")
Back to Journals » Journal of Blood Medicine » Volume 11
Physical Activity and Thrombophilic Risk in a Short Series
Authors Scudiero O , Gentile L, Ranieri A, Coppola E, Di Micco P, Mazzaccara C , D'alicandro G, Leggiero E, Frisso G, Pastore L , Lombardo B
Received 24 June 2019
Accepted for publication 28 October 2019
Published 30 January 2020 Volume 2020:11 Pages 39—42
DOI https://doi.org/10.2147/JBM.S220566
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Martin H Bluth
Olga Scudiero,1,2,* Luca Gentile,2,* Annaluisa Ranieri,1,2 Eduardo Coppola,3 Pierpaolo Di Micco,4 Cristina Mazzaccara,1,2 Giovanni D’alicandro,5 Eleonora Leggiero,2 Giulia Frisso,1,2 Lucio Pastore,1,2 Barbara Lombardo1,2
1Dipartimento di Medicina Molecolare e Biotecnologie Mediche, Università degli Studi di Napoli “Federico II”, Napoli, Italia; 2CEINGE-Biotecnologie Avanzate, Napoli, Italia; 3Vulcanair S.p.A, Casoria, Italia; 4Dipartimento di Medicina Interna, Ospedale Fatebenefratelli, Napoli, Italia; 5Centro di Medicina dello Sport e delle Disabilità, Dipartimento di Neuroscienze e Riabilitazione, AORN, Santobono-Pausillipon, Napoli, Italia
*These authors contributed equally to this work
Correspondence: Pierpaolo Di Micco
Dipartimento di Medicina Interna, Ospedale Fatebenefratelli, Via Alessandro Manzoni, Napoli, NA 80123, Italia
Email [email protected]
Barbara Lombardo
Dipartimento di Medicina Molecolare e Biotecnologie Mediche, Università degli Studi di Napoli “Federico II”, Corso Umberto I, 40, Napoli, NA 80138, Italia
Email [email protected]
Abstract: The role of influence on protein C anticoagulant system and PC deficiency-related thrombophilic risk due to strenuous physical exercise is still under discussion. To investigate the modification of the protein C anticoagulant pathway after vigorous exercise, we measured ProC® Global assay, a protein C activity dependent clotting time, in 20 healthy subjects before and immediately after maximal treadmill exercise, and at 5, 15, 30 and 60 min in the recovery phase. The most evident change was a shortening of ProC® Global clotting time from the average basal value of 123 sec to 84 sec at 30 min in post-exercise. Our study shows that the coagulation unbalance observed after strenuous exercise and with no consequence in healthy individuals with normal PC level, could increase the thrombophilic risk in silent carriers of significant defects of the protein C system and occasionally trigger an episode of deep vein thrombosis.
Keywords: ProC® Global, protein C unbalance after physical exercise, physical exercise; thrombophilic risk
Introduction
Among the effects of physical exercise on coagulation, the influence on protein C anticoagulant system and PC deficiency-related thrombophilic risk are still controversial.1 Several studies describe the impact of physical activity (PA) on the coagulation system.2,3 It is well known, that PA determines a shortening of the activated partial thromboplastin time (APTT) and an increase of the factor VIII.4 On the other hand, little is known about the variations of the anticoagulant determinants and specifically of Protein C (PC) system, during PA, and in the subsequent recovery phase. Sporadic cases of venous thrombosis in early recovery after exercise were reported in athletes bearing major defects of PC anticoagulant system.5 Other authors are still debating whether, and how, PA can trigger deep vein thrombosis (DVT) in subject carriers of a thrombophilic condition.6
In this study, to evaluate whether an unbalance in the PC system, induced by PA, could account for the triggering of thrombosis in subjects with major silent defects of the PC system, we analyzed the variations of the PC system in healthy subjects performing a treadmill procedure.7 We measured PC concentrations in these subjects before and after a physical exercise and during the subsequent recovery phase (up to one hour). It was a pilot study to investigate the modification of the protein C anticoagulant pathway after strenuous exercise in healthy subjects. Our results may be the proof-of-concept for a future study to evaluate the possible DVT risk in subjects carrying significant defects of the PC system.
Cases and Methods
We analyzed the variations of the PC system in healthy subjects performing a treadmill procedure.7 We measured the APTT before and after activation of endogenous PC, in these subjects before and after a physical exercise and during the subsequent recovery phase (up to one hour).
To generate preliminary data for a future validation study, twenty healthy volunteers (twelve males, age 18–43 y; media: 28.5 SD ± 5.30), endurance-trained, were enrolled. All subjects avoided aspirin, anti-inflammatory drugs, and free radical scavengers for two weeks before the test. Normal plasma levels of antithrombin, PC, protein S (PS), activated protein C (APC) resistance and homocysteine (data not shown) were observed. All participants gave informed consent to the study that was performed according to the Helsinki II Declaration and was approved by the Ethics Committee of the University of Naples “Federico II”.
The study was conducted in the morning after an overnight fast in a quiet room at a constant temperature of 21± 1C°. The treadmill procedure is described in detail elsewhere.8 Subjects performed a graded treadmill exercise starting at 3 km/h with a 3% uphill inclination and 3% grade increases every two minutes. Electrocardiographic features and arm blood pressure were continuously monitored during exercise. Subjects exercised until they reached their maximal heart rate-targeted endpoint. Blood samples were withdrawn before, immediately after exercise (i.e., peak value), and 5, 15, 30 and 60 mins after exercise (early recovery phase). Plasma was obtained from blood samples, collected in sodium citrate and centrifuged for 20 min at 3500 rpm. Plasma aliquots were stored at −70° C until assayed.
Protein C activity-dependent clotting time (PCAT) was measured on all blood samples by ProC® Global test (Siemens Healthcare, USA).
APTT (Pathromtin SL, Siemens Healthcare, USA) was also assayed with a BCS instrument.
Data analysis was performed with the GraphPad Prism version 3.0 for Windows (GraphPad Software Inc., San Diego, CA). All results are shown as medians with interquartile ranges. For data analysis was used the non-parametric Friedman test with Dunn’s post-test. Differences were considered significant at p<0.05.
In Table 1, APTT values decreased slightly, i.e., from a basal value of 37.5s (35.0–42.0) to 34.0s (31.0–39.3) and to 35.5s (32.3–38.0) at 15 and at 30 min post-exercise respectively. On the other hand, the Pro C values progressively dropped from a median basal level of 123s (114.7–152.3) to 84.5s (78.3–91.0) at 30 min post-exercise and turned versus baseline levels at 60 min post-exercise.
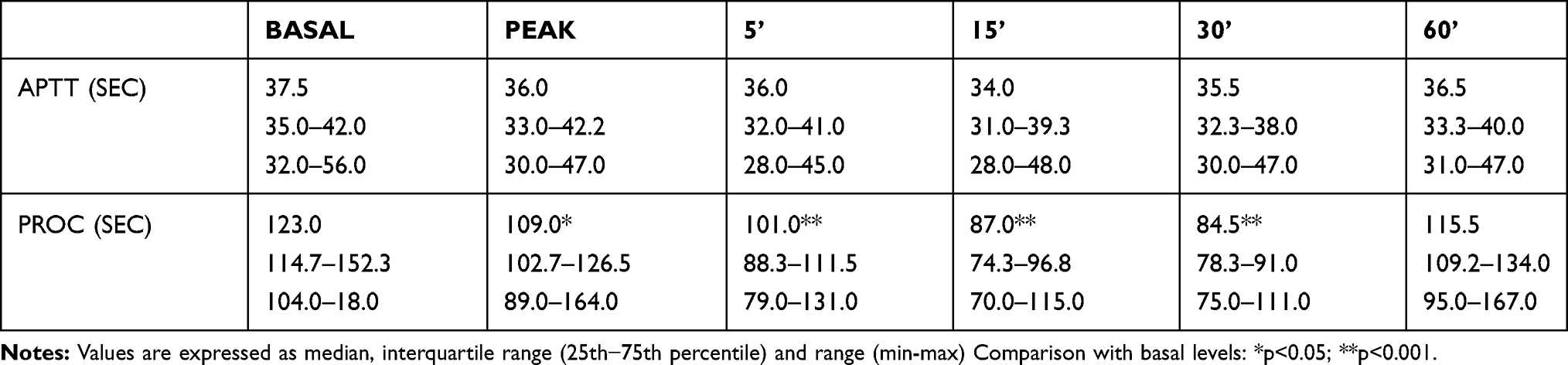 |
Table 1 Time Course of APTT and PROC Test in Subjects Undergoing a Maximal Treadmill Test. Sampling and Assays Were Done Before Exercise, at Peak (Immediately After Ending Exercise) and at 5, 15, 30, 60 Min After (Recovery Phase) |
Discussion
Deep vein thrombosis in professional athletes is a serious condition but to date, the literature is poor on this topic. The impact of vigorous exercise on the coagulation cascade is not yet understood, and the combined effect of exercise and defects of the PC system, should be studied.9,10
According to some studies, post-exercise hypercoagulability is counterbalanced by hyperfibrinolysis, whereas other investigators report that the increased level of fibrinolytic activity falls sharply during the recovery phase and that activation of coagulation persists.11
Our results show that the maximal hypercoagulability develops not during exercise but progressively during the first 30 min of the subsequent recovery phase, peaking at 30 mins.
The exercise-related hypercoagulability develops during the recovery phase to an extent greater than at exercise peak, likely as consequence of hemorheological variations occurring from exercise to resting phase.
It is still controversial whether post-exercise hypercoagulability, after a maximal treadmill, may induce or enhance the thrombophilic risk.12,13 In this study we showed that a temporary imbalance of the PC system occurs within 30 mins; probably this phenomenon may be compensated in healthy subjects by the normal anticoagulant level.
The alteration of protein C levels and activity may be easily related to an endothelial dysfunction due to physical exercise. From a pathophysiological point of view, the reported modification may have several implications in a prothrombotic way: the protein C activity, in fact, is not only associated to inactivation of factor V and factor VIII but also hypofibrinolysis because of the role of thrombomodulin. Therefore, the prothrombotic state may be associated with clinical thrombosis by two different ways an acquired thrombophilia because of the reduced action of protein C and an induced hypofibrinolysis.
Moreover, our results suggest that the subjects with significant silent defects of the PC system, like those described in previous reports,5 could be particularly vulnerable to hypercoagulability during the early recovery phase. A possible explanation is that in this phase the coagulation wave, amplified by the slowing of blood flow, could overwhelm the significantly reduced anticoagulant potential and occasionally trigger an episode of DVT, depending on the association to other circumstantial/environmental factors.1,14
Conclusions
The knowledge about the changes in coagulation status should be further examined and also further studies involved in physical training will be essential in the future to better understand the complex mechanism of coagulation balance. Therefore, the possibility to evaluate the PC system activity together with the treadmill test in subjects that perform physical activity might represent a screening strategy to predict possible DVT episode in individuals carrying significant defects in the coagulation cascade.
The main limitation of our study is its small size. As this is a pilot study, we plan to validate the study enrolling additional healthy subjects, and, above all, analyzing patients with silent major protein C defects, to verify the size of the unbalancing of the PC pathway, with is related to DVT risk.
Ethical Approval and Consent to Participate
Authors certify that the data of each described patient are associated to a specific written informed consent with the agreement to publish this clinical experience.
Acknowledgment
We thank Dr. Ernesto Grimaldi for assistance and for comments that significantly improved the manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Lombardo B, Izzo V, Terracciano D, et al. Laboratory medicine: health evaluation in elite athletes. Clin Chem Lab Med. 2019;57:1450–1473. doi:10.1515/cclm-2018-1107
2. Grabowski G, Whiteside WK, Kanwisher M. Venous thrombosis in athletes. JAAOS. 2013;21(2):108–117. doi:10.5435/JAAOS-21-02-108
3. El Sayed MS, Sale CP, Jones J, Chester M. Blood hemostasis in exercise and training. Med Sci Sports Exerc. 2000;32:918–925. doi:10.1097/00005768-200005000-00007
4. De Caterina M, Grimaldi E, Passaretti M, et al. Four cases of venous thrombosis in athletes with silent hereditary defects of the protein C system. Thromb Haemost. 2005;94:463–464.
5. Lippi G, Franchini M, Favaloro EJ. Unsuspected triggers of venous thromboembolism-trivial or not so trivial. Semin Thromb Hemost. 2009;35:597–604. doi:10.1055/s-0029-1242713
6. Rimmer JE, Cooper PC, Brookfield CJ, Preston FE, Makris M. Evaluation of a global screening assay for the investigation of the protein C anticoagulant pathway. Clin Lab Haematol. 2000;22:351–354. doi:10.1046/j.1365-2257.2000.00336.x
7. Brevetti G, De Caterina M, Martone VD, et al. Exercise increases soluble adhesion molecules ICAM-1 and VCAM-1 in patients with intermittent claudication. Clin Hemoreol Microcirc. 2001;24:193–199.
8. Hegde SS, Goldfarb AH, Hegde S. Clotting and fibrinolytic activity change during the 1 hr after a submaximal run. Med Sci Sports Exerc. 2001;33:887–892. doi:10.1097/00005768-200106000-00006
9. Duchman KR, Westermann RW. Incidence and risk factors for venous thromboembolism following hip arthroscopy: a population-based study. Arthroscopy. 2019;35(8):2380–2384. doi:10.1016/j.arthro.2019.03.054
10. Zadow EK, Adams MJ, Kitic CM, Wu SSX, Fell JW. Acquired and genetic thrombotic risk factors in the athlete. Semin Thromb Hemost. 2018;44(8):723–733. doi:10.1055/s-0038-1673625
11. Lee KW, Lip GYH. Acute versus habitual exercise, thrombogenesis, and exercise intensity. Thromb Haemost. 2004;91:416–419. doi:10.1055/s-0037-1614284
12. Hilberg T, Prasa T, Sturzebecher J, Glasser D, Gabriel HH. Thrombin potential and thrombin generation after exhaustive exercise. Int J Sports Med. 2002;23:500–504. doi:10.1055/s-2002-35123
13. Weiss C, Egermann M, Weiss T, Bartsch P. Exercise-induced activation of coagulation in thrombophilia. J Thromb Haemost. 2003;1:1312–1313. doi:10.1046/j.1538-7836.2003.t01-1-00326.x
14. Mazzaccara C, Conti V, Liguori R, et al. Warfarin anticoagulant therapy: a southern italy pharmacogenetics-based dosing model. PLoS One. 2013;8(8):e71505. doi:10.1371/journal.pone.0071505
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.