")
Back to Journals » Clinical Interventions in Aging » Volume 14
Preliminary study on the effects of movement velocity training of the upper limbs on gait ability in older adults: a nonrandomized controlled trial
Authors Yamamoto S, Iwata A , Yano Y, Ohmine T, Honma K, Senzaki K, Fujiwara M, Murakami T, Inoue J, Sano Y, Okagawa S, Otsuki Y, Wanaka H, Kataoka M, Iwata H
Received 25 January 2019
Accepted for publication 20 February 2019
Published 1 May 2019 Volume 2019:14 Pages 781—788
DOI https://doi.org/10.2147/CIA.S202897
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Richard Walker
Saki Yamamoto,1 Akira Iwata,1 Yuki Yano,1 Toshimitsu Ohmine,1 Keisuke Honma,1 Kazuma Senzaki,1 Minami Fujiwara,1 Takayuki Murakami,1 Junji Inoue,1 Yuki Sano,2 Shuji Okagawa,3 Yuta Otsuki,4 Hideyuki Wanaka,5 Masataka Kataoka,1 Hiroshi Iwata6
1Department of Physical Therapy, Faculty of Comprehensive Rehabilitation, Osaka Prefecture University, Habikino, Osaka, Japan; 2Department of Rehabilitation, Osaka General Medical Center, Osaka, Osaka, Japan; 3Department of Rehabilitation, Tatsumi Hospital, Ikeda, Osaka, Japan; 4Department of Rehabilitation, Kisei Hospital, Osaka, Osaka, Japan; 5Department of Rehabilitation, Kobe Rosai Hospital, Kobe, Hyogo, Japan; 6Department of Cardiovascular Medicine, Juntendo University Graduate School of Medicine, Bunkyo-ku, Tokyo, Japan
Purpose: Movement velocity of the limbs or trunk plays an important determinant of gait speed in older adults. Movement velocity-focused training of the lower limbs or trunk has recently been shown to be an effective intervention to improve gait ability. Because movement velocities of various body regions are significantly correlated, movement velocity training of the upper limbs may also be effective for improving gait speed. Therefore, the purpose of this study was to investigate whether movement velocity training of the upper limbs in a seated position is effective for improving gait ability.
Patients and methods: This study was a nonrandomized controlled trial. The participants were older adults residing in geriatric health service facilities. They were assigned to the movement velocity training of the upper limbs group (n=26) or control group (n=15). The participants in the training group performed exercises (three times per week for 10 weeks) to move the upper limbs as quickly as possible. The outcomes were gait speed, movement velocity, and quadriceps strength. These measurements were performed preintervention and 4, 8, and 10 weeks after intervention.
Results: A significant time–group interaction was found for maximum gait speed and movement velocity of the upper limbs. Bonferroni post-hoc test showed significant improvement in gait speed between preintervention and 10 weeks after intervention in the training group. The movement velocity of the upper limbs was significantly improved between preintervention and 4, 8, and 10 weeks after intervention.
Conclusion: Movement velocity training of the upper limbs showed significant and clinically relevant improvements in maximum gait speed at 10 weeks after intervention. This training is a potentially useful intervention and can be safely performed.
Keywords: older people, movement velocity training, arm, gait speed, seated position
Introduction
Gait speed is a useful predictor of falls, hospitalization, activities of daily living disability, and survival in older adults.1–4 Gait speed is affected by various factors such as age,5 gender,6 muscle strength,7 and muscle power.8 In addition to these factors, movement velocity, which is defined by the speed to move the limbs or trunk as fast as possible, plays an important determinant of gait speed in older adults.9–12 Movement velocity of the lower limbs (knee extensor and ankle planter flexor) was reported to be more correlated with gait speed compared with quadriceps strength.9,10 Movement velocity of the trunk is also significantly associated with gait speed.11 Moreover, movement velocity is a significant determinant of gait speed even in the upper limbs.12 Therefore, movement velocity regardless of any body region is a good determinant of gait speed.
Many studies have investigated the influence of complex training of various body parts focusing on movement velocity on gait speed.13,14 For example, movement velocity training of the upper and lower limbs (leg extension, bench press, ball throwing, countermovement jump, curl up, and back extension) is effective in improving gait ability.13 Furthermore, movement velocity training with no load of the upper and lower limbs (seated row, chest press, shoulder press, biceps curl, triceps extension, knee extension, and knee curl) is effective for improving gait speed compared with traditional muscle strength training.14 In addition to these complex training programs, movement velocity training of one part of the body is also effective for improving gait speed. Movement velocity training of the lower limbs using an ergometer has been reported to significantly improve gait speed.15 We previously clarified that the seated side tapping training, which focuses on trunk movement velocity, is an effective intervention to improve gait ability in patients with total knee arthroplasty.16 These findings indicated that both complex training and one-part movement velocity training have good effects on improving gait. In addition, a significant and moderate correlation is observed between movement velocities of various body regions (r = −0.42–0.61).17
Based on these findings, movement velocity has three characteristics. First, movement velocities of any body part are related to gait ability. Second, movement velocity training of the lower limbs or trunk improves gait ability. Third, movement velocities are moderately correlated with each other. Because the movement velocities of different body regions are related to each other and movement training of the lower limbs and trunk is effective for gait improvement, movement velocity training that focuses on the upper limbs may also be effective for improving gait speed.
Movement velocity training of the upper limbs can be carried out in a seated position; thus, the risk of falls is much lower than training in a standing position or walking. Furthermore, the patients who cannot load their body weight on their legs due to pain or load restriction can perform the training safely. In this study, we aimed to investigate whether movement velocity training of the upper limbs in a seated position is effective for improving gait ability.
Material and methods
Study design and participants
This study was a nonrandomized controlled trial. Participants were recruited by physical therapists from three geriatric health services facilities in Osaka, Japan. The inclusion criteria of the study were as follows: 1) older adults in geriatric health service facilities; 2) aged ≥65 years; 3) the ability to walk at least 8 m with or without an assistive device; 4) the ability to rise from a chair; and 5) the ability to understand and follow instructions. Participants assigned to the training and control groups were recruited between August 2014 and October 2016 and between September 2015 and August 2018, respectively. We set the interval of recruitments more than one year at each facility to wait for the turnover of facility residents. Both groups do not contain the same participants. This study conformed to the ethical principles contained in the Declaration of Helsinki, and was approved by the Human Ethics Committee of Osaka Prefecture University (approval number: 2014–104). All participants gave written informed consent.
Intervention
Movement velocity training of the upper limbs was conducted three times a week for 10 weeks. The training consisted of five types of exercise to move as fast as possible, and no external load was carried other than the items used (a Japanese fan, towel, and stick). Each exercise comprised the following: 1) shoulder horizontal flexion/extension exercise using a Japanese fan (three sets of 10 repetitions); 2) shoulder flexion/extension exercise using a Japanese fan (three sets of 10 repetitions); 3) shoulder horizontal flexion/extension exercise using a towel (three sets of 10 s); (4) shoulder flexion exercise using a stick (five sets of 10 repetitions); and 5) elbow extension exercise using a stick (five sets of 10 repetitions) (Figure 1). Each training was conducted for approximately 20 mins, including stretching of the upper limbs and light exercise (stepping in sitting position). Participants were instructed to move the entire range of motion as fast as possible.
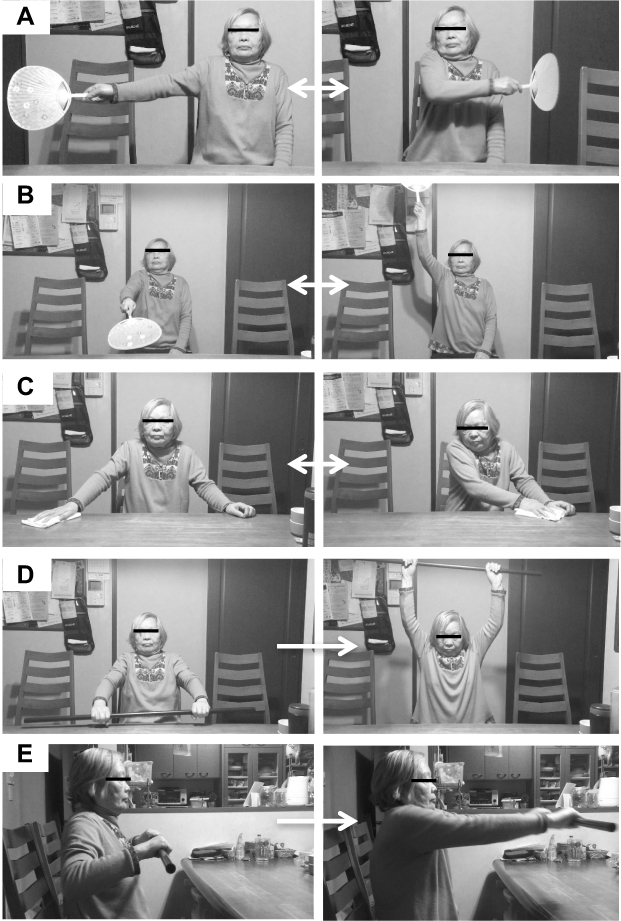 | Figure 1 Movement velocity training of the upper limbs. (A) Shoulder horizontal flexion/extension exercise using a Japanese fan. (B) Shoulder flexion/extension exercise using a Japanese fan. (C) Shoulder horizontal flexion/extension exercise using a towel. (D) Shoulder flexion exercise using a stick. (E) Elbow extension exercise using a stick. |
Measurements
Measurements of mobility
To assess gait speeds, the participants were instructed to walk along an 8-m walkway at their maximal and usual speeds. The 1.5-m space at each end of the walkway for acceleration and deceleration was not timed.11 Maximum and usual gait speeds were measured twice using a stopwatch, and the fastest time was used for analyses.
Timed up and go (TUG) was measured using the method described by Podsiadlo and Richardson.18 Before the measurement, the examiner demonstrated how to perform the TUG and then instructed the participants to stand up, walk 3-m at their usual speed, cross a line, turn around, walk back, and sit down again. The participants were also encouraged to wear their regular footwear and use their walking aids.
The short physical performance battery (SPPB) was evaluated by measuring three physical performance tasks: usual gait speed, maintenance of standing balance, and sit to stand test.19 The corresponding tasks include walking at usual speed over 4 m, three static positions with decreasing base of support to challenge balance, and the ability to rise from a chair without the use of the arms five times as rapidly as possible. Result from each test was ranked using a 0–4 scale, and participants who showed high abilities had higher total scores.
Measurements of movement velocity
Movement velocity of the upper limbs measured the time required to move a small plastic box (90 mm × 60 mm × 20 mm, 200 g) 30 cm laterally as fast as possible using a precision timer.12 According to a previous research, an acceleration area of 10 cm was set on a table. The participants were instructed to move the plastic box over the end line as fast as possible using their right hand. This test was measured five times after two practice trials, and the best time was taken for further analysis.
The maximal joint angular velocity of knee extension was measured to represent movement velocity of the lower limbs.9 A gyroscope (45 mm×25 mm×15 mm; Micro Stone Inc., Saku, Japan) and a 2-kg ankle weight were fixed on the distal position of the tibia. The participants were asked to sit in a chair with their knees and hips at 90 degrees of flexion and to keep their trunk upright. The participants were instructed to extend their knees as quickly as possible. They performed the task five times consecutively.
Measurements of muscle strength
Isometric quadriceps strength was measured with a handheld dynamometer.20 The measurement was performed with the participants in a sitting position, with the hips and knees in approximately 90 degrees of flexion.
Statistical analysis
All variables were expressed as mean and SDs. Differences in baseline characteristics including demographic information between the groups were evaluated using the Student t test. Pearson’s correlation coefficient was conducted to demonstrate the correlation between gait ability and movement velocity. A repeated-measures ANCOVA was performed to examine the main effects of time and interaction between the groups and time. In this analysis, gait ability, movement velocity, and muscle strength measurement values of each time point were included as levels of the within-subject “time” factor. Training and control groups were included as levels of the within-subject “group” factors. Baseline measurements were included as covariates. Differences between preintervention and each time point were examined using post-hoc analysis (Bonferroni test). Effect sizes were measured using partial η2. In a previous study, partial η2 of 0.01, 0.06, and 0.14 may be considered the boundaries for small, medium, and large effects, respectively.21 For all analyses, the level of statistical significance was set at p<0.05 (two-tailed). Statistical analysis was performed according to the standard methods using SPSS version 24.0 (IBM Japan, Ltd., Tokyo, Japan).
Results
Flowchart of participant recruitment and retention in this study is shown in Figure 2. From a pool of 94 participants, 70 adults were eligible to participate, with 24 participants dropping out. Seventeen participants from the movement velocity training group dropped out from the study due to declined (n=4), health conditions unrelated to the study (n=9), discharged from facility (n=3), and questionable data (n=1). A total of 12 participants dropped out from the control group due to declined (n=1), health conditions unrelated to the study (n=7), and discharged from facility (n=4). None of the participants complained of upper limb pain or showed obvious distress due to the training protocol.
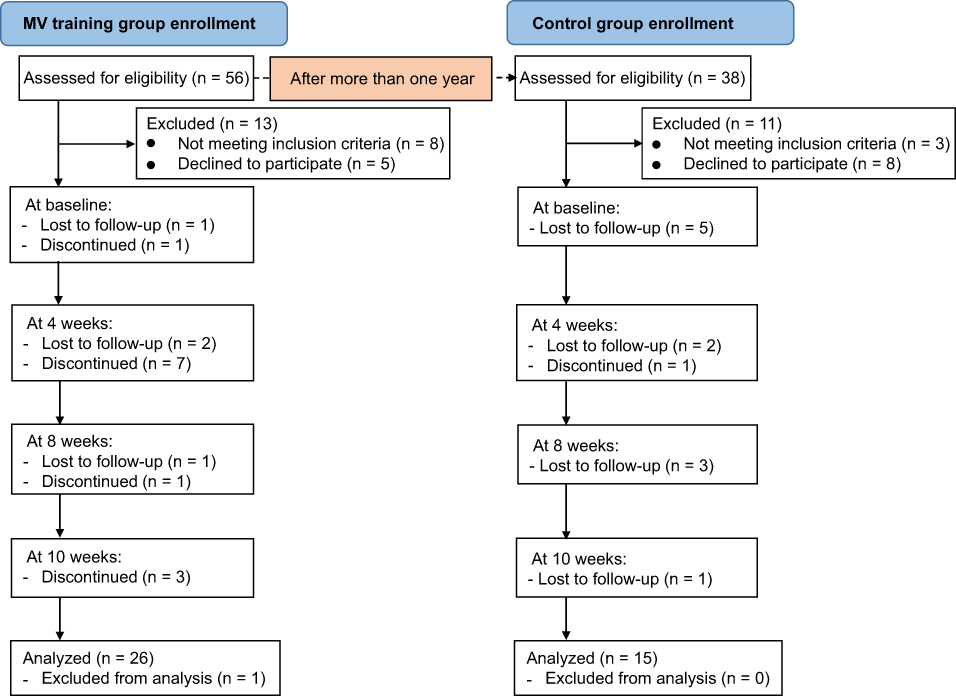 | Figure 2 Flow diagram of subjects through the study. |
Participants’ baseline characteristics are presented in Table 1. No significant difference was found in the characteristics between the two groups. Moreover, the correlation between gait ability and movement velocity is shown in Table 2. A significant correlation was found between gait ability and movement velocity, and the upper and lower limbs of movement velocity.
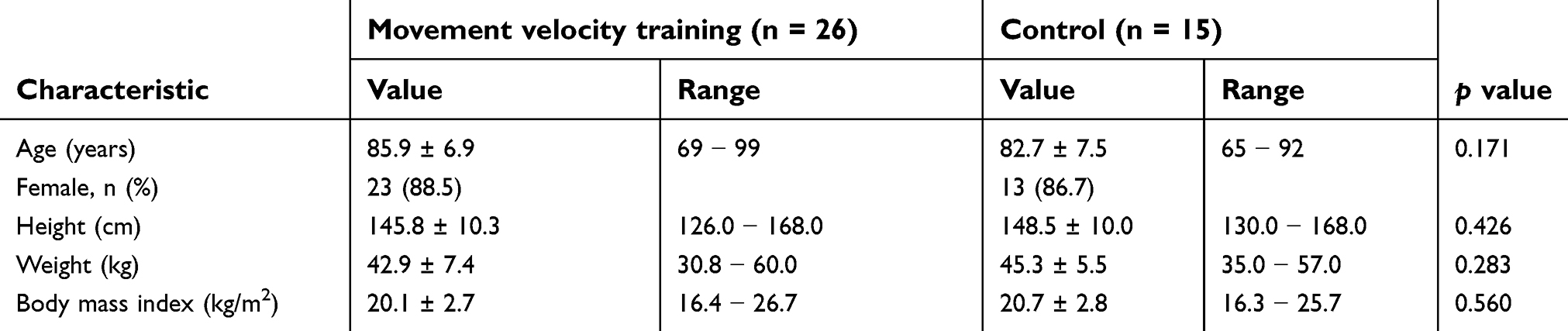 | Table 1. Characteristics of the study population |
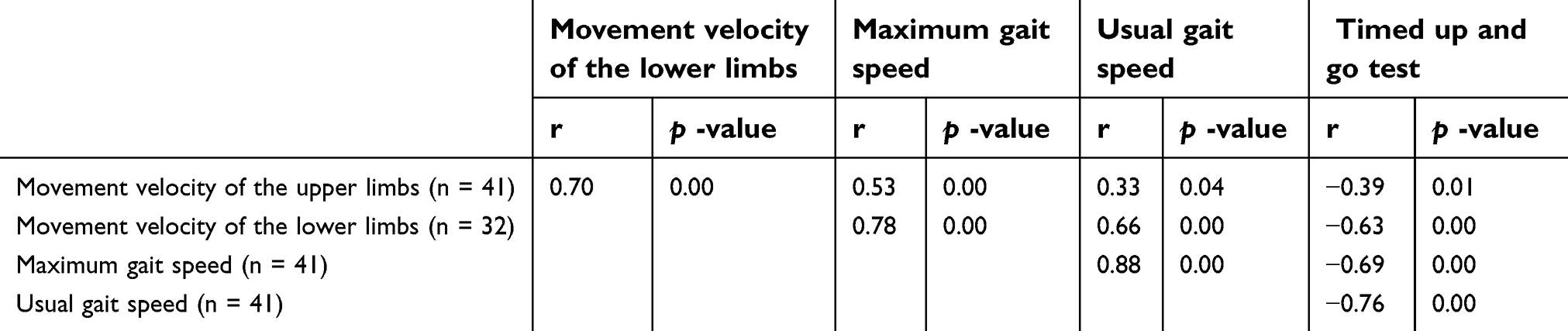 | Table 2. Correlation of gait ability and movement velocity of the upper and lower limbs |
Gait ability
To control for baseline differences, repeated-measures ANCOVA was adjusted for baseline values. A significant time–group interaction was found (p=0.001, partial η2=0.172) for maximum gait speed (Table 3). Bonferroni post-hoc test showed a significant increase in gait speed between pre-intervention and 10 weeks after intervention in the movement velocity training group. No significant time–group interaction was found for usual gait speed and TUG (p=0.076, p=0.563).
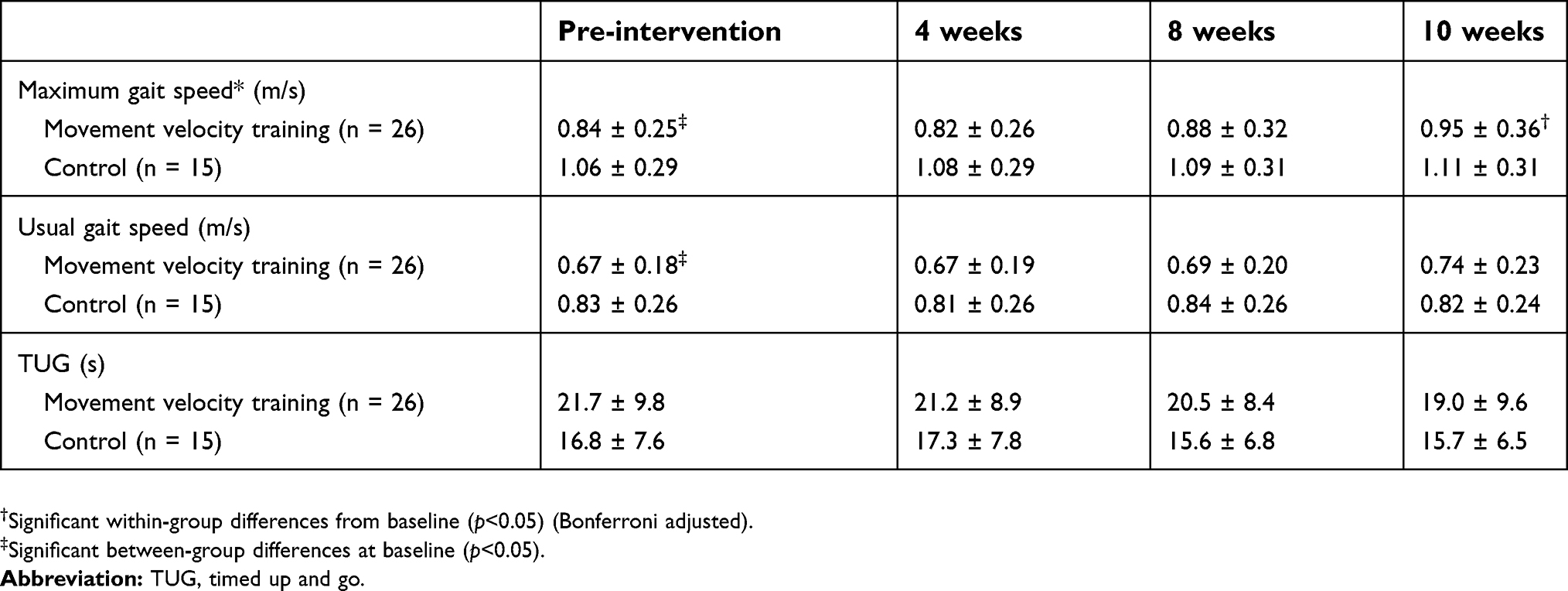 | Table 3. Descriptive statistics and group comparisons of gait ability |
Movement velocity and muscle strength
To control for baseline differences, repeated-measures ANCOVA was adjusted for baseline values. A significant time–group interaction was observed (p=0.02, partial η2=0.126) for movement velocity of the upper limbs (Table 4). Bonferroni post-hoc test showed a significant increase in movement velocity of the upper limbs between pre-intervention and 4 weeks (p=0.018), 8 weeks (p=0.001), and 10 weeks (p=0.000) after intervention in the movement velocity training group. No significant time–group interaction was found for movement velocity of the lower limbs and quadriceps strength (p=0.772, p=0.629).
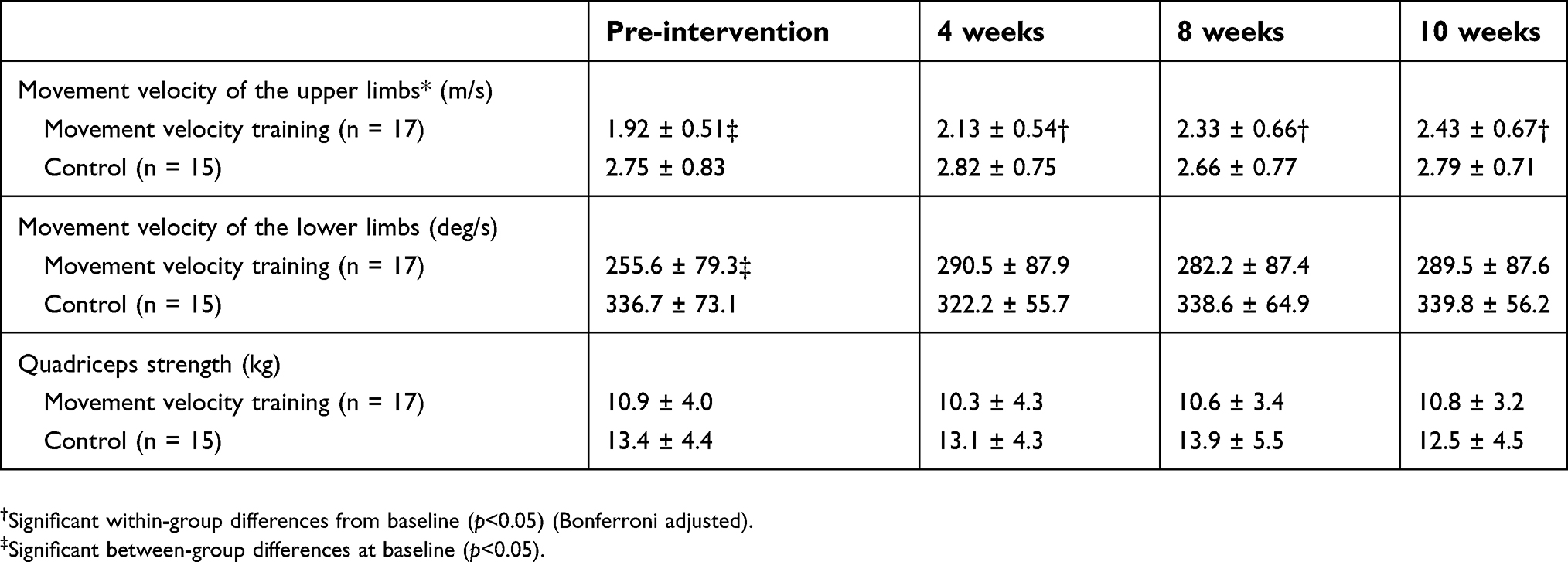 | Table 4. Descriptive statistics and group comparisons of movement velocity and muscle strength |
Discussion
The purpose of this study was to assess the beneficial effects of movement velocity training of the upper limbs on gait ability in older adults in geriatric health service facilities. The movement velocity training of the upper limbs showed a significant improvement in maximum gait speed. In addition, the difference in maximum gait speed between preintervention and 10 weeks after intervention was 0.11 m/s. The clinically significant difference in gait speed is generally accepted at 0.1 m/s or more.22,23 Therefore, this study suggests that movement velocity training of the upper limbs is an effective intervention to improve mobility in older adults.
There are two possible reasons why gait speed improved significantly in the training group compared with that in the control group. First, gait speed improvement may be due to a change in arm swing during gait. Elftman reported that arm swing motion helps stabilize rotational body motion during gait.24 Furthermore, a previous study indicates that arm swing during gait may facilitate lower limb muscle activation via neural coupling.25 Arm swing training also significantly improves the gait speed of stroke patients compared with that of the control group.26 In addition, a previous study also reported that an increase in arm swing speed positively changes the gait parameter, particularly gait speed.27 The movement velocity of the upper limbs was significantly improved by the movement velocity training of the upper limbs, leading to an improvement in gait speed.
Second, trunk muscle strength may be improved by training. Trunk muscle strength contributes to stability during gait,28 and trunk muscle strength training was reported to be effective at improving gait speed in community-dwelling older adults.29 The muscle activation required for the development of muscle strength of the back and abdominal can be achieved during maximum contraction of shoulder extension and horizontal extension muscles.30 Trunk flexion muscles are more active when moving the upper limbs as fast as possible compared with when moving slowly.31 Based on these previous findings, the movement of shoulder joint extension and horizontal extension as fast as possible may be sufficient to improve trunk muscle strength.
Movement velocity training of the upper limbs has factors of both motion direction (extension and horizontal extension of the shoulder joint) and high velocity. Therefore, we supposed that trunk function was improved by training, which led to improvement in gait speed.
Maximum gait speed showed a significant improvement in the training group, but usual gait speed had no significant improvement. Arai et al9 reported that maximum gait speed, but not usual gait speed, is significantly correlated with knee extension movement velocity. Sayers et al32 reported that maximum gait speed improves significantly by movement velocity training. However, they did not find a difference in the change of usual gait speed.32 Movement velocity is a more important factor for maximum gait speed compared with usual gait speed, and the effect of movement velocity training influences only maximum gait speed. Therefore, only maximum gait speed improved in this study.
This study has several limitations. First, the first limitation was the absence of randomization. The number of participants was quite small, and the participants were difficult to divide into two groups at the same time in the same facility. Second, the maximum and usual gait speeds before the intervention of the training group were significantly slower than those of the control group. The difference in trainability between the training and control groups may have influenced the results. Third, the majority of participants were female (male to female ratio was 1:9). Previous studies reported that the characteristics of movement velocity differ depending on gender.33 The effect of gait ability improvement may differ between men and women even in movement velocity training. Finally, we could not elucidate the mechanism by which maximum gait speed was improved by movement velocity training of the upper limbs. Further research is required to investigate factors that increased gait speed.
Conclusion
Movement velocity training of the upper limbs showed significant and clinically relevant improvements in maximum gait speed. The gait function is important not only for healthy older adults,34 but also for older adults with poor physical function, such as the patients who have stroke35 or orthopedic disease.36 Moreover, gait function affects the prognosis more than the cardiac function in older adults with chronic heart failure.37 The movement velocity training of upper limbs is low-load training in a seated position. Therefore, this training is a useful intervention and can be safely performed in a wide range of participants.
Acknowledgment
We thank Mr. Ikushima, Ms. Noguchi, Mr. Kano, Mr. Hamasaki, Mr. Higeno, and Ms. Sakamoto for their help with recruitment of participants for this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Abellan van Kan G, Rolland Y, Andrieu S, et al. Gait speed at usual pace as a predictor of adverse outcomes in community-dwelling older people an International Academy on Nutrition and Aging (IANA) Task Force. J Nutr Health Aging. 2009;13(10):881–889. doi:10.1007/s12603-009-0246-z
2. Montero-Odasso M, Schapira M, Soriano ER, et al. Gait velocity as a single predictor of adverse events in healthy seniors aged 75 years and older. J Gerontol A Biol Sci Med Sci. 2005;60(10):1304–1309. doi:10.1093/gerona/60.10.1304
3. Guralnik JM, Ferrucci L, Simonsick EM, Salive ME, Wallace RB. Lower-extremity function in persons over the age of 70 years as a predictor of subsequent disability. N Engl J Med. 1995;332:556–561. doi:10.1056/NEJM199503023320902
4. Studenski S, Perera S, Patel K, et al. Gait speed and survival in older adults. J Am Med Assoc. 2011;305(1):50–58. doi:10.1001/jama.2010.1923
5. Steffen TM, Hacker TA, Mollinger L. Age- and gender-related test performance in community-dwelling elderly people: six-minute walk test, Berg balance scale, timed up & go test, and gait speeds. Phys Ther. 2002;82(2):128–137. doi:10.1093/ptj/82.2.128
6. Fragala MS, Clark MH, Walsh SJ, et al. Gender differences in anthropometric predictors of physical performance in older adults. Gend Med. 2012;9(6):445–456. doi:10.1016/j.genm.2012.10.004
7. Buchner DM, Larson EB, Wagner EH, Koepsell TD, de Lateur BJ. Evidence for a non-linear relationship between leg strength and gait speed. Age Ageing. 1996;25(5):386–391. doi:10.1093/ageing/25.5.386
8. Bean JF, Kiely DK, Herman S, et al. The relationship between leg power and physical performance in mobility-limited older people. J Am Geriatr Soc. 2002;50(3):461–467. doi:10.1046/j.1532-5415.2002.50111.x
9. Arai T, Obuchi S, Shiba Y, Omuro K, Inaba Y, Kojima M. The validity of an assessment of maximum angular velocity of knee extension (KE) using a gyroscope. Arch Gerontol Geriatr. 2012;54(2):e175–e180. doi:10.1016/j.archger.2011.10.012
10. Arai T, Obuchi S, Shiba Y, Omuro K, Nakano C, Higashi T. The feasibility of measuring joint angular velocity with a gyro-sensor. Arch Phys Med Rehabil. 2008;89(1):95–99. doi:10.1016/j.apmr.2007.07.051
11. Iwata A, Higuchi Y, Kimura D, et al. Quick lateral movements of the trunk in a seated position reflect mobility and activities of daily living (ADL) function in frail elderly individuals. Arch Gerontol Geriatr. 2013;56(3):482–486. doi:10.1016/j.archger.2012.12.002
12. Iwata A, Higuchi Y, Sano Y, et al. Maximum movement velocity of the upper limbs reflects maximum gait speed in community-dwelling adults aged older than 60 years. Geriatr Gerontol Int. 2014;14(4):886–891. doi:10.1111/ggi.12186
13. Henwood TR, Riek S, Taaffe DR. Strength versus muscle power-specific resistance training in community-dwelling older adults. J Gerontol A Biol Sci Med Sci. 2008;63(1):83–91. doi:10.1093/gerona/63.1.83
14. Glenn JM, Gray M, Binns A. The effects of loaded and unloaded high-velocity resistance training on functional fitness among community-dwelling older adults. Age Ageing. 2015;44(6):926–931. doi:10.1093/ageing/afv081
15. Macaluso A, Young A, Gibb KS, Rowe DA, De Vito G. Cycling as a novel approach to resistance training increases muscle strength, power, and selected functional abilities in healthy older women. J Appl Physiol. 2003;95(6):2544–2553. doi:10.1152/japplphysiol.00416.2003
16. Sano Y, Iwata A, Wanaka H, et al. An easy and safe training method for trunk function improves mobility in total knee arthroplasty patients: a quasi-randomized controlled trial. PLoS One. 2018;13(10):e0204884. doi:10.1371/journal.pone.0204884
17. Iwata A, Higuchi Y, Ogaya S, et al. Characteristics of movement velocities of upper and lower limbs and trunk in older adults. Int J Phys Med Rehabil. in press.
18. Podsiadlo D, Richardson S. The timed “Up & go”: a test of basic functional mobility for frail elderly persons. J Am Geriatr Soc. 1991;39(2):142–148. doi:10.1111/j.1532-5415.1991.tb01616.x
19. Guralnik JM, Simonsick EM, Ferrucci L, et al. A short physical performance battery assessing lower extremity function: association with self-reported disability and prediction of mortality and nursing home admission. J Gerontol. 1994;49(2):M85–M94. doi:10.1093/geronj/49.2.M85
20. Takazawa K, Arisawa K, Honda S, Shibata Y, Saito H. Lower-extremity muscle forces measured by a hand-held dynamometer and the risk of falls among day-care users in Japan: using multinomial logistic regression analysis. Disabil Rehabil. 2003;25(8):399–404. doi:10.1080/0963828031000090416
21. ALMohiza MA, Sparto PJ, Marchetti GF, et al. A quality improvement project in balance and vestibular rehabilitation and its effect on clinical outcomes. J Neurol Phys Ther. 2016;40(2):90–99. doi:10.1097/NPT.0000000000000125
22. Perera S, Studenski S, Newman A, et al. Are estimates of meaningful decline in mobility performance consistent among clinically important subgroups? (Health ABC study). J Gerontol A Biol Sci Med Sci. 2014;69(10):1260–1268. doi:10.1093/gerona/glu033
23. Perera S, Mody SH, Woodman RC, Studenski SA. Meaningful change and responsiveness in common physical performance measures in older adults. J Am Geriatr Soc. 2006;54(5):743–749. doi:10.1111/j.1532-5415.2006.00701.x
24. Elftman H. The function of the arms in walking. Hum Biol. 1939;11(4):529–535.
25. Ferris DP, Huang HJ, Kao PC. Moving the arms to activate the legs. Exerc Sport Sci Rev. 2006;34(3):113–120. doi:10.1249/00003677-200607000-00005
26. Shin JH, Kim CB, Choi JD. Effects of trunk rotation induced treadmill gait training on gait of stroke patients: a randomized controlled trial. J Phys Ther Sci. 2015;27(4):1215–1217. doi:10.1589/jpts.27.1215
27. Zampier VC, Vitório R, Beretta VS, et al. Gait bradykinesia and hypometria decrease as arm swing frequency and amplitude increase. Neurosci Lett. 2018;687:248–252. doi:10.1016/j.neulet.2018.09.051
28. Helbostad JL, Moe-Nilssen R. The effect of gait speed on lateral balance control during walking in healthy elderly. Gait Posture. 2003;18(2):27–36. doi:10.1016/S0966-6362(02)00197-2
29. Granacher U, Lacroix A, Muehlbauer T, Roettger K, Gollhofer A. Effects of core instability strength training on trunk muscle strength, spinal mobility, dynamic balance and functional mobility in older adults. Gerontology. 2013;59(2):105–113. doi:10.1159/000343152
30. Tarnanen SP, Ylinen JJ, Siekkinen KM, Mälkiä EA, Kautiainen HJ, Häkkinen AH. Effect of isometric upper-extremity exercises on the activation of core stabilizing muscles. Arch Phys Med Rehabil. 2008;89(3):513–521. doi:10.1016/j.apmr.2007.08.160
31. Hodges PW, Richardson CA. Altered trunk muscle recruitment in people with low back pain with upper limb movement at different speeds. Arch Phys Med Rehabil. 1999;80(9):1005–1012. doi:10.1016/S0003-9993(99)90052-7
32. Sayers SP, Gibson K, Bryan Mann J. Improvement in functional performance with high-speed power training in older adults is optimized in those with the highest training velocity. Eur J Appl Physiol. 2016;116(11–12):2327–2336. doi:10.1007/s00421-016-3484-x
33. Sayers SP, Guralnik JM, Thombs LA, Fielding RA. Effect of leg muscle contraction velocity on functional performance in older men and women. J Am Geriatr Soc. 2005;53(3):467–471. doi:10.1111/j.1532-5415.2005.53166.x
34. Kang HG, Dingwell JB. Effects of walking speed, strength and range of motion on gait stability in healthy older adults. J Biomech. 2008;41(14):2899–2905. doi:10.1016/j.jbiomech.2008.08.002
35. Fulk GD, Ludwing M, Dunning K, Golden S, Boyne P, West T. Estimating clinically important change in gait speed in people with stroke undergoing outpatient rehabilitation. J Neurol Phys Ther. 2011;35(2):82–89. doi:10.1097/NPT.0b013e318218e2f2
36. Kiss RM, Bejek Z, Szendroi M. Variability of gait parameters in patients with total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc. 2012;20(7):1252–1260. doi:10.1007/s00167-012-1965-y
37. Cacciatore F, Abete P, Mazzella F, et al. Six-minute walking test but not ejection fraction predicts mortality in elderly patients undergoing cardiac rehabilitation following coronary artery bypass grafting. Eur J Prev Xardiol. 2012;19(6):1401–1409. doi:10.1177/1741826711422991
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.