")
Back to Journals » Clinical Interventions in Aging » Volume 12
Prevalence and pattern of the elongated styloid process among geriatric patients in Saudi Arabia
Authors AlZarea BK
Received 9 December 2016
Accepted for publication 4 March 2017
Published 30 March 2017 Volume 2017:12 Pages 611—617
DOI https://doi.org/10.2147/CIA.S129818
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 6
Editor who approved publication: Dr Richard Walker
Bader K AlZarea
Department of Prosthodontics, College of Dentistry, AlJouf University, Sakaka, Kingdom of Saudi Arabia
Objective: The objectives of this study were to assess the elongation of the styloid process on digital panoramic radiographs and to evaluate the prevalence of the elongation according to age, sex and types.
Patients and methods: Digital panoramic radiographs of 198 geriatric edentulous patients were analyzed. The radiographic length of the styloid process was measured on both sides using the measurement toolbars on the accompanying analysis software. For statistical analysis, Student’s t-test, chi-square test and analysis of variance test were used.
Results: The elongated styloid process was seen in 87 of the 198 patients. It was observed that as age increased, elongation of the styloid process increased with a male predominance. Type I elongation was more common than other types of elongation. Bilateral elongation was most commonly found than unilateral elongation, and both types of elongation were frequently seen in males compared with females.
Conclusion: The prevalence of the elongated styloid process in the present study was higher in comparison to the other reports from edentulous patients.
Keywords: styloid process, elongation, digital panoramic radiographs
Introduction
The term styloid process has been gleaned from the word “stylos”, which implies the pillar in Greek dialect. The styloid process appertains to the temporal bone of the skull, and it abuts front to the stylomastoid foramen.1 Stylopharyngeus, stylohyoid, styloglossus muscles, stylohyoid and stylomandibular ligaments are attached to the styloid process.2 The length of the styloid process is reported to range between 15.2 mm and 47.7 mm,3 and various authors have observed that the normal length of the styloid process is between 20 mm and 30 mm,3–9 with length >30 mm regarded as elongated.2/a>–4#8211;4,7–13 This elongation of the styloid process or calcification of ligaments, which is the cause of the stylohyoid syndrome or Eagle syndrome, was first reported by the otorhinolaryngologist Eagle.14
Individuals with Eagle syndrome may report neck and cervicofacial pain, difficulty in swallowing and pain at the angle of the mandible, which aggravates while rotating the neck or during protrusion of the tongue. It is proposed that these features are manifested due to the pressure of the styloid process on the neural and vascular structures, which are in its vicinity.15 Differential diagnoses in these patients include cranial nerve neuralgias, unerupted or impacted tooth, temporal arthritis, diseases of the temporomandibular joint, migraine headaches, pharyngotonsillitis and head and neck tumors.2,4 The etiology of the elongation of the styloid process is not yet exactly determined, but the congenital elongation of the styloid process, calcification of the stylohyoid ligament and growth of osseous tissue where the stylohyoid ligament inserts are regarded as few of the causative factors.16,17 Radiographic studies report the prevalence of the elongated styloid process from 2% to 30%.2,6,9,18,19 Elongation may be seen in both sexes, unilaterally or bilaterally and more commonly in elderly individuals.15 Elongation of the styloid process can be determined if this structure is palpable in the region of ipsilateral tonsillar fossa clinically. Nevertheless, the panoramic radiograph taken for various reasons frequently demonstrates the elongation of the styloid process, considering that most of the individuals are devoid of symptoms.19 Although the panoramic radiograph is the more common radiographic view to detect the elongation of the styloid process, other views such as posterior–anterior projection of the mandible, lateral oblique projection of the mandible and axial and cephalometric radiographs can also aid in establishing the elongated process.20
The present study was carried out in the edentulous population of the Kingdom of Saudi Arabia with the following aims and objectives:
- To measure and assess the length of the styloid process on digital panoramic radiographs
- To determine the variation in age, sex, type and sides of the elongated styloid process
- To compare the length of the styloid process between the right and left sides
- To compare the type or pattern of the elongation of the styloid process with the length
Patients and methods
The present study was carried out in the College of Dentistry, AlJouf University, Kingdom of Saudi Arabia. Panoramic radiographs of patients who were >60 years of age, attending the Department of Prosthodontics with various complaints, were examined from January 2015 to January 2016. Clearance was obtained from the ethical committee of the College of Dentistry, AlJouf University, and written consent was obtained from all the participants. Written consent was provided for publication of the accompanying images.
In this study, 198 radiographs were obtained using a digital panoramic imaging system. The radiographic apparatus used was Cranex (Soredex, Tuusula, Finland). The apparent lengths of the styloid process were measured with the aid of measurement tools on the accompanying application software (Digora compatible software DfW 2.6, Soredex). Those radiographs showing the styloid processes of both sides were included in the study, and radiographs with artifacts and those with patient positioning and magnification errors were excluded from the study. The length of the styloid process was measured on the frontal side of the styloid process, from its originating point from the tympanic plate to the tip of the process, regardless of whether the styloid process was segmented (Figure 1). The styloid process that measured >30 mm was considered as elongated, and the one not exceeding 30 mm was regarded as normal. Elongated styloid processes were categorized according to the classification based on radiologic features by Langlais et al as follows: type I as elongated, type II as pseudoarticulated and type III as segmented. The radiographic presentation of type I, of mineralized complex, is seen as an uninterrupted integrity of the stylohyoid complex regardless of its length (Figure 2). In the type II, the styloid process is apparently joined to the mineralized stylomandibular or stylohyoid ligament by a single pseudoarticulation (Figure 3). Type III comprises either short or long noncontinuous portions of the styloid complex or interrupted segments of mineralized styloid ligament (Figure 4).21
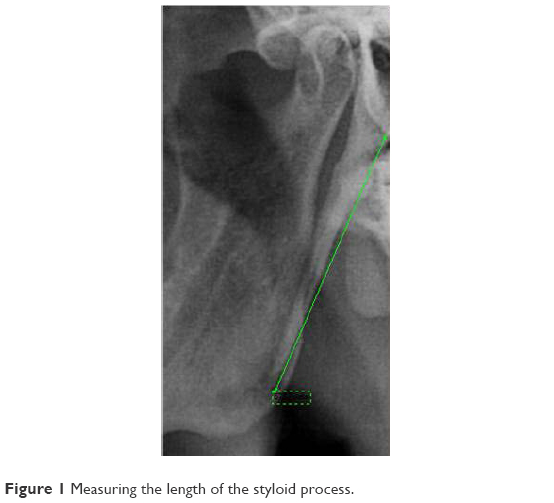 | Figure 1 Measuring the length of the styloid process. |
 | Figure 2 Type I – uninterrupted styloid process. |
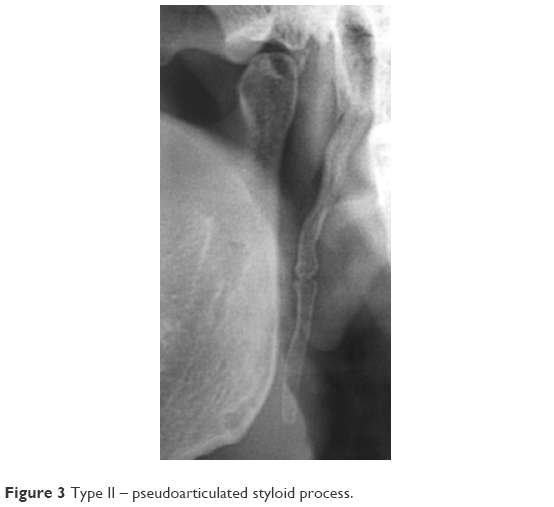 | Figure 3 Type II – pseudoarticulated styloid process. |
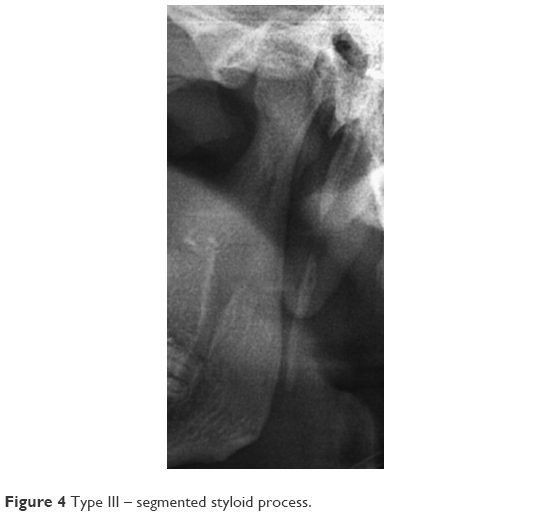 | Figure 4 Type III – segmented styloid process. |
To obtain percentiles for different ages, the radiographs were categorized into three age groups, comprising individuals belonging to the age groups of 60–69 years, 70–79 years and ≥80 years. The collected data were categorized according to age, sex, normal length and elongated length and type or pattern of the elongation of the styloid process on both the right and left sides.
All the radiographs were evaluated by two qualified and experienced observers. In order to check the intraobserver variations, the same examiners repeated measurements after 2 weeks.
Statistical methods
Data were analyzed using SAS 9.2, SPSS 20.0, Stata 10.1, MedCalc 9.0.1, Systat 12.0 and R environment ver.2.11.1 (IBM Corporation, Armonk, NY, USA).
Descriptive and inferential statistical analyses were carried out in the present study. Results on continuous measurements are presented as mean ± standard deviation (SD) (Min–Max), and results of categorical measurements are presented in number and percentage. Significance is assessed at the level of 5%. The following assumptions on data were made:
- Dependent variables should be normally distributed.
- Samples drawn from the population should be random; cases of the samples should be independent.
Analysis of variance was used to find the significance of study parameters between three groups of patients. Student’s t-test (two tailed, independent) was used to find the significance of study parameters on a continuous scale between two groups (intergroup analysis) on metric parameters. Chi-square test was used to find the significance of study parameters on a categorical scale between two or more groups. The reliability of measurements was evaluated by kappa statistics.
Results
The reliability was very good, with kappa values of 0.91 for intraoperator agreement and 0.84 for interoperator agreement. Panoramic radiographs of 198 patients, of whom 103 were males and 95 were female subjects, who were aged ≥60 years, were studied. Among them, 94 subjects belonged to the age group of 60–69 years, 75 subjects belonged to the age group of 70–79 years and 29 subjects were aged ≥80 years.
The length of the styloid process (mm) according to age and sex is represented in Table 1. It was observed that the length of the styloid process increased with an increasing age and the length of the styloid process was more in males compared with females. Type I elongation was more common than other types of elongation on both the right and left sides (Table 2). The length of the elongated styloid process on the right side was less than that on the left side (35.92±7.55), which was significantly more compared to the right side (Table 3).
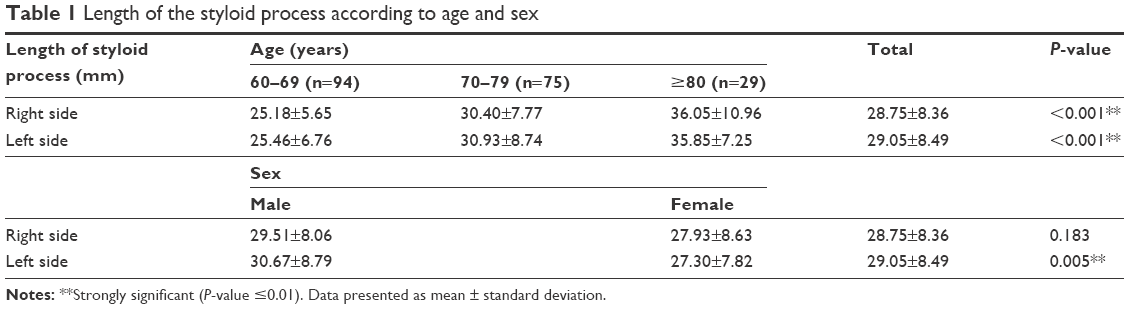 | Table 1 Length of the styloid process according to age and sex |
 | Table 2 Type of elongation of the styloid process |
 | Table 3 Length of the styloid process according to the type of elongation on the right and left sides |
It was observed that a maximum numbers of patients with all the three types of elongation had length in the range of 31–40 mm on both sides (Tables 4 and 5).
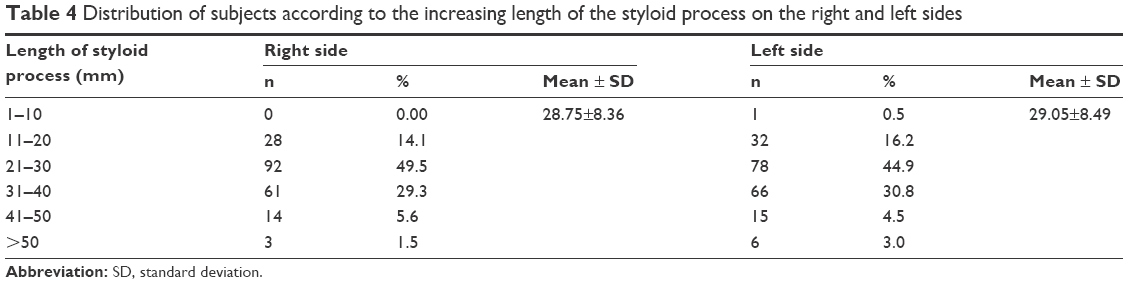 | Table 4 Distribution of subjects according to the increasing length of the styloid process on the right and left sides |
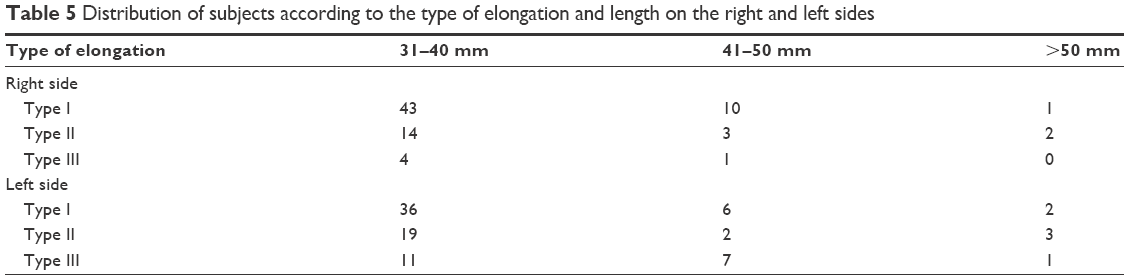 | Table 5 Distribution of subjects according to the type of elongation and length on the right and left sides |
On the right side, type I and type III elongations were more common in patients aged 70–79 years, and type II was more common in patients aged ≥80 years. On the left side, all the three types of elongation were most commonly found in the patients aged 70–79 years (Table 6).
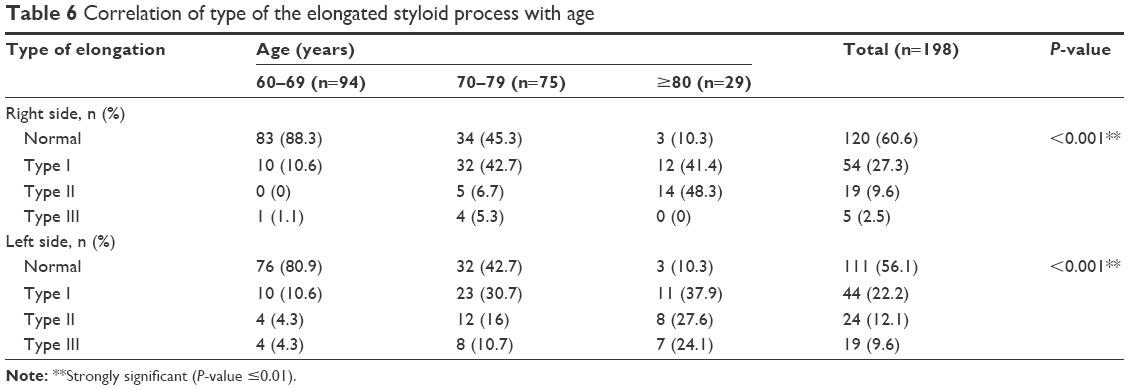 | Table 6 Correlation of type of the elongated styloid process with age |
When compared between the sexes, on the right side, type I and type III elongations were more common in males and type II elongation was more common in females. On the left side, all the three types of elongation were more common in males (Table 7).
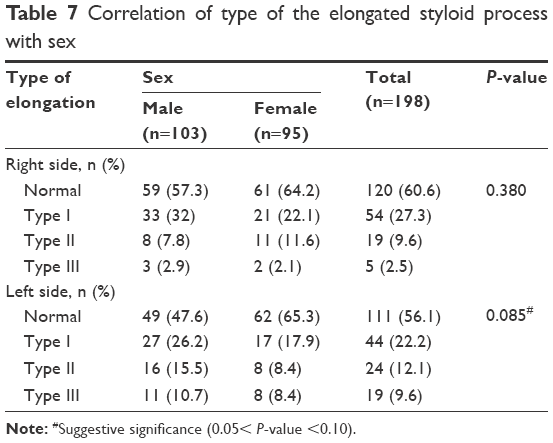 | Table 7 Correlation of type of the elongated styloid process with sex |
Bilateral elongation was most commonly found (71.4%) than unilateral elongation (28.6%). It was also found that unilateral and bilateral elongations were frequently seen in males compared to females (Table 8).
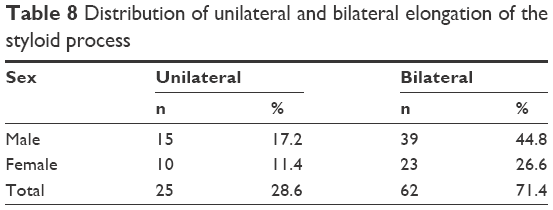 | Table 8 Distribution of unilateral and bilateral elongation of the styloid process |
Discussion
There are assortments of approaches to decide the measurements of the styloid process and analyze Eagle syndrome: panoramic radiographs, lateral views of the neck and processed computed tomography.2,7,8 In some cases, the lengthened styloid process can be clinically recognized by palpating over the tonsillar fossa.22
Scaf et al20 demonstrated that the mineralization of the styloid process is considered present if its length is 30 mm or surpassing from the temporal bone on the panoramic radiographs.
In the present study, it was observed that there was an increase in the length of the styloid process as age increased, which was consistent with the studies by various researchers.19,20,23–25 However, these findings differed from others who suggested that age may not have a role in elongation.18,26
In the present study, it was found that males had more elongated styloid processes than females, which was in accordance with More and Aarani.27 However, in the studies conducted by Roopashri et al,23 Phulambrikar et al24 and Ferrario et al,28 it was found that females had an elongated styloid process than males, but their data were not statistically significant. In the study carried out by Scaf et al,20 an equal distribution of the elongated styloid process in males and females was observed.
In the present study, it was found that type I elongation was more common than other types of elongation on both right and left sides and the data were statistically significant; these observations were similar to the findings reported by few other studies.23,27,29
In this study, the length of the elongated styloid process on the left side was significantly more when compared to the right side. This finding was in accordance with Bozkir et al,19 Vadgaonkar et al,22 Roopashri et al23 and Shaik et al30 However, More and Aarani27 observed that the elongated styloid process was more common on the right side in their study population. Ilgüy et al6 and Custodio et al31 observed no difference in the length of the styloid process when the sides were compared.
Bilateral elongation was most commonly found than unilateral elongation in this study; this finding was consistent with those of other studies.19,23,26,28 Scaf et al noted that the majority of the elongated styloid process was unilateral. It was also found that unilateral and bilateral elongations were frequently seen in males compared to females. However, in the study conducted by and Bozkir et al19 and Roopashri et al,23 it was found that bilateral elongation was frequently seen in females than unilateral elongation.
In the present study, a high prevalence (43.93%) of the elongated styloid process was observed; in contrast to this, Keur et al,2 Bozkir et al,19 Scaf et al20 and Correll et al26 reported a prevalence of <30% in edentulous individuals. This difference may be due to the older age group of the participants in this study compared to the abovementioned studies.
Conclusion
It is vital for the dental practitioner to be aware of the structural deviations of the styloid process whose clinical significance is not well established. Elongation of the styloid process may be a fortuitous asymptomatic radiographic observation. Panoramic radiographs are economical and can demonstrate the exact status of the elongated styloid process that can establish the diagnosis, thus averting misinterpretation of the symptoms as pain originating from tonsillar tissues, odontogenic apparatus or from any other sources. The present study showed a higher prevalence of the elongated styloid process, which is in comparison to the other reports from edentulous patients.
Disclosure
The author reports no conflicts of interest in this work.
References
Standing S. Skull and mandible. Gray’s Anatomy. The Anatomical Basis of Clinical Practice. 39th ed. Edinburg: Elsevier; 2005:470. | ||
Keur JJ, Campbell JP, McCarthy JF, Ralph WJ. The clinical significance of the elongated styloid process. Oral Surg Oral Med Oral Pathol. 1986;61(4):399–404. | ||
Sisman Y, Gokce C, Sipahioglu M, Tarim Ertas E, Oymak O, Utas C. Bilateral elongated styloid process in an end-stage renal disease patient with peritoneal dialysis: is there any role for ectopic calcification? Eur J Dent. 2008;3(2):155–157. | ||
Krennmair G, Piehslinger E. Variations of ossification in the stylohyoid chain. Cranio. 2003;21(1):31–37. | ||
Monsour PA, Young WG. Variability of the styloid process and stylohyoid ligament in panoramic radiographs. Oral Surg Oral Med Oral Pathol. 1986;61(5):522–526. | ||
Ilgüy M, Ilgüy D, Güler N, Bayirli G. Incidence of the type and calcification patterns in patients with elongated styloid process. J Int Med Res. 2005;33(1):96–102. | ||
Kursoglu P, Unalan F, Erdem T. Radiological evaluation of the styloid process in young adults resident in Turkey’s Yeditepe University faculty of dentistry. Oral Surg Oral Med Oral Pathol Oral Radiol Oral Endod. 2005;100(4):491–494. | ||
Jung T, Tschernitschek H, Hippen H, Schneider B, Borchers L. Elongated styloid process: when is it really elongated? Dentomaxillofac Radiol. 2004;33(2):119–124. | ||
Öztunç H, Evlice B, Tatli U, Evlice A. Cone-beam computed tomographic evaluation of styloid process: a retrospective study of 208 patients with orofacial pain. Head Face Med. 2014;10:5. | ||
da Costa RS, Camargo Fontanella VR. Anatomical changes of the styloid process in a Brazilian subpopulation. J Dent Health Oral Disord Ther. 2014;1(1):00006. | ||
Vieira EM, Guedes OA, Morais SD, Musis CRD, Albuquerque PA, Borges ÁH. Prevalence of elongated styloid process in a Central Brazilian Population. J Clin Diagn Res. 2015;9(9):ZC90–ZC92. | ||
Chabikuli NJ, Noffke CEE. Styloid process elongation according to age and gender: a radiological study. S Afr Dent J. 2016;71(10):470–473. | ||
Alpoz E, Akar GC, Celik S, Govsa F, Lomcali G. Prevalence and pattern of stylohyoid chain complex patterns detected by panoramic radiographs among Turkish population. Surg Radiol Anat. 2014;36(1):39–46. | ||
Eagle WW. Elongated styloid process. Report of two cases. Arch Otolaryngol. 1937;25:548–587. | ||
Neville BW, Damm DD, Allen CM, Bouquot JE. Developmental defects of the oral and maxillofacial region. In: Neville BW, Damm DD, Allen CM, Bouquot JE, editors. Oral and Maxillofacial Pathology. Philadelphia, PA: W.B. Saunders Company; 1996:1–43. | ||
Camarda AJ, Deschamps C, Forest D. I. Stylohyoid chain ossification: a discussion of etiology. Oral Surg Oral Med Oral Pathol. 1989;67(5):508–514. | ||
Camarda AJ, Deschamps C, Forest D. II. Stylohyoid chain ossification: a discussion of etiology. Oral Surg Oral Med Oral Pathol. 1989;67(5):515–520. | ||
Gokce C, Sisman Y, Tarim Ertas E, Akgunlu F, Ozturk A. Prevalence of styloid process elongation on panoramic radiography in the Turkey population from Cappadocia region. Eur J Dent. 2008;2(1):18–22. | ||
Bozkir MG, Boga H, Dere F. The evaluation of elongated styloid process in panoramic radiographs in edentulous patients. Tr J Medical Science. 1999;29:481–485. | ||
Scaf G, Freitas DQ, Loffredo Lde C. Diagnostic reproducibility of the elongated styloid process. J Appl Oral Sci. 2003;11(2):120–124. | ||
Langlais RP, Miles DA, Van Dis ML. Elongated and mineralized stylohyoid ligament complex: a proposed classification and report of a case of Eagle’s Syndrome. Oral Surg Oral Med Oral Pathol. 1986;61(5):527–532. | ||
Vadgaonkar R, Murlimanju BV, Prabhu LV, et al. Morphological study of styloid process of the temporal bone and its clinical implications. Anat Cell Biol. 2015;48(3):195–200. | ||
Roopashri G, Vaishali MR, David MP, Baig M, Shankar U. Evaluation of elongated styloid process on digital panoramic radiograph. J Contemp Dent Pract. 2012;13(5):618–622. | ||
Phulambrikar T, Rajeshwari A, Rao BB, Warhekar AM, Reddy P. Incidence of elongated styloid process: a radiographic study. J Indian Acad Oral Med Radiol. 2011;23(3):344–346. | ||
Anbiaee N, Javadzadeh A. Elongated styloid process: is it a pathologic condition. Indian J Dent Res. 2011;22(5):673–677. | ||
Correll RW, Jensen JL, Taylor JB, Rhyne RR. Mineralization of the stylohyoid- stylomandibular ligament complex. A radiographic incidence study. Oral Surg Oral Med Oral Pathol. 1979;48(4):286–291. | ||
More CB, Aarani MK. Evaluation of the styloid process on digital panoramic radiograph. Indian J Radiol Imaging. 2010;20(4):261–265. | ||
Ferrario VF, Sigurta D, Daddona A, et al. Calcification of the stylohyoid ligament incidence and morphoquantitative evaluations. Oral Surg Oral Med Oral Pathol. 1990;69(4):524–529. | ||
Shah SP, Praveen NB, Syed V, Subhashini AR. Elongated styloid process: a retrospective panoramic radiographic study. World J Dent. 2012;3(4):316–319. | ||
Shaik MA, Naheeda, Kaleem SM, Wahab A, Hameed S. Prevalence of elongated styloid process in Saudi population of Aseer region. Eur J Dent. 2013;7(4):449–454. | ||
Custodio ALN, Silva MR, Abreu MH, Araújo LR, de Oliveira LJ. Styloid process of the temporal bone: morphometric analysis and clinical implications. Biomed Res Int. 2016;2016:8792725. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.