")
Back to Journals » Journal of Blood Medicine » Volume 11
Platelet Transfusion: And Update on Challenges and Outcomes
Authors Solves Alcaina P
Received 11 October 2019
Accepted for publication 31 December 2019
Published 24 January 2020 Volume 2020:11 Pages 19—26
DOI https://doi.org/10.2147/JBM.S234374
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Martin H Bluth
Pilar Solves Alcaina
Blood Bank, Hematology Service, Hospital Universitari I Politècnic La Fe, Valencia, CIBERONC, Instituto Carlos III, Madrid, Spain
Correspondence: Pilar Solves Alcaina
Blood Bank, Hematology Service, Hospital Universitari I Politècnic La Fe, Avda Abril Martorell, 106, Valencia 46026, Spain
Email [email protected]
Abstract: Platelet transfusion is a common practice in onco-hematologic patients for preventing or treating hemorrhages. Platelet concentrates can be transfused with therapeutic or prophylactic purposes. With the aim to help clinicians to take the decisions on platelet transfusion, some guidelines have been developed based on the current scientific evidence. However, there are some controversial issues and available scientific evidence is not enough to solve them. There is little information about what is the best platelet product to be transfused: random platelets or single donor apheresis platelets, and plasma-suspended or additive solution suspended platelets. Platelets are often transfused without respecting the ABO compatibility, but influence of this practice on platelet transfusion outcome is not well established. In the prophylactic platelet transfusion set there are some questions unsolved as the platelet threshold to transfuse prior to specific procedures or surgery, and even if platelet transfusion is necessary for some specific procedures as autologous hematopoietic stem cell transplantation. A challenging complication raised from multiple platelet transfusions is the platelet transfusion refractoriness. The study and management of this complication is often disappointing. In summary, although it is a widespread practice, platelet transfusion has still many controversial and unknown issues. The objective of this article is to review the current evidence on platelet transfusion practices, focusing on the controversial issues and challenges.
Keywords: platelet transfusion, prophylactic transfusion, platelet transfusion refractoriness
Introduction
Platelet transfusion is a common practice in thrombocytopenic patients for preventing or treating hemorrhages. About 230,000 platelet component transfusions are given in Spain, and approximately two million of platelet components are transfused in the United States annually.1–3 More than 50% of platelets are transfused to patients diagnosed of onco-hematological diseases and/or undergoing hematopoietic stem cell transplantation. With the aim to help physicians to take the most accurate decisions on platelet transfusion, some guidelines have been developed based on the current-scientific evidence.4–12 However, there are some controversial issues and available scientific evidence is still not enough to solve them. There is little information about which is the best platelet product to be transfused: random platelets or single donor apheresis platelets, and plasma-suspended or additive solution-suspended platelets. Platelets are often transfused without respecting the ABO compatibility due to the limited stock availability, but influence of this practice on platelet transfusion outcome is not well established. In the prophylactic platelet transfusion setting, there are some questions unsolved as the platelet threshold to transfuse prior to specific procedures or surgery, and even if platelet transfusion is necessary for some specific procedures as autologous hematopoietic stem cell transplantation. A challenging complication raised from multiple platelet transfusions is the platelet transfusion refractoriness (PTR). The study and management of this complication is often disappointing.13 In summary, despite being a widely practice, platelet transfusion has still many controversial and unknown issues.
The objective of this article is to review the current evidence on platelet transfusion practices in adult patients, focusing on the controversial issues and challenges.
What Is the Best Platelet Product to Be Transfused: Random-Donor Platelets or Single-Donor Apheresis Platelets?
Platelet concentrates can be obtained either from single donor apheresis (SDAP) or pooled from 4 to 6 units of random donor whole blood (RDP), and both are considered as standard dose. There is a debate persisting over time on which platelet product has more benefits for patients and therefore should be used. RDP are considered the standard of care in many centers of Europe, while in the USA up two-thirds to three-quarters of all transfusions given are SDAP.1,14–16 RDP are obtained from whole-blood collection by the buffy coat method (used commonly in Europe) or from platelet rich plasma (used commonly in the USA). Both RDP and SDAP can be suspended in plasma or in special platelet additive solutions (PAS).17 The use of PAS reduces the plasma content of platelets to 20% and the expected benefit for patients is the reduction of adverse reactions related to plasma.16 Among the benefits of transfusing SDAP platelets are decreasing donor exposure and the reduction in septic/infectious and non-infectious platelet transfusion reactions.14,18 In fact, the RDP units are associated with a 5–6 fold higher risk of bacterial contamination and a two-fold higher risk of transfusion transmitted infection (TTI) compared to SDAP.19,20 The current risk of TTI is very low in our area, having been confirmed in the last 15 years a reduction in the donor incidence rate and in the residual risk for the case of HBV.21 However, emerging TTI could cause an epidemic situation similar to HIV virus infection and therefore use of RDP represents a higher infectious potential risk. The reduction of febrile transfusion reactions is also a benefit of using SDAP over RDP,14 however with the implementation of universal leukoreduction this advantage has been significantly reduced. Trial to Reduce Alloimmunization to Platelets Study Group (TRAP) showed no significant advantage of SDAP over RDP for the prevention of alloimmunization, being leukodepletion a useful method to prevent it.22 In the TRAP study, patients diagnosed of acute leukemia receiving induction chemotherapy (n=530) and without platelet alloantibodies were randomly assigned to be transfused with one of four types of platelet products: pooled platelet concentrates from random donors (control group); filtered, pooled platelet concentrates from random donors (F-PC); ultraviolet B-irradiated, pooled platelet concentrates from random donors (UVB-PC); or filtered platelets obtained by apheresis from single random donors (F-AP). Up to 13% of patients in the control group developed lymphocytotoxic antibodies as compared to 3%, 5% and 4% in the F-PC, UVB-PC and F-AP, respectively (p< or =0.03).22 Filtered SDAP did not provide additional benefit as compared to filtered RDP to prevent alloantibody mediated platelet refractoriness.
Currently, blood products are leukoreduced at the time of preparation in Spain and other European countries as well as in the USA.16
High platelet yield have also seen in SDAP as compared to PRD, and also post-transfusion platelet increments have been confirmed to be higher in patients receiving SDAP transfusions.14,23–25 However, in patients undergoing hematopoietic stem cell transplantation or chemotherapy, Slichter et al23 found that at doses between 1.1 x 1011 and 4.4 x 1011 platelets per square meter, the number of platelets in the prophylactic transfusion had no effect on the incidence of bleeding. This study23 randomly assigned 1272 hospitalized patients undergoing hematopoietic stem cell transplantation or chemotherapy to receive prophylactic platelet transfusions at doses of 1.1 x 1011/m2 (low dose), 2.2 x 1011/m2 (medium dose), or 4.4 x 1011/m2 (high dose), when platelet counts were ≤10,000/mm3. The primary end point was WHO bleeding of grade 2 or higher. Up to 71%, 69%, and 70% of the patients in the low-dose group, the medium-dose group, and the high-dose group, suffered a bleeding episode of grade 2 or higher, respectively (p=ns).23 Then, one can conclude that higher yields of SDAP do not necessarily imply a clear clinical benefit.
Other authors found that due to improvement and standardization of production methods with time, both platelet products SDAP and RDP have become comparable in platelet yields and quality.4,26 Another advantage of SDAP which is generally underestimated, is the low red blood cell contamination that contributes to decrease the risk of alloimmunization when transfusing RhD-positive platelets to RhD-negative patients.1,27 Red blood cell content is approximately of 0.036 mL for RDP and 0.00043 mL for SDAP.12 In none of the published studies in which RhD-negative patients were transfused only with RhD-positive platelets from single-donor apheresis, anti-D alloimmunization was detected.28–30 This issue must be considered in RhD-negative childbearing women receiving RhD-positive platelet transfusions, when RhD-negative platelets are not available.31
The set of advantages explained above have led to some authors to conclude that transfusing SDAP improves patient care,13 but to date no studies have shown clear benefits of SDAP over RDP in terms of decreasing severe bleeding and improving outcome, and both platelet products are considered equivalent.4,12 The main and consistent argument in favor of use of PRD is the better use of resources and the lower costs as compared to SDAP, this has to be taken into account especially in those countries with public health services as Spain. An important and unsolved question is whether SDAP have enough clinical benefits to justify the higher production costs. Currently, SDAP should be especially used for pediatric population and patients with immune platelet refractoriness.12
What Is the Current Risk of the ABO Incompatible Platelet Transfusions?
Platelets are a valuable resource whose availability is not always guaranteed by transfusion centers.1 It has been demonstrated the presence of ABO antigens on platelet surface,32,33 but needs for ABO compatibility in platelet transfusions remains a controversial issue of ongoing debate.34 A survey of a high number of North American laboratories showed that 17% of transfusion services did not have a clear policy regarding the use of ABO-incompatible platelets.33 Most current guidelines do not address this aspect.7,8,12 Only British11 guidelines recommend that hospitals should have a strategy to maximise the transfusion of ABO compatible platelets.
Although transfusion policy varies between centres, platelets transfusion is usually made in part across the ABO barrier. This strategy has some clear advantages as better availability and better response in emergency situations, avoiding platelets wastage. On the contrary, some studies have demonstrated higher post-transfusion platelets increments after ABO identical platelet transfusion, supporting this practice.35 A systematic review of literature in which 1502 patients from three randomized controlled trials and sixteen observational studies were included, showed the largest difference in increment between ABO-identical and ABO non-identical PLT transfusion was 4 x 109/L. Survival and assessment of haemorrhage was considered inadequate.35 Therefore, the clinical significance of the greater post-transfusion platelets increment has not been clarified.36
Transfusion of ABO-minor incompatible platelets has been associated to some reports to acute haemolytic transfusion reactions due to the exposure of recipient to ABO-incompatible plasma containing anti-A or anti-B isoagglutinins.37 In order to prevent this and other adverse effects, many transfusion centres suspend platelets in additive solutions that significantly reduced the quantity of plasma and the risk of hemolysis.17 British11 and Italian4 transfusion guides establish that if incompatible group O platelets are used for patients with group A, B or AB they must be re-suspended in PAS or had low anti-A/B titers.
Despite these considerations, the relevance of ABO match in platelet transfusions is not clearly determined. Our group analysed 529-consecutive patients who underwent 553-autologous progenitor stem cell transplants at our hospital between January 2000 and December 2013. The patients received a total of 2,772 pooled platelet concentrates, of which 2,053 (74.0%) were ABO identical and 719 (26.0%) ABO non-identical; of these latter, 309 were compatible and 410 incompatible with the patients’ plasma, respectively. Platelet and red blood cell transfusion requirements and patient outcome were similar for patients who received ABO identical and ABO non-identical platelets.38 No hemolytic reaction was detected in any case. Patients received RDP from 4 whole-blood donations suspended in PAS.
What Is the Best Platelet Transfusion Strategy: Prophylactic or Therapeutic?
Thrombocytopenic patients are at high risk of suffering clinical bleeding, especially those with platelet counts ≤5000/µL.23 Platelet transfusion can be used with therapeutic and/or prophylactic approach. Therapeutic platelet transfusions are used to treat acute haemorrhage, while prophylactic platelet transfusions are used to prevent haemorrhage in patients with treatment-induced thrombocytopenia and/or platelet dysfunctions, before invasive procedures and surgery. Patients diagnosed of hematological malignancies undergoing chemotherapy or hematopoietic stem cell transplantation have often long period of thrombocytopenia and high platelet transfusion requirements, so are the population in which more studies are available evaluating prophylactic versus therapeutic platelet transfusion strategy. The current evidence from various randomized clinical trials and meta-analyses support the prophylactic strategy for patients with hematological malignancies receiving chemotherapy and allogeneic hematopoietic stem cell transplantation.16,39–47 Transfusing platelets in these patients decreases in a significant manner the WHO grade 2 or greater bleeding complications. Stanworth et al39 conducted a randomized trial that included 600 patients receiving chemotherapy or undergoing HSCT. Patients were randomized to receive (n=299) or not to receive (n=301) prophylactic platelets when platelet counts were <10,000/µL. WHO grade bleeding 2, 3 or 4 occurred in 43% and 50% of prophylaxis group and no prophylaxis group, respectively (p=0.06).39 The results of this trial support the benefit of prophylactic transfusion strategy for reducing bleeding as compared to non-prophylactic strategy.
There are different studies and Cochrane reviews focusing on the optimal doses and threshold for prophylactic platelet transfusions.23,24,45,46 The conclusions of these studies are in favor of transfusing lower dose of platelets. As commented above, in patients affected of hematological malignancies platelet transfusions of lower dose (1.1 x 1011/m2), standard dose (2.2 x 1011/m2), or higher-dose (4.4 x 1011/m2) have the same clinical benefits (bleeding events, days of bleeding, life-threatening bleedings) and similar mortality,23 while transfusion adverse events were higher in patients receiving higher doses of platelets.23,46 A randomized controlled trial47 evaluated 255 adolescents and adults (age, 16 to 70 years) with newly diagnosed acute myeloid leukemia (excluding acute promyelocytic leukemia), of which 135 were randomly assigned to receive a transfusion when their platelet count was <10,000 per cubic millimeter (group 1), and 120 patients were assigned to be transfused when their platelet count was <20,000 per cubic millimeter (group 2). Patients in the group 1 received 21.5 percent fewer platelet transfusions than the patients in the group 2 (p=0.001). Red blood cell transfusions, major bleeding episodes and days of hospitalization were similar for both groups. In summary, prophylactic transfusion strategy using low-dose platelets (threshold of 10 x 109/L) is the current recommendation for hematological patients undergoing chemotherapy or allogeneic stem cell transplantation. This threshold should be increased to 20 x 109/L if there are some additional-risk factors for bleeding.4,8,11,12 Current guidelines also recommend different thresholds for prophylactic platelet transfusion before surgery or invasive procedures.4,7,8,11,12
On the other hand, the benefit of prophylactic platelet transfusions has not been confirmed in the autologous stem cell transplantation setting.39,40 In this subset of patients, therapeutic strategy is not superior to therapeutic strategy. There is lack of evidence to recommend or not prophylactic strategy in patients with bone marrow failure and chronic thrombocytopenia where recovery is not anticipated, and without active treatment.44
Which are the Recommended Thresholds for Prophylactic Platelet Transfusion Before Invasive Procedures and Surgery?
There is quite a variability in platelet threshold recommendations for invasive procedures and surgery according to different current guidelines.7–21 This is probably due to the lack of scientific evidence available with guidelines, mainly based on expert opinions. The degree of thrombocytopenia is not the only factor associated with bleeding, other factors as hematocrit, coagulation factors and drugs also contribute to the risk of bleeding.48 These factors are not always considered in available platelet transfusion recommendations. All the guidelines recommend the threshold of equal or less than 10 x 109/L platelets for prophylactic transfusion in patients affected by hematological malignancies and allogeneic hematopoietic stem cell transplantation. This is the only point in which all the guides agree. Spanish,8 Italian4 and British11 guidelines specify thresholds for a higher number of procedures than AABB and ASCO guidelines, that recommend thresholds only for a few procedures each one. In Table 1 there is a summary of thresholds published in different guidelines. Only the Spanish guide8 recommends the threshold of 5 x 109/L for patients with chronic thrombocytopenia from central origin without active treatment while BSH11 and ASCO12 guidelines recommend a non-prophylactic platelet transfusion strategy for these patients. A trigger of 100 x 109/L is often used for patients in need of neurosurgery or ophthalmological bleeding.14,49 In general, there are no recommendations for or against platelet transfusion in patients receiving antiplatelet therapy and severe bleeding,4,7,12 while British guidelines suggest considering platelet transfusion as an additional measure to control severe bleeding.11 All the recommendations showed in the table have been developed by scientific societies related to hematology and oncology, but other medical specialties have their own guidelines and recommend different thresholds. A Society of Interventional Radiology recommends 50 x 109/L platelets to place a central venous line,50 while anesthesiologists suggest a count of 75 x 109/L for neuraxial blockade.51
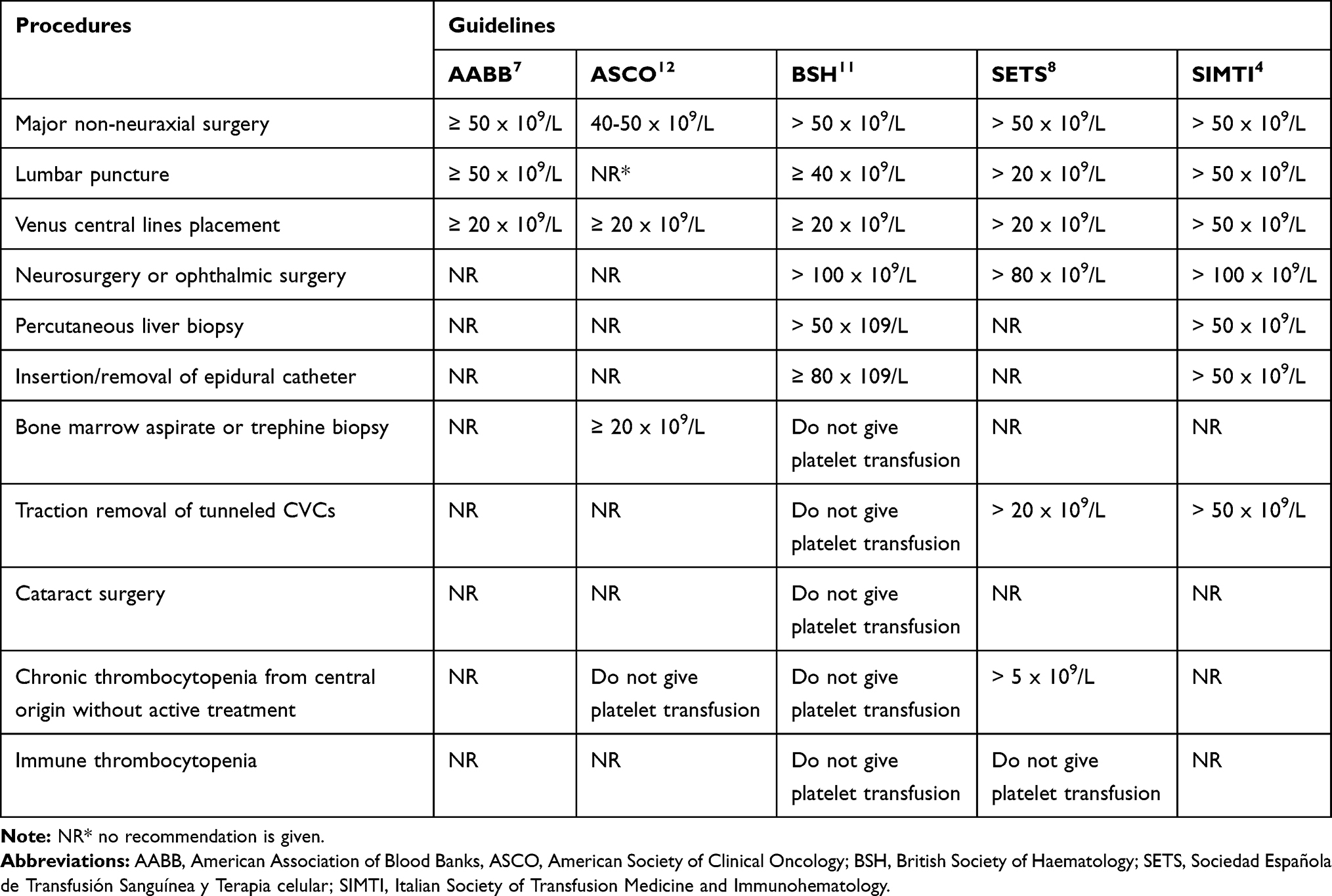 |
Table 1 Prophylactic Platelet Transfusion: Comparative Thresholds for Invasive Procedures and Surgery According to Different Guidelines |
The thresholds for treatment of active bleedings are more homogeneous: in severe bleeding the recommended threshold is mostly 50 x 109/L, and 100 x 109/L for patients with multiple trauma or brain injury.4,8,11 There is little evidence about the effectiveness of alternative treatments to platelet transfusions.52 BSH guidelines recommend considering administration of tranexamic acid in trauma patients with severe bleeding and also in patients with chronic thrombocytopenia due to bone marrow failure in addition to platelet transfusion therapy.11
Is the Platelet Transfusion Refractoriness Properly Diagnosed and Treated?
A challenging complication raised from multiple platelet transfusions is the platelet transfusion refractoriness (PTR) that leads to increased rates of morbidity and mortality.53 PTR is defined as the lack of adequate post-transfusion platelet count increment. One therapeutic unit of platelets should increase the platelet count by 35,000/µL to 40,000/µL as measured within 10 mins and 1 hr following the transfusion. Either post-transfusion platelet increment (PPI) < 10 x 109/L or corrected count increment (CCI) at 10–60 mins <5–10 x 109/L on two occasions after transfusion of ABO compatible platelets stored for less than 72 h, are used to diagnose PTR.13,54 Although a 10-min to 1-h determination is necessary to define platelet refractoriness, it is not usually until the following day control when suspicion may be aroused due to an inappropriate-low platelet count. A 20-h CCI determination shows a good correlation with the 1-h CCI.55 Despite the clinical relevance, PTR is often underdiagnosed even in hematologic patients because of the complexity of the process and the need for collaboration between professionals in different areas. There are only few studies analyzing the incidence of PTR in hematological patients, in patients undergoing hematopoietic stem cell transplantation PTR rate can be as high as near 60% of transfusions.56–58
Etiology of PTR is often multifactorial and can be classified as immune and non-immune causes. Non-immune causes involve near 80% of PTR episodes, being the most frequently reported infection/sepsis, fever, disseminated intravascular coagulation, splenomegaly, graft versus host disease, and antibiotics.54 Development of antibodies against human leukocyte antigens (HLA) or less frequently against human platelet specific antigens (HPA) still represent approximately one-third of refractory episodes, even though the efforts made in the last decades for preventing alloimmunization.13,59 Immune refractoriness is quite well characterized and has some possibilities for treatment, as HLA-matched platelets, cross-matched platelets and antibody specificity prediction.60,61 However, these therapeutic approaches are not always successful. Rioux-Masse et al62 found that only 25% of cross-matched platelet transfusions and 29% of HLA-matched platelets achieved a CCI of more than 5 x 109/L. Therefore, refractoriness is a complex, multifactorial problem, and the mere presence of anti-HLA and/or anti-platelet antigens do not exclude other causes. And not only the presence, but also the titers of anti-HLA antibodies must be taken into account to select adequate platelets for treatment. If HLA-matched platelets are not available, platelet transfusion must be avoided in absence of hemorrhagic events.12 Other approaches as Rituximab, activated factor and platelet continuous infusion have been used to treat severe platelet refractoriness and active bleeding in hematological patients.11,63–65
Treatment for non-immune platelet refractoriness, which is the most frequent cause, is often ineffective and is a complicated challenge. Guidelines4,11 recommend transfusing fresh and ABO compatible platelets in this subset of patients. This approach, however, is often unsuccessful.
Conclusions
Platelet transfusion is a widespread practice that is not always supported by scientific evidence. Available guidelines recommend different prophylactic platelet transfusion thresholds for the same procedures, complicating the physician decision-making. Diagnosing and treating immune and non-immune platelet transfusion refractoriness is a difficult challenge that has an impact on patient outcome. Well-designed prospective randomized trials are needed to provide scientific evidence to support the clinical practice.
Disclosure
The author reports no conflicts of interest in this work.
References
1. Heal JM, Blumberg N. Optimizing platelet transfusion therapy. Blood Rev. 2004;18:149–165. doi:10.1016/S0268-960X(03)00057-2
2. Informe hemovigilancia; 2017. Available from: https://www.mscbs.gob.es/profesionales/saludPublica/medicinaTransfusional/hemovigilancia/docs/Informe2017.pdf. Accessed January 15, 2020.
3. Ellingson KD, Sapianzo MRP, Haass KA, et al. Continue decline in blood collection and transfusion in the United States-2015. Transfusion. 2017;27:1588–1598. doi:10.1111/trf.14165
4. Liumbruno G, Bennardello F, Lattanzio A, Piccoli P, Rossetti G; Italian Society of Transfusion Medicine and Immunohaematology (SIMTI) Work Group. Recommendations for the transfusion of plasma and platelets. Blood Transfus. 2009;7(2):132–150. doi:10.2450/2009.0005-09
5. McCullough J. Overview of platelet transfusion. Semin Hematol. 2010;47(3):235–242. doi:10.1053/j.seminhematol.2010.04.001
6. Cid J, Harm SK, Yazer MH. Platelet transfusion: the art and science of compromise. Transfus Med Hemother. 2013;40:160–171. doi:10.1159/000351230
7. Kaufman RM, Djulbegovic B, Gernsheimer T, et al. Platelet transfusion: a clinical practice guideline from the AABB. Ann Intern Med. 2015;162:205–213. doi:10.7326/M14-1589
8. SETS. Guía sobre la transfusión de componentes sanguíneos y derivados plasmáticos. SETS, Ed, 5; 2015.
9. Nahirniak S, Slichter SJ, Tanael S, et al. Guidance on platelet transfusion for patients with hypoproliferative thrombocytopenia. Transfus Med Rev. 2015;29:3–13. doi:10.1016/j.tmrv.2014.11.004
10. Slichter SJ. Evidence-based platelet transfusion guidelines. Hematology. 2017;1:172–178. doi:10.1182/asheducation-2007.1.172
11. Scourt LJ, Birchall J, Allard S, et al. Guidelines for the use of platelet transfusions. Br J Haematol. 2017;176:365–394. doi:10.1111/bjh.14423
12. Schiffer CA, Bohlke K, Delaney M, et al. Platelet transfusion for patients with cancer: American Society of Clinical Oncology Clinical Practice Guideline Update. J Clin Oncol. 2018;36(3):283–299. doi:10.1200/JCO.2017.76.1734
13. Stanworth SJ, Navarrete C, Estcourt L, et al. Platelet refractoriness-practical approaches and ongoing dilemmas in patient management. Br J Haematol. 2015;171:297–305. doi:10.1111/bjh.13597
14. Ness PM, Campbell-Lee SA. Single donor versus pooled random donor platelet concentrates. Curr Opin Hematol. 2001;8(6):392–396. doi:10.1097/00062752-200111000-00013
15. Whitaker BI, Green J, King MR, et al. The 2007 Nationwide Blood Collection and Utilization Survey Report. Department of Health and Human Services, Washington, DC; 2008. Available from: http://www.hhs.gov/ophs/bloodsafety/20076nbcus_survey.pdf.
16. Storch EK, Custer BS, Jacobs MR, Menitove JE, Mintz PD. Review of current transfusion therapy and blood banking practices. Blood Rev. 2019;25:100593. doi:10.1016/j.blre.2019.100593
17. Andreu G, Vasse J, Hervé F, Tardivel R, Semana G. Introduction of platelet additive solutions in transfusion practice. Advantages, disadvantages and benefit for patients. Transfus Clin Biol. 2007;14(1):100–106. doi:10.1016/j.tracli.2007.03.009
18. Xiao W, Tormey CA, Capetillo A, Maitta RW. Allergic transfusion reactions to platelets are more commonly associated with prepooled than apheresis components. Vox Sang. 2013;105:334–340. doi:10.1111/vox.12063
19. Vamvakas EC. Risk-reduction strategies for platelet transfusion in the United States. Sci World J. 2011;11:624–640. doi:10.1100/tsw.2011.60
20. Vamvakas EC. Relative safety of pooled whole-blood-derived versus single-donor (apheresis) platelets in the United States: a systematic review of disparate risks. Transfusion. 2009;49:2743–2758. doi:10.1111/j.1537-2995.2009.02338.x
21. López-Menchero C, Alvarez M, Fernández P, Guzmán M, Ortiz-de-Salazar MI, Arbona C. Evolution of the residual risk of HBV, HCV and HIV transmission through blood transfusion in the region of Valencia, Spain, during a 15-year period (2003-2017). Blood Transfus. 2019;7:1–12. doi:10.2450/2019.0058-19
22. Trial to Reduce Alloimmunization to Platelets Study Group. Leukocyte reduction and ultraviolet B irradiation of platelets to prevent alloimmunization and refractoriness to platelet transfusions. N Engl J Med. 1997;337(26):1861–1869. doi:10.1056/NEJM199712253372601.
23. Slichter SJ, Kaufman RM, Assmann SF, et al. Dose of prophylactic platelet transfusions and prevention of hemorrhage. N Engl J Med. 2010;362:600–613. doi:10.1056/NEJMoa0904084
24. Triulzi DJ, Assmann SF, Strauss RG, et al. The impact of platelet transfusion characteristics on posttransfusion platelet increments and clinical bleeding in patients with hypoproliferative thrombocytopenia. Blood. 2012;7:8553–8561. doi:10.1182/blood-2011-11-393165
25. Singh RP, Marwaha N, Malhotra P, Dash S. Quality assessment of platelet concentrates prepared by platelet rich plasma-platelet concentrate, buffy coat poor-platelet concentrate (BC-PC) and apheresis-PC methods. Asian J Transfus Sci. 2009;3(2):86–94. doi:10.4103/0973-6247.53882
26. Pietersz RN. Pooled platelet concentrates: an alternative to single donor apheresis platelets? Transfus Apher Sci. 2009;41(2):115–119. doi:10.1016/j.transci.2009.07.003
27. Weinstein R, Simard A, Ferschke J, et al. Prospective surveillance of D- recipients of D+ apheresis platelets: alloimmunisation against D is not detected. Transfusion. 2015;55:1327–1330. doi:10.1111/trf.12972
28. Molnar R, Johnson R, Sweat LT, Geiger TL. Absence of alloimmunization in D– pediatric oncology patients receiving D-incompatible single-donor platelets. Transfusion. 2002;42:177–182. doi:10.1046/j.1537-2995.2002.00015.x
29. Villalba A, Santiago M, Freiria C, et al. Anti-D alloimmunization after RhD-positive platelet transfusion in RhD-negative women under 55 years diagnosed with acute leukemia: results of a retrospective study. Transfus Med Hemother. 2018;45(3):162–166. doi:10.1159/000488804
30. O´Brian KL, Hasper RL, Uhl L. Anti-D alloimmunization after D-incompatible platelet transfusions: a 14-year single-institution retrospective review. Transfusion. 2014;54:650–654. doi:10.1111/trf.12341
31. Cid J, Yazer MH, Lozano M. Platelet transfusion and respecting patient D type. Curr Opin Hematol. 2015;22(6):540–546. doi:10.1097/MOH.0000000000000185
32. Cooling LL, Kelly K, Barton J, Hwang D, Koerner TA, Olson JD. Determinants of ABH expression on human blood platelets. Blood. 2005;15:3356–3364. doi:10.1182/blood-2004-08-3080
33. Curtis BR, Edwards JT, Hessner MJ, Klein JP, Asher RH. Blood group A and B antigens are strongly expressed on platelets of some individuals. Blood. 2000;15:1574–1581. doi:10.1182/blood.V96.4.1574
34. Lozano M, Heddle N, Williamson LM, et al. Practices associated with ABO-incompatible platelets transfusions: a BEST collaborative international survey. Transfusion. 2010;50:1743–1748. doi:10.1111/j.1537-2995.2010.02642.x
35. Shehata N, Tinmouth A, Naglie G, Freedman J, Wilson K. ABO-identical versus nonidentical platelet transfusión: a systematic review. Transfusion. 2009;49:2442–2453. doi:10.1111/j.1537-2995.2009.02273.x
36. Dunbar NM, Ornstein DL, Dumont L. ABO incompatible platelets: risks versus benefit. Curr Opin Hematol. 2012;19:475–479. doi:10.1097/MOH.0b013e328358b135
37. Cooling L. ABO and platelet transfusion therapy. Immunohematology. 2007;23:20–33.
38. Solves P, Carpio N, Balaguer A, et al. Transfusion of ABO non-identical platelets does not influence the clinical outcome of patients undergoing autologous haematopoietic stem cell transplantation. Blood Transfus. 2015;13(3):411–416. doi:10.1007/s00277-017-3168-6
39. Stanworth SJ, Esrcourt LJ, Powter G, et al. A no-prophylaxis platelet transfusion strategy for hematologic cancers. N Engl J Med. 2013;368:1771–1780. doi:10.1056/NEJMoa1212772
40. Wandt H, Schaefer-Eckart K, Wendelin K, et al. Therapeutic platelet transfusion versus routine prophylactic transfusions in patients with haematological malignancies; an open-label, multicenter, randomized study. Lancet. 2012;380:1309–1313. doi:10.1016/S0140-6736(12)60689-8
41. Stanworth SJ, Escourt IJ, Llewelyn CA, Murphy MF, Wood EM. Impact of prophylactic platelet transfusions on bleeding events in patients with hematologic malignancies: a subgroup analysis of a randomized trial. Transfusion. 2014;54:2385–2393. doi:10.1111/trf.12646
42. Crighton GL, Schaefer-Eckart K, Wendelin K, et al. A therapeutic-only versus prophylactic platelet transfusion strategy for preventing bleeding in patients with haematological disorders after myelosuppressive chemotherapy or stem cell transplantation. Cochrane Database Syst Rev. 2015:CD010981. doi:10.1002/14651858.CD010981.
43. Crighton GL, Estcourt IJ, Llewelyn CA, et al. Platelet transfusions in patients with hypoproliferative thrombocytopenia: conclusions from clinical trials and current controversies. Hematol Oncol Clin North Am. 2016;30:541–560. doi:10.1016/j.hoc.2016.01.002
44. Malouf R, Ashraf A, Hadjinicolaoau AV, et al. Comparison of a therapeutic-only versus prophylactic platelet transfusion policy for people with congenital or acquired bone marrow failure disorders. Cochrane Database Syst Rev. 2018;4:CD012342. doi:10.1002/14651858.CD012342
45. Estcourt LJ, Stanworth SJ, Doree C, Hopewell S, Trivella M, Murphy MF. Comparison of different platelet count thresholds to guide administration pf prophylactic platelet transfusion for preventing bleeding in people with haematological disorders after myelosuppressive chemotherapy or stem cell transplantation. Cochrane Database Syst Rev. 2015;11:CD010983. doi:10.1002/14651858.CD010983
46. Estocurt LJ, Stanworth S, Doree C, et al. Different doses of prophylactic platelet transfusions for preventing bleeding in people with haematological disorders after myelosuppressive chemotherapy or stem cell transplantation. Cochrane Database Syst Rev. 2015;10:CD010984. doi:10.1002/14651858.CD010984
47. Rebulla P, Finazzi G, Marangoni F, et al. The threshold for prophylactic platelet transfusions in adults with acute myeloid leukemia. Gruppo Italiano Malattie Ematologiche Maligne dell’Adulto. N Engl J Med. 1997;337(26):1870–1875. doi:10.1056/NEJM199712253372602
48. Uhl L, Assmann SF, Hamza TH, Harrison RW, Gernsheimer T, Slichter SJ. Laboratory predictors of bleeding and the effect of platelet and RBC transfusions on bleeding outcomes in the PLADO trial. Blood. 2017;130:1247–1258. doi:10.1182/blood-2017-01-757930
49. Fletcher CH, DomBourian MG, Millward PA. Platelet transfusion for patients with cancer. Cancer Control. 2015;22(1):47–51. doi:10.1177/107327481502200107
50. Patel IJ, Davidson JC, Nikolic B, et al. Consensus guidelines for periprocedural management of coagulation status and hemostasis risk in percutaneous image-guided interventions. Standards of Practice Committee, with Cardiovascular and Interventional Radiological Society of Europe (CIRSE) Endorsement. J Vasc Interv Radiol. 2012;23(6):727–736. doi:10.1016/j.jvir.2012.02.012
51. Shah A, Stanworth SJ, McKechnie S. Evidence and triggers for the transfusion of blood and blood products. Anaesthesia. 2015;70 Suppl 1:
52. Desborough M, Hadjinicolaou AV, Chaimani A, et al. Alternative agents to prophylactic platelet transfusion for preventing bleeding in people with thrombocytopenia due to chronic bone marrow failure: a meta-analysis and systematic review. Cochrane Database Syst Rev. 2016;10:CD012055. doi:10.1002/14651858.CD012055.pub2
53. Kerkhoffs JL, Eikenboom JC, van de Watering LM, van Wordragen-vlaswinkel RJ, Wijermans PW, Brand A. The clinical impact of platelet refractoriness: correlation with bleeding and survival. Transfusion. 2008;48(9):1959–1965. doi:10.1111/j.1537-2995.2008.01799.x
54. Hod E, Schwartz J. Platelet transfusion refractoriness. Br J Haematol. 2008;142:348–360. doi:10.1111/j.1365-2141.2008.07189.x
55. Bishop JF, Matthews JP, McGrath K, Yuen K, Wolf MM, Szer J. Factors influencing 20-hour increments after platelet transfusion. Transfusion. 1991;31(5):392–396. doi:10.1046/j.15372995.1991.31591263191.x
56. Comont T, Tavitian S, Bardiaux L, et al. Platelet transfusion refractoriness in patients with acute myeloid leukemia treated by intensive chemotherapy. Leuk Res. 2017;61:62–67. doi:10.1016/j.leukres.2017.08.015
57. Solves P, Sanz J, Freiria C, et al. Factors influencing platelet transfusion refractoriness in patients undergoing allogeneic hematopoietic stem cell transplantation. Ann Hematol. 2018;97(1):161–167. doi:10.1007/s00277-017-3168-6
58. Tanoue S, Konuma T, Kato S, et al. Platelet transfusion refractoriness in single-unit cord blood transplantation for adults: risk factors and clinical outcomes. Biol Blood Marrow Transplant. 2018;24(9):1873–1880. doi:10.1016/j.bbmt.2018.05.006
59. Slichter SJ, Davis K, Enright H, et al. Factors affecting posttransfusion platelet increments, platelet refractoriness, and platelet transfusion intervals in thrombocytopenic patients. Blood. 2005;105:4106. doi:10.1182/blood-2003-08-2724
60. Forest SK, Hod EA. Management of the platelet refractory patient. Hematol Oncol Clin N Am. 2016;30:665–677. doi:10.1016/j.hoc.2016.01.008
61. Juskewitch JE, Norgan AP, De Goey SR, et al. How do I … manage the platelet transfusion-refractory patient? Transfusion. 2017;57(12):2828–2835. doi:10.1111/trf.14316
62. Rioux-Massé B, Cohn C, Lindgren B, Pulkrabek S, McCullough J. Utilization of cross matched or HLA-matched platelets for patients refractory to platelet transfusion. Transfusion. 2014;54:3080–3087. doi:10.1111/trf.12739
63. Yu QH, Shen YP, Ye BD, Zhou YH. Successful use of rituximab in platelet transfusion refractoriness in a multi-transfused patient with myelodysplastic syndrome. Platelets. 2015;26:195. doi:10.3109/09537104.2013.789842
64. Cid J, Guijarro F, Carbassé G, Lozano M. 24-h continuous infusion of platelets for patients with platelet transfusion refractoriness. Br J Haematol. 2018;181(3):386–389. doi:10.1111/bjh.14572
65. Cid J, Magnano L, Acosta M, Alba C, Esteve J, Lozano M. Rituximab, plasma exchange and intravenous immunoglobulins as a new treatment strategy for severe HLA alloimmune platelet refractoriness. Platelets. 2015;26(2):190–194. doi:10.3109/09537104.2014.895922
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.