration was not significantly changed with advanced age in both men and women, this tendency was similar to that of a previous study.23
The CVs of gait parameters that were unaffected by age were CVs of step width, average foot pressure in women, stance duration in men, and stride time in men. About CV of step width, we considered that an adaptation to gait stability, as described above, was affected. CV of average foot pressure increased with advanced age in men; however, age change was negligible in women, and the trend was non-significant. CVs of stance duration and stride time were not significantly changed according to age among men, and any change tendencies were not consistent. For the other parameters, the CVs tended to increase with advanced age, indicating that the control of gait fluctuates with aging. These results were consistent with a previous study.23
There were several limitations to this study. Selection bias is possible since participants came to the survey site by themselves. A previous study3 that examined associations between walking speed and the onset of functional dependence in a community population found that the risk of functional dependence in the first quartile was increased two to six times compared to the fourth quartile level. Thus, below when examining values below the twentieth percentile in the present reference value dataset, the risk of adverse events may be increased, however future studies are necessary to examine the association between each gait parameters reference value and adverse event risk.In addition, participants walked on the sensor mat barefoot. In barefoot walking, step length is larger, stance duration is shorter, and cadence is higher than in walking while wearing standard shoes.34
Conclusions
This study determined reference values of the gait parameters measured by a plantar pressure platform in community-dwelling older Japanese adults. These reference values would be useful for gait assessment in the elderly.
Acknowledgments
We are grateful to the local authorities of the Itabashi Ward and the individuals who participated in this study. This study was supported by grants from the Tokyo Metropolitan Government; Tokyo Metropolitan Institute of Gerontology; the Research Committee of Comprehensive Research on Aging and Health; the Ministry of Health, Labor, and Welfare of Japan (grant number: H27-Choju-Ippan-005); Japan Agency for Medical Research and Development (AMED [grant number: JP16dk0110018]); and Japan Society for the Promotion of Science KAKENHI (grant numbers: 16K11908, JP17K13239).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Perera S, Patel KV, Rosano C, et al. Gait speed predicts incident disability: a pooled analysis. J Gerontol A Biol Sci Med Sci. 2016;71(1):63–71. doi:10.1093/gerona/glv126
2. Studenski S, Perera S, Patel K, et al. Gait speed and survival in older adults. JAMA. 2011;305(1):50–58. doi:10.1001/jama.2010.1923
3. Shinkai S, Watanabe S, Kumagai S, et al. Walking speed as a good predictor for the onset of functional dependence in a Japanese rural community population. Age Ageing. 2000;29(5):441–446. doi:10.1093/ageing/29.5.441
4. Himann JE, Cunningham DA, Rechnitzer PA, Paterson DH. Age-related changes in speed of walking. Med Sci Sports Exerc. 1988;20(2):161–166. doi:10.1249/00005768-198820020-00010
5. Samson MM, Crowe A, de Vreede PL, Dessens JA, Duursma SA, Verhaar HJ. Differences in gait parameters at a preferred walking speed in healthy subjects due to age, height and body weight. Aging. 2001;13(1):16–21.
6. Murray MP, Kory RC, Clarkson BH. Walking patterns in healthy old men. J Gerontol. 1969;24(2):169–178. doi:10.1093/geronj/24.2.169
7. Kaneko M, Morimoto Y, Kimura M, Fuchimoto K, Fuchimoto T. A kinematic analysis of walking and physical fitness testing in elderly women. J Can Sci Sport. 1991;16(3):223–228.
8. Jerome GJ, Ko SU, Kauffman D, Studenski SA, Ferrucci L, Simonsick EM. Gait characteristics associated with walking speed decline in older adults: results from the Baltimore Longitudinal Study of Aging. Arch Gerontol Geriat. 2015;60(2):239–243. doi:10.1016/j.archger.2015.01.007
9. Mortaza N, Abu Osman NA, Mehdikhani N. Are the spatio-temporal parameters of gait capable of distinguishing a faller from a non-faller elderly? Eur J Phys Rehabil Med. 2014;50(6):677–691.
10. Paterson K, Hill K, Lythgo N. Stride dynamics, gait variability and prospective falls risk in active community dwelling older women. Gait Posture. 2011;33(2):251–255. doi:10.1016/j.gaitpost.2010.11.014
11. Verghese J, Holtzer R, Lipton RB, Wang C. Quantitative gait markers and incident fall risk in older adults. J Gerontol A Biol Sci Med Sci. 2009;64(8):896–901. doi:10.1093/gerona/glp033
12. Hausdorff JM, Rios DA, Edelberg HK. Gait variability and fall risk in community-living older adults: a 1-year prospective study. Arch Phys Med Rehabil. 2001;82(8):1050–1056. doi:10.1053/apmr.2001.24893
13. Brach JS, Studenski SA, Perera S, VanSwearingen JM, Newman AB. Gait variability and the risk of incident mobility disability in community-dwelling older adults. J Gerontol A Biol Sci Med Sci. 2007;62(9):983–988. doi:10.1093/gerona/62.9.983
14. Dumurgier J, Artaud F, Touraine C, et al. Gait speed and decline in gait speed as predictors of incident dementia. J Gerontol A Biol Sci Med Sci. 2017;72(5):655–661.
15. Ojagbemi A, D’Este C, Verdes E, Chatterji S, Gureje O. Gait speed and cognitive decline over 2 years in the Ibadan study of aging. Gait Posture. 2015;41(2):736–740. doi:10.1016/j.gaitpost.2015.01.011
16. Taniguchi Y, Yoshida H, Fujiwara Y, Motohashi Y, Shinkai S. A prospective study of gait performance and subsequent cognitive decline in a general population of older Japanese. J Gerontol A Biol Sci Med Sci. 2012;67(7):796–803. doi:10.1093/gerona/glr243
17. Allali G, Launay CP, Blumen HM, et al. Falls, cognitive impairment, and gait performance: results from the GOOD initiative. J Am Med Dir Assoc. 2017;18(4):335–340. doi:10.1016/j.jamda.2016.10.008
18. Montero-Odasso M, Muir SW, Hall M, et al. Gait variability is associated with frailty in community-dwelling older adults. J Gerontol A Biol Sci Med Sci. 2011;66(5):568–576. doi:10.1093/gerona/glr007
19. Lord SR, Lloyd DG, Nirui M, Raymond J, Williams P, Stewart RA. The effect of exercise on gait patterns in older women: a randomized controlled trial. J Gerontol A Biol Sci Med Sci. 1996;51(2):M64–70. doi:10.1093/gerona/51A.2.M64
20. Bohannon RW. Comfortable and maximum walking speed of adults aged 20-79 years: reference values and determinants. Age Ageing. 1997;26(1):15–19. doi:10.1093/ageing/26.1.15
21. Seino S, Shinkai S, Fujiwara Y, et al. Reference values and age and sex differences in physical performance measures for community-dwelling older Japanese: a pooled analysis of six cohort studies. PLoS One. 2014;9(6):e99487. doi:10.1371/journal.pone.0099487
22. Oberg T, Karsznia A, Oberg K. Basic gait parameters: reference data for normal subjects, 10-79 years of age. J Rehabil Res Dev. 1993;30(2):210–223.
23. Hollman JH, McDade EM, Petersen RC. Normative spatiotemporal gait parameters in older adults. Gait Posture. 2011;34(1):111–118. doi:10.1016/j.gaitpost.2011.03.024
24. McKay MJ, Baldwin JN, Ferreira P, et al. Spatiotemporal and plantar pressure patterns of 1000 healthy individuals aged 3-101 years. Gait Posture. 2017;58:78–87. doi:10.1016/j.gaitpost.2017.07.004
25. Fryzowicz A, Murawa M, Kabacinski J, Rzepnicka A, Dworak LB. Reference values of spatiotemporal parameters, joint angles, ground reaction forces, and plantar pressure distribution during normal gait in young women. Acta Bioeng Biomech. 2018;20(1):49–57.
26. Taniguchi Y, Watanabe Y, Osuka Y, et al. Characteristics for gait parameters of community-dwelling elderly Japanese with lower cognitive function. PLoS One. 2019;14(3):e0212646. doi:10.1371/journal.pone.0212646
27. Bioengineering B. P-WALK. Available from: https://www.btsbioengineering.com/products/p-walk/Accessed July 1, 2019.
28. Bilney B, Morris M, Webster K. Concurrent related validity of the GAITRite walkway system for quantification of the spatial and temporal parameters of gait. Gait Posture. 2003;17(1):68–74. doi:10.1016/S0966-6362(02)00053-X
29. Izquierdo-Renau M, Perez-Soriano P, Ribas-Garcia V, Queralt A. Intra and intersession repeatability and reliability of the S-Plate(R) pressure platform. Gait Posture. 2017;52:224–226. doi:10.1016/j.gaitpost.2016.12.001
30. Ramachandra P, Maiya AG, Kumar P. Test-retest reliability of the win-track platform in analyzing the gait parameters and plantar pressures during barefoot walking in healthy adults. Foot Ankle Spec. 2012;5(5):306–312. doi:10.1177/1938640012457680
31. Seino S, Shinkai S, Iijima K, et al. Reference values and age differences in body composition of community-Dwelling Older Japanese men and women: a pooled analysis of four cohort studies. PLoS One. 2015;10(7):e0131975. doi:10.1371/journal.pone.0131975
32. Cacciatore F, Abete P, Mazzella F, et al. Six-minute walking test but not ejection fraction predicts mortality in elderly patients undergoing cardiac rehabilitation following coronary artery bypass grafting. Eur J Prev Cardiol. 2012;19(6):1401–1409. doi:10.1177/1741826711427505
33. Levine RV, Lynch K, Miyake K, Lucia M. The type A city: coronary heart disease and the pace of life. J Behav Med. 1989;12(6):509–524. doi:10.1007/BF00844822
34. Broscheid KC, Zech A. Influence of barefoot, minimalist, and standard footwear conditions on gait and balance in healthy older adults. J Am Geriatr Soc. 2016;64(2):435–437. doi:10.1111/jgs.13980
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.