")
Back to Journals » Drug Design, Development and Therapy » Volume 10
Reducing the trigger dose of recombinant hCG in high-responder patients attending an assisted reproductive technology program: an observational study
Authors Tiboni GM, Colangelo EC, Ponzano A
Received 2 February 2016
Accepted for publication 17 March 2016
Published 18 May 2016 Volume 2016:10 Pages 1691—1694
DOI https://doi.org/10.2147/DDDT.S105607
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Wei Duan
Gian Mario Tiboni, Enrica Concetta Colangelo, Adalisa Ponzano
Department of Medicine and Aging Sciences, University “G d’Annunzio” of Chieti-Pescara, Chieti, Italy
Abstract: Decreasing the dose of human chorionic gonadotropin (hCG) used to trigger final oocyte maturation in assisted reproductive technology programs is regarded as a useful intervention in the prevention of ovarian hyperstimulation syndrome, but the minimal effective dose has not been yet identified. In this study, the capacity of a reduced dose of recombinant hCG (r-hCG) to provide adequate oocyte maturation was tested for the first time. Thirty-five high-responder patients received a dose of 125 µg (half of the standard dose) of r-hCG for triggering final oocyte maturation. The number of oocytes retrieved per patient and the proportion of mature oocytes were evaluated. As a result, a mean number of 14 oocytes were retrieved, of which 85% were found to be mature (MII). There was only one patient developing a moderate form of ovarian hyperstimulation syndrome and not requiring hospitalization. It is suggested that r-hCG at 125 µg can be effective in triggering final oocyte maturation in high-responder patients. Additional properly powered and controlled studies are needed to support this contention.
Keywords: recombinant hCG, low dose, triggering oocyte maturation, OHSS
Introduction
Human chorionic gonadotropin (hCG) has been adopted in cycles of assisted reproductive technology (ART) to effect the final oocyte maturation. Exogenous hCG can be used as a surrogate luteinizing hormone because of the high degree of homology between the two hormones. The clinical use of hCG in controlled ovarian stimulation for ART cycles is favored by the longer circulating half-life (>24 hours) of this hormone in comparison to luteinizing hormone (60 minutes).1 As major downside, hCG is a key determinant of ovarian hyperstimulation syndrome (OHSS), which is the major complication of controlled ovarian stimulation. The crucial role played by hCG in the initiation of OHSS is exemplified by the observations that when hCG is withheld, OHSS rarely occurs and that, on the other hand, multiple doses of hCG (as when hCG is used for luteal support) increase the incidence of OHSS.2 More to the point, endogenous production of hCG, associated with the pregnant status, is known to increase both OHSS severity and duration.3 OHSS has been estimated to occur in 1%–14% of ART women, albeit severe forms of OHSS are seen in 0.1%–2% of patients.3 Since the mechanisms and etiological factors behind OHSS are known only in part, its prevention primarily relies on the identification of high-risk patients and the application of preventive measures. The risk factors for OHSS include young age, high antral follicle count, polycystic ovary syndrome or PCO-like ovary, and previous OHSS.4 The preventive measures include coasting, use of gonadotropin-releasing hormone (GnRH) antagonists, agonist trigger in GnRH antagonist cycles, dopamine agonist therapy, freezing of all the embryos, and decreasing the trigger dose of hCG. Focusing on this latter intervention, a crucial prerequisite to lower hCG exposure is the identification of the minimal effective dose, ie, the hCG dose effective in reducing the occurrence of OHSS and, at the same time, effective in ensuring a sufficient number of mature oocytes.
Under such a concept, the purpose of this pilot study was to test, since never done before, whether a reduced dose of r-hCG (125 μg) is sufficient to trigger final oocyte maturation in a group of patients developing a hyper response during a long pituitary downregulation protocol for ART.
Patients and methods
This prospective observational cohort study included 35 high-responder infertile patients attending our infertility unit for in vitro fertilization (IVF) treatment between November 2013 and September 2014. Informed consent was obtained from all patients participating in the study. The study followed principles in the Declaration of Helsinki. Approval was not sought from the IRB since decreasing the trigger dose of hCG is a validated clinical approach in the prevention of OHSS which is routinely used in our ART unit. The ovarian stimulation protocol consisted of a luteal-phase GnRH agonist downregulation with buserelin acetate (Suprefact; Sanofi-Aventis, Bridgewater, NJ, USA) administered as a nasal spray at a daily dose of 0.9 mg starting on day 21 of the preceding cycle. Ovarian stimulation with recombinant follicle stimulating hormone (FSH; Gonal-f; Merck Serono S.p.A, Rome, Italy) was started on day 3 of full menstrual flow if pituitary suppression was complete as assessed by the absence of ovarian cysts on ultrasound scan, the presence of small antral follicles (diameter 2–6 mm), and an endometrial thickness <5 mm. The initial recombinant FSH dose (150 IU/d) was adjusted based on the ovarian response. From the fifth day of stimulation, the follicle size and number were monitored daily. The recombinant hCG (r-hCG) was administered when at least three follicles of 18 mm were present. Patients having an estradiol level ≥3,000 pg/mL but <5,000 pg/mL on the day of hCG administration were included in the study and received a dose of 125 μg of r-hCG (Ovitrelle; Merk Serono). This dosage is half of the current standard dose of r-hCG. Women with estradiol >5,000 pg/mL were coasted. Ovum pickup was scheduled 36 hours after r-hCG injection. All the IVF treatments were performed by intracytoplasmic sperm injection (ICSI). All the collected oocytes were denuded and their nuclear maturation stage determined. Embryo transfer was performed 72–76 hours after ovum pickup. The luteal phase was supported with 600 mg of micronized progesterone vaginally administered from the day after oocyte retrieval. Pregnancy test was performed by dosing βhCG serum blood, 14 days after embryo transfer. Clinical pregnancy was defined as the presence of a gestational sac with fetal heart activity visible on ultrasound scan at 7 weeks of gestation. OHSS was classified according to the criteria proposed by Golan et al.5
Results
The mean age of the 35 high-responder women included in the study was 34.46±4.27 years. They had a mean body mass index of 21.82±2.93 kg/m2 and a basal serum FSH of 6.83±1.42 mIU/mL. The main indications for ART were tubal factor (34.28%), male factor (28.57%), ovulatory factor (2.85%), endometriosis (5.71%), combined factor (8.57%), and unexplained infertility (20.00%). The cycle outcome of the patients is listed in Table 1. The mean duration of stimulation was 11.18±1.70 days. The total dose of FSH administered was 1,648±77 IU. The mean number of follicles with diameter >14 mm was 13.56±3.42. The mean number of oocytes collected was 13.80±4.40, with the number of mature oocytes (MII) being 11.64±4.40. The percentage of MII/oocytes retrieved per patient was 84.9±16.1 (95% CI -81.82%-88.18%). Fertilization and implantation rates were 88.0% and 14.74%, respectively. The mean number of transferred embryos was 2.71±0.46. There was a 34.26% (12/35) clinical pregnancy rate, with a 2.86% twin pregnancy rate. The delivery rate per clinical pregnancy was 83.33% (10/12).
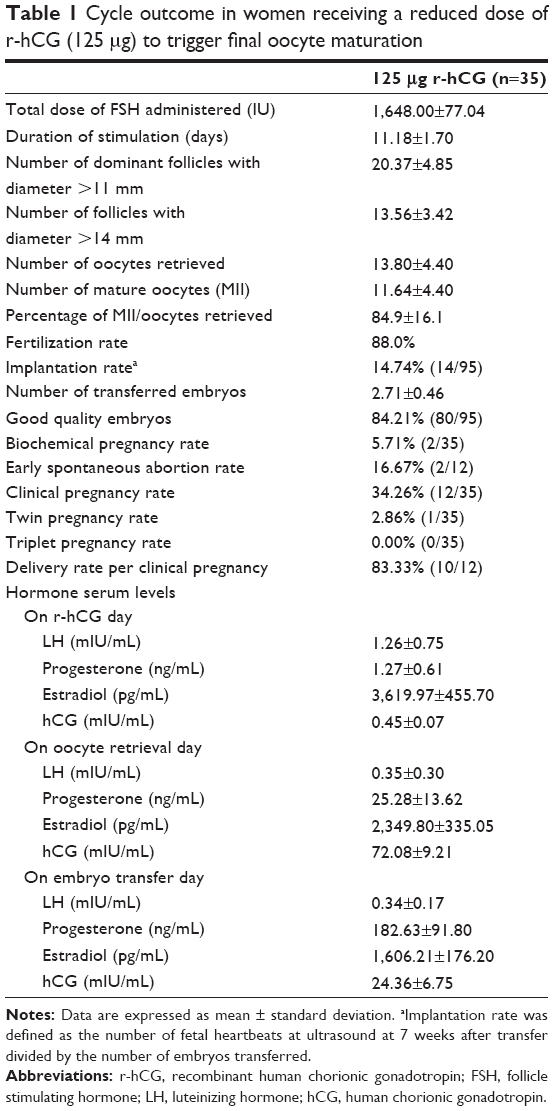 | Table 1 Cycle outcome in women receiving a reduced dose of r-hCG (125 μg) to trigger final oocyte maturation |
With respect to OHSS incidence, only one case (2.86%) of moderate OHSS was recorded. The patient was 28 years old and had an estradiol level on the hCG day of 3,890 pg/mL, with 25 oocytes retrieved. The patient did not require hospitalization.
Discussion
The link between hCG exposure and occurrence of OHSS has long been recognized, and circulating levels of hCG, along with the number of follicles, have been identified as the most significant predictor of OHSS risk.6 Decreasing the dose of hCG administered to trigger final oocyte maturation may have the potential to reduce OHSS incidence.7 Unfortunately, the lowest effective dose for ART programs has not yet been established.8 Urinary hCG (u-hCG) is commonly given at 10,000 IU with the dose of 5,000 IU representing the standard low dose. The value of a reduced dose regimen of r-hCG in triggering final follicular maturation has not yet been evaluated and formed the basis for this study. The obtained results suggest that a dose of r-hCG as low as 125 μg, corresponding to half of the standard dose, is feasible in triggering final oocyte maturation in high-responder patients. A mean number of 14 oocytes were retrieved after low-dose triggering. This number was comparable with the number of the follicles >14 mm (13.56±3.42) seen by ultrasound. Eighty-five percent of the collected eggs were found to be mature (MII). High progesterone levels were detected on oocyte retrieval day, indicating that the low r-hCG dose is effective in initiating early luteinization process.
As far as OHSS is considered, the reduced dose of r-hCG tested in this study did not fully prevent OHSS, since one patient developed a moderate form of the syndrome, not requiring hospitalization. Considering both safety and efficacy, 250 μg has been proposed as the dose of choice for triggering ovulation.9 This dosage corresponds to ~6,500 IU of u-hCG,10 and thus, the r-hCG dose tested in this study equals to 3,250 IU of u-hCG. In a pilot study involving 21 high-responder patients, Nargund et al11 found that a u-hCG dose as low as 2,500 IU was fully effective in preventing OHSS without compromising success rates. Triggering with a single bolus of 2,000 IU of u-hCG was found to be feasible to prevent OHSS in a small group of six hyperresponders.12 Abdalla et al13 reported that 2,000 IU was a less effective dose than 5,000 IU in ensuring adequate oocyte maturation, whereas doses of 5,000 IU and 10,000 IU were comparably effective. In randomized controlled trial in patients with polycystic ovary syndrome, Kolibianakis et al14 found comparable outcomes, in terms of fertilization rates and ongoing pregnancy, after triggering with u-hCG at 2,500 IU, 5,000 IU, or 10,000 IU. Nevertheless, triggering with 2,500 IU was associated with the lowest number of oocytes retrieved, the lowest fertilization rate, the lowest proportion of MII oocytes, and the highest proportion of patients with no embryos for transfer.14 The use of r-hCG offering high purity, high specific activity, and batch-to-batch consistency may help to precisely define the minimum effective trigger dose. Our results fit well with data from a retrospective review of IVF clinical data by Schmidt et al,15 showing a reduced dose of 3,300 IU of u-hCG as effective for final oocyte maturation with optimal fertilization rates and clinical pregnancy rates in high-response population. Kashyap et al7 assessed the impact of a sliding scale protocol for u-hCG trigger dose on OHSS incidence. The doses ranged between 3,300 and 10,000 IU depending on the estradiol level. Low-dose u-hCG appeared independently and significantly to reduce the risk of early and severe OHSS by factors of ~7 and ~4, respectively, without compromising the number of oocytes retrieved, the number of embryos available for transfer, or clinical pregnancy rates.7
Conclusion
It seems that a low r-hCG regimen does not compromise final oocyte maturation in high-responder women undergoing ICSI, although the lack of a control group and the small sample size limit the ability to make this conclusion as definitive. Further prospective randomized clinical trials on the same kind of population (ie, two groups of patients at the same risk of OHSS treated by full dose or alternatively by half dose of r-HCG) are needed to corroborate these preliminary findings.
Acknowledgment
This study is supported by internal funds.
Disclosure
The authors report no conflicts of interest in this work.
References
Ludwig M, Doody KJ, Doody KM. Use of recombinant human chorionic gonadotropin in ovulation induction. Fertil Steril. 2003;79(5):1051–1059. | ||
Humaidan P, Quartarolo J, Papanikolaou EG. Preventing ovarian hyperstimulation syndrome: guidance for the clinician. Fertil Steril. 2010;94(2):389–400. | ||
Navot D, Bergh PA, Laufer N. Ovarian hyperstimulation syndrome in novel reproductive technologies: prevention and treatment. Fertil Steril. 1992;58(2):249–261. | ||
Klemetti R, Sevón T, Gissler M, Hemminki E. Complications of IVF and ovulation induction. Hum Reprod. 2005;20(12):3293–3300. | ||
Golan A, Ron-el R, Herman A, Soffer Y, Weinraub Z, Caspi E. Ovarian hyperstimulation syndrome: an update review. Obstet Gynecol Surv. 1989;44(6):430–440. | ||
Shapiro BS, Daneshmand ST, Garner FC, Aguirre M, Ross R, Morris S. Effects of ovulatory serum concentration of human chorionic gonadotropin on the incidence of ovarian hyperstimulation syndrome and success rates for in vitro fertilization. Fertil Steril. 2005;84(1):93–98. | ||
Kashyap S, Parker K, Cedars MI, Rosenwaks Z. Ovarian hyperstimulation syndrome prevention strategies: reducing the human chorionic gonadotropin trigger dose. Semin Reprod Med. 2010;28(6):475–485. | ||
Tsoumpou I, Muglu J, Gelbaya TA, Nardo LG. Symposium: update on prediction and management of OHSS. Optimal dose of HCG for final oocyte maturation in IVF cycles: absence of evidence? Reprod Biomed Online. 2009;19(1):52–58. | ||
Al-Inany H, Aboulghar MA, Mansour RT, Proctor M. Recombinant versus urinary gonadotrophins for triggering ovulation in assisted conception. Hum Reprod. 2005;20(8):2061–2073. | ||
European Medicines Agency Science Medicines Health [webpage on the Internet]. Ovitrelle. Available from: http://www.ema.europa.eu/ema/index.jsp?curl=pages/medicines/human/medicines/000320/human_med_000964.jsp. Accessed April 6, 2016. | ||
Nargund G, Hutchison L, Scaramuzzi R, Campbell S. Low-dose HCG is useful in preventing OHSS in high-risk women without adversely affecting the outcome of IVF cycles. Reprod Biomed Online. 2007;14(6):682–685. | ||
Chen X, Chen SL, He YX, Ye DS. Minimum dose of hCG to trigger final oocyte maturation and prevent OHSS in a long GnRHa protocol. J Huazhong Univ Sci Technolog Med Sci. 2013;33(1):133–136. | ||
Abdalla HI, Ah-Moye M, Brinsden P, Howe DL, Okonofua F, Craft I. The effect of the dose of human chorionic gonadotropin and the type of gonadotropin stimulation on oocyte recovery rates in an in vitro fertilization program. Fertil Steril. 1987;48(6):958–963. | ||
Kolibianakis EM, Papanikolaou EG, Tournaye H, Camus M, Van Steirteghem AC, Devroey P. Triggering final oocyte maturation using different doses of human chorionic gonadotropin: a randomized pilot study in patients with polycystic ovary syndrome treated with gonadotropin-releasing hormone antagonists and recombinant follicle-stimulating hormone. Fertil Steril. 2007;88(5):1382–1388. | ||
Schmidt DW, Maier DB, Nulsen JC, Benadiva CA. Reducing the dose of human chorionic gonadotropin in high responders does not affect the outcomes of in vitro fertilization. Fertil Steril. 2004;82(4):841–846. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.