")
Back to Journals » Clinical Interventions in Aging » Volume 15
Percutaneous Transforaminal Endoscopic Decompression for Geriatric Patients with Central Spinal Stenosis and Degenerative Lumbar Spondylolisthesis: A Novel Surgical Technique and Clinical Outcomes
Received 17 April 2020
Accepted for publication 22 June 2020
Published 21 July 2020 Volume 2020:15 Pages 1213—1219
DOI https://doi.org/10.2147/CIA.S258702
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Zhi-Ying Wu
Xiao-Kang Cheng, Bin Chen
Orthopaedic Department, Chengde Medical University Affiliated Hospital, Chengde 067000, Hebei, People’s Republic of China
Correspondence: Bin Chen
Orthopaedic Department, Chengde Medical University Affiliated Hospital, Chengde 067000, Hebei, People’s Republic of China
Tel +86 15633142760
Email [email protected]
Purpose: Percutaneous transforaminal endoscopic decompression (PTED) is an ultra-minimally invasive surgical option for patients that does not involve the same amount of destabilizing facet joint removal as a traditional laminectomy. The objective of this study was to describe the procedure of PTED under local anesthesia for geriatric patients with central spinal stenosis and degenerative lumbar spondylolisthesis (CSS-DLS).
Materials and Methods: From January 2016 to December 2018, 30 consecutive geriatric patients who underwent surgery for single-level CSS-DLS were retrospectively reviewed. All patients were followed for at least 12 months (12– 24 months). The visual analog scale (VAS) scores, Oswestry disability index (ODI) scores and modified MacNab criteria were used to evaluate the clinical results.
Results: The mean age was 73.1± 6.0 years. Follow-up ranged from 12 to 36 months. The mean±SD values of the preoperative VAS for leg pain and ODI were 7.4± 1.0 and 67.2± 8.4, respectively. The values improved to 2.2± 1.1 and 19.9± 8.1 at 12 months postoperatively. The outcomes of the modified MacNab criteria showed that 93.3% of patients obtained a good-to-excellent rate. The percent slippage of spondylolisthesis before surgery (13.8± 2.5%) and at the end of follow-up (14.0± 2.5%) was not significantly different.
Conclusion: PTED under local anesthesia could be a useful supplement to traditional decompression in geriatric patients with CSS-DLS.
Keywords: percutaneous transforaminal endoscopic decompression, degenerative lumbar spondylolisthesis, central spinal stenosis, geriatric patients
Introduction
DLS, a common spinal disorder, is used to describe slippage of an upper vertebra on the inferior vertebra with an intact neural arch. This pathologic disorder leads to CSS, mainly due to the superior endplate of the inferior vertebral body.1 Due to the compression of the cauda equina and nerve roots, patients often present with signs and symptoms consistent with neurogenic claudication and radiculopathy. The clinical effects of CSS are magnified by the presence of degenerative slippage that further narrows the central spinal canal. When conservative treatment thoroughly fails, surgical treatment is considered.2
Traditionally, decompression with instrumented fusion procedures has been performed for patients with neurogenic claudication and nerve root compression. Ghogawala et al3 concluded that among patients with DLS, the addition of fusion was associated with significant improvements in quality of life compared with decompression alone. However, Forsth et al4 concluded that the addition of fusion did not result in additional benefits for patients with DLS. The natural disease course suggests that DLS does not always lead to instability in patients who have probably reached a stabilization phase and spontaneous fusion.5
PTED, a minimally invasive technique, is preferred by patients with lumbar degenerative diseases worldwide.6 Compared with traditional decompression, PTED has many advantages: a faster recovery, less trauma, lower costs, a higher percentage of patient satisfaction, and a reduced rate of anesthesia-related morbidity.7 Most importantly, PTED can preserve the posterior ligament complex (PLC) and other biomechanical structures.8 The natural course of CSS-DLS suggests that spontaneous fusion can be achieved in geriatric patients.5 Therefore, PTED has no impact on instability and should not influence the natural course of CSS-DLS.
Some surgeons9 have achieved satisfying outcomes by using the PTED technique in patients with unilateral neurogenic claudication and radiculopathy who have lumbar spinal stenosis and low-grade DLS. However, to the best of our knowledge, no published studies have included patients with bilateral leg pain or neurogenic claudication. The objective of this study was to describe the procedure of PTED for geriatric CSS-DLS.
Materials and Methods
General Information
From January 2016 to December 2018, 30 consecutive patients underwent surgery for single-level CSS-DLS. The inclusion criteria were as follows: 1) a diagnosis of predominant low-grade DLS based on clinical symptoms, physical examination results and imaging studies; 2) failure of conservative treatment for at least three months; 3) bilateral leg symptoms (intermittent claudication, lower extremity pain, or numbness) without severe back pain; and 4) an age of 65 years or older. The exclusion criteria were as follows: 1) segmental instability on preoperative dynamic radiographs; 2) mainly back pain symptoms; 3) a history of previous lumbar surgery; and 4) pathological conditions such as tumor, trauma, or infection. The preoperative demographic characteristics, perioperative outcomes and clinical outcomes were recorded.
Surgical Procedure
The surgical procedure included three steps: 1) foraminoplasty: removal of the ligamentum flavum (LF) and the ventral elements on the superior articular process (SAP); 2) discectomy: removal of the posterior longitudinal ligament, perineural scar, and extruded lumbar disc material; and 3) resection of the superior endplate of the inferior vertebral body.
To open the patient’s disc, a soft roll was placed under the waist after the patient was placed in the lateral decubitus position on the radiolucent table. The entry point was located at the more severe symptomatic side and was 1–3 cm above the iliac crest and 8–12 cm from the midline horizontally. A total of 20 mL of 2% lidocaine combined with 30 mL of 1:200,000 epinephrine was used during the procedure. 1): The skin was infiltrated with 5 mL of mixed local anesthetic, and a 25-G needle was inserted to anaesthetize the trajectory with 15 mL, the foramen with 10–15 mL, and the articular process with 15–20 mL of mixed local anesthetic. 2): An incision was made, and sequential drills were used to resect the hypertrophy of the LF and the ventral osteophytes on the SAP (foraminoplasty). 3): The endoscope was inserted after the working cannula was placed [Figure 1]. A Maxmore percutaneous transforaminal endoscopic spine system (Maxmore spine® by Hoogland Spine Products, Germany) was used in the PTED.
 |
Figure 1 Fluoroscopic views before endoscopic manipulation. (A and B) The drill was inserted to resect the LF and the ventral osteophytes on the SAP. (C and D) The working cannula was placed. |
The remaining part of the ipsilateral LF and the ventral SAP, the extruded disc material, the posterior longitudinal ligament, and the perineural scar were resected with endoscopic forceps step by step [Figure 2]. For full ventral decompression, the critical point of PTED was to remove the superior endplate of the inferior vertebral body (L5 vertebral body) bit by bit using endoscopic forceps, a high-speed drill, or an endoscopic bone knife. After ipsilateral 270-decompression, the endoscopic abduction angle needed to be increased to perform contralateral decompression. The fully 270-degree ipsilateral decompressed traversing nerve root and 180-degree contralateral decompressed traversing nerve root could be pulsed freely with the heart rate.
 |
Figure 2 Intraoperative endoscopic views. (A and B) The superior endplate of the inferior vertebra (L5) was removed with an endoscopic bone knife. (C) Dorsal and ventral L5 nerve roots were fully decompressed. (D) The dura was torn with nucleus forceps. The white arrow represents the traversing nerve root (L5), and the black arrow represents the superior endplate of the inferior vertebra. |
After adequate hemostasis, a drainage tube was placed postoperatively and removed one day after the surgery.
Measures
The clinical results were evaluated by using the VAS and ODI preoperatively and at three months, six months and 12 months postoperatively. In addition, surgical satisfaction rates were assessed by using the modified Macnab criteria10 at the final follow-up.
Statistical Assessments
The clinical results were analyzed statistically using the SPSS 21 program (IBM, Armonk, USA). Paired t tests and one-way analysis of variance were used to compare the differences in the mean outcome scores from pre- and postoperative variables. P < 0.05 was considered statistically significant.
Results
Preoperative Demographic Characteristics and Outcomes
The preoperative demographic characteristics and outcomes are shown in Table 1. The average follow-up period was at least 12 months (12–36 months). A total of 8 men and 22 women were involved in this study. The average age was 73.1 years (65–89 years). The average duration of symptoms was 44.1 months (6–240 months). The most common comorbidity was cardiovascular problems (50.0%), such as hypertensive disorders (Table 2), followed by endocrinology diseases (16.7%). There were only 5 patients without comorbidities. Radiologic evaluation showed that spondylolisthesis was located at L4-5 in all patients. The mean operation time was 72.0 minutes (50–100 minutes), the amount of blood loss was 13.7 mL (10–25 mL), and the drainage volume was 31.1 mL (0–180 mL). The average hospital stay was 5.0 days (3–8 days).
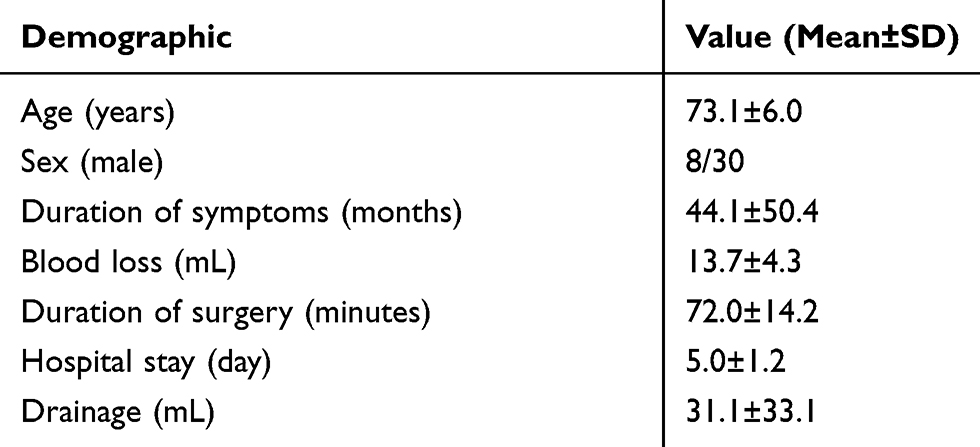 |
Table 1 Demographics of the Included Patients |
 |
Table 2 Comorbidities |
Clinical Results
Significant improvements in clinical results from preoperation to three months, six months, twelve months and the final follow-up after the operation were quantified using the VAS-leg pain score, ODI score and the modified MacNab criteria (Figure 3). The mean preoperative ODI and VAS-leg pain scores were 67.2±8.4 and 7.4±1.0, respectively; all mean scores improved postoperatively to 19.9±8.1 and 2.2±1.1 after 12 months, respectively. The patients’ estimated walking distance improved from 150.3±95.2 to 1355.0±631.7 m. The good-to-excellent rate in patients was 93.3%. One patient had fair results. One reported a poor outcome. The average percent slippage of spondylolisthesis was 13.8±2.5% before surgery and 14.0±2.5% at the final follow-up. There were no statistically significant differences between them (P > 0.05).
 |
Figure 3 Clinical outcomes before and after PTED at different follow-up time points. (A) The VAS-leg pain scores. (B) ODI before and after PTED. (C) Outcome of the modified MacNab criteria. |
Complications
One patient had a dural tear and cerebrospinal fluid leakage, which was not repaired at the time of surgery, and no permanent neurological sequelae were indicated during the follow-up period. There were no reports of infection, thrombophlebitis, cauda equina syndrome, or vascular injury.
Discussion
The goal of this retrospective research was to introduce a new PTED method for CSS-DLS. Although most of our patients experienced symptom relief, complications still occurred. The reasons for these complications might shed light on future improvements in this technique. The preliminary results demonstrated that PTED was a feasible and safe way to treat CSS-DLS.
CSS-DLS has specific pathologic features. CSS results from dorsal compression of the hypertrophic SAP and LF, ventral compression of posterior disc protrusion, the posterior longitudinal ligament and, particularly, the superior endplate of the inferior vertebra.11 The clinical effects of CSS are magnified by the presence of degenerative slippage that further narrows the central spinal canal. Lower extremity pain with or without claudication typically results from compression of the cauda equina and traversing nerve roots. Most experts believe that three to six months of nonsurgical treatment failure is an indication for spinal decompression surgery.12 Conventional decompression surgery, such as TLIF or PLIF, has been considered the gold-standard procedure for CSS-DLS due to the wide decompression of the cauda equina and nerve roots and the correction of the deformity. Karsy and Bisson13 concluded that, compared with medical management alone, surgical treatment showed a better incremental cost-effectiveness ratio in selected patients. Some experts8 considered that by releasing operational capacity, decompression alone could save medical resources as a result of the shorter hospitalization. However, other experts thought that simple decompression would cause the risk of reoperation due to iatrogenic destabilization, which is the consequence of removing the osseo musculotendinous complex and other posterior bony elements.14
Although decompression combined with fusion may decrease the risks caused by decompression alone, it has also been shown that instrument implantation increases the risk of adjacent segment disease and hardware-related complications.15 In addition, it is crucial to reconsider the necessity for instrumented fusion in geriatric patients who have comorbidities. In addition, cost-effectiveness studies indicate that decompression alone is less expensive than additional fusion.16
Microendoscopic decompression (MED), as a standard, minimally invasive spinal technique, can be used to treat CSS-DLS. Similar to traditional laminectomy, spinal canal expansion mainly depends on dorsal decompression.17,18 Although MED may be possible with epidural anesthesia, most surgeons conduct MED under general anesthesia in reality. In addition, posterior elements must be severely removed, which increases the risk of dural sac injury and iatrogenic instability and may lead to reoperation.
PTED is more minimally invasive than MED for geriatric patients with degenerative spinal disease.19 For complete decompression, the ventral osteophytes of the SAP and hypertrophic LF are removed (foraminoplasty), and the posterior longitudinal ligament, degenerated intervertebral disc, and peripheral scars of nerves should also be removed with endoscopic forceps. Most importantly, the superior endplate of the inferior vertebral body (L5) compressing the traversing nerve roots and cauda equina must be resected carefully. After that, the central spinal canal and lateral recess can be enlarged [Figure 4].
 |
Figure 4 Pre- and postoperative CT and MRI. (A and B) The superior endplate of the inferior vertebra (arrow) before surgery. (C and D) Central spinal canal stenosis (circle). (E and F) The protruding vertebral bone was removed (arrow), and this procedure led to restoration of the original spinal canal shape. (G and H) The central spinal canal (circle) was enlarged. The superior endplate of the inferior vertebra was indicated by arrow. The central spinal canal stenosis and the enlarged central spinal canal was indicated by circle. |
There was no significant progression of slippage in our study. This means that PTED did not influence the natural course of CSS-DLS, and restabilization occurred. Ventral decompression of the traversing nerve roots and cauda equina can lead to restoration of the central spinal canal and lateral recess morphology. In addition, ventral bone resection can avoid excessive dorsal resection of the osseo musculotendinous complex and other posterior bony elements. Therefore, this dorsal decompression only of the LF and SPA did not cause significant iatrogenic instability.
One patient had a dural tear and cerebrospinal fluid leakage in this study because the nucleus forceps accidentally tore the dura mater, resulting from an unclear operative view.20 To prevent intraoperative bleeding and provide a clear operative view, the bone should be lifted carefully, and strict bleeding control is needed. Epinephrine mixed with local anesthetic during the operation, combined with adequate irrigation pressure and radiofrequency coagulation, can provide a clear operative field. Finally, significant enlargement of the central spinal canal is achieved by dorsal and ventral decompression.
Awake geriatric patients represent a highly desirable patient population for surgeons. 1): For geriatric patients with severe comorbidities and contraindications to general anesthesia, the PTED procedure under local anesthesia may be the best option. 2): Local anesthesia can provide feedback from patients when stimulating the nerve root.
With the development of improvements in surgical devices and anesthesiology, the majority of geriatric patients can withstand minimally invasive TLIF and expect satisfactory improvement.21 Therefore, we believe that the procedure should be determined jointly by the patient and the expert. To some extent, PTED is just an effective supplement to traditional decompression.
Limitations
The study has some limitations: 1): Although PTED shows good short-term results, it still requires long-term follow-up. 2): Due to the strict inclusion criteria in our study, the sample size was relatively small. 3): The cross-sectional area of the lateral recess was not measured, as we attributed the relief of leg symptoms to the enlargement of the spinal canal.
Conclusion
As the elderly demographic increases in number and gets older, spine physicians need to consider treatment paradigms that factor in risk, patient downtime, and health care costs and that are specifically tailored to this older population. The operation has no anesthesia complications and does not damage the paravertebral muscles of the lumbar spine or the stability of the lumbar spine, and the short-term effect is acceptable. We believe that this procedure may be used as an alternative therapeutic option for CSS-DLS.
Abbreviations
PTED, percutaneous transforaminal endoscopic decompression; DLS, degenerative lumbar spondylolisthesis; CSS, central spinal stenosis; VAS, visual analog scale; ODI, Oswestry disability index; CT, computed tomography; MRI, magnetic resonance imaging.
Data Sharing Statement
The data used to support the findings of this study are available from the corresponding author upon request.
Ethics Approval and Informed Consent
This retrospective study was approved by the Ethics Committee of the Chengde Medical University Affiliated Hospital, and written informed consent was obtained from participants prior to data collection. This study was conducted in accordance with the Declaration of Helsinki.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Kirkaldy-Willis WH, Wedge JH, Yong-Hing K. Pathology and pathogenesis of lumbar spondylosis and stenosis. Spine (Phila). 2019;3:319–328. doi:10.1097/00007632-197812000-00004
2. Montano N, Stifano V, Papacci F, et al. Minimally invasive decompression in patients with degenerative spondylolisthesis associated with lumbar spinal stenosis. Report of a surgical series and review of the literature. Neurol Neurochir Pol. 2018;52:448–458. doi:10.1016/j.pjnns.2018.06.004
3. Ghogawala Z, Dziura J, Butler WE, et al. Laminectomy plus fusion versus laminectomy alone for lumbar spondylolisthesis. N Engl J Med. 2016;374:1424–1434. doi:10.1056/NEJMoa1508788
4. Forsth P, Olafsson G, Carlsson T, et al. A randomized, controlled trial of fusion surgery for lumbar spinal stenosis. N Engl J Med. 2016;374:1413–1423. doi:10.1056/NEJMoa1513721
5. Hasegawa K, Kitahara K, Shimoda H, et al. Lumbar degenerative spondylolisthesis is not always unstable: clinicobiomechanical evidence. Spine. 2014;39:2127–2135. doi:10.1097/BRS.0000000000000621
6. Xiong C, Li T, Kang H, et al. Early outcomes of 270-degree spinal canal decompression by using TESSYS-ISEE technique in patients with lumbar spinal stenosis combined with disk herniation. Eur Spine J. 2019;28:78–86. doi:10.1007/s00586-018-5655-4
7. Zhu Y, Zhao Y, Fan G, et al. Comparison of 3 anaesthetic methods for percutaneous transforaminal endoscopic discectomy: a prospective study. Pain Physician. 2019;21:E347–E353.
8. Shin SH, Bae JS, Lee SH, et al. Transforaminal endoscopic decompression for lumbar spinal stenosis: a novel surgical technique and clinical outcomes. World Neurosurg. 2018;114:e873–e882. doi:10.1016/j.wneu.2018.03.107
9. Li XF, Jin LY, Lv ZD, et al. Endoscopic ventral decompression for spinal stenosis with degenerative spondylolisthesis by partially removing posterosuperior margin underneath the slipping vertebral body: technical note and outcome evaluation. World Neurosurg. 2019;126:e517–e525. doi:10.1016/j.wneu.2019.02.083
10. Macnab I. Negative disc exploration: an analysis of the causes of nerve-root involvement in sixty-eight patients. JBJS. 1971;53:891–903. doi:10.2106/00004623-197153050-00004
11. Rampersaud YR, Fisher C, Yee A, et al. Health-related quality of life following decompression compared to decompression and fusion for degenerative lumbar spondylolisthesis: a Canadian multicentre study. Can J Surg. 2014;57:E126–E133. doi:10.1503/cjs.032213
12. Matz Paul G, Meagher RJ, Lamer T, et al. Guideline summary review: an evidence-based clinical guideline for the diagnosis and treatment of degenerative lumbar spondylolisthesis. Spine J. 2014;16:439–448. doi:10.1016/j.spinee.2015.11.055
13. Karsy M, Bisson EF. Surgical Versus Nonsurgical Treatment of Lumbar Spondylolisthesis. Neurosurg Clin N Am. 2019;30(3):333–340. doi:10.1016/j.nec.2019.02.007
14. Urakawa H, Jones T, Samuel A, et al. The necessity and risk factors of subsequent fusion after decompression alone for lumbar spinal stenosis with lumbar spondylolisthesis: 5 years follow-up in 2 different large populations [published online ahead of print, 2020 May 14]. Spine J. 2020.
15. Deyo RA, Mirza SK, Martin BI, et al. Trends, major medical complications, and charges associated with surgery for lumbar spinal stenosis in older adults. J Am Med Assoc. 2010;303:1259–1265. doi:10.1001/jama.2010.338
16. Vorhies JS, Hernandez-Boussard T, Alamin T. Treatment of degenerative lumbar spondylolisthesis with fusion or decompression alone results in similar rates of reoperation at 5 years. Clin Spine Surg. 2018;1:E74–E79. doi:10.1097/BSD.0000000000000564
17. Minamide A, Simpson AK, Okada M. Microendoscopic decompression for lumbar spinal stenosis with degenerative spondylolisthesis: the influence of spondylolisthesis stage (Disc Height and Static and Dynamic Translation) on Clinical Outcomes. Clin Spine Surg. 2019;32:E20–E26. doi:10.1097/BSD.0000000000000710
18. Youn MS, Shin JK, Goh TS, et al. Endoscopic posterior decompression under local anaesthesia for degenerative lumbar spinal stenosis. J Neurosurg Spine. 2018;29:661–666. doi:10.3171/2018.5.SPINE171337
19. Hasan S, McGrath LB, Sen RD, et al. Comparison of full-endoscopic and minimally invasive decompression for lumbar spinal stenosis in the setting of degenerative scoliosis and spondylolisthesis. Neurosurg Focus. 2019;46(5):E16. doi:10.3171/2019.2.FOCUS195
20. Lv Z, Jin L, Wang K, et al. Comparison of effects of PELD and fenestration in the treatment of geriatric lumbar lateral recess stenosis. Clin Interv Aging. 2019;14:2187–2194. doi:10.2147/CIA.S226295
21. Chan AK, Bisson EF, Bydon M, et al. A comparison of minimally invasive and open transforaminal lumbar interbody fusion for grade 1 degenerative lumbar spondylolisthesis: an analysis of the prospective quality outcomes database [published online ahead of print, 2020 May 14]. Neurosurgery. 2020;nyaa097.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.