")
Back to Journals » Clinical Interventions in Aging » Volume 9
Optimal management of elderly cancer patients: usefulness of the Comprehensive Geriatric Assessment
Authors Caillet P, Laurent M, Bastuji-Garin S, Liuu E, Culine S, Lagrange J, Canoui-Poitrine F, Paillaud E
Received 30 May 2014
Accepted for publication 18 July 2014
Published 29 September 2014 Volume 2014:9 Pages 1645—1660
DOI https://doi.org/10.2147/CIA.S57849
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Philippe Caillet,1,2 Marie Laurent,1,2 Sylvie Bastuji-Garin,1,3,4 Evelyne Liuu,2 Stephane Culine,5 Jean-Leon Lagrange,6 Florence Canoui-Poitrine,1,2,3,* Elena Paillaud1,2,*
1Laboratoire d’Investigation Clinique (LIC), Faculté de Medecine, Université Paris Est Créteil (UPEC), Créteil, Paris, 2Unité de Coordination d’Onco-Gériatrie, Département de Médecine Interne et Gériatrie, Hôpital Henri-Mondor, Assistance Publique – Hopitaux de Paris (AP-HP), Créteil, 3Service de Santé Publique, Hôpital Henri-Mondor, AP-HP, Créteil, 4Unité de Recherche Clinique, Hôpital Henri-Mondor, AP-HP, Créteil, 5Service d’Oncologie Médicale, Hôpital Saint-Louis, AP-HP, Paris, 6Service de Radiotherapie, Hôpital Henri-Mondor, AP-HP, Créteil, France
*These authors contributed equally to this work
Background: Cancer is common in older patients, who raise specific treatment challenges due to aging-related, organ-specific physiologic changes and the presence in most cases of comorbidities capable of affecting treatment tolerance and outcomes. Identifying comorbid conditions and physiologic changes due to aging allows oncologists to better assess the risk/benefit ratio and to adjust the treatment accordingly. Conducting a Comprehensive Geriatric Assessment (CGA) is one approach developed for this purpose. We reviewed the evidence on the usefulness of CGA for assessing health problems and predicting cancer treatment outcomes, functional decline, morbidity, and mortality in older patients with solid malignancies.
Methods: We searched Medline for articles published in English between January 1, 2000 and April 14, 2014, and reporting prospective observational or interventional studies of CGA feasibility or effectiveness in patients aged ≥65 years with solid malignancies. We identified studies with at least 100 patients, a multivariate analysis, and assessments of at least five of the following CGA domains: nutrition, cognition, mood, functional status, mobility and falls, polypharmacy, comorbidities, and social environment.
Results: All types of CGA identified a large number of unrecognized health problems capable of interfering with cancer treatment. CGA results influenced 21%–49% of treatment decisions. All CGA domains were associated with chemotoxicity or survival in at least one study. The abnormalities that most often predicted mortality and chemotoxicity were functional impairment, malnutrition, and comorbidities.
Conclusion: The CGA uncovers numerous health problems in elderly patients with cancer and can affect treatment decisions. Functional impairment, malnutrition, and comorbidities are independently associated with chemotoxicity and/or survival. Only three randomized published studies evaluated the effectiveness of CGA-linked interventions. Further research into the effectiveness of the CGA in improving patient outcomes is needed.
Keywords: cancer, geriatric assessment, elderly, mortality, chemotoxicity, outcomes
Introduction
The management of older cancer patients has become a major public health concern in Western countries because of the aging of the population and the steady increase in cancer incidence with advancing age. Today, over 60% of all cancers are diagnosed in patients older than 65 years in Europe and the USA. This percentage is expected to rise to 70% within the next 30 years.1,2 The care of older patients thus constitutes an important part of everyday oncology practice. However, despite the rapid growth of the geriatric oncology population in the real-life setting, older patients are underrepresented in the clinical trials that set the standards of care in oncology.3 As a result, there is a lack of evidence on the risk/benefit ratio of cancer treatments in older patients. Comorbidities and disabilities become increasingly prevalent with advancing age and are associated with treatment-related side effects and poorer outcomes.4–7 Thus, a major issue for oncologists treating older cancer patients is determination of the intensity of cancer treatment best suited to each patient. There is considerable heterogeneity among patients of the same age, so that chronologic age alone provides little information regarding an individual’s tolerance to cancer treatments.
Identifying comorbid conditions and aging-related, organ-specific physiologic changes that increase the risk of toxicities may allow oncologists to better assess the risk/benefit ratio in individual patients, to develop customized treatment adjustments, and to implement interventions designed to decrease the risk of toxicity. The Comprehensive Geriatric Assessment (CGA) is one approach developed for this purpose. The CGA was designed by geriatricians as a multidimensional assessment of general health status based on validated geriatric scales and tests that produce an inventory of health problems, allowing the development of an individualized geriatric intervention program. Since the mid-1990s, oncologists and geriatricians have worked to integrate CGA approaches into oncologic practice. The International Society of Geriatric Oncology created a taskforce to determine the best CGA format for use in oncology.8 Independent of these recommendations, the feasibility and effectiveness of the CGA in managing older cancer patients and the evidence of its usefulness in everyday oncology practice deserve consideration. Only two systemic reviews have focused on the CGA in older cancer patients.9–11
The objectives of this review were to depict CGA components in everyday oncology practice and to assess the usefulness of the CGA in assessing health problems, guiding decisions about cancer treatments, predicting outcomes, and developing a coordinated program of tailored geriatric interventions. We also reviewed the available data on the benefits of specific CGA-based interventions.
Materials and methods
Data sources
We conducted a systematic comprehensive search of Medline (PubMed) for articles published in English between January 1, 2000, and April 14, 2014.
Study eligibility criteria
We used four eligibility criteria to select studies for our review: a focus on older patients (65 years or older) with solid cancer (excluding hematologic malignancies) who were seen in oncology or surgery or geriatric-oncology clinics (as outpatients or inpatients); prospective data collection and observational or interventional design; a sample size of at least 100 patients; and assessment of at least five CGA domains (from nutrition, cognition, mood, functional status, mobility and falls, polypharmacy, comorbidities, and social environment). We excluded editorials, case studies, studies published as abstracts, and review articles other than the two most recent systematic reviews of the CGA in geriatric oncology.9–11
For assessment of the ability of the CGA to detect previously unrecognized health problems, the studies had to contain information on the frequencies of CGA domain alterations or on the data needed to compute these frequencies. We therefore excluded articles that did not report the frequencies of CGA domain alterations. To assess the usefulness of the CGA in predicting outcomes such as postoperative complications, feasibility of chemotherapy, chemotoxicity, functional decline/disability, and mortality, we included only studies involving a multivariate analysis. To enable an evaluation of the impact of CGA-based geriatric interventions, a randomized design was required.
We designed a specific algorithm for each objective:
- Algorithm 1 to assess the usefulness of the CGA in assessing health problems (Figure 1): (“Neoplasms” [Mesh] OR “cancer” [Text Word]) AND (“Geriatric Assessment” [Mesh] OR “Comprehensive Geriatric Assessment” [Text Word]);
- Algorithm 2 to assess the usefulness of the CGA in predicting outcomes (Figure 2): (“Geriatric Assessment” [Mesh] OR “Comprehensive Geriatric Assessment” [Text Word]) AND (“Neoplasms” [Mesh] OR “cancer” [Text Word]) AND (“Epidemiologic Studies” [Mesh] OR “Epidemiologic Research Design” [Mesh] OR “Survival” [Mesh] OR “Mortality” [Mesh] OR “toxicity” [Subheading] OR “Morbidity” [Mesh] OR “Treatment Outcome” [Mesh]);
- Algorithm 3 to assess the usefulness of the CGA in developing a coordinated program of tailored geriatric interventions (Figure 3): (“Geriatric Assessment-based intervention” [Mesh] OR “Comprehensive Geriatric Assessment-based intervention” [Text Word]) AND (“tumor” [Text Word] OR “cancer” [Text Word] OR “neoplasms” [Mesh]) AND (“clinical trial” [Mesh] OR “trial” [Mesh] OR “randomized trial” [text Word]).
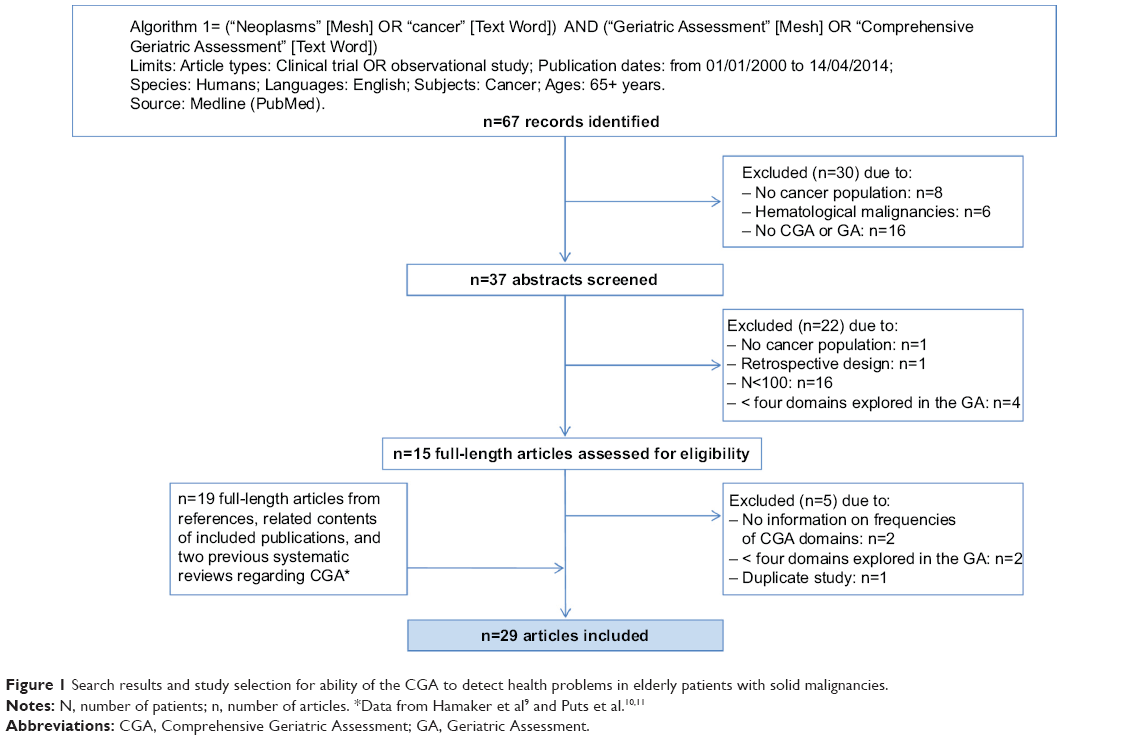 | Figure 1 Search results and study selection for ability of the CGA to detect health problems in elderly patients with solid malignancies. |
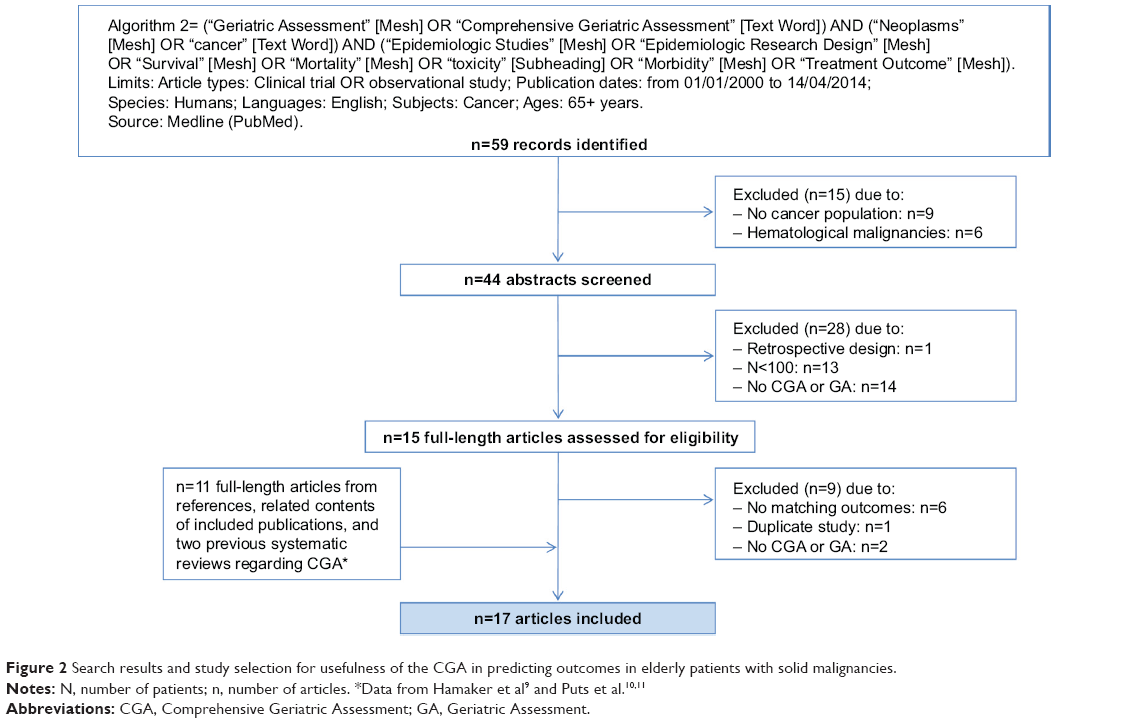 | Figure 2 Search results and study selection for usefulness of the CGA in predicting outcomes in elderly patients with solid malignancies. |
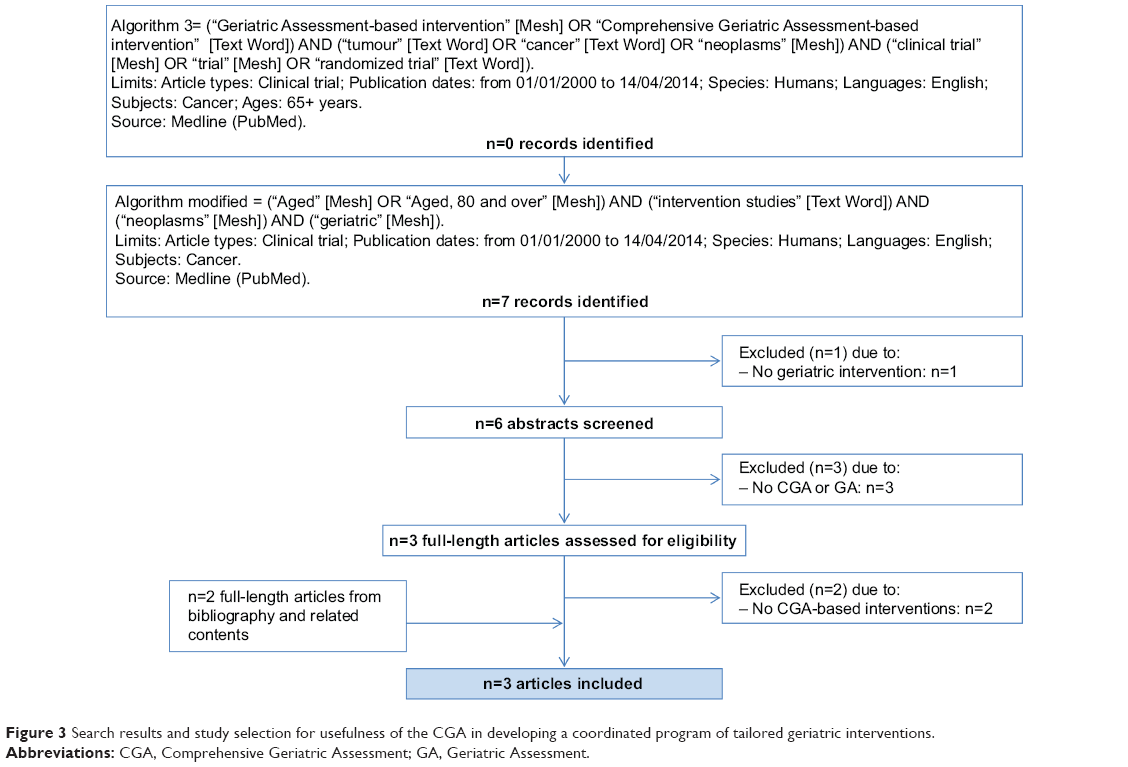 | Figure 3 Search results and study selection for usefulness of the CGA in developing a coordinated program of tailored geriatric interventions. |
For the three algorithms, we used the following limits: Article Types, Clinical Trial OR Observational Study; Publication Dates from January 1, 2000 to April 14, 2014; Species, Humans; Language, English; Subjects, Cancer; and Ages, 65+ years.
Study selection
Articles were selected initially by three senior medical doctors specialized in geriatric oncology (PC, FCP, and EP), based on the titles and abstracts and on the eligibility criteria described above. When one or more of these three investigators were uncertain about whether the article fulfilled the eligibility criteria, the abstract was included and the full-length article was analyzed by the same three investigators. Disagreements were resolved by consensus. We also reviewed the reference lists of all selected articles, related contents of the Medline search, and reference lists of the three above-mentioned reviews9–11 to look for relevant articles.
The three investigators used the PRISMA® (Preferred Reporting Items for Systematic Reviews and Meta-analysis) guidelines (http://www.prisma-statement.org/statement.htm) to assess the quality of included studies. Disagreements were resolved by consensus.
What is the CGA?
Definition
The CGA was defined in 1988 as
[…] a multidisciplinary evaluation in which the multiple problems of older persons are uncovered, described, and explained, if possible, and in which the resources and strengths of the person are catalogued, need for services assessed, and a coordinated care plan developed […]12
CGA components and assessment tools
The core components of the CGA are functional status, cognition, mood and emotional status, social support, financial concerns, nutritional status, comorbidities and polypharmacy, geriatric syndromes (fall risk, confusion, urinary incontinence, visual or hearing impairments), goals of care, and advance care planning.8 The CGA uses validated geriatric scales and tests to produce an inventory of health problems, which can then serve to develop an individualized geriatric intervention plan. The content of the assessment varies with the care setting (eg, home, clinic, hospital, or nursing home). In many settings, the CGA process relies on a core team consisting of a physician, a nurse, and a social worker, who obtain assistance as needed from other health care professionals (eg, nutritionist, physical therapist, and/or psychologist).
The effects of implementing a CGA-based approach have been evaluated in a number of controlled studies conducted in inpatients and community-dwelling outpatients. A meta-analysis of 28 controlled trials comprising 4,959 patients who underwent one of five CGA types and 4,912 controls13 showed that the CGA, when used to guide management decisions and combined with long-term follow-up, detected a greater number of health problems and improved survival, functional status, and unplanned admissions in older patients with nonmalignant diseases, compared with usual care. However, the effect size was greater for inpatients than for community-dwelling patients. A meta-analysis of 21 trials with 10,315 patients indicated that the CGA increased the likelihood of patients being alive and in their own homes 6 months after an emergency admission.14
Conducting the CGA in oncology
To help oncologists select the best treatment for older patients, the US National Comprehensive Cancer Network, International Society of Geriatric Oncology, and European Organisation for Research and Treatment of Cancer recommend a CGA-based approach for elderly cancer patients.8,15 However, the best CGA type and implementation method for cancer patients in everyday practice remain to be defined. Limitations to the widespread use of the CGA in everyday practice are the considerable time and human resources needed to conduct the assessment and the failure of some health insurance systems to reimburse it. The abundance of studies investigating the effectiveness of the CGA or using CGA components supports the feasibility of this assessment in geriatric oncology. Only one large prospective multicenter study16 carried out in ten hospitals in Belgium, including 1,967 older cancer patients, has specifically addressed the feasibility of the CGA. In this study, the high inclusion rate involving 71% of patients indicated that the implementation of a geriatric assessment was very feasible. Nevertheless, this study showed that the information revealed by the CGA did not always reach treating physicians and efforts were needed to improve the interaction between the oncologist, geriatrician, and trained health care worker.
Ability to detect previously unrecognized health problems in the elderly with solid malignancies
Table 1 recapitulates the results of 29 studies describing CGA findings in elderly patients with solid malignancies.5,7,16–42 Functional status was consistently assessed using the Eastern Cooperative Oncology Group-Performance Status (ECOG-PS), Activities of Daily Living (ADL) index, and/or instrumental ADL index. Functional impairment defined as an ECOG-PS grade ≥2 was noted in 2%–50% of patients. Deficiency in at least one ADL or instrumental ADL item was found in 10%–61% and 25%–73% of patients, respectively. Mobility or fall risk was assessed in 22/29 (75.9%) studies. The Timed Get-Up-and-Go or Tinetti test of gait and balance indicated a risk of falls in 14%–55% of patients. Of the 29 studies selected for this review, 13 (44.8%) used the Mini-Nutritional Assessment to evaluate nutritional status. Malnutrition or a high risk for malnutrition was found in 27%–83% of patients. The Mini-Mental State Examination was performed to evaluate cognition in 20/29 (69%) studies and showed cognitive dysfunction in 6%–42% of patients. The Geriatric Depression Scale (in its variants with 2, 4, 15, or 30 items) was the most widely used tool to assess depressive symptoms (19/29 studies, 65.5%) and showed depression in 10%–65% of patients. All 29 studies evaluated comorbidities, generally using the Cumulative Illness Rating Scale for Geriatrics (12/29 studies, 41%) or the Charlson Comorbidity Index (10/29 studies, 34.5%). Using these tools, at least one comorbidity was found in 23%–70% of patients, at least two comorbidities in 16%–59%, and at least three comorbidities in 50%–81%.
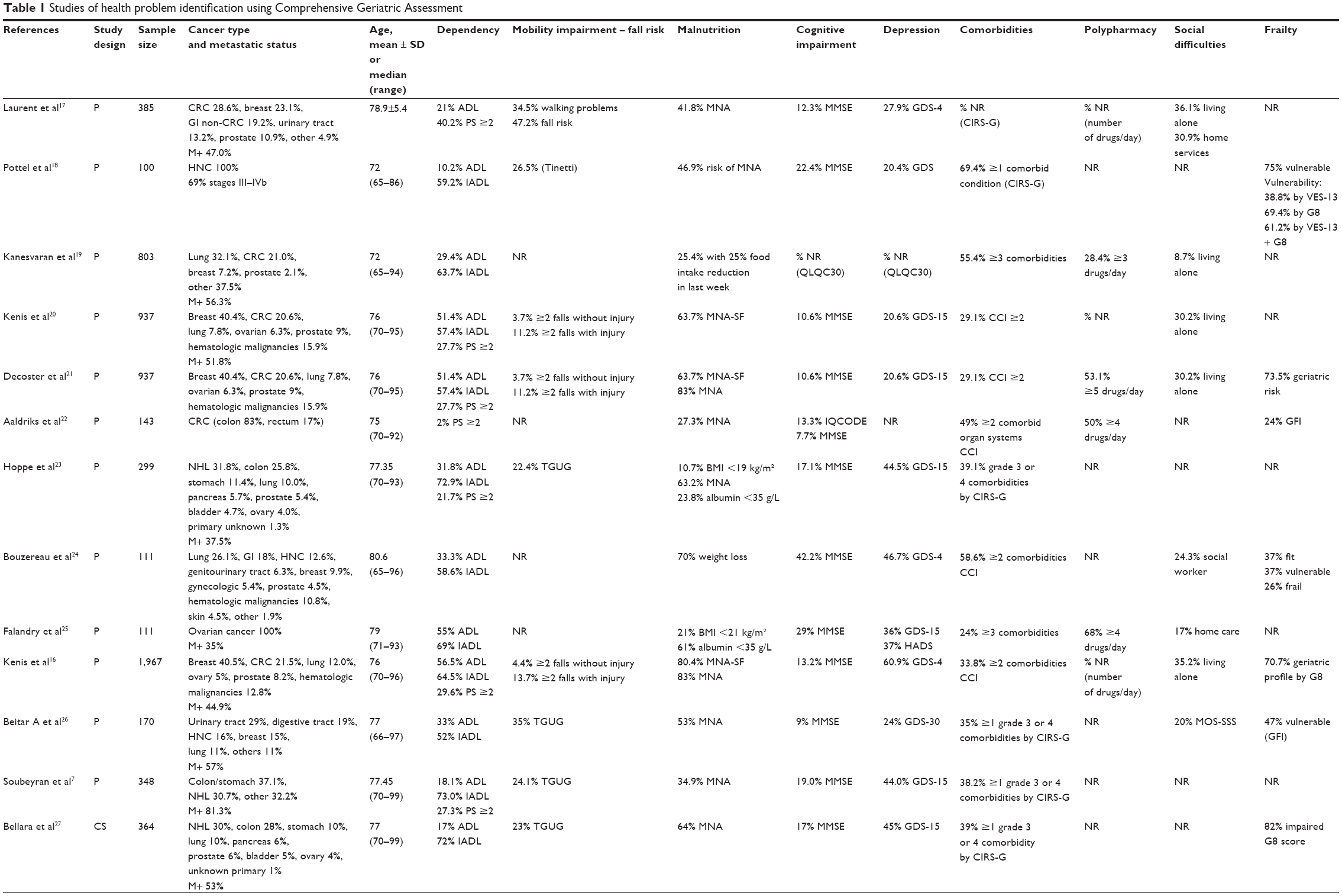 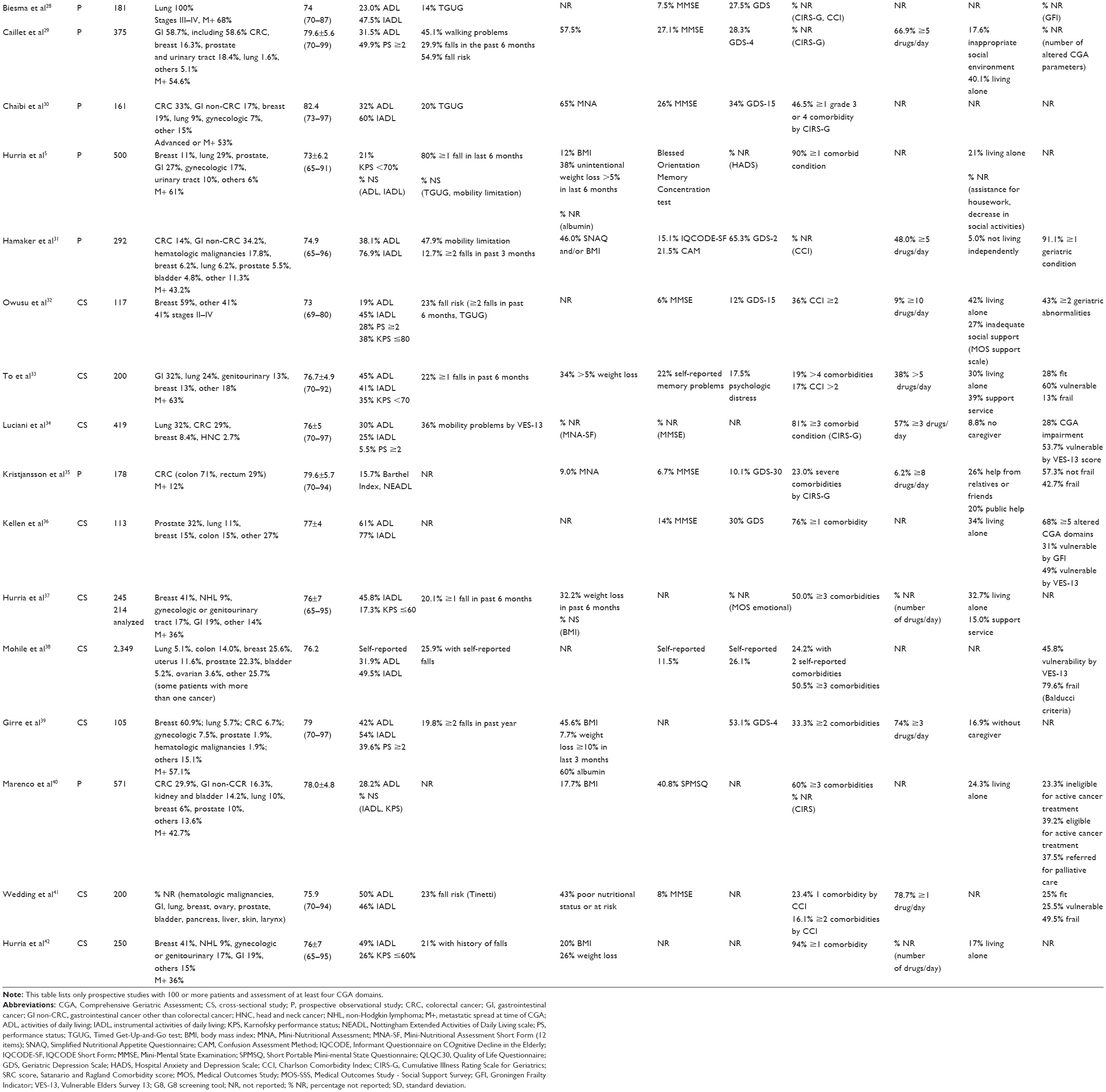 | Table 1 Studies of health problem identification using Comprehensive Geriatric Assessment |
Thus, all CGA types identified large numbers of geriatric problems and multiple comorbidities likely to interfere with cancer treatment and to compete with cancer as a cause of death. Identifying these problems is therefore a crucial initial step when implementing comprehensive care for older patients with cancer.
Influence of CGA on treatment decisions
The CGA is recommended in older cancer patients to help physicians determine whether the best option is standard anticancer treatment, anticancer treatment adjusted according to existing health problems other than cancer, or supportive care only. Nevertheless, the relationship between CGA findings and the treatment decision-making process remains unclear. To date, few studies have addressed the influence of CGA on decision-making.
A prospective study16 of 1,967 older cancer patients (87.2% with solid malignancies and 12.8% with hematologic malignancies) evaluated the prevalence of changes in treatment decisions based on CGA findings. The oncologists were aware of the CGA results at the time of treatment decision-making for only 61.3% of patients and, among these, 25.3% had changes in the final treatment decision in response to the CGA results. This study did not assess relationships between individual CGA parameters and cancer treatment decisions.
Two studies used univariate analyses to investigate associations between CGA parameters and treatment decisions. In a prospective study of 105 older cancer patients (98.1% with solid malignancies),39 the treatment plan was modified after CGA in 38.7% of cases. By univariate analysis, body mass index ≤23 and absence of depression were associated with treatment changes. In another prospective study of 161 patients with solid malignancies,30 the CGA influenced cancer treatment decisions in 49% of cases. Chemotherapy intensity was diminished in 21% of patients (by using less intensive regimens in 18% and by delaying treatment initiation in 3%) and augmented in 28% of patients.
Only two prospective studies involved multivariate analyses to identify CGA parameters associated with treatment decisions. In 571 older patients with solid malignancies,40 factors independently associated with receiving supportive care only were older age, living alone, ADL impairment, and low body mass index, whereas a higher instrumental ADL score was associated with receiving active cancer treatment. The other study29 included 375 older patients with solid malignancies, of whom 20.8% had CGA-based changes in their treatment plan, which consisted of decreased treatment intensity in 81% of cases. By multivariate analysis, factors independently associated with treatment changes were a lower ADL score and malnutrition.
These five studies suggest that some CGA parameters may influence treatment decisions. Function and nutritional status may have the strongest effect.
CGA components predicting cancer-treatment outcomes, functional decline, morbidity, and mortality in older patients with solid malignancies
Determining the optimal therapeutic strategy is a major challenge in older cancer patients. An important goal of the CGA is prediction of mortality and cancer treatment toxicities. Table 2 shows the findings from 17 studies reporting associations that link CGA components to cancer treatment outcomes, functional decline, and mortality in elderly patients with solid malignancies.5–7,17,23,25,28,35,43–52 Four studies5,6,25,44 investigated relationships between CGA components and chemotoxicity. Dependency as indicated by impaired instrumental ADL or ECOG-PS values, mobility impairment, cognitive dysfunction, malnutrition, social difficulties, and polypharmacy were significantly associated with chemotoxicity. Nine studies7,25,45,47–52 assessed the ability of CGA components to predict mortality. Dependency assessed by instrumental ADL and/or ECOG-PS, mobility impairment, cognitive dysfunction, depressive mood, malnutrition, and comorbidities was associated with mortality independently from cancer parameters. Finally, each CGA domain was associated with chemotoxicity and survival in at least one study. The domains most often reported as predicting mortality and chemotoxicity were functional impairment, malnutrition, and comorbidities.
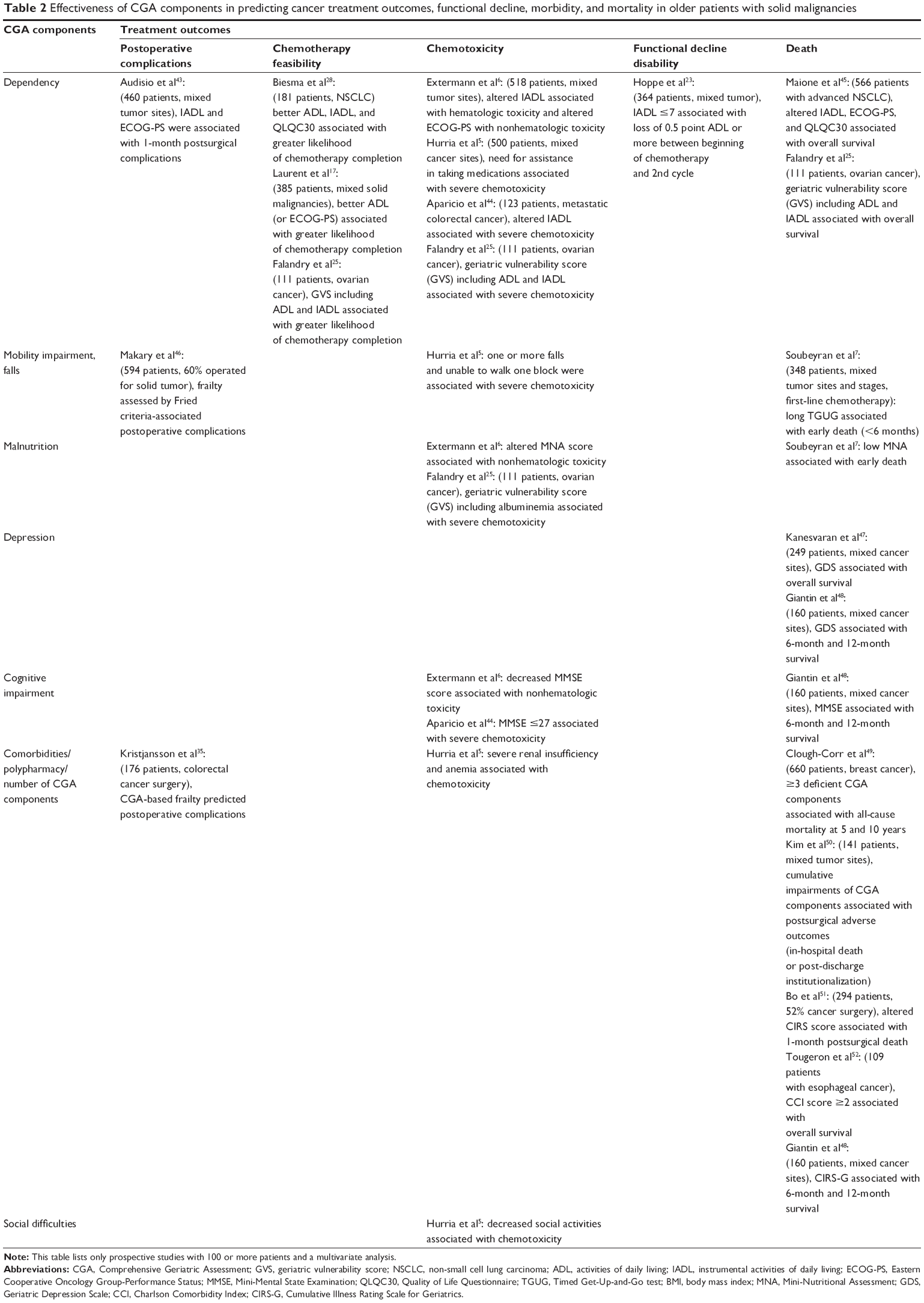 | Table 2 Effectiveness of CGA components in predicting cancer treatment outcomes, functional decline, morbidity, and mortality in older patients with solid malignancies |
CGA-based individually tailored coordinated care plans
An important aim in conducting a CGA is to develop and implement individually tailored geriatric interventions. Few studies have described the interventions carried out based on CGA results in older patients with cancer. In one study, a geriatrician performed a CGA, then suggested multidisciplinary interventions based on the results in 375 patients referred to a geriatric oncology unit.29 The interventions involved social support for 172 (46%) patients, physiotherapy for 157 (41%), changes in current chronic medications for 115 (31%), nutritional care for 262 (70%), a memory evaluation for 79 (21%), and psychologic care for 135 (36%). Similar findings were obtained in a study30 of 161 patients, among whom 122 (76%) received CGA-based interventions, including nutritional care (43%), treatment of depression (19%), a memory evaluation (18%), changes in chronic medications (37%), and/or social support (20%). In a recent large cohort study16 of 1,967 patients, the results of CGA led to intervention plans targeting all CGA domains in 25% of patients.
Very few randomized trials have assessed the potential effect on patient outcomes of CGA-based management and follow-up of health problems in older cancer patients (Figure 3). Two randomized trials in older post-surgical cancer patients showed significant survival gains with home care by advanced practice nurses53 or improved appropriateness of treatment strategies with nurse case management.54 A secondary subset analysis of data from a randomized 2×2 factorial trial comparing care in a geriatric inpatient unit, geriatric outpatient clinic, both, and neither in frail older cancer inpatients showed that inpatient geriatric assessment and management significantly improved quality of life but not 1-year survival.55 In a recent randomized trial in older patients undergoing elective surgery for solid cancer, an individualized geriatric intervention plan based on patient-related risk factors for delirium failed to decrease the occurrence of postoperative delirium, other complications, or death.56 We urgently need randomized controlled trials of patient outcomes after CGA-based geriatric interventions. The available data suggest that these trials will demonstrate significant improvements, thus helping to convince health authorities that geriatric oncology teams must receive strong support. Seven such trials are ongoing and are registered on clinicaltrials.gov (Table 3).
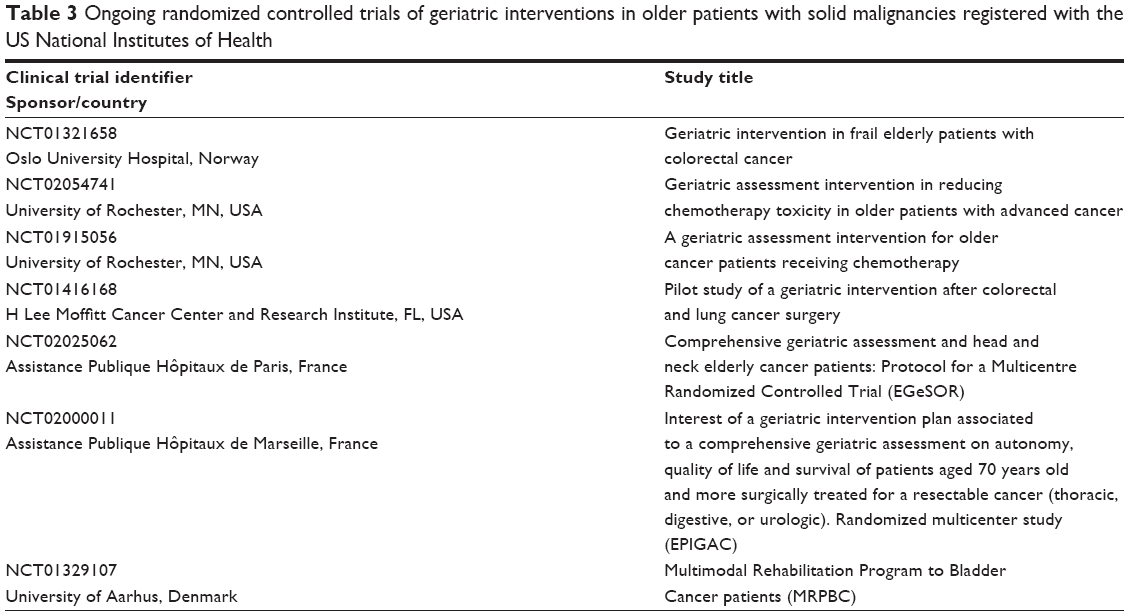 | Table 3 Ongoing randomized controlled trials of geriatric interventions in older patients with solid malignancies registered with the US National Institutes of Health |
Conclusion
All CGA types detect numerous unrecognized health problems that may interfere with cancer treatment and/or compete with cancer as a cause of death. CGA results affected treatment decisions in 21%–49% of patients in available studies. The results of 17 studies with large sample sizes and multivariate analyses indicate independent associations linking functional impairment, malnutrition, depressive symptoms, and comorbidities to chemotoxicity and/or overall survival. Only three randomized trials of the effectiveness of CGA-based interventions have been published. Further research to produce high-level evidence about the effects of CGA on patient outcomes are needed.
Acknowledgments
This paper is published on behalf of the ELCAPA Study Group, which comprises three oncologists (S Culine, Ch Tournigand, B Rousseau), one radiotherapist (J-L Lagrange), five geriatricians (P Caillet, M Laurent, E Liuu, E Paillaud, H Vincent), three epidemiologists (F Canouï-Poitrine, S Bastuji-Garin, E Audureau), one pharmacist (M Carvahlo-Verlinde), one biostatistician (A Le Thuaut), one clinical research medical doctor (N Reinald), and one clinical research assistant (A Radenne). We thank A Wolfe for editing the manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
Smith BD, Smith GL, Hurria A, Hortobagyi GN, Buchholz TA. Future of cancer incidence in the United States: burdens upon an aging, changing nation. J Clin Oncol. 2009;27(17):2758–2765. | ||
Arnold M, Karim-Kos HE, Coebergh JW, et al. Recent trends in incidence of five common cancers in 26 European countries since 1988: analysis of the European Cancer Observatory. Eur J Cancer. October 8, 2013. [Epub ahead of print]. | ||
Scher KS, Hurria A. Under-representation of older adults in cancer registration trials: known problem, little progress. J Clin Oncol. 2012;30(17):2036–2038. | ||
Turrentine FE, Wang H, Simpson VB, Jones RS. Surgical risk factors, morbidity, and mortality in elderly patients. J Am Coll Surg. 2006;203(6):865–877. | ||
Hurria A, Togawa K, Mohile SG, et al. Predicting chemotherapy toxicity in older adults with cancer: a prospective multicenter study. J Clin Oncol. 2011;29(25):3457–3465. | ||
Extermann M, Boler I, Reich RR, et al. Predicting the risk of chemotherapy toxicity in older patients: the Chemotherapy Risk Assessment Scale for High-Age Patients (CRASH) score. Cancer. 2012;118(13):3377–3386. | ||
Soubeyran P, Fonck M, Blanc-Bisson C, et al. Predictors of early death risk in older patients treated with first-line chemotherapy for cancer. J Clin Oncol. 2012;30(15):1829–1834. | ||
Extermann M, Aapro M, Bernabei R, et al. Use of comprehensive geriatric assessment in older cancer patients: recommendations from the task force on CGA of the International Society of Geriatric Oncology (SIOG). Crit Rev Oncol Hematol. 2005;55(3):241–252. | ||
Hamaker ME, Vos AG, Smorenburg CH, de Rooij SE, van Munster BC. The value of geriatric assessments in predicting treatment tolerance and all-cause mortality in older patients with cancer. Oncologist. 2012;17(11):1439–1449. | ||
Puts MT, Hardt J, Monette J, Girre V, Springall E, Alibhai SM. Use of geriatric assessment for older adults in the oncology setting: a systematic review. J Natl Cancer Inst. 2012;104(15):1133–1163. | ||
Puts MT, Santos B, Hardt J, et al. An update on a systematic review of the use of geriatric assessment for older adults in oncology. Ann Oncol. 2014;25(2):307–315. | ||
Solomon DH. Geriatric assessment: methods for clinical decision making. JAMA. 1988;259(16):2450–2452. | ||
Stuck AE, Siu AL, Wieland GD, Adams J, Rubenstein LZ. Comprehensive geriatric assessment: a meta-analysis of controlled trials. Lancet. 1993;342(8878):1032–1036. | ||
Ellis G, Whitehead MA, O’Neill D, Langhorne P, Robinson D. Comprehensive geriatric assessment for older adults admitted to hospital. Cochrane Database Syst Rev. 2011;7:CD006211. | ||
Pallis AG, Wedding U, Lacombe D, Soubeyran P, Wildiers H. Questionnaires and instruments for a multidimensional assessment of the older cancer patient: what clinicians need to know? Eur J Cancer. 2010;46(6):1019–1025. | ||
Kenis C, Bron D, Libert Y, et al. Relevance of a systematic geriatric screening and assessment in older patients with cancer: results of a prospective multicentric study. Ann Oncol. 2013;24(5):1306–1312. | ||
Laurent M, Paillaud E, Tournigand C, et al. Assessment of solid cancer treatment feasibility in older patients: a prospective cohort study. Oncologist. 2014;19(3):275–282. | ||
Pottel L, Lycke M, Boterberg T, et al. Serial comprehensive geriatric assessment in elderly head and neck cancer patients undergoing curative radiotherapy identifies evolution of multidimensional health problems and is indicative of quality of life. Eur J Cancer Care. 2014;23(3):401–412. | ||
Kanesvaran R, Wang W, Yang Y, et al. Characteristics and treatment options of elderly Chinese patients with cancer as determined by Comprehensive Geriatric Assessment (CGA). J Geriatr Oncol. 2014;5(2):171–178. | ||
Kenis C, Decoster L, Van Puyvelde K, et al. Performance of two geriatric screening tools in older patients with cancer. J Clin Oncol. 2014;32(1):19–26. | ||
Decoster L, Kenis C, Van Puyvelde K, et al. The influence of clinical assessment (including age) and geriatric assessment on treatment decisions in older patients with cancer. J Geriatr Oncol. 2013;4(3):235–241. | ||
Aaldriks AA, Giltay EJ, le Cessie S, et al. Prognostic value of geriatric assessment in older patients with advanced breast cancer receiving chemotherapy. Breast. 2013;22(5):753–760. | ||
Hoppe S, Rainfray M, Fonck M, et al. Functional decline in older patients with cancer receiving first-line chemotherapy. J Clin Oncol. 2013;31(31):3877–3882. | ||
Bouzereau V, Le Caer F, Guardiola E, et al. Experience of multidisciplinary assessment of elderly patients with cancer in a French general hospital during 1 year: a new model care study. J Geriatr Oncol. 2013;4(4):394–401. | ||
Falandry C, Weber B, Savoye A-M, et al. Development of a geriatric vulnerability score in elderly patients with advanced ovarian cancer treated with first-line carboplatin: a GINECO prospective trial. Ann Oncol. 2013;24(11):2808–2813. | ||
Baitar A, Van Fraeyenhove F, Vandebroek A, et al. Evaluation of the Groningen Frailty Indicator and the G8 questionnaire as screening tools for frailty in older patients with cancer. J Geriatr Oncol. 2013;4(1):32–38. | ||
Bellera CA, Rainfray M, Mathoulin-Pelissier S, et al. Screening older cancer patients: first evaluation of the G-8 geriatric screening tool. Ann Oncol. 2012;23(8):2166–2172. | ||
Biesma B, Wymenga AN, Vincent A, et al. Quality of life, geriatric assessment and survival in elderly patients with non-small-cell lung cancer treated with carboplatin-gemcitabine or carboplatin-paclitaxel: NVALT-3 a phase III study. Ann Oncol. 2011;22(7):1520–1527. | ||
Caillet P, Canoui-Poitrine F, Vouriot J, et al. Comprehensive geriatric assessment in the decision-making process in elderly patients with cancer: ELCAPA study. J Clin Oncol. 2011;29(27):3636–3642. | ||
Chaibi P, Magne N, Breton S, et al. Influence of geriatric consultation with comprehensive geriatric assessment on final therapeutic decision in elderly cancer patients. Crit Rev Oncol Hematol. 2011;79(3):302–307. | ||
Hamaker ME, Buurman BM, van Munster BC, Kuper IM, Smorenburg CH, de Rooij SE. The value of a comprehensive geriatric assessment for patient care in acutely hospitalized older patients with cancer. Oncologist. 2011;16(10):1403–1412. | ||
Owusu C, Koroukian SM, Schluchter M, Bakaki P, Berger NA. Screening older cancer patients for a Comprehensive Geriatric Assessment: a comparison of three instruments. J Geriatr Oncol. 2011;2(2):121–129. | ||
To TH, Okera M, Prouse J, Prowse RJ, Singhal N. Infancy of an Australian geriatric oncology program – characteristics of the first 200 patients. J Geriatr Oncol. 2010;1:81–86. | ||
Luciani A, Ascione G, Bertuzzi C, et al. Detecting disabilities in older patients with cancer: comparison between Comprehensive Geriatric Assessment and Vulnerable Elders Survey-13. J Clin Oncol. 2010;28(12):2046–2050. | ||
Kristjansson SR, Nesbakken A, Jordhoy MS, et al. Comprehensive geriatric assessment can predict complications in elderly patients after elective surgery for colorectal cancer: a prospective observational cohort study. Crit Rev Oncol Hematol. 2010;76(3):208–217. | ||
Kellen E, Bulens P, Deckx L, et al. Identifying an accurate pre-screening tool in geriatric oncology. Crit Rev Oncol Hematol. 2010;75(3):243–248. | ||
Hurria A, Li D, Hansen K, et al. Distress in older patients with cancer. J Clin Oncol. 2009;27(26):4346–4351. | ||
Mohile SG, Xian Y, Dale W, et al. Association of a cancer diagnosis with vulnerability and frailty in older Medicare beneficiaries. J Natl Cancer Inst. 2009;101(17):1206–1215. | ||
Girre V, Falcou MC, Gisselbrecht M, et al. Does a geriatric oncology consultation modify the cancer treatment plan for elderly patients? J Gerontol A Biol Sci Med Sci. 2008;63(7):724–730. | ||
Marenco D, Marinello R, Berruti A, et al. Multidimensional geriatric assessment in treatment decision in elderly cancer patients: 6-year experience in an outpatient geriatric oncology service. Crit Rev Oncol Hematol. 2008;68(2):157–164. | ||
Wedding U, Kodding D, Pientka L, Steinmetz HT, Schmitz S. Physicians’ judgement and comprehensive geriatric assessment (CGA) select different patients as fit for chemotherapy. Crit Rev Oncol Hematol. 2007;64(1):1–9. | ||
Hurria A, Lichtman SM, Gardes J, et al. Identifying vulnerable older adults with cancer: integrating geriatric assessment into oncology practice. J Am Geriatr Soc. 2007;55(10):1604–1608. | ||
Audisio RA, Pope D, Ramesh HS, et al. Shall we operate? Preoperative assessment in elderly cancer patients (PACE) can help. A SIOG surgical task force prospective study. Crit Rev Oncol Hematol. 2008;65(2):156–163. | ||
Aparicio T, Jouve JL, Teillet L, et al. Geriatric factors predict chemotherapy feasibility: ancillary results of FFCD 2001–2002 phase III study in first-line chemotherapy for metastatic colorectal cancer in elderly patients. J Clin Oncol. 2013;31(11):1464–1470. | ||
Maione P, Perrone F, Gallo C, et al. Pretreatment quality of life and functional status assessment significantly predict survival of elderly patients with advanced non-small-cell lung cancer receiving chemotherapy: a prognostic analysis of the multicenter Italian lung cancer in the elderly study. J Clin Oncol. 2005;23(28):6865–6872. | ||
Makary MA, Segev DL, Pronovost PJ, et al. Frailty as a predictor of surgical outcomes in older patients. J Am Coll Surg. 2010;210(6):901–908. | ||
Kanesvaran R, Li H, Koo KN, Poon D. Analysis of prognostic factors of comprehensive geriatric assessment and development of a clinical scoring system in elderly Asian patients with cancer. J Clin Oncol. 2011;29(27):3620–3627. | ||
Giantin V, Valentini E, Iasevoli M, et al. Does the Multidimensional Prognostic Index (MPI), based on a Comprehensive Geriatric Assessment (CGA), predict mortality in cancer patients? Results of a prospective observational trial. J Geriatr Oncol. 2013;4(3):208–217. | ||
Clough-Gorr KM, Thwin SS, Stuck AE, Silliman RA. Examining five- and ten-year survival in older women with breast cancer using cancer-specific geriatric assessment. Eur J Cancer. 2012;48(6):805–812. | ||
Kim KI, Park KH, Koo KH, Han HS, Kim CH. Comprehensive geriatric assessment can predict postoperative morbidity and mortality in elderly patients undergoing elective surgery. Arch Gerontol Geriatr. 2013;56(3):507–512. | ||
Bo M, Cacello E, Ghiggia F, Corsinovi L, Bosco F. Predictive factors of clinical outcome in older surgical patients. Arch Gerontol Geriatr. 2007;44(3):215–224. | ||
Tougeron D, Di Fiore F, Thureau S, et al. Safety and outcome of definitive chemoradiotherapy in elderly patients with oesophageal cancer. Br J Cancer. 2008;99(10):1586–1592. | ||
McCorkle R, Strumpf NE, Nuamah IF, et al. A specialized home care intervention improves survival among older post-surgical cancer patients. J Am Geriatr Soc. 2000;48(12):1707–1713. | ||
Goodwin JS, Satish S, Anderson ET, Nattinger AB, Freeman JL. Effect of nurse case management on the treatment of older women with breast cancer. J Am Geriatr Soc. 2003;51(9):1252–1259. | ||
Rao AV, Hsieh F, Feussner JR, Cohen HJ. Geriatric evaluation and management units in the care of the frail elderly cancer patient. J Gerontol A Biol Sci Med Sci. 2005;60(6):798–803. | ||
Hempenius L, Slaets JP, van Asselt D, de Bock GH, Wiggers T, van Leeuwen BL. Outcomes of a geriatric liaison intervention to prevent the development of postoperative delirium in frail elderly cancer patients: report on a multicentre, randomized, controlled trial. PLoS One. 2013;8(6):e64834. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.