")
Back to Journals » Clinical Interventions in Aging » Volume 11
Patterns of scheduled follow-up appointments following hospitalization for heart failure: insights from an urban medical center in the United States
Authors Goyal P, Sterling M, Beecy A, Ruffino J, Mehta S, Jones E, Lachs M, Horn E
Received 24 May 2016
Accepted for publication 6 July 2016
Published 26 September 2016 Volume 2016:11 Pages 1325—1332
DOI https://doi.org/10.2147/CIA.S113442
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Richard Walker
Parag Goyal,1 Madeline R Sterling,2 Ashley N Beecy,2 John T Ruffino,2 Sonal S Mehta,3 Erica C Jones,1 Mark S Lachs,3 Evelyn M Horn1
1Division of Cardiology, Department of Medicine, 2Department of Medicine, 3Division of Geriatrics, Department of Medicine, Weill Cornell Medicine, New York, NY, USA
Objectives: Although postdischarge outpatient follow-up appointments after a hospitalization for heart failure represent a potentially effective strategy to prevent heart failure readmissions, patterns of scheduled follow-up appointments upon discharge are poorly described. We aimed to characterize real-world patterns of scheduled follow-up appointments among adult patients with heart failure upon hospital discharge.
Patients and methods: This was a retrospective cohort study performed at a large urban academic center in the United States among adults hospitalized with a principal diagnosis of congestive heart failure between January 1, 2013, and December 31, 2014. Patient demographics, administrative data, clinical parameters, echocardiographic indices, and scheduled postdischarge outpatient follow-up appointments were collected.
Results: Of the 796 patients hospitalized for heart failure, just over half of the cohort had a scheduled follow-up appointment upon discharge. Follow-up appointments were less likely among patients who were white and had heart failure with preserved ejection fraction and more likely among patients with Medicaid and chronic obstructive pulmonary disease. In an adjusted multivariable regression model, age ≥65 years was inversely associated with a scheduled follow-up appointment upon hospital discharge, despite higher rates of several cardiovascular and noncardiovascular comorbidities.
Conclusion: Just half of the patients discharged home following a hospitalization for heart failure had a follow-up appointment scheduled, representing a missed opportunity to provide a recommended care transition intervention. Despite a greater burden of both cardiovascular and noncardiovascular comorbidities, older adults (age ≥65 years) were less likely to have a follow-up appointment scheduled upon discharge compared with younger adults, revealing a disparity that warrants further investigation.
Keywords: appointments, patient readmission, ageism, heart failure
Introduction
Heart failure affects about 6 million people in the United States and costs >30 billion dollars per year.1 Given its heavy burden on the health care system, there is increased focus on improving the quality and efficiency of health care delivery for this patient population. Readmission rates, namely at 30 days, have become an important measure of health care quality. In addition to contributing to patient morbidity and mortality, 30-day readmissions are now closely tied to reimbursement.2 Although imperfect as a single metric of quality, readmission rates reflect care provided both during hospitalization and after discharge and have led to increased emphasis on improving transitions of care.
Although interventions aimed at reducing readmission rates for heart failure patients have produced mixed results, outpatient follow-up is generally agreed upon as an important element of any transitional program3,4 and is supported by the American Heart Association and the American College of Cardiology.5 Among hospital-based strategies, Bradley et al6 demonstrated scheduled follow-up appointments upon discharge to be associated with reduced risk-standardized 30-day readmission rates. Despite their important impact on readmission, real-world patterns of scheduled follow-up appointments upon discharge are not well described.
This study sought to characterize patterns of scheduled follow-up appointments for adult patients with heart failure upon hospital discharge, as identifying and subsequently targeting deficiencies related to scheduling follow-up appointments may offer a cost-effective strategy to curb readmission rates.
Patients and methods
Population
This retrospective cohort included consecutive patients admitted with a principal diagnosis of congestive heart failure who were subsequently discharged home from the Medicine service at an 850-bed urban academic tertiary medical center in New York City, New York (USA), between January 1, 2013, and December 31, 2014. A principal diagnosis of congestive heart failure was identified based on the presence of any of the following International Classification of Diseases, ninth revision, Clinical Modification codes,7 as used by the Centers for Medicare & Medicaid Services for publicly reporting heart failure quality measures: 402.01, 402.11, 402.91, 404.01, 404.03, 404.11, 404.13, 404.91, 404.93, or 428.xx.
Patients discharged to another hospital, skilled nursing facility, and short or intermediate care facility were excluded. Patients discharged with hospice care were also excluded. This study was approved by the Weill Cornell Institutional Review Board (Protocol #1404014979R001). The Weill Cornell Institutional Review Board deemed informed consent unnecessary, given the retrospective nature of the study.
Data collection
Patient demographic and administrative data were acquired through an automated query of the electronic health record. Clinical parameters including heart failure characteristics and patient comorbidity were collected at the time of discharge by manual chart review. Structural and functional cardiac indices were collected from echocardiograms performed as close to the discharge date as possible, up to 6 months prior. Heart failure with preserved ejection fraction (HFpEF) was defined based on guideline criteria,5 a left ventricular ejection fraction ≥50% on echocardiography. Scheduled postdischarge outpatient follow-up appointments were defined as any appointment with a specified date and time after discharge and were identified by reviewing the discharge summary from the electronic health record, which contains a specified section for scheduled follow-up appointments. Follow-up appointments were classified based on specialty. Appointments with physician extenders including nurse practitioners and physician assistants were included based on the specialty of the supervising physician. If a follow-up appointment was scheduled with both a cardiologist and noncardiology physician, both were included in the analysis. At this medical center, inpatient medical providers and/or administrative staff must call the offices of the requested outpatient providers in order to schedule follow-up appointments.
Statistical methods
The primary outcome of interest was the presence of a scheduled follow-up appointment upon discharge. Descriptive statistics were performed, stratified by follow-up appointment, age, and payer status. Associations were tested for statistical significance using the Pearson χ2 statistic for dichotomous variables and the Student’s t-test for continuous variables with confidence intervals set to 95%. We used multivariable logistic regression to identify factors associated with a scheduled follow-up appointment, adjusting for demographic variables as well as comorbidities found to have statistical significance in bivariate analysis. All calculations were performed using IBM SPSS Statistics Version 20 (IBM Corporation, Armonk, NY, USA).
Results
Scheduled follow-up appointments
A total 796 unique patients with a mean age of 70±15 years were hospitalized with a principal diagnosis of heart failure. Patients had a scheduled follow-up appointment in 56% of cases, including 45% with a cardiologist and 31% with a noncardiology physician. Among the patients, 30% had a scheduled follow-up appointment within 7 days of discharge and 44% had a scheduled appointment within 14 days. The underlying reasons for why patients did not have a scheduled follow-up appointment were not known.
As shown in Table 1, patients who did not have a scheduled follow-up appointment were older, more commonly white, and less likely to have Medicaid compared with those with a scheduled follow-up appointment. Patients without a scheduled follow-up appointment had a slightly higher left ventricular ejection fraction and higher rates of HFpEF compared to those with a scheduled follow-up appointment. New York Heart Association classification and frequency of right ventricular dysfunction and severe valvular disease were similar between groups. Regarding cardiovascular comorbidities, prevalence of coronary artery disease, atrial fibrillation/flutter, hypertension, diabetes, cerebrovascular accident, and peripheral vascular disease were similar between groups. Among noncardiovascular comorbidities, chronic obstructive pulmonary disease occurred more commonly among patients with a scheduled follow-up appointment. Prevalence of other noncardiovascular comorbidities, including gastrointestinal bleeding, liver disease, cancer, and major psychiatric disorders, were comparable between groups.
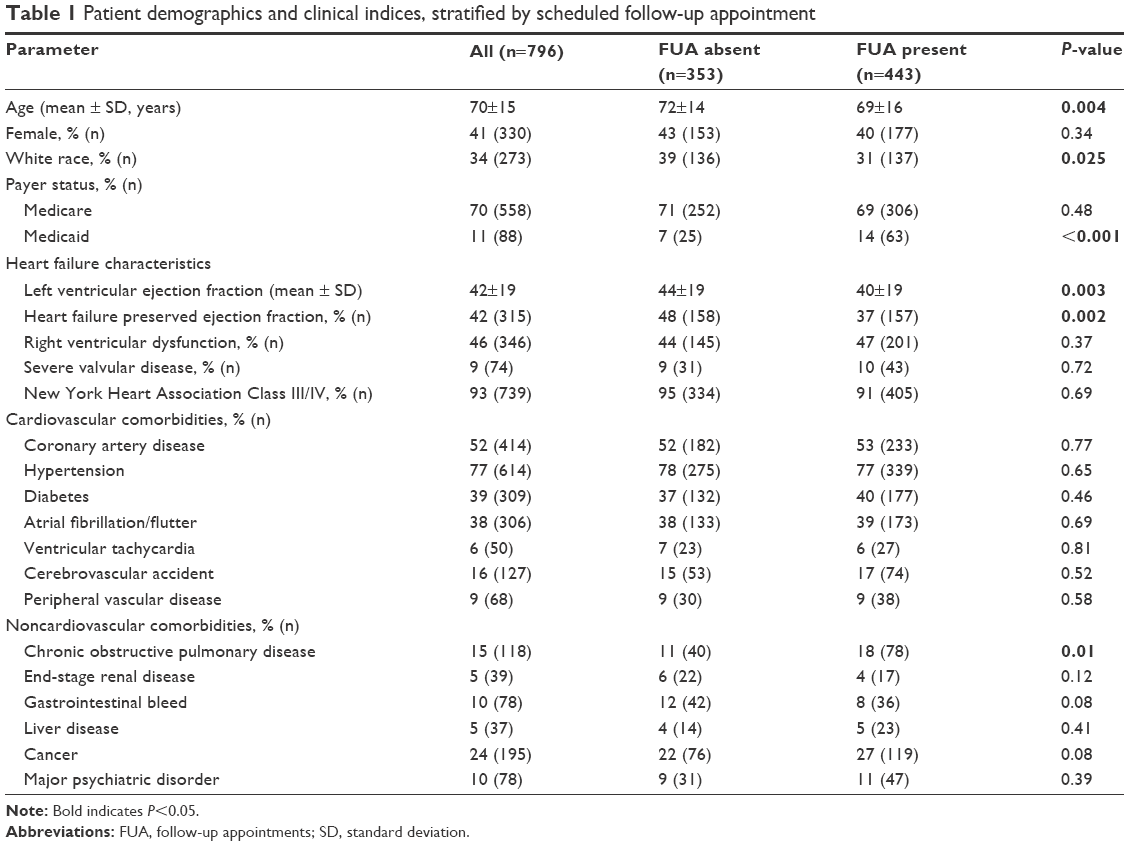 | Table 1 Patient demographics and clinical indices, stratified by scheduled follow-up appointment |
Scheduled follow-up appointments among older adults
Of the patient cohort, 68% (n=540) represented older adults, aged 65 years and older. Older adults had a scheduled follow-up appointment upon discharge less frequently than younger adults. They were less likely to be scheduled to see a cardiologist or a noncardiology physician compared with younger adults (Table 2). Noncardiology physicians predominantly included primary care physicians (67%) and medicine subspecialties (27%). Rates of scheduled follow-up appointments within 7 days and within 14 days of discharge did not differ between age groups.
 | Table 2 Rates of scheduled follow-up appointments |
Table 3 demonstrates patient characteristics stratified by age. Older adults were more commonly white and more likely to have Medicare. Regarding their heart failure, older adults had a higher left ventricular ejection fraction, with higher rates of HFpEF, compared with younger adults. Patient groups were similar with respect to New York Heart Association classification, right ventricular dysfunction, and severe valvular disease.
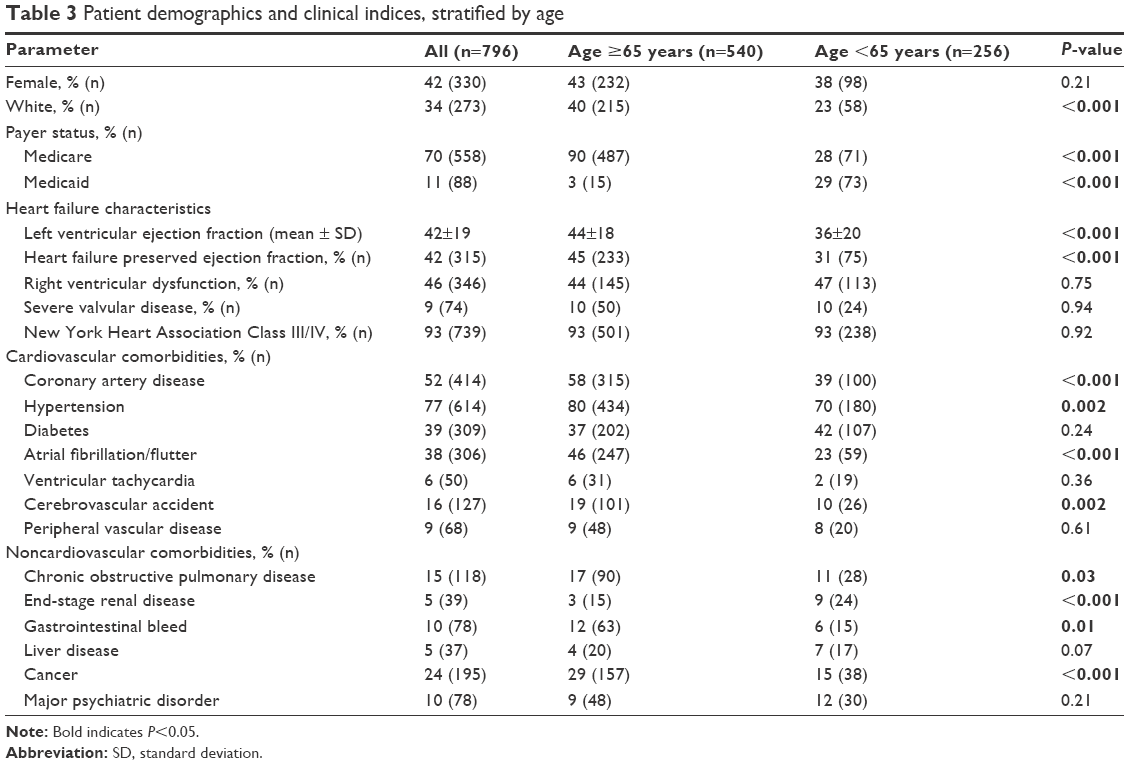 | Table 3 Patient demographics and clinical indices, stratified by age |
Among cardiovascular comorbidities, coronary artery disease, atrial fibrillation/flutter, hypertension, and cerebrovascular accident occurred more frequently among older adults compared with younger adults. Diabetes, peripheral vascular disease, and ventricular tachycardia occurred with similar frequency between groups. Older adults also had higher rates of noncardiovascular comorbidities including chronic obstructive pulmonary disease, gastrointestinal bleeding, and cancer. Rates of liver disease and major psychiatric disorders were comparable between groups.
Stratification by payer status (Table 4) revealed the characteristics of patients with Medicare (mean age 76±12 years) to parallel the characteristics of older adults – those with Medicare were more commonly white, more frequently had HFpEF, and had a higher burden of comorbidities, including coronary artery disease, hypertension, atrial fibrillation/flutter, cerebrovascular accident, cancer, and gastrointestinal bleeding.
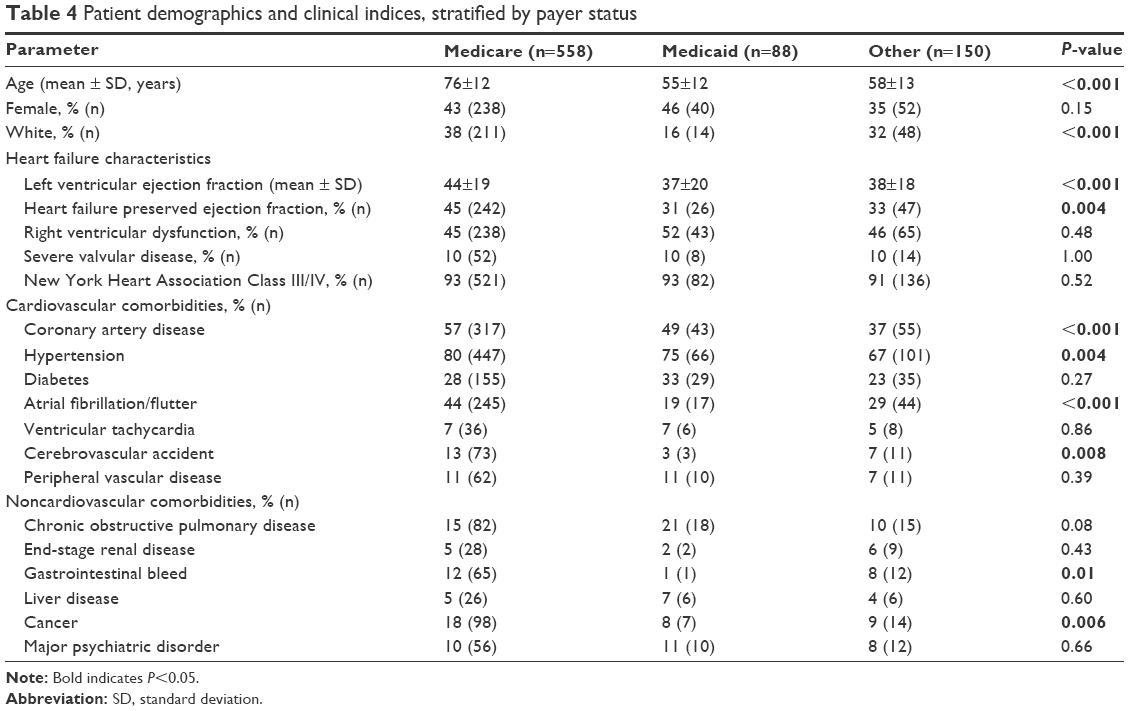 | Table 4 Patient demographics and clinical indices, stratified by payer status |
Multivariable regression analysis
In the multivariable regression analysis, age ≥65 years was inversely associated with having a scheduled follow-up appointment upon hospital discharge, after adjusting for sex, race, payer status, HFpEF, and chronic obstructive pulmonary disease (Table 5). In this adjusted model, patients with HFpEF were also less likely to have follow-up appointments compared with those with heart failure with reduced ejection fraction (HFrEF). On the other hand, this model revealed that patients with concurrent chronic obstructive pulmonary disease were more likely to have a follow-up appointment upon discharge compared with those without chronic obstructive pulmonary disease.
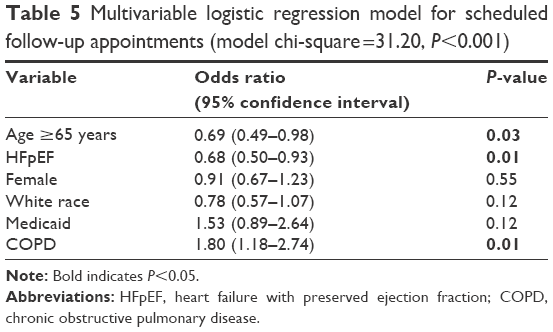 | Table 5 Multivariable logistic regression model for scheduled follow-up appointments (model chi-square =31.20, P<0.001) |
Discussion
There are several important findings in this study. First, despite guideline recommendations, only half of the cohort was scheduled for any follow-up appointments upon discharge. Second, comorbidities were common among patients admitted with heart failure, but most were not associated with higher rates of scheduled follow-up appointments. Third, patients with HFpEF were less likely to have scheduled follow-up appointments compared with those with HFrEF. Finally, despite a greater burden of both cardiovascular and noncardiovascular comorbidities, patients ≥65 years old were less likely to have a follow-up appointment scheduled upon discharge compared with younger adults after controlling for other factors.
Postdischarge office follow-up has been identified as a key element of care transitions.3 It has frequently been incorporated into transitional care model interventions aimed at improving postdischarge outcomes, such as readmission and mortality, and is supported by the American Heart Association and American College of Cardiology.5 Consistent with a rate of 61% observed in a previous study,8 this cohort demonstrated a scheduled follow-up appointment rate of just >50%. Similar to a recently published study by Baker et al,9 this included just 30% with a follow-up appointment within 7 days of discharge, the optimal time interval recommended by the American College of Cardiology’s Hospital to Home program.10 These statistics occurred within health systems where the importance of follow-up appointments is emphasized, thus highlighting an important area for improvement and suggesting the need to identify barriers to scheduling follow-up appointments. At present, reasons for inadequate follow-up rates are not well understood. Investigating factors such as provider availability and prioritization of hospitalized patients for follow-up appointments in particular may be informative and potentially reveal opportunities for improvement.
Comorbidity is an important factor associated with hospital readmissions, preventable hospitalizations, and mortality11,12 in patients with heart failure. Previous literature demonstrates that older adults have higher rates of comorbidity compared with their younger counterparts.13 In this cohort, several cardiovascular and noncardiovascular comorbidities were more common among older adults compared with younger adults, including coronary artery disease, atrial fibrillation/flutter, hypertension, cerebrovascular accident, cancer, chronic obstructive pulmonary disease, and gastrointestinal bleeding. Interestingly, despite the fact that many of these conditions are independently associated with a worse prognosis in heart failure,14–17 only patients with chronic obstructive pulmonary disease were more likely to have a scheduled follow-up appointment upon discharge. These findings suggest that, while consideration of comorbid conditions is increasingly being recognized as an important priority in heart failure management,18,19 there is ongoing need for care transition strategies to better incorporate this concept into real-time discharge planning.
HFpEF represents an important subtype of heart failure, with a prevalence comparable to that of HFrEF.20 Consistent with these findings, HFpEF was common in our study, comprising 42% of the cohort. The majority of patients with HFpEF were ≥65 years old, paralleling other studies20–22 that have characterized HFpEF as a geriatric syndrome.23 HFpEF patients perform particularly poorly following hospitalization for heart failure, illustrated by outcomes from the OPTIMIZE registry where one third of patients hospitalized with HFpEF were either rehospitalized or dead within 3 months of discharge.21 Comparing HFpEF and HFrEF in >40,000 Medicare recipients, Cheng et al24 found similar adjusted mortality rates and a higher all-cause readmission rate among patients with HFpEF, demonstrating poor outcomes among heart failure patients irrespective of ejection fraction. Despite these findings, our study revealed that patients with HFpEF were less likely to have a scheduled follow-up appointment upon discharge. An antiquated view among care providers that HFpEF represents a benign subtype of heart failure given the preservation of ejection fraction may contribute to this finding.
Surprisingly, our study also demonstrated that patients aged 65 years and older were less likely to have a follow-up appointment scheduled, despite a higher burden of cardiovascular and noncardiovascular comorbidities compared with younger patients. This remained after controlling for comorbidities and HFpEF. Postdischarge follow-up for older adults is particularly important given that age is a well-documented risk factor for hospital readmission.25,26 Older adults contend with unique age-related issues including multimorbidity27,28 and polypharmacy,29 frailty,30,31 and cognitive impairment32 that may increase vulnerability to worse outcomes following hospital discharge. Additionally, posthospital syndrome has been described as a transient condition of increased susceptibility to adverse health events related to exposure to stress during hospitalization33 and is particularly relevant for the elderly.34 Altfeld et al35 demonstrated that most geriatric patients experienced problems within the first 2 days of discharge, including almost half of whom had difficulty understanding and complying with self-care needs and one-third of whom struggled to cope with change. Postdischarge follow-up has the potential to alter this course. Follow-up appointments offer the medical provider with an opportunity to elicit and manage symptomatology related to suboptimally treated disease, gaps in knowledge that may contribute to poor self-efficacy, and nonadherence to medications and/or diet. They also provide allotted time for patients and/or caregivers to ask questions and voice concerns to their physicians in person, facilitating improved communication and strengthened physician–patient interrelationships. Finally, they create a setting in which medication reconciliation can occur, as errors and discrepancies in discharge medications are common.36,37 Indeed, follow-up appointments represent an important pillar in care transitions, bridging acute inpatient care of volume overload to outpatient disease management of chronic heart failure. Although other modalities beyond follow-up appointments can provide critical postdischarge contact with medical providers, neither postdischarge nursing telephone calls nor telemedicine capabilities were used at our institution during the study period. Thus, our finding that older adults had lower rates of scheduled follow-up appointments upon discharge is concerning.
Treatment of patients based on their age can result from implicit thoughts and behaviors that occur even without conscious awareness or control.38 Previous studies examining differences in medical care provided to older adults compared with the general population have found physicians to be less engaged, less supportive,39 and less likely to offer potentially life-saving treatment.40 Among ~58,000 patients admitted with heart failure, Forman et al41 demonstrated that older adults were less likely to receive counseling or follow-up. Whether age-related provider bias is a significant contributor to lower rates of scheduled follow-up appointments is unclear and warrants further investigation.
Our study has some limitations. First, our cohort originated from a single institution, albeit a large academic center located in a diverse urban area. Variations in age, race, and payer status revealed a heterogeneous cohort, offering generalizability to a wide range of patients. Investigation of local patterns and trends facilitated a patient-level examination of potential barriers to widespread implementation of an evidence-based intervention – early postdischarge follow-up. Second, we could not account for follow-up appointments scheduled by the patient after discharge or the rate at which they were actually seen by a provider, as these data were not available. It is plausible that patients not scheduled for a follow-up appointment upon discharge either preferred or were encouraged to schedule a follow-up appointment after they returned home. However, in light of challenges older adults face following hospitalization, incorporating appointments scheduled by the patient following discharge would likely have widened the difference observed between older and younger adults. Third, some scheduled appointments may not have been adequately documented, potentially leading to an underreporting of scheduled appointments. This likely represented a minority of cases, as the study was conducted at an institution where documentation of a follow-up appointment in the specified section of the discharge summary is required, if scheduled. Furthermore, it is unlikely that underreporting would have affected age groups differently and, therefore, would not have changed results in a significant manner.
Conclusion
Only half of the patients discharged home following a hospitalization for heart failure had a follow-up appointment scheduled, representing a missed opportunity to provide a recommended care transition intervention. Scheduled follow-up appointments were less common among patients aged ≥65 years, a particularly vulnerable population whose outcomes might be improved by identifying sources of this disparity.
Disclosure
The authors report no conflicts of interest in this work.
References
Mozaffarian D, Benjamin EJ, Go AS, et al. Heart disease and stroke statistics – 2015 update: a report from the American Heart Association. Circulation. 2015;131(4):e29–e322. | ||
Center for Medicare and Medicaid [webpage on the Internet]. Readmission Reduction Program. Available from: www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/AcuteInpatientPPS/Readmissions-Reduction-Program.html. Accessed August 27, 2015. | ||
Albert NM, Barnason S, Deswal A, et al; American Heart Association Complex Cardiovascular Patient and Family Care Committee of the Council on Cardiovascular and Stroke Nursing, Council on Clinical Cardiology, and Council on Quality of Care and Outcomes Research. Transitions of care in heart failure: a scientific statement from the American Heart Association. Circ Heart Fail. 2015;8(2):384–409. | ||
Coleman EA, Williams MV. Executing high-quality care transitions: a call to do it right. J Hosp Med. 2007;2(5):287–290. | ||
Yancy CW, Jessup M, Bozkurt B, et al. 2013 ACCF/AHA guideline for the management of heart failure: executive summary: a report of the American College of Cardiology Foundation/American Heart Association Task Force on practice guidelines. Circulation. 2013;128(16):1810–1852. | ||
Bradley EH, Curry L, Horwitz LI, et al. Hospital strategies associated with 30-day readmission rates for patients with heart failure. Circ Cardiovasc Qual Outcomes. 2013;6(4):444–450. | ||
National Center for Health Statistics [webpage on the Internet]. International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM). Available from: http://www.cdc.gov/nchs/icd/icd9cm.htm. Accessed July 1, 2015. | ||
Grafft CA, McDonald FS, Ruud KL, Liesinger JT, Johnson MG, Naessens JM. Effect of hospital follow-up appointment on clinical event outcomes and mortality. Arch Intern Med. 2010;170(11):955–960. | ||
Baker H, Oliver-McNeil S, Deng L, Hummel SL. Regional hospital collaboration and outcomes in Medicare heart failure patients: see you in 7. JACC Heart Fail. 2015;3(10):765–773. | ||
American College of Cardiology [webpage on the Internet]. Hospital to Home. Available from: http://cvquality.acc.org/Initiatives/H2H.aspx. Accessed November 27, 2015. | ||
Muzzarelli S, Leibundgut G, Maeder MT, et al; TIME-CHF Investigators. Predictors of early readmission or death in elderly patients with heart failure. Am Heart J. 2010;160(2):308–314. | ||
Braunstein JB, Anderson GF, Gerstenblith G, et al. Noncardiac comorbidity increases preventable hospitalizations and mortality among Medicare beneficiaries with chronic heart failure. J Am Coll Cardiol. 2003;42(7):1226–1233. | ||
Hoffman C, Rice D, Sung HY. Persons with chronic conditions. Their prevalence and costs. JAMA. 1996;276(18):1473–1479. | ||
Levy WC, Mozaffarian D, Linker DT, et al. The Seattle Heart Failure Model: prediction of survival in heart failure. Circulation. 2006;113(11):1424–1433. | ||
Mamas MA, Caldwell JC, Chacko S, Garratt CJ, Fath-Ordoubadi F, Neyses L. A meta-analysis of the prognostic significance of atrial fibrillation in chronic heart failure. Eur J Heart Fail. 2009;11(7):676–683. | ||
Hasin T, Gerber Y, McNallan SM, et al. Patients with heart failure have an increased risk of incident cancer. J Am Coll Cardiol. 2013;62(10):881–886. | ||
Mentz RJ, Schulte PJ, Fleg JL, et al. Clinical characteristics, response to exercise training, and outcomes in patients with heart failure and chronic obstructive pulmonary disease: findings from heart failure and a controlled trial investigating outcomes of exercise training (HF-ACTION). Am Heart J. 2013;165(2):193–199. | ||
Murad K, Goff DC Jr, Morgan TM, et al. Burden of comorbidities and functional and cognitive impairments in elderly patients at the initial diagnosis of heart failure and their impact on total mortality: the cardiovascular health study. JACC Heart Fail. 2015;3(7):542–550. | ||
Mentz RJ, Kelly JP, von Lueder TG, et al. Noncardiac comorbidities in heart failure with reduced versus preserved ejection fraction. J Am Coll Cardiol. 2014;64(21):2281–2293. | ||
Steinberg BA, Zhao X, Heidenreich PA, et al; Get With the Guidelines Scientific Advisory Committee and Investigators. Trends in patients hospitalized with heart failure and preserved left ventricular ejection fraction: prevalence, therapies, and outcomes. Circulation. 2012;126(1):65–75. | ||
Fonarow GC, Stough WG, Abraham WT, et al; OPTIMIZE-HF Investigators and Hospitals. Characteristics, treatments, and outcomes of patients with preserved systolic function hospitalized for heart failure: a report from the OPTIMIZE-HF Registry. J Am Coll Cardiol. 2007;50(8):768–777. | ||
Yancy CW, Lopatin M, Stevenson LW, De Marco T, Fonarow GC; ADHERE Scientific Advisory Committee and Investigators. Clinical presentation, management, and in-hospital outcomes of patients admitted with acute decompensated heart failure with preserved systolic function: a report from the acute decompensated heart failure national registry (ADHERE) database. J Am Coll Cardiol. 2006;47(1):76–84. | ||
Upadhya B, Taffet GE, Cheng CP, Kitzman DW. Heart failure with preserved ejection fraction in the elderly: scope of the problem. J Mol Cell Cardiol. 2015;83:73–87. | ||
Cheng RK, Cox M, Neely ML, et al. Outcomes in patients with heart failure with preserved, borderline, and reduced ejection fraction in the Medicare population. Am Heart J. 2014;168(5):721–730. | ||
Garcia-Perez L, Linertova R, Lorenzo-Riera A, Vazquez-Diaz JR, Duque-Gonzalez B, Sarria-Santamera A. Risk factors for hospital readmissions in elderly patients: a systematic review. QJM. 2011;104(8):639–651. | ||
Marcantonio ER, McKean S, Goldfinger M, Kleefield S, Yurkofsky M, Brennan TA. Factors associated with unplanned hospital readmission among patients 65 years of age and older in a Medicare managed care plan. Am J Med. 1999;107(1):13–17. | ||
Chamberlain AM, St Sauver JL, Gerber Y, et al. Multimorbidity in heart failure: a community perspective. Am J Med. 2015;128(1):38–45. | ||
Tinetti ME, Fried TR, Boyd CM. Designing health care for the most common chronic condition – multimorbidity. JAMA. 2012;307(23):2493–2494. | ||
Gastelurrutia P, Benrimoj SI, Espejo J, Tuneu L, Mangues MA, Bayes-Genis A. Negative clinical outcomes associated with drug-related problems in heart failure (HF) outpatients: impact of a pharmacist in a multidisciplinary HF clinic. J Card Fail. 2011;17(3):217–223. | ||
Cacciatore F, Abete P, Mazzella F, et al. Frailty predicts long-term mortality in elderly subjects with chronic heart failure. Eur J Clin Invest. 2005;35(12):723–730. | ||
Pulignano G, Del Sindaco D, Di Lenarda A, et al. Usefulness of frailty profile for targeting older heart failure patients in disease management programs: a cost-effectiveness, pilot study. J Cardiovasc Med (Hagerstown). 2010;11(10):739–747. | ||
Dodson JA, Truong TT, Towle VR, Kerins G, Chaudhry SI. Cognitive impairment in older adults with heart failure: prevalence, documentation, and impact on outcomes. Am J Med. 2013;126(2):120–126. | ||
Krumholz HM. Post-hospital syndrome – an acquired, transient condition of generalized risk. N Engl J Med. 2013;368(2):100–102. | ||
Ranasinghe I, Wang Y, Dharmarajan K, Hsieh AF, Bernheim SM, Krumholz HM. Readmissions after hospitalization for heart failure, acute myocardial infarction, or pneumonia among young and middle-aged adults: a retrospective observational cohort study. PLoS Med. 2014;11(9):e1001737. | ||
Altfeld SJ, Shier GE, Rooney M, et al. Effects of an enhanced discharge planning intervention for hospitalized older adults: a randomized trial. Gerontologist. 2013;53(3):430–440. | ||
Coleman EA, Smith JD, Raha D, Min SJ. Posthospital medication discrepancies: prevalence and contributing factors. Arch Intern Med. 2005;165(16):1842–1847. | ||
Wong JD, Bajcar JM, Wong GG, et al. Medication reconciliation at hospital discharge: evaluating discrepancies. Ann Pharmacother. 2008;42(10):1373–1379. | ||
Levy BR. Eradication of ageism requires addressing the enemy within. Gerontologist. 2001;41(5):578–579. [discussion 580]. | ||
Greene MG, Adelman R, Charon R, Hoffman S. Ageism in the medical encounter: an exploratory study of the doctor-elderly patient relationship. Lang Commun. 1986;6(1–2):113–124. | ||
Giugliano RP, Camargo CA Jr, Lloyd-Jones DM, et al. Elderly patients receive less aggressive medical and invasive management of unstable angina: potential impact of practice guidelines. Arch Intern Med. 1998;158(10):1113–1120. | ||
Forman DE, Cannon CP, Hernandez AF, et al; Get with the Guidelines Steering Committee and Hospitals. Influence of age on the management of heart failure: findings from get with the guidelines-heart failure (GWTG-HF). Am Heart J. 2009;157(6):1010–1017. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.