")
Back to Journals » Drug Design, Development and Therapy » Volume 13
Pharmacokinetics of fixed-dose combination of atorvastatin and metformin compared with individual tablets
Authors Ghim JL, Phuong NTT, Kim MJ, Kim EJ , Song GS, Ahn S , Shin JG, Kim EY
Received 2 November 2018
Accepted for publication 7 March 2019
Published 13 May 2019 Volume 2019:13 Pages 1623—1632
DOI https://doi.org/10.2147/DDDT.S193254
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sukesh Voruganti
Jong-Lyul Ghim,1–3,* Nguyen Thi Thu Phuong,1–2,4,* Min Jung Kim,1,2 Eun-Ji Kim,5 Geun Seog Song,5 Sangzin Ahn,1,2 Jae-Gook Shin,1,2 Eun-Young Kim1–3
1Department of Pharmacology and Clinical Pharmacology, PharmacoGenomics Research Center, Inje University College of Medicine, Busan, Republic of Korea; 2Center for Personalized Precision Medicine of Tuberculosis, Inje University College of Medicine, Busan, Republic of Korea; 3Department of Clinical Pharmacology, Inje University Busan Paik Hospital, Busan, Republic of Korea; 4Faculty of Pharmacy, Hai Phong University of Medicine and Pharmacy, Haiphong, Vietnam; 5CJ HealthCare Co., Ltd, Seoul, Republic of Korea
*These authors contributed equally to this work
Purpose: The aims of this study was to investigate the mutual pharmacokinetic interactions between steady-state atorvastatin and metformin and the effect of food on the fixed-dose combined (FDC) tablet of atorvastatin and metformin extended release (XR).
Subjects and methods: Study 1, an open-labeled, fixed sequence, multiple-dose pharmacokinetic drug-drug interaction study, was divided into 2 parts. Atorvastatin (40 mg) or metformin (1,000 mg) XR tablets were administered once daily via mono- or co-therapy for 7 days. Plasma levels of atorvastatin and 2-OH-atorvastatin, were quantitatively determined for 36 h in part A (n=50) while metformin plasma concentration was measured up to 24 h in part B (n=16) after the last dosing. Study 2, a randomized, open-labeled, single-dose, two-treatment, two-period, two-sequence crossover study, involved 27 healthy subjects to investigate the impact of food intake on the pharmacokinetics of a combined atorvastatin/metformin XR 20/500 mg (CJ-30056 20/500 mg) tablet.
Results: After multiple doses of mono- or co-therapy of atorvastatin (40 mg) and metformin (1,000 mg) XR, the 90% confidence intervals (CIs) of the geometric mean ratios (GMRs) for the peak plasma concentration at steady state (Cmax,ss) and area under the plasma concentration–time curve during the dosing interval at steady state (AUCτ,ss) were 1.07 (0.94–1.22) and 1.05 (0.99–1.10) for atorvastatin, 1.06 (0.96–1.16) and 1.16 (1.10–1.21) for 2-OH-atorvastatin, and 1.00 (0.86–1.18) and 0.99 (0.87–1.13) for metformin, respectively. Food delayed time to reach maximum concentration (tmax), decreased atorvastatin Cmax by 32% with a GMR (90% CI) of 0.68 (0.59–0.78), and increased metformin AUCt by 56% with a GMR (90% CI) of 1.56 (1.43–1.69).
Conclusion: No clinically relevant pharmacokinetic interaction was seen when atorvastatin was co-administered with metformin. Food appeared to change the absorption of atorvastatin and metformin from an FDC formulation. These alterations were in accordance with those described with the single reference drugs when ingested with food.
Keywords: pharmacokinetics, drug interaction, atorvastatin, metformin, food effect
Introduction
Cardiovascular disease (CVD) is the leading cause of death and morbidity for patients with type 2 diabetes.1,2 All adult diabetes patients are at a high risk of a recurrent cardiovascular event, and hyperlipidemia is one of the major risk factors for cardiovascular events.1 During glucose control, it is recommended that an assessment of the cardiovascular risk factor be performed at diagnosis and at least annually.3 Among the risk factors of CVD, co-morbidity of type 2 diabetes and dyslipidemia is approximately 80%, which means many people with type 2 diabetes mellitus also have dyslipidemia.2 It is strongly recommended by the International Diabetes Federation Guideline Development Group to treat dyslipidemia in high-risk individuals with type 2 diabetes mellitus.4 Strong and consistent evidence has shown that statins reduce the risk of death or CVD events over a wide range of cholesterol levels; this was also observed when the cholesterol level was within the normal range.5–7 For persons with type 2 diabetes, it is highly recommended that dyslipidemia be treated concomitantly with glucose control. It is also recommended that combination therapy of antidiabetic drugs and statin be indicated.2 Owing to this, in a clinical setting, hypoglycemic medication and lipid-lowering agents are frequently prescribed together.
As a 3‐hydroxy‐3‐methyl-glutaryl coenzyme A reductase inhibitor, atorvastatin efficiently reduces cholesterol8 and triglyceride levels in a dose‐dependent manner in hyperlipidemic patients. Among statins, atorvastatin results in greater reductions in cholesterol and triglycerides than other drugs in this class. It has also become one of the most widely used statin worldwide.8–10 Atorvastatin is administered in the active acid form, which is completely absorbed after oral administration. However, atorvastatin is extensively metabolized by cytochrome P450 3A4 (CYP3A4) in the gut wall and liver, to form the main active hydroxy-metabolite, ortho‐hydroxy‐atorvastatin (2‐OH‐atorvastatin).11 Metformin is generally considered the first choice oral medication for the treatment of type 2 diabetes, unless there is evidence of renal impairment or other contraindications.12 Metformin does not undergo metabolism13 and is eliminated in the urine as unchanged drug. It also has a half-life of approximately 5 h.14 When administered once daily, metformin extended release (XR) appears more effective than the conventional immediate release formulation for the improvement of glyco-metabolic control, lipid panel, and the levels of some adipocytokines in type 2 diabetes mellitus patients.15 However, an evaluation of the effect of food on a fixed-dose combination tablet containing ẽ component, is required during drug development. This is because the gastrointestinal pH and changes in transit time can result in variability in drug release and/or absorption.
To develop a novel combination tablet containing atorvastatin (20 mg) and metformin (500 mg) XR, we conducted 2 clinical studies. Study 1 investigated the mutual pharmacokinetic interaction of reference formulation of atorvastatin and metformin XR after multiple-dose administration. Study 2, on the other hand, was aimed at assessing the effect of food on FDC tablet containing atorvastatin and metformin XR.
Material and methods
Subjects
The study protocols (ClinicalTrials.gov identifier: NCT01765023 for Study 1 and NCT02160743 for Study 2) were reviewed and approved by the Inje University Busan Paik Hospital Institutional Review Board. The study was conducted in accordance with the Declaration of Helsinki, the International Conference on Harmonisation of Good Clinical Practice (ICH-GCP), and the guideline for Korean Good Clinical Practice (KGCP).
Healthy male subjects aged 19–45 years and within 20% of their standard body weight according to the Broca formula,16 were eligible for participation in the studies. The volunteers were determined to be healthy by physical examination, vital signs, 12-lead ECG, and clinical laboratory values. Subjects that met any of the following criteria were excluded: administration of inducers or inhibitors of CYP3A4 1 month prior to this study, symptoms of acute disease 4 weeks prior to this study, an allergic disease history or hypersensitivity reactions, gastrointestinal surgery or disease that could potentially impact drug absorption during the study period, abnormal laboratory test results, excessive caffeine intake (>5 cups/day), smoking (>10 cigarettes/day), alcohol consumption (>30 g/day), a special diet containing foods known to influence the pharmacokinetic of the drugs administered in the study (eg, grapefruit juice), a history of participation in another clinical study 60 days prior to this study, donated blood 60 days prior to this study, or has a known allergy to metformin or atorvastatin. All subjects gave written informed consent before study initiation.
Study design
The schematic designs of two studies are shown in Figure 1. In Study 1, an open-labeled, fixed sequence, consisting of multiple dosing was applied to evaluate the pharmacokinetic interactions of atorvastatin and metformin at steady state. This drug interaction study consisted of 2 parts: part A evaluated the pharmacokinetic of atorvastatin while part B evaluated the pharmacokinetic of metformin. For atorvastatin and metformin, with approximate 8 hr half-life in subjects with normal renal function, steady-state concentrations could be reached after 4–5 days. Therefore, to evaluate the effect of metformin XR on atorvastatin disposition in a steady state in part A, atorvastatin (40 mg) was dispensed once daily for 7 days. After the 2-week washout period,17 atorvastatin (40 mg) and 2 tablets of metformin (500 mg) XR were dispensed together once daily for 7 days. The drugs were administered at 8 AM, following overnight fasting. Plasma samples were collected at pre-dose (0 h), 0.33, 0.66, 1, 1.5, 2, 3, 4, 6, 8, 12, 24 and 36 h on the 7th day of every administration of atorvastatin (only), and combined atorvastatin and metformin XR. The number of subjects was calculated from previous studies.17,18 The minimal number of subject enrolled was 47; however, after the expected dropout, 60 subjects were enrolled. To investigate the effect of atorvastatin on metformin pharmacokinetics at steady state in part B of study 1, 2 tablets of metformin (500 mg) XR were dispensed once daily for 7 days. After the 1-week washout period,14 2 tablets of metformin (500 mg) XR and atorvastatin (40 mg) were dispensed once daily for 7 days. The drugs were administered at 8 AM, following an overnight fasting. Plasma samples for metformin were collected every 7th day at predose (0 h), 1, 2, 3, 4, 5, 6, 7, 8, 10, 12, 14 and 24 h. The number of subjects was calculated from previous studies.14,19 Based on an inter-subject coefficient of variation of 22% for both the AUC0–t and Cmax of metformin, the minimum number of participants was 12; however, following the expected dropout, 20 subjects were enrolled. According to the recommendation of the US Food and Drug Administration,20 to maximize the potential drug-drug interaction (DDI) effect, atorvastatin (40 mg) (Lipitor®, Pfizer, Inc.) and 2 tablets of metformin (500 mg) XR (Glucophage® XR, Merck Serono, Inc.) were used for in parts A and B of study 1.
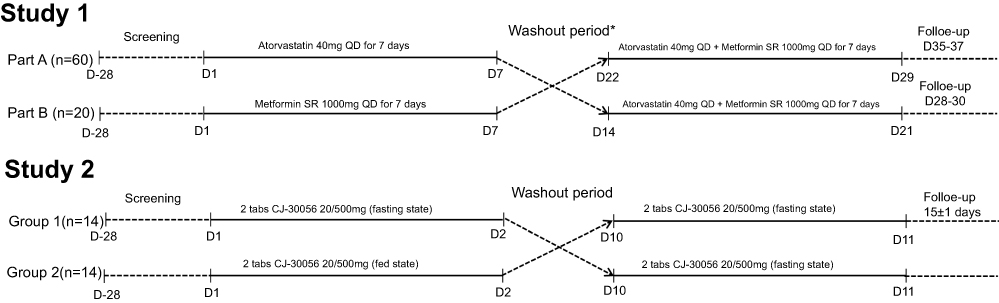 | Figure 1 Study design. *In study 1, the washout periods in part A and part B are 2 weeks and 1 week, respectively. |
Study 2 was performed to investigate the safety and the effect of food intake on the pharmacokinetic of the FDC tablet of atorvastatin/metformin XR 20/500 mg (CJ-30056 20/500 mg) (CJ HealthCare Co., Ltd., Korea) using a randomized, open-labeled, single-dose, two-treatment, two-period, two-sequenced crossover method. In the fasting state study, the test drugs were administered at 8 AM, following overnight fasting. In the fed state study, the drug was also dispensed at 8 AM; however, a high-fat diet was provided 30 min before medication, and the subjects consumed their meal in 10 mins. Fasting and fed state studies were performed in a crossover manner with a washout period of 1 week. Plasma samples were collected pre-dose (0 h), 0.33, 0.66, 1, 1.5, 2, 3, 4,5, 6, 8, 12, 24 and 36 h, and pre-dose (0 h), 1, 2, 3, 4, 5, 6, 7, 8, 10, 12, 14 and 24 h for atorvastatin and metformin analysis, respectively. The number of subjects in the study was according to the Korean bioequivalence study guideline.14 Based on the guided recommendation of the FDA, a minimum number of 12 evaluable subjects per group should be recruited to conduct the bioequivalence studies. Considering the dropout rate, 14 subjects were enrolled for each group.
To evaluate the safety of the drugs, vital signs (including sitting blood pressure, heart rate, and tympanic temperatures), physical examination, and laboratory tests (including hematology, biochemistry and urinalysis) were assessed.
Bioanalysis
Blood sample was prepared by liquid-phase extraction for atorvastatin and its metabolite. A simple protein precipitation was applied to extract metformin from the plasma. Validated LC-MS/MS methods were used to measure the study drugs.21,22 The assay had lower limits of quantification (LLQ) in plasma, 0.2 ng/mL for atorvastatin and 2-OH-atorvastatin, and 10 ng/mL for metformin. The validated linear concentration ranges were 0.2–100 ng/mL for atorvastatin and its metabolite and 10–3,000 ng/mL for metformin. The overall coefficient of variation (CV) for assay precision in atorvastatin and 2-OH atorvastatin ranged from 1.4% to 4.7% and 1.4% to 4.0%, respectively. The overall accuracy for atorvastatin and 2-OH atorvastatin ranged from 91.5% to 109.5% and 92.3% to 105.2%, respectively. The overall CV for assay precision and accuracy in metformin ranged from 0.6% to 2.3% and 96.6% to 105.1%, respectively.
Pharmacokinetic analysis and statistical methods
Noncompartmental analysis was applied to describe pharmacokinetic profiles of atorvastatin, 2-OH-atorvastatin, and metformin for both studies using Phoenix WinNonlin® software, version 6.3 (Pharsight Corporation, California). In study 1, the maximum concentration at steady state (Cmax,ss) and the area under the concentration-time curve during dosing interval at steady state (AUCτ,ss), were considered primary endpoints. The Cmax,ss and the time to reach Cmax,ss (tmax,ss) were calculated directly from the concentration-time curve. The AUCτ,ss was calculated using a combination of linear-up and log-down trapezoidal methods.
Continuous variables are expressed as mean ± SD. Geometric mean ratios (GMRs) and its 90% confidence intervals (CIs) of Cmax,ss and AUCτ,ss, AUCt, AUCinf for atorvastatin, its active metabolite, and metformin were estimated.
Statistical analysis was performed in the SAS software (SAS Institute Inc., Cary, NC, USA) and R software, version 3.2.4 (A Language and Environment for Statistical Computing, Vienna, Austria23). Time to maximum plasma concentration comparisons were conducted using the Wilcoxon signed-rank test and the Hodges–Lehmann estimate of median difference. The frequencies of overall adverse events (AEs) and AEs classified by system organ class were compared between treatments by means of a 95% CI for the difference between paired proportions and P-values from McNemar’s test.
Results
Study subjects
In the study of atorvastatin DDI with metformin (Study 1), 50 of the 60 subjects completed the study as 5 subjects withdrew consent, 2 were excluded due to investigator’s discretion, and 3 were excluded due to the lab abnormality result of mild hepatic enzyme elevation. In the study of metformin DDI with atorvastatin, 16 of the 20 subjects completed the study as 2 subjects withdrew and 2 were excluded because of mild hepatic enzyme elevation. In study 2 to assess the effect of food on FDC tablet, 1 subject withdrew and a total of 27 subjects completed the study.
In the DDI study, mean ± SD values for age, weight, height in part A and B of study 1 were 24.88±3.53 and 23.90±2.34 years, 69.32±6.12 and 66.12±6.70 kg, 174.57±5.54, and 175.95±5.52 cm, respectively. The effect of food study was conducted in Korean adult male subjects ranging in age from 20 to 29 years (mean ± SD, 24.36±2.47 and 25.29±2.70), weighing between 69.58±9.22 and 67.43±8.93 kg, and averaging 175.57±6.32 and 174.50±4.94 cm in height for groups 1 and 2, respectively. The participants’ demographic characteristics did not differ significantly between the sequences and parts in both studies (P-value >0.05, 2-sample t-test)
Drug-drug interaction study
Figure 2 shows the plasma concentration versus time profiles of atorvastatin, 2-OH atorvastatin, and metformin. The pharmacokinetic parameters and statistics are presented in Table 1.
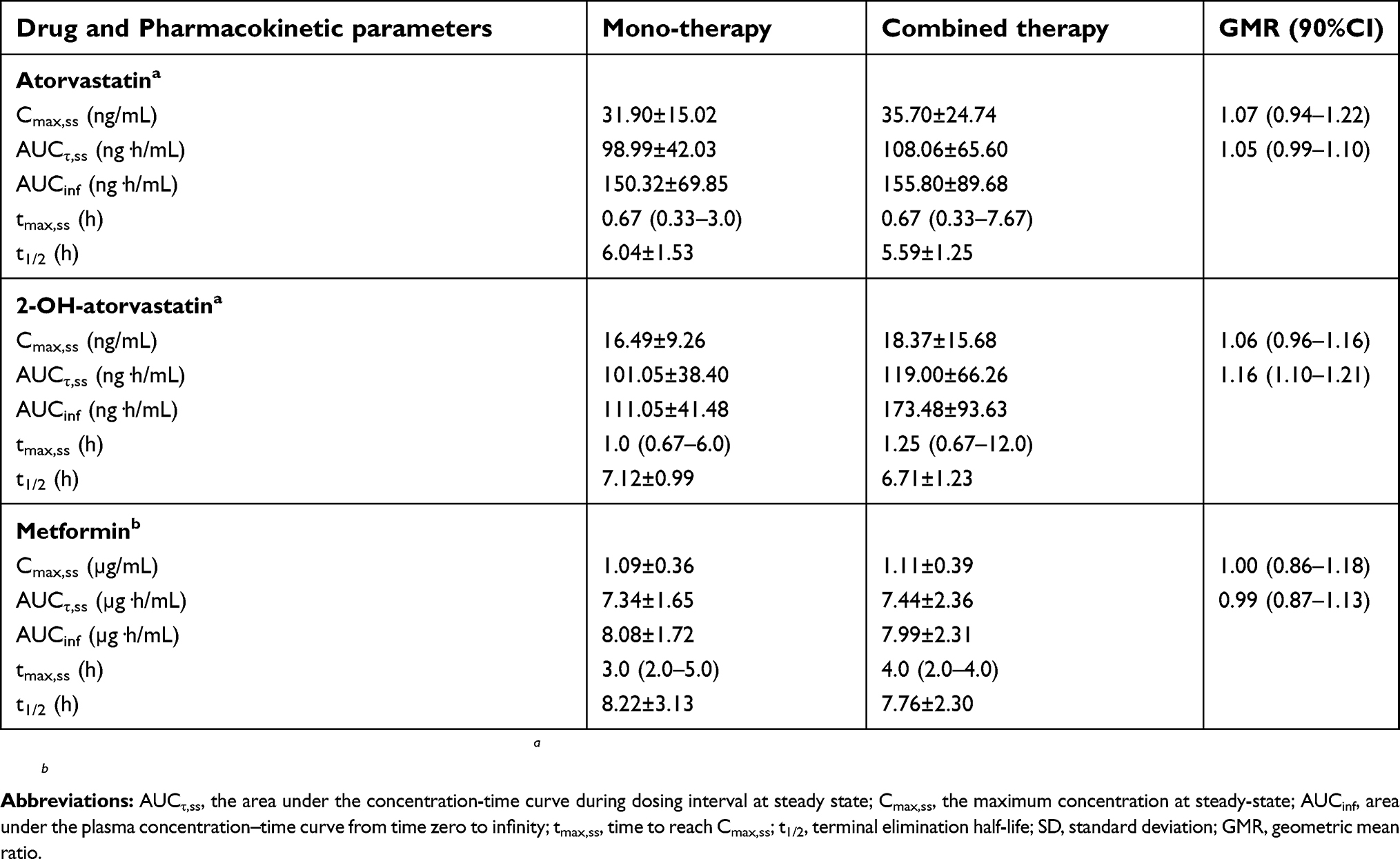 | Table 1 Pharmacokinetic parameters of atorvastatin, 2-OH-atorvastatinstherapy |
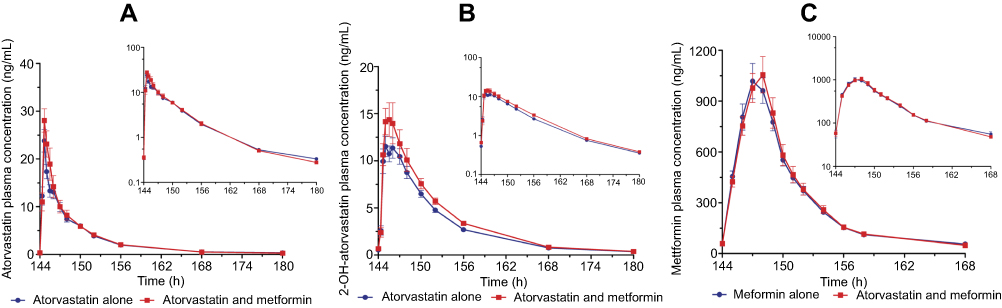 | Figure 2 Mean (standard error) plasma concentration–time profiles of atorvastatin (A), 2-OH-atorvastatin (B) and metformin (C) in healthy Korean subjects on Study Day 7 following the oral administration of atorvastatin 40 mg and 2 tablets of metformin 500 mg XR daily (red squares, dash line) or atorvastatin 40 mg (only) daily (blue circles, solid line). |
When the co-therapy regimen was administered, steady state exposures of atorvastatin, 2-OH-atorvastatin, and metformin were minimally affected (<20% change). Atorvastatin AUCτ,ss and Cmax,ss increased when co-administered with metformin by 5% and 7% (GMR [90%CI], 1.05 [0.99–1.10] and 1.07 [0.94–1.22], respectively); the tmax,ss (~1 h) did not differ (P-value=0.495, Hodges-Lehmann estimate). Similarly, the AUCτ,ss and Cmax,ss of 2-OH-atorvastatin increased by 6% and 5% (GMR [90%CI], 1.16 [1.10–1.21] and 1.06 [0.96–1.16], respectively). The tmax,ss (~2 h) and elimination half-life displayed no recognizable difference when metformin was dispensed. In addition, AUCτ,ss and Cmax,ss for metformin at steady state were similar to the GMR (90%CI) values (0.99 [0.87–1.13] and 1.01 [0.86–1.18], respectively). The tmax,ss and t1/2 did not appear to have a significant difference (P-value =0.152 and 0.838, respectively, Hodges-Lehmann estimate) between with and without atorvastatin co-therapy regimen.
In general, AUCτ,ss and Cmax,ss of 2-OH-atorvastatin, the active metabolite of atorvastatin, and metformin showed similar results compared to mono- and co-administration (Figure 2B). The 90% CIs for the GMR for the combination therapy to the monotherapy were completely within the limits of 0.80 and 1.25 for AUCτ,ss and Cmax,ss of atorvastatin, 2-OH-atorvastatin, and metformin.
Food effect study
Food showed a significant effect on the extent of absorption of metformin from a combination tablet. GMR and 90% CI for log-transformed Cmax of atorvastatin in fed conditions were lower than those in the fasting condition (32% lower; GMR [90%], 0.68 [0.59–0.78]); AUCt did not differ. The reduction in Cmax suggested that food slowed the rate of atorvastatin absorption in the combined tablet, as indicated by the tmax for atorvastatin and its active metabolite occurring approximately 2–3 h later when fasting is compared to the fed condition (Table 2 and Figure 3). Food significantly increased the absorption of metformin from the FDC formulation. GMR values and 90%CIs, AUCt and AUCinf of metformin under fasted and fed conditions were 1.56 (1.43–1.69) and 1.51 (1.40–1.63), respectively. A recognizable difference was not observed in the Cmax, which was only 3% higher (GMR[90%CI], 1.03 [0.94–1.12]). Similarly with atorvastatin, the time to reach the maximum concentration of metformin was slower as this occurred approximately 2 h later under the effect of food.
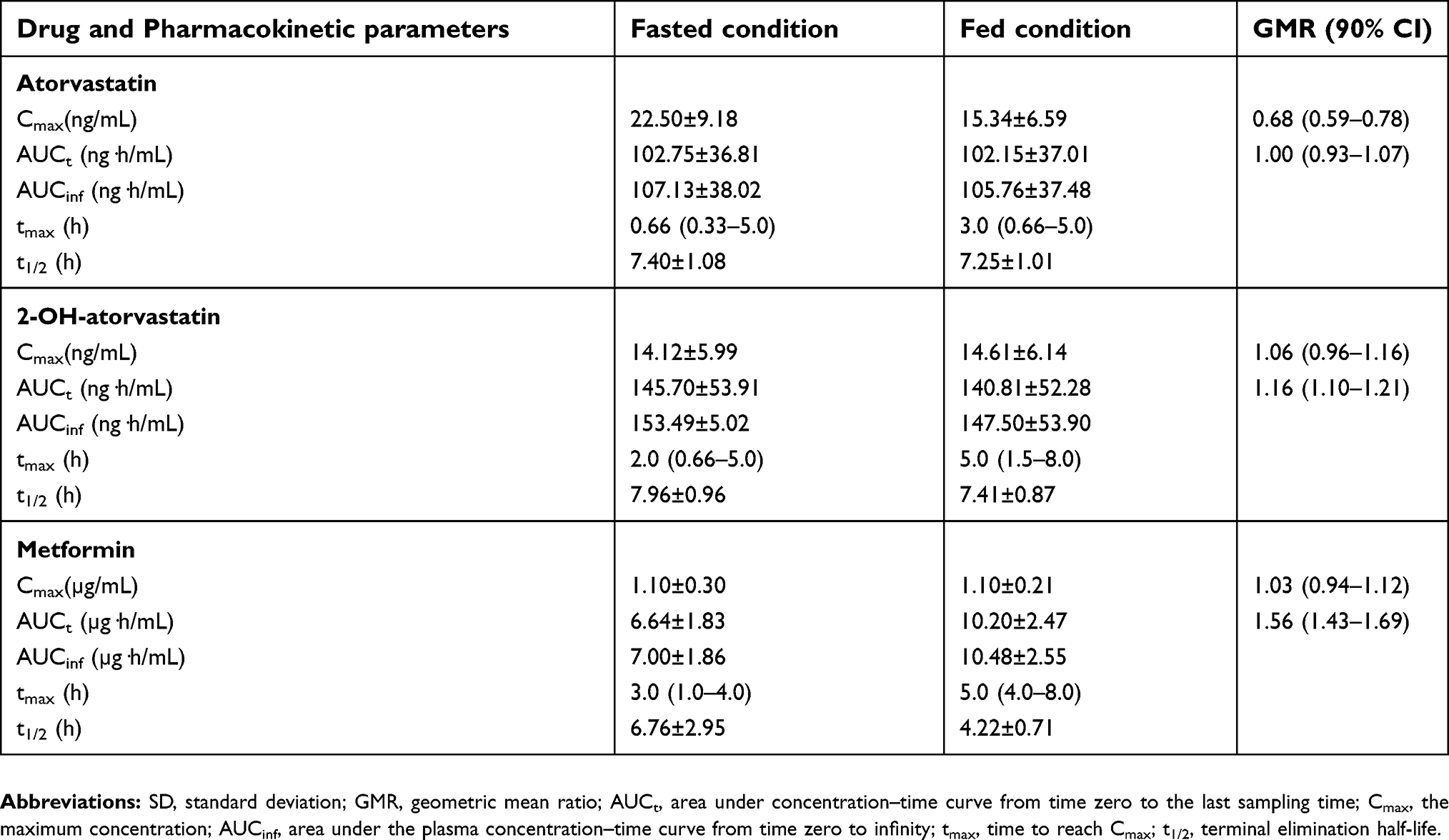 | Table 2 Pharmacokinetic parameters of atorvastatin, 2-OH-atorvastatin, metformin after a single oral dose of 2 tablets of fixed-dose combined atorvastatin 20 mg/metformin 500 mg XR under fasted and fed conditions |
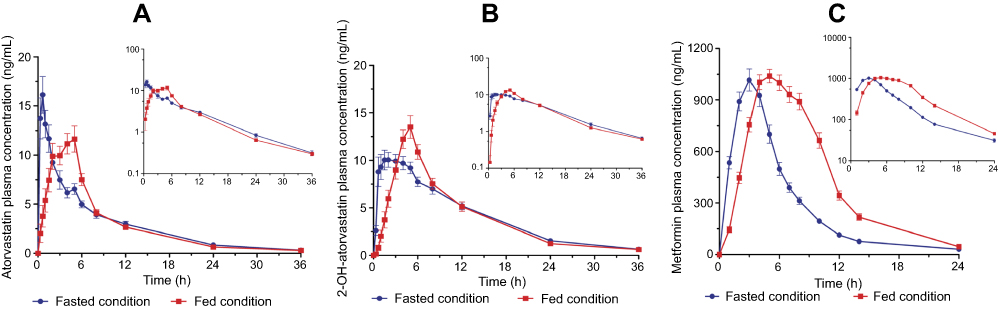 | Figure 3 Mean (standard error) plasma concentration–time profiles of atorvastatin (A), 2-OH-atorvastatin (B) and metformin (C) in 23 healthy Korean subjects following a single oral administration of 2 tablets of fixed-dose combined atorvastatin/metformin XR 20/500 mg under fasted condition (blue circles, solid line) or fed condition (red squares, dash line). |
Safety and tolerability profile
Co-administration of metformin and atorvastatin in multiple doses for 7 days and in a single-dose were well tolerated in healthy subjects. No serious adverse events were reported. In the DDI study, to evaluate the effect of metformin on the pharmacokinetic of atorvastatin at steady state, 10 of the 60 participants (16.67%) in monotherapy group and 13 of the 51 participants (25.49%) in the co-therapy group reported drug-related AEs and laboratory abnormalities. However, the difference between the 2 treatments was not statistically significant (P-value =0.241, McNemar’s test). To investigate the impact of atorvastatin on the pharmacokinetic of metformin, 7 of the 20 participants (35%) in the monotherapy group and 2 of the 17 participants (11.76%) in the co-therapy group reported drug-related AEs and laboratory abnormalities. There was no significant difference between the 2 groups (P-value =0.850, McNemar’s test). The most common reported AE was gastrointestinal disorders in both parts of the study. All AEs were noted as being mild to moderate with a spontaneous recovery.
In the effect of food evaluation study, 1 of 27 subjects (3.7%) reported to having a mild headache after taking an FDC of atorvastatin/metformin XR 20 mg/500 mg in fasting state whereas no adverse events occurred among the 27 subjects was reported during fed condition. No clinically remarkable alterations were observed in the laboratory tests results, including hematology, biochemistry, and urinalysis, vital signs, or physical examination.
Discussion
The present study demonstrated that there was no clinically relevant interaction between atorvastatin and metformin XR when co-administered after multiple dosing; the combination was well tolerated by the study subjects. We also observed that food increased metformin XR exposure without affecting atorvastatin bioavailability.
Differences between the pharmacokinetic properties of atorvastatin and metformin have been illustrated in previous studies.7,24,25 Atorvastatin was extensively metabolized by CYP3A to form active metabolites whereas metformin was not metabolized in the liver.13,26 In various transport studies, atorvastatin has been demonstrated to be a P-glycoprotein substrate and an inhibitor of multidrug resistance-associated protein 2 (MRP2) and organic anion transporting polypeptide. Interestingly, organic cation transporters are primarily responsible for the absorption, liver uptake and renal excretion of metformin.14,27,28 This suggests that the possibility of DDI between atorvastatin and metformin is minute.
A great advantage of the co-administration of metformin and atorvastatin has been reported. Tousoulis et al observed that the combination partially prevented glucose loading induced elevation of glucose levels, and reduced the post-glucose loading levels of TNF-α compared to metformin monotherapy.29 The study by Matafome et al evaluated liver complications occurring in type 2 diabetes patients with hyperlipidemia and the effects of atorvastatin and metformin. Indeed, the combination therapy further lowered C-reactive protein, adiponectin, liver tumor necrosis factor-α and interleukin-6, systemic and hepatic oxidative stress and portal inflammation. Another study indicated that the combination of atorvastatin and metformin may improve liver injury in people with type 2 diabetes mellitus with hyperlipidemia.30 A study investigating the effect of statins on glucose-induced endothelial dysfunction indicated that in patients with type 2 diabetes, glucose loading blunted endothelial function and deteriorated endothelium-dependent dilation (EDD). The co-administration of metformin and atorvastatin for 6 weeks partially prevented the glucose-induced impairment of EDD in these patients.31 More interestingly, metformin inhibited both glucose and lipid biosynthesis by downregulating sterol regulatory element −2 gene expression.32 These findings support the need for the combined formulation of metformin and atorvastatin when treating type 2 diabetes mellitus with or without dyslipidemia. This will decrease the pill burden and increase patient compliance.
Based on these facts, the atorvastatin/metformin XR 20 mg/500 mg FDC tablet was developed and mutual pharmacokinetic (PK) interaction was evaluated in healthy subjects against the reference formulation of atorvastatin and metformin XR after multiple-dose administration. The results of our study clearly showed that the two therapies containing mono- and co-therapy displayed similar pharmacokinetic profiles for atorvastatin and metformin in healthy subjects. The 90% CIs for pharmacokinetic parameters (Cmax and AUC) for atorvastatin and metformin were well within regulatory acceptance criteria, demonstrating no clinically significant PK interaction at steady state of atorvastatin when combined with metformin XR.
The regular administration of metformin XR tablet is once daily with the evening meal, while atorvastatin is prescribed for intake either in the morning or in the evening, regardless of meal consumption. Owing to different drug administrations between atorvastatin and metformin, an additional study was carried out to evaluate the impact of food intake on the pharmacokinetic behaviors of the 2 drugs. Two tablets of atorvastatin/metformin XR 20/500 mg [total dose of atorvastatin (40 mg) and metformin (1,000 mg)] FDC were administered once for the fasting and fed state. The delaying effect of food on the absorption of atorvastatin and metformin was expected, and were similar in magnitude to changes observed in previous food effect pharmacokinetic studies using the reference formulations.33 When the fed state pharmacokinetic parameters of atorvastatin were compared to the fasting state, Cmax decreased by 32% (GMR [90%CI], 0.68 [0.59–0.78]), whereas AUC0-t was similar (GMR [90%CI], 1.00 [0.93–1.07]) to the fasting state. The results showed that the absorption rate decreased while the total absorption amount did not change when atorvastatin was administered with food. Owing to high solubility and permeability, atorvastatin acid is completely absorbed after ingestion. However, atorvastatin acid extensively undergoes a first-pass metabolism in the gut wall and liver, with an oral bioavailability of 14%. Food decreases the rate and extent of atorvastatin absorption after oral administration.17 Based on previous findings, the effect of food does not appear to result in significant changes in the clinical effect of the drugs.
The AUCt of metformin was significantly increased by 56% (GMR [90%CI], 1.56 [1.43–1.69]) during steady state condition; however, the Cmax value (GMR [90%CI], 1.03 [0.94–1.12]) did not change when compared to the fasting state. The magnitudes of AUCinf,tmax (~2 hrs), and t1/2 (0.46 hrs) following the administration of metformin under the fed condition, were consistent with previous studies on XR formulation. A high-fat diet delayed the median tmax by 3 hrs and decreased t1/2 of metformin (substained-release) by 1.36 hrs in healthy volunteers, without changing the AUC.34 Although a previous study of metformin XR found no change in the Cmax, metformin was shown to be influenced by food, with ~ a 40% lower Cmax, 25% lower AUC, and tmax prolongation.35 Metformin is a poorly absorbed drug with a 50~60% bioavailability in the fasted state. Although the extent of metformin absorption (as measured by AUC) from the metformin XR tablet increased by approximately 50% when administered with food, there was no effect of food on Cmax and tmax of metformin.20 The results of the bioavailability study for the effect of food on FDC of atorvastatin and metformin XR were similar to the results of single administration of atorvastatin and metformin XR.
Conclusion
There is no clinically significant interaction at steady state of atorvastatin when combined with metformin XR. However, food slowed the rate of atorvastatin absorption and increased the extent of metformin absorption from an FDC of atorvastatin/metformin XR 20 mg/500 mg. These changes are consistent with those observed in the individual reference formulations for administration with food. All formulations were safe and well tolerated based on the drug-drug and food-drug pharmacokinetic study. The atorvastatin/metformin XR 20/500 mg FDC tablet is recommended to be prescribed for intake with meals, to reduce the symptoms of gastrointestinal intolerability associated with metformin.
Data sharing
- Whether the authors intend to share individual deidentified participant data? No.
- What specific data they intend to share? Not available.
- What other study-related documents will be made available? Not available.
- How the data will be accessible? Not applicable.
- When and for how long they will be made available? Not applicable.
Acknowledgments
This study was conducted with support by CJ HealthCare (Seoul, Republic of Korea), and we thank all clinical trial staff members for their contributions to this study.
Disclosure
Eun-Ji Kim and Geun Seog Song are employees of CJ HealthCare (Seoul, Republic of Korea). Eun-Ji Kim reports a patent 10-1397343-0000; Geun Seog Song reports a patent 10-1397343-0000. Jae-Gook Shin report grants from a contracted clinical trial, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Haffner SM, Lehto S, Ronnemaa T, Pyorala K, Laakso M. Mortality from coronary heart disease in subjects with type 2 diabetes and in nondiabetic subjects with and without prior myocardial infarction. N Engl J Med. 1998;339:229–234. doi:10.1056/NEJM199807233390404
2. Stevens RJ, Kothari V, Adler AI, Stratton IM. The UKPDS risk engine: a model for the risk of coronary heart disease in Type II diabetes (UKPDS 56). Clin Sci. 2001;101:671–679.
3. Buse JB, Ginsberg HN, Bakris GL, et al. Primary prevention of cardiovascular diseases in people with diabetes mellitus: a scientific statement from the American Heart Association and the American Diabetes Association. Diabetes Care. 2007;30:162–172. doi:10.2337/dc07-9917
4. International Diabetes Federation Guideline Development Group. Global guideline for type 2 diabetes. Diabetes Res Clin Pract. 2014;104:1–52. doi:10.1016/j.diabres.2012.10.001
5. Baigent C, Keech A, Kearney PM, et al. Efficacy and safety of cholesterol-lowering treatment: prospective meta-analysis of data from 90,056 participants in 14 randomised trials of statins. Lancet. 2005;366:1267–1278. doi:10.1016/S0140-6736(05)67394-1
6. Colhoun HM, Betteridge DJ, Durrington PN, et al. Primary prevention of cardiovascular disease with atorvastatin in type 2 diabetes in the Collaborative Atorvastatin Diabetes Study (CARDS): multicentre randomised placebo-controlled trial. Lancet. 2004;364:685–696. doi:10.1016/S0140-6736(04)16895-5
7. Kandhwal K, Dey S, Nazarudheen S, et al. Pharmacokinetics of a fixed-dose combination of atorvastatin and metformin extended release versus concurrent administration of individual formulations: a randomized, open-label, two-treatment, two-period, two-sequence, single-dose, crossover, bioequivalence study. Clin Drug Investig. 2011;31:853–863. doi:10.2165/11592920-000000000-00000
8. Nawrocki JW, Weiss SR, Davidson MH, et al. Reduction of LDL cholesterol by 25% to 60% in patients with primary hypercholesterolemia by atorvastatin, a new HMG-CoA reductase inhibitor. Arterioscler Thromb Vasc Biol. 1995;15:678–682.
9. Adams SP, Tsang M, Wright JM. Lipid-lowering efficacy of atorvastatin. Cochrane Database Syst Rev. 2015;(3):Cd008226.
10. Bakker-Arkema RG, Davidson MH, Goldstein RJ, et al. Efficacy and safety of a new HMG-CoA reductase inhibitor, atorvastatin, in patients with hypertriglyceridemia. JAMA. 1996;275:128–133.
11. Jacobsen W, Kuhn B, Soldner A, et al. Lactonization is the critical first step in the disposition of the 3-hydroxy-3-methylglutaryl-CoA reductase inhibitor atorvastatin. Drug Metab Dispos. 2000;28:1369–1378.
12.
13. Hardie DG. AMP-activated protein kinase as a drug target. Annu Rev Pharmacol Toxicol. 2007;47:185–210. doi:10.1146/annurev.pharmtox.47.120505.105304
14. Graham GG, Punt J, Arora M, et al. Clinical pharmacokinetics of metformin. Clin Pharmacokinet. 2011;50:81–98. doi:10.2165/11534750-000000000-00000
15. Derosa G, D’Angelo A, Romano D, Maffioli P. Effects of metformin extended release compared to immediate release formula on glycemic control and glycemic variability in patients with type 2 diabetes. Drug Des Devel Ther. 2017;11:1481–1488. doi:10.2147/DDDT.S131670
16. Pai MP, Paloucek FP. The origin of the “ideal” body weight equations. Ann Pharmacother. 2000;34:1066–1069. doi:10.1345/aph.19381
17. Lennernas H. Clinical pharmacokinetics of atorvastatin. Clin Pharmacokinet. 2003;42:1141–1160. doi:10.2165/00003088-200342130-00005
18. Mendoza L, Hajduch M, Plausinaitis R, Platilova V, Emritte N, Svoboda M. Pharmacokinetic and bioequivalence testing of atorvastatin formulations in healthy male volunteers. Pharmazie. 2006;61:805–806.
19. Najib N, Idkaidek N, Beshtawi M, et al. Bioequivalence evaluation of two brands of metformin 500 mg tablets (Dialon & Glucophage)–in healthy human volunteers. Biopharm Drug Dispos. 2002;23:301–306. doi:10.1002/bdd.326
20.
21. Wang Y, Tang Y, Gu J, Fawcett JP, Bai X. Rapid and sensitive liquid chromatography-tandem mass spectrometric method for the quantitation of metformin in human plasma. J Chromatogr B Analyt Technol Biomed Life Sci. 2004;808:215–219. doi:10.1016/j.jchromb.2004.05.006
22. He BX, Shi L, Qiu J, et al. Quantitative determination of atorvastatin and ortho-hydroxy atorvastatin in human plasma by liquid chromatography tandem mass spectrometry and pharmacokinetic evaluation. Methods Find Exp Clin Pharmacol. 2010;32:481–487. doi:10.1358/mf.2010.32.7.1487086
23.
24. Sharma P, Butters CJ, Smith V, Elsby R, Surry D. Prediction of the in vivo OATP1B1-mediated drug-drug interaction potential of an investigational drug against a range of statins. Eur J Pharm Sci. 2012;47:244–255. doi:10.1016/j.ejps.2012.04.003
25. Balasubramanian R, Varadharajan S, Kathale A, et al. Assessment of the efficacy and tolerability of a fixed dose combination of atorvastatin 10 mg + metformin SR 500 mg in diabetic dyslipidaemia in adult Indian patients. J Indian Med Assoc. 2008;106:464–467.
26. Park JE, Kim KB, Bae SK, Moon BS, Liu KH, Shin JG. Contribution of cytochrome P450 3A4 and 3A5 to the metabolism of atorvastatin. Xenobiotica. 2008;38:1240–1251. doi:10.1080/00498250802334391
27. Wu X, Whitfield LR, Stewart BH. Atorvastatin transport in the Caco-2 cell model: contributions of P-glycoprotein and the proton-monocarboxylic acid co-transporter. Pharm Res. 2000;17:209–215.
28. Chen C, Mireles RJ, Campbell SD, et al. Differential interaction of 3-hydroxy-3-methylglutaryl-coa reductase inhibitors with ABCB1, ABCC2, and OATP1B1. Drug Metab Dispos. 2005;33:537–546. doi:10.1124/dmd.104.002477
29. Tousoulis D, Koniari K, Antoniades C, et al. Combined effects of atorvastatin and metformin on glucose-induced variations of inflammatory process in patients with diabetes mellitus. Int J Cardiol. 2011;149:46–49. doi:10.1016/j.ijcard.2009.11.038
30. Matafome P, Louro T, Rodrigues L, et al. Metformin and atorvastatin combination further protect the liver in type 2 diabetes with hyperlipidaemia. Diabetes Metab Res Rev. 2011;27:54–62. doi:10.1002/dmrr.1157
31. Tousoulis D, Koniari K, Antoniades C, et al. Impact of 6 weeks of treatment with low-dose metformin and atorvastatin on glucose-induced changes of endothelial function in adults with newly diagnosed type 2 diabetes mellitus: a single-blind study. Clin Ther. 2010;32:1720–1728. doi:10.1016/j.clinthera.2010.09.007
32. Madsen A, Bozickovic O, Bjune JI, Mellgren G, Sagen JV. Metformin inhibits hepatocellular glucose, lipid and cholesterol biosynthetic pathways by transcriptionally suppressing steroid receptor coactivator 2 (SRC-2). Sci Rep. 2015;5:16430. doi:10.1038/srep16430
33. Whitfield LR, Stern RH, Sedman AJ, Abel R, Gibson DM. Effect of food on the pharmacodynamics and pharmacokinetics of atorvastatin, an inhibitor of HMG-CoA reductase. Eur J Drug Metab Pharmacokinet. 2000;25:97–101. doi:10.1007/BF03190074
34. Choi HY, Noh YH, Kim YH, et al. Effects of food on the pharmacokinetics of gemigliptin/metformin sustained-release 50/1,000 mg (25/500 mg x 2 tablets) fixeddose combination tablet in healthy male volunteers. Int J Clin Pharmacol Ther. 2014;52:381–391. doi:10.5414/CP202038
35.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.