")
Back to Journals » Integrated Pharmacy Research and Practice » Volume 9
Medication Therapy Management: Current Challenges
Authors Ferreri SP , Hughes TD, Snyder ME
Received 11 December 2019
Accepted for publication 10 March 2020
Published 2 April 2020 Volume 2020:9 Pages 71—81
DOI https://doi.org/10.2147/IPRP.S179628
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Jonathan Ling
Stefanie P Ferreri,1 Tamera D Hughes,1 Margie E Snyder2
1UNC Eshelman School of Pharmacy, University of North Carolina at Chapel Hill, Chapel Hill, NC 27599-7574, USA; 2College of Pharmacy, Purdue University, Indianapolis, IN 46202, USA
Correspondence: Stefanie P Ferreri
Practice Advancement and Clinical Education, UNC Eshelman School of Pharmacy, 301 Pharmacy Lane, Chapel Hill, NC, 27599-7574, USA
Tel +1 919 843 9765
Fax +1 919 843 3861
Email [email protected]
Abstract: Medication therapy management (MTM) services have evolved as a means for pharmacists and other providers to assist patients and caregivers in improving therapeutic outcomes and reducing health care expenditures. More than a decade has passed since the Medicare Modernization Act of 2003 provided pharmacists with the opportunity to deliver MTM services to Medicare beneficiaries. MTM continues to offer pharmacists the opportunity to use their knowledge; yet, pharmacists have reported challenges with service delivery. Identifying the challenges that affect MTM services in pharmacy practice is necessary in order to seek improvement to MTM delivery. This narrative review explores the current challenges pharmacists face with MTM delivery, summarizes potential solutions for addressing challenges, and seeks to incite further debate, service reconfiguration, and ultimately service improvement of pharmacist-provided MTM services.
Keywords: community pharmacy services, community pharmacy, medication management, drug therapy management, pharmaceutical services
Introduction
Throughout the world, pharmacists provide “medication management services,”
spectrum of patient-centered, pharmacist-provided, collaborative services that focus on medication appropriateness, effectiveness, safety, and adherence with the goal of improving health outcomes.1,2
In the United Kingdom, pharmacists are contracted to perform “medicines use review” (MUR), a free service available to all patients. The purposes of MURs are to improve patients’ understanding of their medicines and adherence, particularly among those with chronic conditions, highlight problematic side effects and propose solutions where appropriate, and to reduce medicines wastage.3 Similarly, in Canada, pharmacist provides “medication management”, a comprehensive pharmacy service that helps optimize health outcomes and patients targeted medication outcomes. In Canada, this service is offered to residents taking at least one medication.4 Australia provides a similar model, “home medicines reviews”, whereby a pharmacist-conducts medication reviews in the community setting; however, it is government funded.5,6
In the United States, the passage of the Medicare Modernization Act (MMA) of 2003 provided a prescription drug benefit under Medicare Part D, which included the delivery of medication therapy management (MTM) services for eligible Medicare beneficiaries. This legislation created a new mechanism for health care professionals, including community pharmacists, to provide and to be compensated for these services. Consequently, a profession-wide consensus definition of MTM was created in 2005. The definition states that
MTM is a distinct service or group of services that optimize therapeutic outcomes for individual patients. MTM services are independent of, but can occur in conjunction with, the provision of a medication product.7
Although a consensus definition was created in the United States, little was done to provide a standardized implementation for the service. In response, the American Pharmacists Association (APhA) and the National Association of Chain Drug Stores (NACDS) Foundation created a framework titled, “Medication Therapy Management in Community Pharmacy Practice – Core Elements of an MTM Service (Version 1.0).8 However, when Part D implementation of MTM initiated in 2006 the regulations were open for interpretation and it was up to the prescription-drug plans (PDPs) to decide how the service was delivered (e.g. telephone, face-to-face, etc.) and who delivered the service (e.g. nurse, pharmacist, etc.).
Further development of the “Core Elements” model produced a second version in 2008. It incorporated input from an advisory panel. The goal of this revised document was to “improve continuity of care and patient outcomes” by achieving a maximum level of “effectiveness and efficiency of MTM service” across a variety of pharmacy practice settings. Although strides were taken to incorporate this framework into practice, its adoption was voluntary.9
Moreover, as authors have noted previously, outcomes from MTM services have been mixed.10 Since the enactment of the Act, a plethora of studies have found that MTM services effectively reduce potentially inappropriate medication use and medication nonadherence. However, a systematic review conducted in the last decade demonstrates substantial variation in performance across PDPs and PDPs have not proven that their MTM services improve patient outcomes or reduce health care expenditures.11 More recently, a review identified strategies used by community pharmacies to implement patient care services, including MTM.12 While Part D MTM delivery has grown to about 65% of plans utilizing community pharmacists through MTM vendor contracts, there continues to be the need to focus on challenges associated with this delivery.13 Many PDPs are not utilizing community pharmacists to be the primary provider for Part D MTM services. This paper explores the challenges associated with MTM implementation and delivery in community pharmacy settings.
Methods
This review was conducted with a focus on MTM delivery by community pharmacists. It employs a narrative review methodology. Narrative reviews provide a critical and objective analysis of the current knowledge on a topic and summarize patterns and trends in the literature to identify gaps or inconsistencies in a body of knowledge.14 Here we provide the most important and critical aspects of the current challenges community pharmacists face with MTM implementation and delivery.
Identifying Relevant Studies
The authors searched PubMed for articles using MeSH terms, title words and keyword synonyms. Figure 1 depicts the steps taken to identify pertinent literature and synthesize findings. Studies selected for further review were those that discussed challenges in MTM and met other inclusion criteria including a publication date from January 1, 2008 to September 25, 2019. This date was chosen because “medication therapy management” was introduced as a MeSH term in 2008. In addition to the 256 publications that were found in our search, we also reviewed bibliographies and included previously known landmark studies to gain information on the beginning stages of Part D MTM and its initial goals.
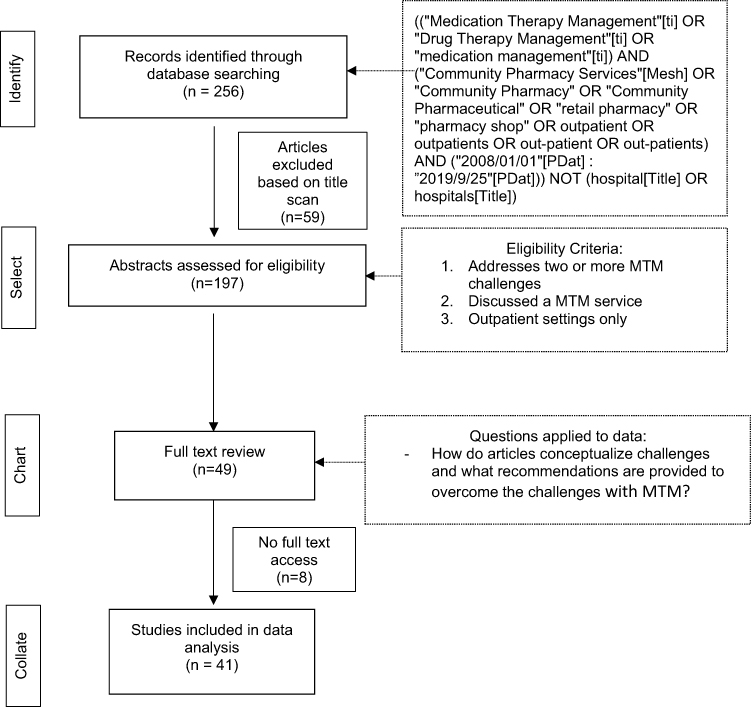 |
Figure 1 Methodology of Narrative Review. Abbreviations: PDat, Publication Date; MTM, medication therapy management. |
Selecting the (Relevant) Studies
All of the articles identified from the search were imported into a database displaying the title, PMID, author and abstract. Two researchers separately reviewed all article titles (S.P.F., T.D.H.) and applied the inclusion screening criteria to determine their eligibility for abstract review. Then, each researcher reviewed the abstracts selected for review and applied the following inclusion criteria: 1) focus on multiple MTM challenges; 2) involve MTM services 3) services performed in outpatient settings. The team reviewed the selected articles, discussed the findings, and resolved disagreements on study selection and data extraction by consensus and through discussion.
Charting the Data
We adopted a descriptive analytical approach to the included articles. To identify the current challenges’ community pharmacies face with MTM, we applied the following analytical question to our data/literature set: how do articles conceptualize challenges and what recommendations are provided to overcome the challenges with MTM?
Collating, Summarizing, and Reporting the Results
Articles were collated and examined for patterns.
Results
The narrative review identified 41 articles meeting inclusion criteria. Recurring barriers to MTM implementation were identified, with a focus on barriers related to implementation challenges for community pharmacists in the United States. Specifically, we identified challenges in the following areas: 1) integration of MTM within the pharmacy workflow; 2) integration of MTM within the health care team; 3) technology; 4) business model for MTM; and 5) patient engagement.
Integration of MTM Within the Pharmacy Workflow
While there is enthusiasm for the benefits of MTM, there are limited formal organizational and staffing structures within community pharmacies to support it. Literature suggests that guidance for MTM workflow is not clear. Pharmacies have struggled to identify whether MTM should be integrated as part of their regular dispensing workflow or if it should be a consult service separate from dispensing. Many US community pharmacists, regardless of receiving payment, have expressed great difficulty in implementing MTM within their current workflow.15 Similarly, a Canadian study found that MTM services have not expanded because relevant stakeholders did not consider how MTM would co-exist with current pharmacy workflow demands when the new service was introduced.16 The literature review points specifically to challenges with pharmacist attitudes, lack of time, lack of trained support personnel, excessive workload/lack of management support, and physical facilities (e.g. store layout, lack of privacy, overall lack of space).17
Many studies discussed the personal characteristics that influence pharmacist-provided MTM services.18 Pharmacies that have personnel that are adaptive to change have been successful integrating clinical services into workflow.18,19 The relationship between pharmacist’s attitudes and the provisions of patient care services has always merited further research and pharmacists job descriptions detailing this expanding role are also lacking.19,20
With regard to time constraints, both pharmacists as well as patients reported similar concerns.21 The challenges with not having enough time usually are tied to lack of pharmacy staff (89.6%) as well as inconsistencies with staffing.19,22 Pharmacies who have support from residents were able to implement MTM programs more easily than those without this staff support.18,23
Although an increase in technician hours is associated with an increase in successful MTM implementation, pharmacists’ attitudes towards technician engagement varies.19 Some pharmacists believe technicians do not have adequate training to be involved in MTM. Proper training for MTM integration is essential for delegation of clinical and technical roles.24 Because training is not consistent, there is resistance with assigning MTM responsibility to non-pharmacist staff.25 The lack of established roles and responsibilities lead to internal team dynamic obstacles. The literature suggests that the majority of the team dynamics obstacles in MTM surround the use of technicians. In fact, some of these barriers discourage technicians from supporting MTM. Confidence and trust are also recurring themes challenging technician involvement with MTM. Technicians are often not involved in the patient work up and some MTM software platforms do not allow technician login making it difficult for them to assist in the management of patient medications.25 Staff turnover for technicians also makes it difficult to have them involved in MTM. A pharmacy reported an increase difficulty in training technicians to do MTM because of staff turnover. Pharmacists who do train their technicians to support MTM described frustration with “bringing them up to speed, [but] then they leave, and I have to find somebody else”—making the MTM workload fall back on the pharmacist.24,25
Adding to these challenges is a lack of pharmacy management support. In a feasibility study, inadequate management support from pharmacy owners, corporate entities and pharmacy benefit managers was a challenge to delivery of MTM.26 Some owners and staff members are resistant to providing MTM. One study had pharmacists self-report challenges across services and identified strategies that management could use to incorporate change.27
The lack of adequate physical facilities has also affected the delivery of MTM services. Several studies highlighted the need for appropriate physical spaces for medication and disease state management services in community pharmacies.28,29 Some pharmacies stopped providing medication management service due to the lack of private space.27
Integration of MTM Within the Health Care Team
Lack of pharmacist integration with other members of the health care team was cited as a recurring challenge impacting MTM in all countries and a frustration to pharmacists.30,31 In the United States, community pharmacists typically operate in a “silo” and most MTM services are provided without full integration of the pharmacist as a member of the health care team.30
An Australian study reported that relationships, communication and teamwork affect the ability to implement MTM.27 Interdisciplinary teams are the solution for managing complex and challenging healthcare. However, in an already busy environment, communication between community pharmacists, community nurses and general practitioners is very difficult to achieve.32 Not having a standard process for pharmacists to report findings and make recommendations to prescribers was also found to be a barrier.33
In addition, integrating the pharmacist as a member of the team has been documented as challenging because other members of that team do not understand the pharmacist’s role beyond dispensing.20 Another study cited resistance by physicians or state medical associations as a barrier to pharmacy provided clinical services. The literature demonstrates that physicians see the expansion of pharmacist roles as a threat to their practice’s independence and autonomy.34 Older physicians simply want to stick to “their own system of evaluating things” and concerns regarding pharmacists’ clinical skills were unknown.21
Technology
A challenge that affects MTM delivery within the community pharmacy as well as across the health care continuum is technology. While access to medical records has been noted as an important driver in the success of MTM, integrating the pharmacist into the health information technology (HIT) infrastructure has been difficult and adoption of shared electronic health record (EHR) systems in community pharmacies has been minimal.22,35-37 Specifically, interoperability and bi-directionality of health information, pharmacy informatics development, and burdensome documentation were cited as barriers for MTM delivery.38 HIT has always posed challenges in healthcare simply due to the volume, velocity and variety of big data.39
Some companies have implemented corporate policies that prohibit providing MTM services through web-based vendors.38–40 This security concern presents a technological challenge. MTM vendors typically require contracted community pharmacists to utilize the vendor’s web-based propriety software portals for MTM documentation and billing. However, the use of MTM vendor web-based software platforms also creates other challenges. There is a lack of standardization across MTM vendor systems and, in many circumstances, a lack of interoperability with the pharmacy’s management system.40 The pharmacy management system or the information system is a system that stores data and enables functionality that organizes and maintains the medication use process within pharmacies. Moreover, pharmacists find it difficult to operate more than a few disparate billing and documentation systems, and pharmacy management systems may require pharmacists to document services in their management system and document payer/vendor-specific services in another.10,30,41
Business Model for MTM
While sustainable business models for MTM exist in the literature,42,43 evidence is limited. Widespread coverage of MTM services in the United States by payers beyond Part D does not exist. From a payer perspective, there are numerous barriers to pharmacist-delivered MTM. While Medicaid programs have been able to see the benefits, many private payers have yet to see value and compensate for these services.43 Several concerns were cited by healthcare executives that limit the reimbursement to pharmacies. These concerns include qualifications of pharmacists’, lack of physicians’ knowledge about pharmacists training, physician reluctance to partner with pharmacists, poorly developed population health models, lack of standardized fee structure, and an evolving business model.36 Moreover, even when services are covered by payers, low financial compensation is a significant barrier to MTM delivery.17 In addition, most commonly it is the pharmacies, not individual pharmacists, who receive reimbursement. Ambiguity and uneasiness amongst stakeholders surrounding the legality of billing for pharmacists’ services also exists.34 Collectively, low volume and low reimbursement make it difficult for many community pharmacies to make a business case for MTM delivery.44
Patient Engagement
Patients have also been cited as a barrier to MTM delivery. Lack of familiarity and limited expectations from the service, not being referred for MTM from physicians, and cost concerns were commonly cited as barriers.45 Literature cited that patients do not understand the expanding role of the community pharmacist in healthcare. Many consumers see pharmacists as only dispensers of medications, and not as healthcare professionals that collaborate with their physicians. Consequently, patients are satisfied with pharmacists’ traditional dispensing model and do not see the need for additional services.43 In one study, pharmacists agreed that their struggle with providing MTM is due to “patients’ perceptions of what we could do.”19 Pharmacists stated,
unfortunately, some of our patients just aren’t comfortable with the idea and others believe we are infiltrating their protected patient–provider relationship and counteracting or complicating the original therapeutic plan.34
This disconnect between patient expectations and the services their pharmacist provide was identified by Bislew and Sorensen to be largely the reason why patients lack interest in pharmacist services.46
In addition, limited studies demonstrated that patients were referred from physicians to pharmacists for MTM. In fact, most patients were unaware that pharmacists work with their physicians to make medication recommendations. One consumer stated, “I don’t believe there’s a relationship at all between the two of them.”43 Patients also expressed concern about the cost of the service. One study found that patients’ willingness to pay for MTM varied.47 Patients willingness to pay did not offset the cost therefore the service would not be sustainable to pharmacies.
Discussion
The barriers identified in this narrative review align with those noted in prior reviews and demonstrates that barriers to MTM implementation have persisted since Medicare Part D was implemented in 2006.10,15-19,21,22,25,26,30-36,40,41,43-48 More work is needed to overcome these challenges and produce consistently positive outcomes from MTM.48 The literature points to considerations for potential solutions for overcoming each of the identified challenges to MTM delivery and these are summarized below.
Considerations for Incorporating MTM into Pharmacy Workflow
Integration of MTM services into pharmacy workflow is essential for success. Three potential solutions to identified challenges are evident from the literature: 1) develop a standardized approach to MTM delivery that is followed regardless of payer; 2) offer MTM to all patients; and 3) define roles and responsibilities for personnel involved in MTM delivery.
MTM programs in Minnesota, Connecticut and Iowa have yielded positive results outside of Part D requirements. These programs have standardized elements that differ from current Part D MTM practices such as standardized documentation of MTM interventions, follow-up and tracking of patient’s progress toward clinical goals and standardized billing processes.49 In the Minnesota program, pharmacists take responsibility for all the medication-related outcomes of all patients. This program expands beyond the typical Part D requirements and pharmacists focus on the whole patient and optimizing their entire medication regimen.50
MTM was passed as legislature for Medicare patients, however in practice, community pharmacists care for more than Medicare patients. Incorporating MTM for some patients, but not all, and following different steps for patient identification and documentation depending on the payer potentiates challenges with integrating MTM into pharmacy practice. As a result of community pharmacists not incorporating Part D MTM into workflow, some PDPs are starting to increase the use on nonpharmacist providers.51 To succeed, strategies for establishing MTM services in community pharmacies must be patient-centered, collaborative, and aligned with the move toward value-based care for all patients.
Addressing inefficiencies among pharmacy personnel that improves MTM workflow has been cited as a potential solution.16,52,53 Members of the pharmacy staff must have clearly defined roles and responsibilities in MTM. Pharmacy technicians have been utilized to support MTM through assistance in medication reconciliation, making reminder phone calls, and assistance with service documentation.25 Standardized training for pharmacy technicians that delineates administrative support from pharmacists’ role of clinical decision-making could help pharmacists obtain greater efficiency in MTM delivery.54,55 Pilot studies demonstrating that the use of a tech-check-tech model for dispensing services frees up pharmacists so they can focus on clinical services.56 Similarly, exploring innovative models that allow technicians to focus on technical tasks related to MTM while pharmacists become integrated into team-based care for the clinical aspects of MTM could alleviate many of the workflow barriers in the pharmacy.
Considerations for Incorporating MTM into the Health Care Team
Successful integration of community pharmacists into team-based care is essential for optimizing MTM delivery. Two solutions for supporting integration could be considered: 1) cultivate informal and formal relationships between pharmacists and other healthcare professionals; and 2) encourage health information exchange/shared access to the EHR.
Studies demonstrate that healthcare professionals can successfully partner informally with community pharmacists,57–63 with the most successful physician–pharmacist relationships characterized by open communication, mutual trust, agreement on role specifications, and high-quality pharmacist contributions that are performed consistently and within a well-defined structure.64,65 A strong working relationship between pharmacists and prescribers is necessary to optimize healthcare for each patient.26,66,67
In addition to informal relationships, formal steps can be taken to enhance collaboration. For example, formal referral mechanisms can be created wherein patients who might otherwise not be eligible for MTM through their payer could receive covered services upon referral. Pharmacists and physicians could also utilize collaborative drug therapy management (CDTM) arrangements in order to improve communication and service efficiency by agreement on tasks pharmacists can complete independently (e.g., dose titration).68,69 These arrangements to support MTM delivery would improve relevance of the pharmacists’ services and likely improve provider trust as they are now truly working collaboratively. Several articles have published strategies for pharmacists and other health care providers to establish practice agreements.70–72
The authors are aware that full integration into the health care team is dependent on pharmacists’ access to the EHR. We will share more considerations in the technology section.
Building Sustainable Business Models for MTM
Because financial factors were commonly cited as a challenge to MTM service delivery, strategies for building a sustainable business model need to be considered. Aligning MTM with value-based care delivery through the development of payment models which reward positive outcomes needs to occur.73 Numerous strategies for better aligning incentives for all MTM stakeholders have been proposed in the literature.49,74 In addition, CMS is currently studying the impact of changes to the Medicare Part D MTM program, including new payment models, as part of the Enhanced MTM (EMTM) Program.75 Given the ongoing nature of the EMTM program, data regarding the effectiveness of these new payment models for MTM are unknown. Therefore, additional considerations for building sustainable business models for MTM should be explored once EMTM findings are available.
Considerations for Technology
At state and regional levels, changes have begun to lift barriers to health information exchange (HIE),76,77 however the change is slow. Three additional solutions to overcome MTM delivery barriers pertaining to technology could be considered: 1) create financial and other incentives to encourage EHR access for MTM delivery; 2) prevent payers from requiring the use of specific software systems for documentation and billing, and 3) designate common data capture points for MTM in the EHR.
Technology exists in community pharmacies to aid in dispensing. However, programs that allow pharmacists to communicate with local physicians and hospitals in HIE and give them access to local or regional EHRs is not common in community practice. Literature demonstrates that access to medical records for patients has resulted in more medication-related problems being identified and better continuity of care among providers.54,78 Technological enablers result in improved medication adherence, improved safety, better patient education, and coordinated care with other healthcare team members.79 Because of this, some pharmacies have been proactive and identified access to necessary HIT for their patients, including local practices’ electronic medical records (EMRs).54,80 Others have worked to develop successful communication protocols to optimize medications for patients62,81 and have begun exploring communicating with providers via Direct Secure Messaging within EMR systems.26 Payers of MTM services should continue to incentivize community pharmacies to gain access to HIE so patient outcomes can be optimized.
To reduce inefficiencies created by requiring pharmacists to use multiple software systems, payers of MTM services should accept MTM documentation completed in any system as long as specific common data elements are captured.10,82 Processes for this are starting to develop in community pharmacies such as the use of the e-care plan. These technological successes allow a pharmacist to have a single sign on gain access to bi-directional communication and allows the entire health care team to see the drug therapy problems identified.83
Considerations to Improve Patient Engagement in MTM
Strategies to engage the patient are critical as MTM services are tailored to improve patient adherence and reduce patient medication-related problems. MTM services have been available for more than a decade, yet participation by eligible patients continues to be lower than expected. Three solutions from the literature could be considered to change patient perceptions: 1) refine and improve patient-facing MTM materials; 2) Offer patients financial incentives, and 3) develop communication training for professionals involved in MTM delivery.
Results from a systematic review identified that there were a multitude of factors patients considered when selecting a pharmacy. A relationship with a respectful, friendly, competent pharmacist is important pharmacist-related attributes in the process of pharmacy selection. Important pharmacy-related attributes include cost, convenience, wait times. Availability of auto-refill service was also a frequently reported attribute in this review. However, the only medication management services rated high were medication safety (detecting drug interactions) on patients’ preferences.84 Findings from studies indicate that the public is unaware of MTM services; therefore, public health campaigns are needed to promote MTM.85 Providing patient with incentives, such as waived copays, has proven beneficial for MTM programs.86
In addition to public health campaigns and potential incentives, personalized dialogue about medication use can also assist with patient engagement.87 Proactive communication training for pharmacy personnel, including the use of scripts, can generate demand for services and improve acceptance.46,88-90 Improving patient satisfaction and information about MTM services provided by pharmacies needs to become common so the services are sold through word-of-mouth.91–93 There is a tremendous, untapped opportunity to improve patient expectations of community pharmacist-provided MTM services.
Conclusion
While positive outcomes have resulted from MTM, challenges in service delivery persist. In order for MTM to achieve consistent positive outcomes for patients’, these challenges must be recognized and mitigation strategies implemented. This paper identified several challenges described in the literature as well as potential solutions that could be considered by MTM stakeholders, including pharmacists, physicians, payers and patients.
Acknowledgments
The authors would like to thank Rebecca Carlson, MLS, for her recommendations for the literature search strategy and the methodology of this review.
Disclosure
Dr Snyder serves as a consultant to Westat, Inc. on an evaluation of the CMS enhanced MTM program, also reports personal fees from Westat, Inc. The authors report no other conflicts of interest in this work.
References
1. Gray C. Evolution of the medicare Part D medication therapy management program from inception in 2006 to the present. Am Health Drug Benefits. 2019;12(5):243.
2. Medication-management-services-definition-and-key-points-version-1.pdf. Available from: https://jcpp.net/wp-content/uploads/2018/05/Medication-Management-Services-Definition-and-Key-Points-Version-1.pdf.
3. Stewart D, Whittlesea C, Dhital R, Newbould L, McCambridge J. Community pharmacist led medication reviews in the UK: a scoping review of the medicines use review and the new medicine service literatures. Res Soc Adm Pharm. 2019. doi:10.1016/j.sapharm.2019.04.010
4. Henrich N, Tsao N, Gastonguay L, Lynd L, Marra CA. BC medication management project. Can Pharm J CPJ. 2015;148(2):90–100. doi:10.1177/1715163515569571
5. Chen TF. Pharmacist-led home medicines review and residential medication management review: the Australian model. Drugs Aging Auckl. 2016;33(3):199–204. doi:10.1007/s40266-016-0357-2
6. Zagaria MAE, Chris Alderman. Community-based medication management in the U.S. and Australia. Available from: https://www.uspharmacist.com/article/community-based-medication-management-in-the-us-and-australia.
7. Bluml BM. Definition of medication therapy management: development of profession wide consensus. JAPhA. 2005;45(5):566–572. doi:10.1331/1544345055001274
8. American Pharmacists Association. National Association of Chain Drug Stores Foundation. Medication therapy management in community pharmacy practice: core elements of an MTM service (version 1.0). JAPhA. 2005;45(5):573–579. doi:10.1331/1544345055001256.
9. American Pharmacists Association. National Association of Chain Drug Stores Foundation. Medication therapy management in pharmacy practice: core elements of an MTM service model (version 2.0). JAPhA. 2008;48(3):341–353. doi:10.1331/JAPhA.2008.08514.
10. Snyder ME, Jaynes HA, Gernant SA, Lantaff WM, Hudmon KS, Doucette WR. Variation in medication therapy management delivery: implications for health care policy. J Manag Care Spec Pharm. 2018;24(9):896–902. doi:10.18553/jmcp.2018.24.9.896
11. Olinger L, Fair S, Mercincavage L, Stratos S Daniella Perlroth Grecia Marrufo Alejandro Montesinos Catherine Lewis Anjali Dixit Bingbing Li Emil Rusev Ekta Ghimire Michael Packard.:242.
12. Bacci JL, Bigham KA, Dillon‐Sumner L, et al. Community pharmacist patient care services: a systematic review of approaches used for implementation and evaluation. JACCP. 2019;2(4):423–432. doi:10.1002/jac5.1136
13. Adeoye OA, Farley JF, Coe AB, et al. Medication therapy management delivery by community pharmacists: insights from a national sample of medicare Part D beneficiaries. JACCP. 2019;2(4):373–382. doi:10.1002/jac5.1160
14. Onwuegbuzie AJ. 7 Steps to a Comprehensive Literature Review: A Multimodal & Cultural Approach. London: SAGE Publications; 2016.
15. Smith MG, Ferreri SP, Brown P, Wines K, Shea CM, Pfeiffenberger TM. Implementing an integrated care management program in community pharmacies: a focus on medication management services. J Am Pharm Assoc. 2017;57(2):229–235.e1. doi:10.1016/j.japh.2016.12.074
16. Houle SKD, Charrois TL, Faruquee CF, Tsuyuki RT, Rosenthal MM. A randomized controlled study of practice facilitation to improve the provision of medication management services in Alberta community pharmacies. Res Soc Adm Pharm. 2017;13(2):339–348. doi:10.1016/j.sapharm.2016.02.013
17. Blake KB, Madhavan SS, Scott VG, Meredith Elswick BL. Medication therapy management services in West Virginia: pharmacists’ perceptions of educational and training needs. RSAP. 2009;5(2):182–188. doi:10.1016/j.sapharm.2008.06.003
18. Smith MG, Shea CM, Brown P, Wines K, Farley JF, Ferreri SP. Pharmacy characteristics associated with the provision of medication management services within an integrated care management program. JAPhA. 2017;57(2):217–221.e1. doi:10.1016/j.japh.2016.12.073
19. Adeoye OA, Lake LM, Lourens SG, Morris RE, Snyder ME. What predicts medication therapy management completion rates? The role of community pharmacy staff characteristics and beliefs about medication therapy management. JAPhA. 2018;58(4S):S7–S15.e5. doi:10.1016/j.japh.2018.03.001
20. Jorgenson D, Dalton D, Farrell B, Tsuyuki RT, Dolovich L. Guidelines for pharmacists integrating into primary care teams. Can Pharm J CPJ. 2013;146(6):342–352. doi:10.1177/1715163513504528
21. Leung HY, Saini B, Ritchie HE. Medications and pregnancy: the role of community pharmacists - a descriptive study. PLoS One. 2018;13(5):e0195101. doi:10.1371/journal.pone.0195101
22. Lounsbery JL, Green CG, Bennett MS, Pedersen CA. Evaluation of pharmacists’ barriers to the implementation of medication therapy management services. JAPhA. 2009;49(1):51–58. doi:10.1331/JAPhA.2009.017158
23. Branham AR, Katz AJ, Moose JS, Ferreri SP, Farley JF, Marciniak MW. Retrospective analysis of estimated cost avoidance following pharmacist-provided medication therapy management services. J Pharm Pract. 2013;26(4):420–427. doi:10.1177/0897190012465992
24. Burnside TPT, Scott NJ, Smith MG. Implementation of technician driven medication therapy management program in community pharmacies. J Am Pharm Assoc. 2019;59(4):S156–S160.e2. doi:10.1016/j.japh.2019.06.014
25. Hohmeier KC, McDonough SLK, Rein LJ, Brookhart AL, Gibson ML, Powers MF. Exploring the expanded role of the pharmacy technician in medication therapy management service implementation in the community pharmacy. JAPhA. 2019;59(2):187–194. doi:10.1016/j.japh.2018.11.006
26. Isetts B. Integrating Medication Therapy Management (MTM) services provided by community pharmacists into a community-based Accountable Care Organization (ACO). Pharm Basel Switz. 2017;5:4. doi:10.3390/pharmacy5040056
27. Hattingh HL, Kelly F, Fowler J, Wheeler AJ. Implementation of a mental health medication management intervention in Australian community pharmacies: facilitators and challenges. RSAP. 2017;13(5):969–979. doi:10.1016/j.sapharm.2017.05.017
28. Domiati S, Sacre H, Lahoud N, Sili G, Salameh P. Knowledge of and readiness for medication therapy management among community pharmacists in Lebanon. Int J Clin Pharm. 2018;40(5):1165–1174. doi:10.1007/s11096-018-0666-0
29. Hattingh HL, Emmerton L, Ng Cheong Tin P, Green C. Utilization of community pharmacy space to enhance privacy: a qualitative study. Health Expect Int J Public Particip Health Care Health Policy. 2016;19(5):1098–1110. doi:10.1111/hex.12401
30. Smith MA, Spiggle S, McConnell B. Strategies for community-based medication management services in value-based health plans. Res Soc Adm Pharm. 2017;13(1):48–62. doi:10.1016/j.sapharm.2016.01.005
31. Redmond P, Carroll H, Grimes T, et al. GPs’ and community pharmacists’ opinions on medication management at transitions of care in Ireland. Fam Pract. 2016;33(2):172–178. doi:10.1093/fampra/cmw006
32. Lee CY, Goeman D, Beanland C, Elliott RA. Challenges and barriers associated with medication management for home nursing clients in Australia: a qualitative study combining the perspectives of community nurses, community pharmacists and GPs. Fam Pract. 2019;36(3):332–342. doi:10.1093/fampra/cmy073
33. Michaels NM, Jenkins GF, Pruss DL, Heidrick JE, Ferreri SP. Retrospective analysis of community pharmacists’ recommendations in the North Carolina Medicaid medication therapy management program. JAPhA. 2010;50(3):347–353. doi:10.1331/JAPhA.2010.09021
34. Tewksbury A, Bozymski KM, Ruekert L, Lum C, Cunningham E, Covington F. Development of collaborative drug therapy management and clinical pharmacy services in an outpatient psychiatric clinic. J Pharm Pract. 2018;31(3):272–278. doi:10.1177/0897190017710521
35. Haga SB, Allen LaPointe NM, Moaddeb J. Challenges to integrating pharmacogenetic testing into medication therapy management. J Manag Care Spec Pharm. 2015;21(4):346–352. doi:10.18553/jmcp.2015.21.4.346
36. Maidment ID, Aston L, Moutela T, Fox CG, Hilton A. A qualitative study exploring medication management in people with dementia living in the community and the potential role of the community pharmacist. Health Expect Int J Public Particip Health Care Health Policy. 2017;20(5):929–942. doi:10.1111/hex.12534
37. Bosworth HB, Zullig LL, Mendys P, et al. Health information technology: meaningful use and next steps to improving electronic facilitation of medication adherence. JMIR Med Inform. 2016;4(1):e9. doi:10.2196/medinform.4326
38. Newsome J. Virtual medication therapy management: the cornerstone to a pharmacy renaissance. JAPhA. 2013;53(2):159–162. doi:10.1331/JAPhA.2013.12188
39. Ma C, Smith HW, Chu C, Juarez DT. Big data in pharmacy practice: current use, challenges, and the future. Int Pharm Res Pract. 2015;4:91. doi:10.2147/IPRP.S55862.
40. Turner K, Renfro C, Ferreri S, Roberts K, Pfeiffenberger T, Shea CM. Supporting community pharmacies with implementation of a web-based medication management application. Appl Clin Inform. 2018;9(2):391–402. doi:10.1055/s-0038-1651488
41. Millonig MK. Mapping the route to medication therapy management documentation and billing standardization and interoperabilility within the health care system: meeting proceedings. JAPhA. 2009;49(3):372–382. doi:10.1331/JAPhA.2008.09518
42. Isetts BJ, Schondelmeyer SW, Artz MB, et al. Clinical and economic outcomes of medication therapy management services: the Minnesota experience. J Am Pharm Assoc. 2008;48(2):203–214. doi:10.1331/JAPhA.2008.07108
43. Smith M, Cannon-Breland ML, Spiggle S. Consumer, physician, and payer perspectives on primary care medication management services with a shared resource pharmacists network. RSAP. 2014;10(3):539–553. doi:10.1016/j.sapharm.2013.08.003
44. Rosenquist A, Best BM, Miller TA, Gilmer TP, Hirsch JD. Medication therapy management services in community pharmacy: a pilot programme in HIV specialty pharmacies. J Eval Clin Pract. 2010;16(6):1142–1146. doi:10.1111/j.1365-2753.2009.01283.x
45. Schnur ES, Adams AJ, Klepser DG, Doucette WR, Scott DM, PCMHs A. medication management: lessons learned from early research partnerships. J Manag Care Pharm JMCP. 2014;20(2):201–205. doi:10.18553/jmcp.2014.20.2.201
46. Garcia GM, Snyder ME, McGrath SH, Smith RB, McGivney MS. Generating demand for pharmacist-provided medication therapy management: identifying patient-preferred marketing strategies. JAPhA. 2009;49(5):611–616. doi:10.1331/JAPhA.2009.08089
47. Hong SH, Liu J, Wang J, Brown L, White-Means S. Conjoint analysis of patient preferences on Medicare medication therapy management. JAPhA. 2011;51(3):378–387. doi:10.1331/JAPhA.2011.10039
48. Blake KB, Madhavan SS. Perceived barriers to provision of medication therapy management services (MTMS) and the likelihood of a pharmacist to work in a pharmacy that provides MTMS. Ann Pharmacother. 2010;44(3):424–431. doi:10.1345/aph.1M386
49. Rucker NL. Medicare Part D’s Medication Therapy Management: Shifting from Neutral to Drive. AARP Public Policy Institute. 2012; 12.
50. Balick R. Patients cheer a Minnesota-based MTM program. Pharm Today. 2018;24(3):46–47. doi:10.1016/j.ptdy.2018.02.029
51. Pestka DL, Zillich AJ, Coe AB, et al. Nationwide estimates of medication therapy management delivery under the Medicare prescription drug benefit. JAPhA. 2020. doi:10.1016/j.japh.2019.12.002
52. Turner K, Weinberger M, Renfro C, et al. Stages of change: moving community pharmacies from a drug dispensing to population health management model. MCRR. 2019;2019:1077558719841159. doi:10.1177/1077558719841159.
53. Angelo LB, Ferreri SP. Assessment of workflow redesign in community pharmacy. JAPhA. 2005;45(2):145–150. doi:10.1331/1544345053623474
54. Gernant SA, Zillich AJ, Snyder ME. Access to medical records’ impact on community pharmacist–delivered medication therapy management: a pilot from the medication safety research network of indiana (Rx-SafeNet). J Pharm Pract. 2018;31(6):642–650. doi:10.1177/0897190017735422
55. Renfro CP, Turner K, Desai R, Counts J, Shea CM, Ferreri SP. Implementation process for comprehensive medication review in the community pharmacy setting. JAPhA. 2019;59(6):836–841.e2. doi:10.1016/j.japh.2019.07.007
56. Timothy P, Frost, Adams AJ. Pharmacist and technician perceptions of tech-check-tech in community pharmacy practice settings. J Pharm Pract. 2018;31(2):190–194.
57. Isasi F, Krofah E The expanding role of pharmacists in a transformed health care system - center for pharmacy practice accreditation. Available from: https://www.pharmacypracticeaccredit.org/resources/the-expanding-role-of-pharmacists-in-a-transformed-health-care-system. Accessed November 16, 2019.
58. Smith M, Bates DW, Bodenheimer T, Cleary PD. Why pharmacists belong in the medical home. Health Aff (Millwood). 2010;29(5):906–913. doi:10.1377/hlthaff.2010.0209
59. Pringle JL, Boyer A, Conklin MH, McCullough JW, Aldridge A. The Pennsylvania Project: pharmacist intervention improved medication adherence and reduced health care costs. Health Aff Proj Hope. 2014;33(8):1444–1452. doi:10.1377/hlthaff.2013.1398
60. Luder HR, Shannon P, Kirby J, Frede SM. Community pharmacist collaboration with a patient-centered medical home: establishment of a patient-centered medical neighborhood and payment model. JAPhA. 2018;58(1):44–50. doi:10.1016/j.japh.2017.10.006
61. Ferreri SP. Strategies to set up shared EHR use between community pharmacies and primary care practices. Pharm Today. 2018;24(4):41. doi:10.1016/j.ptdy.2018.03.026
62. Turner K, Weinberger M, Renfro C, et al. The role of network ties to support implementation of a community pharmacy enhanced services network. RSAP. 2019;15(9):1118–1125. doi:10.1016/j.sapharm.2018.09.015
63. Pezzino NC, Marciniak MW, Smith MG, Ferreri SP. Physician-reported factors that encourage collaboration with community pharmacists. JAPhA. 2017;57(3S):S279–S283.e2. doi:10.1016/j.japh.2017.02.016
64. Snyder ME, Zillich AJ, Primack BA, et al. Exploring successful community pharmacist-physician collaborative working relationships using mixed methods. RSAP. 2010;6(4):307–323. doi:10.1016/j.sapharm.2009.11.008
65. Fay AE, Ferreri SP, Shepherd G, Lundeen K, Tong GL, Pfeiffenberger T. Care team perspectives on community pharmacy enhanced services. JAPhA. 2018;58(4S):S83–S88.e3. doi:10.1016/j.japh.2018.05.009
66. Smith MG, Ferreri SP. A model to inform community pharmacy’s collaboration in outpatient care. RSAP. 2016;12(3):529–534. doi:10.1016/j.sapharm.2015.07.005
67. Vink J, Morton D, Ferreri S. Pharmacist identification of medication-related problems in the home care setting. Consult Pharm J Am Soc Consult Pharm. 2011;26(7):477–484. doi:10.4140/TCP.n.2011.477
68. Snyder ME, Earl TR, Gilchrist S, et al. Collaborative drug therapy management: case studies of three community-based models of care. Prev Chronic Dis. 2015;12. doi:10.5888/pcd12.140504.
69. Hammond RW, Schwartz AH, Campbell MJ, et al. Collaborative drug therapy management by pharmacists—2003. Pharmacother J Hum Pharmacol Drug Ther. 2003;23(9):1210–1225. doi:10.1592/phco.23.10.1210.32752
70. Bacci JL, Coley KC, McGrath K, Abraham O, Adams AJ, McGivney MS. Strategies to facilitate the implementation of collaborative practice agreements in chain community pharmacies. JAPhA. 2016;56(3):257–265.e2. doi:10.1016/j.japh.2016.02.014
71. Glenn ZM, Mahdavian SL, Woodard TJ. Preparing to provide MTM services. J Pharm Pract. 2015;28(1):6–9. doi:10.1177/0897190014562349
72. Funk KA, Weaver KK. Team work and collaborative practice agreements among pharmacists and nurse practitioners. JAPhA. 2018;58(1):117–119. doi:10.1016/j.japh.2017.10.016
73. Farley JF, Ferreri SP, Easter JC, McClurg MR. The North Carolina experiment: active research in the development and assessment of new practice models. N C Med J. 2017;78(3):186–190. doi:10.18043/ncm.78.3.186
74. Armistead LT, Ferreri SP. Improving value through community pharmacy partnerships. Popul Health Manag. 2019;22(1):5–8. doi:10.1089/pop.2018.0040
75. Was this helpful? Available from: https://cmmicoordinator.survey.fm/was-this-helpful?iframe=https%3A%2F%2Finnovation.cms.gov%2Finitiatives%2Fenhancedmtm%2F&ft=1.
76. DeBenedette V. Health information technology in the community pharmacy. Drug Topics. Available from https://www.drugtopics.com/chains-business/health-information-technology-community-pharmacy.
77. Bonner L. Pharmacists inch closer to accessing EHRs and HIEs. Pharm Today. 2016;22(5):44–47. doi:10.1016/j.ptdy.2016.04.031
78. Mantzourani E, Way CM, Hodson KL. Does an integrated information technology system provide support for community pharmacists undertaking discharge medicines reviews? An exploratory study. Integr Pharm Res Pract. 2017;6:145–156. doi:10.2147/IPRP.S133273
79. Figge HLF. CLSSS Senior Sales Strategy Consultant, AllscriptsMysis Chairman, Task Force for Education and Publications Pharmacy Informatics Section, American Society of Health-System Pharmacists Clifton Park, New. Using Technological Reducing Medication Errors Innovations. 2019;11. Available from: https://www.uspharmacist.com/article/reducing-medication-errors-using-technological-innovations-12633.
80. Fuji KT, Gait KA, Siracuse MV, Christoffersen JS. Electronic health record adoption and use by Nebraska pharmacists. Perspect Health Inf Manag AHIMA. 2011;8(Summer).
81. Renfro CP, Ferreri S, Barber TG, Foley S. Development of a communication strategy to increase interprofessional collaboration in the outpatient setting. Pharm Basel Switz. 2018;6:1. doi:10.3390/pharmacy6010004
82. Schafer KM, Gionfriddo MR, Boehm DH. Shared decision making and medication therapy management with the use of an interactive template. JAPhA. 2016;56(2):166–172. doi:10.1016/j.japh.2015.12.013
83. Health information technology in the community pharmacy. Drug Topics. Published 2016. https://www.drugtopics.com/drug-topics/news/health-information-technology-community-pharmacy.
84. Patel PM, Vaidya V, Osundina F, Comoe DA. Determining patient preferences of community pharmacy attributes: a systematic review. JAPhA. 2019. doi:10.1016/j.japh.2019.10.008
85. Taylor AM, Axon DR, Campbell P, et al. What patients know about services to help manage chronic diseases and medications: findings from focus groups on medication therapy management. J Manag Care Spec Pharm. 2018;24(9):904–910. doi:10.18553/jmcp.2018.24.9.904
86. Tomaszewski D, Cernohous T, Vaidyanathan R. Evaluating patient preferences for different incentive programs to optimize pharmacist-provided patient care program enrollment. J Manag Care Spec Pharm. 2017;23(11):1140–1147. doi:10.18553/jmcp.2017.23.11.1140
87. Shimp LA, Kucukarslan SN, Elder J, et al. Employer-based patient-centered medication therapy management program: evidence and recommendations for future programs. JAPhA. 2012;52(6):768–776. doi:10.1331/JAPhA.2012.11186
88. Miguel A, Hall A, Liu W, et al. Improving comprehensive medication review acceptance by using a standardized recruitment script: a randomized control trial. J Manag Care Spec Pharm. 2017;23(1):13–21. doi:10.18553/jmcp.2017.23.1.13
89. Denvir PM, Cardone KE, Parker WM, Cerulli J. How do I say that?”: using communication principles to enhance medication therapy management instruction. Curr Pharm Teach Learn. 2018;10(2):185–194. doi:10.1016/j.cptl.2017.10.014
90. Angelo LB, Christensen DB, Ferreri SP. Impact of community pharmacy automation on workflow, workload, and patient interaction. JAPhA. 2005;45(2):138–144. doi:10.1331/1544345053623537
91. Nicole Brandt P. Evolution of the medicare Part D medication therapy management program from inception in 2006 to the present. 2019. Available from: http://www.ahdbonline.com/issues/2019/september-2019-vol-12-no-5/2844-evolution-of-the-medicare-part-d-medication-therapy-management-program-from-inception-in-2006-to-the-present.
92. Tong Z, Cooke CE, Brandt NJ. Online provision of Part D medication therapy management program information. J Manag Care Spec Pharm. 2019;25(8):898–903. doi:10.18553/jmcp.2019.25.8.898
93. Brandt NJ, Cooke CE, Sharma K, et al. Findings from a national survey of medicare beneficiary perspectives on the medicare Part D medication therapy management standardized format. J Manag Care Spec Pharm. 2019;25(3):366–391. doi:10.18553/jmcp.2019.25.3.366
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.