")
Back to Journals » Drug Design, Development and Therapy » Volume 13
Omalizumab for chronic spontaneous urticaria in “complex” patients: data from real-life clinical practice
Authors Vollono L , Piccolo A , Lanna C , Esposito M, Bavetta M , Campione E , Bianchi L, Diluvio L
Received 7 May 2019
Accepted for publication 2 August 2019
Published 6 September 2019 Volume 2019:13 Pages 3181—3186
DOI https://doi.org/10.2147/DDDT.S214307
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Yan Zhu
Laura Vollono1, Arianna Piccolo1, Caterina Lanna1, Maria Esposito2, Mauro Bavetta1, Elena Campione1, Luca Bianchi1, Laura Diluvio1
1Dermatology Department, University of Rome, Tor Vergata, Italy; 2Dermatology Department, University of L’Aquila, L’Aquila, Italy
Correspondence: Laura Vollono
Dermatology Department, University of Rome Tor Vergata, Viale Oxford 81, Rome 00133, Italy
Tel +39 06 2090 0252
Email [email protected]
Introduction: Omalizumab is a recombinant humanized anti-IgE monoclonal antibody, approved for patients affected by chronic spontaneous urticaria resistant to antihistamines. Although the clinical benefit of omalizumab has been established in several clinical trials, there are very little data about long-term treatment with this drug and real-life reports regarding its use in patients affected by comorbidities other than urticaria are lacking.
Objectives: To assess omalizumab efficacy and safety in a heterogeneous population of patients affected by chronic spontaneous urticaria and several comorbidities in a real-world setting.
Materials and methods: Patients affected by chronic spontaneous urticaria with weekly urticaria activity score >16 resistant to antihistamines were treated with omalizumab 300 mg injection as add-on to H1-antihistamines administered every 4 weeks for 6 months. Clinical assessment of weekly urticaria activity score, dermatology life quality index and blood tests were performed at baseline, 12, 24 and 52 weeks of treatment. Response was assessed based on reduction weekly urticaria activity score.
Results: Thirty-two patients (22F; 10M) with a mean age of 52.4 years (range 27–72) affected by chronic spontaneous urticaria were enrolled. Comorbidities affecting our study population were divided into 6 categories: cardio-metabolic (77%), oncologic (19%), infectious (16%), allergic (45%) immunologic (41%) and others (18%). Omalizumab determined a satisfactory reduction of symptoms of chronic spontaneous urticaria and an amelioration of quality of life within our population. No relevant alterations regarding patients’ underlying conditions were encountered. This is the first study regarding the use of omalizumab for chronic spontaneous urticaria in a population of adult patients affected by several comorbidities, eg, cardio-metabolic, oncologic, infectious, allergic, immunologic and psychiatric diseases. Real-life data represent a valuable source of information about a drug’s safety and efficacy profile, especially in patients affected by different comorbidities that are widely diffused in Western countries.
Keywords: chronic spontaneous urticaria, omalizumab, oncologic, cardiovascular, allergic and immunologic conditions, comorbidities
Introduction
Chronic spontaneous urticaria (CSU) is a condition characterized by the presence of wheals lasting for more than 6 weeks, variably associated with the presence of angioedema.1,2 CSU is the most common type of urticaria and affects about 1% of the population, causing a notable deterioration in the patient’s quality of life and bearing a substantial social and health care burden.3–6 The presence of angioedema in patients affected by CSU has been associated with a prolonged disease duration compared with those experiencing wheals only.7 CSU is twice as common in women as in men, and most commonly affects patients aged 20–40 years.4,8 Unlike inducible urticaria, which is provoked by a variety of physical stimuli (cold, heat, pressure, etc.), its exact nosology is still not fully elucidated. The release of histamine from mast cells in the skin is considered a key factor in its pathogenesis.2,8–10 A role of functional autoantibodies against the high-affinity immunoglobulin E (IgE) receptor and other autoantibodies such as anti-thyroperoxidase has been postulated.8,11 Although modern second-generation H1-antihistamines are the standard of care for patients with CSU, adjunctive treatments may be required for effective control of symptoms in many patients.4 Omalizumab is a humanized IgG1k monoclonal antibody that specifically binds to free human IgE, firstly indicated for the treatment of allergy-induced asthma.12,13 In 2014, FDA approved omalizumab also for patients affected by CSU aged 12 years or older who continue to have symptoms despite antihistamines treatment. Omalizumab represents the first biologic medicine and the first new class of pharmacological agent approved for CSU since the introduction of non-sedating H1-antihistamines and it is available in Italy since 2015. Randomized controlled trials showed a good safety and tolerability profile in patients affected by CSU.14–16 However, safety data of long-term treatment with this biologic drug are scarce and real-life reports regarding its use in patients affected by comorbidities other than CSU are lacking. We hereby present our experience with the use of omalizumab in a heterogeneous Italian population of patients affected by CSU and other different comorbidities in a real-life setting.
Materials and methods
This study is a retrospective analysis of data collected at the Urticaria Clinic of the Dermatology Department of Policlinico Tor Vergata, Rome, Italy. Written informed consent was obtained from all patients included in the study. In view of the retrospective nature of the study, only a notification to the Ethical Committee of the investigator Center (Policlinico Tor Vergata, Rome, Italy) was required and submitted. Patients aged >18 years affected by moderate-to-severe CSU [defined as weekly Urticaria Activity Score (UAS7) >28], who remained symptomatic despite H1-antihistamines at up to 4 times the licensed dose, were included in the study. Medical history, presence of angioedema, clinical assignment of UAS-7, Dermatology Life Quality Index (DLQI) and laboratory assessments (complete blood count, liver and renal function test, electrophoresis, parasitology stool test, thyroid function test, antithyroid antibody test, antinuclear antibody [ANA] test, extractable nuclear antigen [ENA] test, IgE level assessment [PRIST]) were performed at BaseLine (BL), 12 weeks (W12), 24 weeks (W24) and 52 weeks (W52) of therapy. Patients received 300 mg subcutaneous injection as add-on to H1-antihistamines administered every 4 weeks for 6 months, followed by an 8-week treatment interruption. In case of recurrence, a second cycle of 5 additional doses of omalizumab 300 mg every 4 weeks (5 months) had been administered. Clinical response was assessed based on reduction of UAS-7 [outcomes were classified as complete (=0), partial (=0–28) or no response (>28)] and DLQI [outcomes were classified as complete (<6), partial (6–10) or no response (>10)]. Safety has been monitored performing blood and instrumental tests.
Results
A total of 32 patients (22 F;10 M) with mean age of 52.4 years (range 27–72) affected by CSU were enrolled. Mean duration of urticaria symptoms before treatment with omalizumab was 7 years (range 1–40). Three out of the enrolled patients were diagnosed with concomitant inducible urticaria (CIndU) triggered by physical activity, cold and UV light, respectively. Ten patients reported angioedema concurrently with itch and wheals. Comorbidities affecting our study population were divided into 6 categories, as reported in Table 1. Thirteen patients completed 2 cycles of treatment (13 months), while 10 patients had completed 1 cycle of treatment (6 months) and 8 patients had undergone 12 weeks (1/2 cycle) of treatment to date. One patient stopped the treatment because of increased arterial blood pressure after 24 weeks of treatment, whilst one other patient experienced acute ischemic heart disease (NSTEMI myocardial infarction) not leading to discontinuation. One patient reported generalized arthralgia and myalgia immediately after the first injection but not following subsequential injections. One patient referred regular episodes of fatigue and sleepiness the day after omalizumab injections, not leading to treatment discontinuation. Mild, transient local skin immediate reactions were observed in one patient. No cases of anaphylaxis or serious adverse events were reported in our patients. Twenty patients added second-generation H1-antihistamines to omalizumab because of persistence of pruritus and wheals after 2–4 weeks of treatment with omalizumab in monotherapy. Two patients affected by atopic dermatitis received methotrexate 15mg/week during treatment with omalizumab. Patients taking medications for their underlying conditions continued therapy under surveillance of their referral physicians. The trends of UAS-7 and DLQI median scores in our population are shown in Figures 1 and 2.
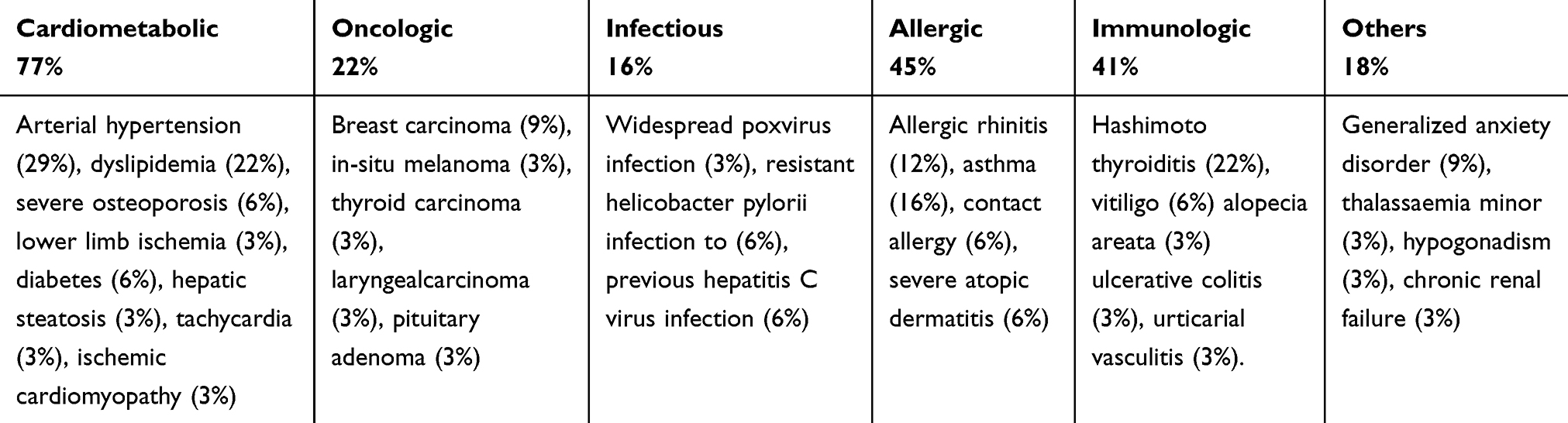 |
Table 1 Percentages of patients affected by different comorbidities in our study population |
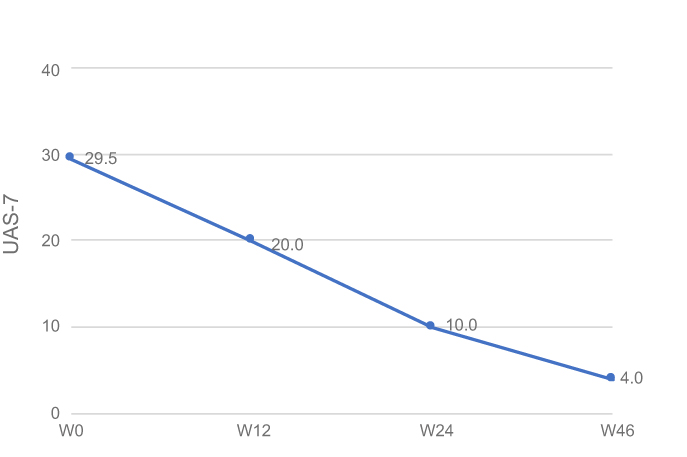 |
Figure 1 Trend of median UAS-7 score. UAS-7 median score decreased from 29.5 at baseline (BL) over 32 patients to 20.0 at W12 over 32 patients and kept decreasing to a value of 10.0 over 25 patients at W24. A further reduction of UAS-7 was observed at W46, with a mean value of 4.0 over 13 patients. |
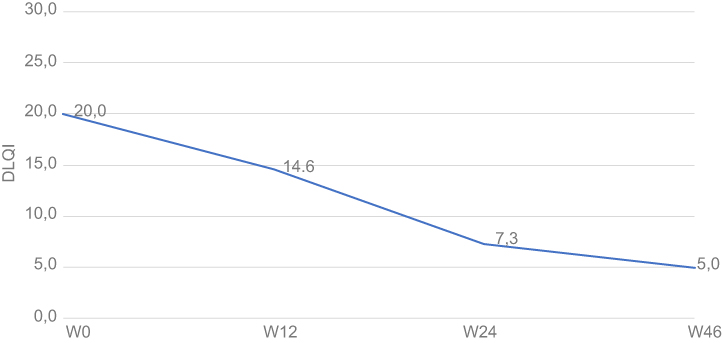 |
Figure 2 Trend of median DLQI score. DLQI median score decreased from a value of 20,0 at BL over 32 patients to 14.6 over 32 patients at W12, to a value of 7.3 over 25 patients at W24 and reduced to a value of 5.0 over 13 patients at W46. |
Discussion
This observational study investigated the effect of omalizumab administered to a population of patients simultaneously affected by CSU and cardiometabolic, oncologic, infectious, immunologic and psychiatric comorbidities. To our knowledge, this is the first real-life report regarding the use of this anti-IgE antibody in such “complex” patients.
Alongside with data reported in literature, we observed a very low discontinuation rate due to AEs (0.32%).17–19 No serious adverse events or case of anaphylaxis were reported in our cohort. In fact, data from RCTs and post-marketing surveillance showed that hypersensitivity reactions to the drug are infrequent and anaphylaxis is rare.20
In our cohort, two patients with a history of previous Hepatitis C Virus (HCV)-related hepatitis are successfully treated and their viral load did not change during therapy, suggesting that there is no risk of HCV exacerbation. The HCV infection did not seem to diminish the efficacy of omalizumab in this subset of patients. Only few cases of patients undergoing treatment with omalizumab with concurrent infection by hepatotropic virus, in particular, Hepatitis B Virus (HBV) and C virus, have been reported to date.21–23 In all patients, no side effects or infection worsening were documented, with concurrent substantial improvement of symptoms of asthma or urticaria. A decrease in the viral load was detected in a patient with active infection by HBV. A case of a patient with cytomegalic hepatitis treated with valganciclovir and omalizumab for CSU described remission of the infective symptoms and good control of CSU.24 These reports suggest that omalizumab is safe in terms of liver function.
In our cohort, we did not observe a higher incidence of viral infections during treatment with omalizumab. While a higher incidence of nasopharyngitis, influenza, upper respiratory tract infection in children treated with omalizumab has been reported in the literature, other authors observed a decrease in the duration of rhinovirus infections, viral shedding and risk of rhinovirus illnesses, hypothesizing a role of the anti-IgE agent in improving virus-induced IFN-alpha response.25–27
Although IgE blockade may theoretically impair the immune control of parasites, we did not report any case of parasitic infections. Our findings align with the overall low risk of parasitic infections reported in RCTs and in observational studies.28,29
One case of acute ischemic heart disease not leading to discontinuation was reported in our cohort. No patient reported bleeding or thrombosis. Only one patient, a post-menopausal female aged 54, interrupted the therapy because of an increase in arterial blood pressure 6 months after treatment. Bisoprolol was administered with good control of symptoms. On the other hand, our series includes other 9 patients with preexisting arterial hypertension, who underwent treatment with omalizumab without any complication or significant alteration of blood pressure value.
No data regarding cardiovascular and cerebrovascular adverse events (AEs) in patients treated with omalizumab for CSU are available to date. In a post-marketing observational study on asthma patients, a higher rate of cardiovascular and cerebrovascular serious AEs (arterial and venous thrombosis) was noticed compared to no-treated patients.30 A real-life retrospective analysis asthma patients treated with omalizumab for uncontrolled severe asthma reported one case of venous thrombosis not leading to discontinuation of therapy.29 Surveillance is advisable owing to the apparently very low frequency of these AEs. The higher incidence of arterial hypertension in asthma patients is well documented, as well as its association with obesity and the overall increased cardiovascular risk of patients affected by asthma.31–33 On the contrary, cardiovascular risk does not seem to be increased in patients affected by CSU.34
Our data-set included one patient with chronic renal failure (CRF). Regular laboratory, clinical and instrumental assessments did not show any significant modification. The patient obtained a satisfactory control of symptoms of CSU without any worsening of his general conditions.
Our series includes 7 patients with a history of previous cancer (see Table 1). All of them were regularly monitored with physical examination, blood and instrumental tests as recommended by their referral physicians. These patients had been monitored from BL for a medium range of 12 months, without any known neoplastic recurrence or progression. These results are consistent with literature data, showing that treatment with omalizumab was not associated with an increased risk of malignancies.35 Our findings may further support the idea that omalizumab treatment is safe also in patients with previous cancers, as it does not seem to increase the risk of relapse. Long-term real-life data on a larger population are needed in order to further confirm this hypothesis.
Two patients of our series were affected by both CSU and severe atopic dermatitis (AD). They were treated with methotrexate (15 mg/week) and concurrently started omalizumab treatment, with satisfying results. Observational studies of omalizumab for AD, in general, report more positive results compared to the RCTs.36 The interpretation of improvement as an effect of treatment should accommodate the fact that most patients with AD (75%) have a spontaneous remission of disease before adolescence.37 Thus, recommendation for use in clinical practice awaits evidence from larger randomized controlled trials.
Our patients affected by immunoallergic comorbidities reported improvement of symptoms related to their underlying condition, requiring lower doses of their medications.
Regarding psychiatric comorbidities, no specific assessment has been performed during treatment. However, we did not observe any worsening of clinical symptoms. From the other hand, DLQI of both patients who were affected or not by psychiatric comorbidities was significantly reduced during treatment with omalizumab, suggesting that mental health of CSU patients may benefit from the improvement of clinical symptoms.
Relevant limitations of our study are the small sample, the lack of controls and the relatively short period of follow-up (average 12 months). Observation of this cohort of patients over time may represent an interesting source of information about omalizumab safety profile. The main strength of our work is the heterogeneity of comorbidities affecting our population. These diseases are widely diffused in Western countries; however, safety data on affected patients are commonly not available from RCTs, owing to their exclusion criteria. Data from real-life observational studies therefore represent a valuable source of information for clinicians who have to deal with “complex” patients still needing treatment for CSU. In our study, we focused on the safety profile of omalizumab in such patients. Given the heterogeneity of comorbidities and related classes of medications, interactions between such drugs and omalizumab were not analyzed in our population. Investigating the possible drug interactions between omalizumab and other concomitant medications and the possible influence of the latter on the response to omalizumab represents a very fertile field for future research.
Conclusion
Our results suggest that omalizumab may be considered as a safe and well-tolerated therapeutic option even in patients affected by several comorbidities. Further analysis based on a larger cohort of patients and a longer period of treatment is required to confirm our preliminary observations.
Acknowledgment
The authors wish to thank Novartis Farma Italia for support in the publication of this manuscript and Dr Valeria Manuelli for proofreading.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Marzano AV, Pigatto P, Cristaudo A. Management of chronic spontaneous urticaria: practical parameters. G Ital Dermatol Venereol. 2015;150:237–246.
2. Zuberbier T, Aberer W, Asero R. The EAACI/GA 2 LEN/EDF/WAO guideline for the definition, classification, diagnosis, and management of urticaria: the 2013 revision and update. Allergy. 2014;69:868–887. doi:10.1111/all.12462
3. Balp -M-M, Vietri J, Tian H, Isherwood G. The impact of chronic urticaria from the patient’s perspective: a survey in five European countries. Patient - Patient-Centered Outcomes Res. 2015;8:551–558. doi:10.1007/s40271-015-0145-9
4. Maurer M, Ma D, Wei JF, et al. Unmet clinical needs in chronic spontaneous urticaria. A GA2LEN task force report1. Allergy. 2011;66:317–330. doi:10.1111/j.1398-9995.2011.02683.x
5. Maurer M, Church MK, Marsland AM, et al. Questions and answers in chronic urticaria: where do we stand and where do we go? J Eur Acad Dermatol Venereol. 2016;30:7–15. doi:10.1111/jdv.13695
6. Staubach P, Eckhardt-Henn A, Dechene M, et al. Quality of life in patients with chronic urticaria is differentially impaired and determined by psychiatric comorbidity. Br J Dermatol. 2006;154:294–298. doi:10.1111/bjd.2006.154.issue-2
7. Maurer M, Sofen H, Ortiz B, Kianifard F, Gabriel S, Bernstein JA. Positive impact of omalizumab on angioedema and quality of life in patients with refractory chronic idiopathic/spontaneous urticaria: analyses according to the presence or absence of angioedema. J Eur Acad Dermatol Venereol. 2017;31:1056–1063. doi:10.1111/jdv.2017.31.issue-6
8. Greaves MW. Chronic Urticaria. N Engl J Med. 1995;332:1767–1772. doi:10.1056/NEJM199506293322608
9. Altman K, Chang C. Pathogenic intracellular and autoimmune mechanisms in urticaria and angioedema. Clin Rev Allergy Immunol. 2013;45:47–62. doi:10.1007/s12016-012-8326-y
10. Beck L, Bernstein J, Maurer M. A review of international recommendations for the diagnosis and management of chronic urticaria. Acta Derm Venereol. 2017;97:
11. Chang TW, Chen C, Lin CJ. The potential pharmacologic mechanisms of Omalizumab in patients with chronic spontaneous urticaria. J Allergy Clin Immunol. 2015;135:337–342. doi:10.1016/j.jaci.2014.04.036
12. Zhao Z-T, Ji CM, Yu WJ Omalizumab for the treatment of chronic spontaneous urticaria: a meta-analysis of randomized clinical trials. J Allergy Clin Immunol. 2016;137:1742–1750.e4. doi:10.1016/j.jaci.2015.12.1342
13. Global initiative for asthma. Global strategy for asthma management and prevention; 2017Available from: www.ginasthma.com.
14. Kaplan A, Ledford D, Ashby M. Omalizumab in patients with symptomatic chronic idiopathic/spontaneous urticaria despite standard combination therapy. J Allergy Clin Immunol. 2013;132:
15. Maurer M, Rosén K, Hsieh HJ. Omalizumab for the treatment of chronic idiopathic or spontaneous urticaria. N Engl J Med. 2013;368:924–935. doi:10.1056/NEJMoa1215372
16. Saini SS, Bindslev-Jensen C, Maurer M. Efficacy and safety of omalizumab in patients with chronic idiopathic/spontaneous urticaria who remain symptomatic on H 1 antihistamines: a randomized, placebo-controlled study. J Invest Dermatol. 2015;135:67–75. doi:10.1038/jid.2014.306
17. Cazzola M, Camiciottoli G, Bonavia M. Italian real-life experience of omalizumab. Respir Med. 2010;104:1410–1416. doi:10.1016/j.rmed.2010.04.013
18. Cherrez-Ojeda I, Maurer M, Bernstein JA. Learnings from real-life experience of using omalizumab for chronic urticaria in Latin America. World Allergy Organ J. 2019;12:100011. doi:10.1016/j.waojou.2019.100011
19. Košnik M, Kopač P, Eržen R. Omalizumab in chronic urticaria: our experience and literature review. Acta Dermatovenerol Alp Pannonica Adriat. 2014;23:57–61. doi:10.15570/actaapa.2014.14
20. Cox L, Platts-Mills TA, Finegold Iet al. American academy of allergy, asthma & immunology.; american college of allergy, asthma and immunology. American academy of allergy, asthma &immunology/american college of allergy, asthma and immunology joint taskforce report on omalizumab-associated anaphylaxis. J Allergy Clin Immunol. 2007;120(6):1373e–1377e.
21. Antonicelli L, Stagnozzi G, Giuliodoro S. The safety of Omalizumab therapy in a patient with severe persistent allergic asthma and hepatitis C. Ann Allergy Asthma Immunol. 2009;103:269–270. doi:10.1016/S1081-1206(10)60194-9
22. Chicharro P, Rodríguez-Jiménez P, de Argila D. Efficacy and safety of omalizumab in a patient with chronic spontaneous urticaria and active hepatitis B virus infection. Actas Dermosifiliogr. 2017;108:383–384. doi:10.1016/j.ad.2016.10.005
23. Leiva-Salinas M, Francés L, Marin‐Cabanas I. Effectiveness and safety of omalizumab in a patient with chronic urticaria and hepatitis C. J Eur Acad Dermatol Venereol. 2015;29:1027–1028. doi:10.1111/jdv.12669
24. Gonçalves R, Valente C, Ferreira E, Serra JE, Da Cunha JS. Cytomegalic hepatitis in a patient receiving omalizumab. IDCases. 2016;5:83–84. doi:10.1016/j.idcr.2016.08.001
25. Odajima H, Ebisawa M, Nagakura T, et al. Long-term safety, efficacy, pharmacokinetics and pharmacodynamics of Omalizumab in children with severe uncontrolled asthma. Allergology Int. 2017;66:106–115. doi:10.1016/j.alit.2016.06.004
26. Esquivel A, Busse WW, Calatroni A. Effects of omalizumab on rhinovirus infections, illnesses, and exacerbations of asthma. Am J Respir Crit Care Med. 2017;196:985–992. doi:10.1164/rccm.201701-0120OC
27. Teach SJ, Kull S, Rennert S, et al. Preseasonal treatment with either Omalizumab or an inhaled corticosteroid boost to prevent fall asthma exacerbations. J Allergy Clin Immunol. 2015;136:1476–1485. doi:10.1016/j.jaci.2015.04.010
28. Cruz AA, Lima F, Sarinho E, et al. Safety of anti-immunoglobulin E therapy with Omalizumab in allergic patients at risk of geohelminth infection. Clin Exp Allergy. 2007;37:197–207. doi:10.1111/cea.2007.37.issue-2
29. Di Bona D, Fiorino I, Taurino M, et al. Long-term “real-life” safety of Omalizumab in patients with severe uncontrolled asthma: a nine-year study. Respir Med. 2017;130:55–60. doi:10.1016/j.rmed.2017.07.013
30. Iribarren C, Rahmaoui A, Long AA, et al. Cardiovascular and cerebrovascular events among patients receiving omalizumab: results from EXCELS, a prospective cohort study in moderate to severe asthma. J Allergy Clin Immunol. 2017;139:1489–1495.e5. doi:10.1016/j.jaci.2016.07.038
31. Chipps BE, Zeiger RS, Luskin AT. Baseline asthma burden, comorbidities, and biomarkers in omalizumab-treated patients in PROSPERO. Ann Allergy Asthma Immunol. 2017;119:524–532.e2. doi:10.1016/j.anai.2017.09.056
32. Ali Z, Ulrik CS. Obesity and asthma: a coincidence or a causal relationship? A systematic review. Respir Med. 2013;107:1287–1300. doi:10.1016/j.rmed.2013.03.019
33. Xu M, Xu J, Asthma YX. Risk of cardiovascular disease or all-cause mortality: a meta-analysis. Ann Saudi Med. 2017;37:99–105. doi:10.5144/0256-4947.2017.99
34. Egeberg A, Kofoed K, Gislason G, Vestergaard C, Thyssen J. Cardiovascular risk is not increased in patients with chronic urticaria: a retrospective population-based cohort study. Acta Derm Venereol. 2017;97:261–262. doi:10.2340/00015555-2516
35. Long A, Rahmaoui A, Rothman KJ, et al. Incidence of malignancy in patients with moderate-to-severe asthma treated with or without Omalizumab. J Allergy Clin Immunol. 2014;134:560–567.e4. doi:10.1016/j.jaci.2014.02.007
36. Holm JG, Agner T, Sand C, Thomsen SF. Omalizumab for atopic dermatitis: case series and a systematic review of the literature. Int J Dermatol. 2017;56:18–26. doi:10.1111/ijd.2017.56.issue-1
37. Thomsen SF. Atopic dermatitis: natural history, diagnosis, and treatment. ISRN Allergy. 2014;2014:1–7. doi:10.1155/2014/354250
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.