")
Back to Journals » Clinical Interventions in Aging » Volume 15
Medical Students’ and Internal Medicine Trainees’ Knowledge of Drug Prescribing Recommendations in Older Patients with Impaired Kidney Function
Authors Deskur-Smielecka E, Kotlinska-Lemieszek A, Kropinska S , Wieczorowska-Tobis K
Received 17 September 2019
Accepted for publication 5 December 2019
Published 15 January 2020 Volume 2020:15 Pages 53—60
DOI https://doi.org/10.2147/CIA.S231330
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Richard Walker
Ewa Deskur-Smielecka, 1, 2 Aleksandra Kotlinska-Lemieszek, 1, 2 Sylwia Kropinska, 1 Katarzyna Wieczorowska-Tobis 1, 2
1Chair and Department of Palliative Medicine, Poznan University of Medical Sciences, Poznan, Poland; 2Palliative Medicine Unit, University Hospital of Lord’s Transfiguration, Poznan, Poland
Correspondence: Ewa Deskur-Smielecka
Chair and Department of Palliative Medicine, Poznan University of Medical Sciences, Osiedle Rusa 55, Poznań 61-245, Poland
Tel/Fax +48 61 8738303
Email [email protected]
Background: Numerous medications used in older adults require dose modification or should be avoided in individuals with impaired kidney function.
Purpose: To assess medical students’ and physicians’ knowledge of drug prescribing recommendations in older patients with estimated glomerular filtration rate (eGFR) < 30 mL/min/1.73m 2.
Patients and Methods: A survey comprising a list of 64 drugs conducted in 183 medical students (Students), and 138 post-graduate trainees in internal medicine (Physicians). The respondents were asked to classify each drug into one of three categories: 1) no renal precautions; 2) dose should be reduced; and 3) medication should be avoided.
Results: A range of 16.9– 68.3% students and 14.5– 81.2% physicians correctly classified drugs in the category “No renal precautions.” Drugs requiring dose reduction were correctly classified by 6– 67.2% students, and 24.6– 85.5% physicians. For drugs that should be avoided in subjects with eGFR < 30 mL/min/1.73m 2, the range was 6– 44.8% in the Students, and 8.7– 76.1% in the Physicians. The Physicians did better than the Students by classifying five drugs that do not require renal precautions, 12 drugs requiring dose reduction, and six medications that should be avoided. The Students had a higher percentage of correct answers for seven drugs in the category “no renal precautions,” and one drug requiring dose reduction.
Conclusion: Medical students and post-graduate trainees in internal medicine have poor knowledge of drug prescribing recommendations in older patients with renal impairment.
Keywords: older, chronic kidney disease, reduced glomerular filtration rate, drug dosing, knowledge
Introduction
Chronic kidney disease (CKD) is a common health problem in older subjects. It is defined as abnormalities in kidney structure or function, present for > 3 months, with implications for health.1 Although questionable, it is usually diagnosed based on decreased estimated glomerular filtration rate (eGFR) in clinical practice. The prevalence of CKD defined as eGFR < 60 mL/min/1.73m2 in the older generation is generally high, but varies greatly (11–37%) depending on the population assessed and the method of GFR estimation used.2–5
Numerous medications commonly used in older adults require dose modification or should be avoided in individuals with impaired kidney function due to increased risk of drug accumulation and dose-related adverse reactions, or their potential nephrotoxicity.6–10 Patients with renal impairment are at higher risk of medication side-effects,11 often resulting from errors in drug prescribing.12 Inappropriate prescription of drugs that require dose modification or that should be avoided in older subjects with renal impairment has been reported as a common problem, ranging from 9 to 67% in hospitalized patients,13–18 and from 1 to 37% in an outpatient setting.19 The prevalence of potentially inappropriate drug use in the Polish national population-based study PolSenior was particularly high, reaching 40% in subjects with eGFR < 60 mL/min/1.73m2.20 In those with more advanced kidney disease (eGFR < 30 mL/min/1.73m2) it was even higher, reaching 58%.20
As older patients usually receive care from general physicians and specialists other than geriatricians and nephrologists, it is important that all graduates in medicine have adequate knowledge about dose adjustment recommendations in subjects with impaired renal function. The aim of the study was to assess the knowledge of medical students and post-graduate trainees in internal medicine with regard to drug prescribing recommendations in older patients with impaired kidney function defined as eGFR < 30 mL/min/1.73m2.
Materials and Methods
We conducted a cross-sectional survey to assess knowledge of drug prescribing recommendations in older patients with eGFR < 30 mL/min/1.73m2 in two groups of respondents: 1) medical students at the Poznan University of Medical Sciences (Students); and 2) post-graduate trainees in internal medicine (Physicians). The pre-graduate education in medicine lasts 6 years. The questionnaires were filled out by the 4th year students at the beginning of clinical training in geriatrics. All students had completed a pharmacology course, and a clinical training in internal medicine earlier in the program of education. The physicians filled the questionnaires in during a course organized by our department as an obligatory part of a 3-year post-graduate training in internal medicine. Physicians from the whole country were enrolled to the course.
The questionnaire comprised a list of 64 drugs commonly used in older patients, 45 of which require dose adjustment or should be avoided in subjects with eGFR < 30 mL/min/1.73m2. Drugs were divided into 11 groups: diuretics (5 drugs), cardiovascular (9 drugs), antithrombotic (4 drugs), neuropsychotropic (17 drugs), analgesics (5 drugs), antirheumatic (3 drugs), gastrointestinal (5 drugs), antibiotic/antiviral (9 drugs), antidiabetic (2 drugs), antiallergic (3 drugs), and antiosteoporotic (2 drugs). The questionnaire comprised three possible responses to each medication: 1) does not need any renal precautions; 2) dose should be reduced; and 3) should be avoided. If a respondent did not choose any option, it was interpreted as “I do not know.” The selection of drugs for analysis and recommendations on prescription modifications were based on guidelines from the American Geriatrics Society 2015 Beers Criteria Update Expert Panel,8 the 2019 American Geriatrics Society Beers Criteria Update Expert Panel,9 and the Consensus Guidelines for Oral Dosing of Primarily Renally Cleared Medications in Older Adults by Hanlon et al.10 Additionally, several medications were analyzed based on information given in The Renal Drug Handbook by Ashley and Dunleavy.7 Only drugs registered in Poland were assessed. The list of drugs and recommendations for their use in subjects with estimated glomerular filtration rate < 30 mL/min/1.73m2 is shown in Table 1. Respondents were not allowed to use any mobile or computer-based dose-adjusting systems. Percentage of correct answers (“no renal precautions,” “dose reduction” and “avoid”) was calculated for each medication. As prescribing recommendations may vary between sources, we additionally analyzed combined category “drugs with renal recommendations” (“dose reduction” + “avoid”) to assess “renal awareness.” Percentage of correct answers in both groups of respondents was compared with the chi2 test with Yates correction (if appropriate). Statistical analysis was performed with StatSoft Statistica v12. P value < 0.05 was considered significant.
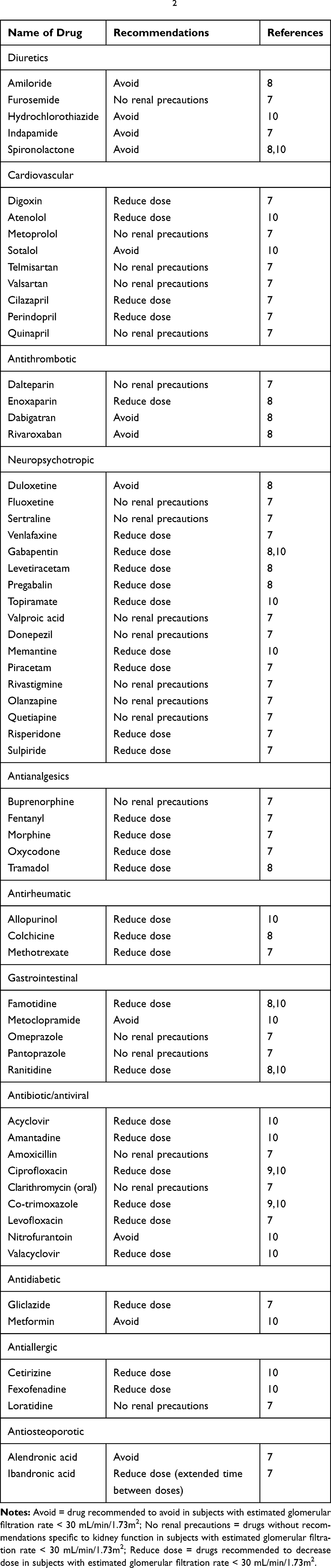 |
Table 1 List of Drugs Chosen for Analysis and Prescription Recommendations in Patients with Estimated Glomerular Filtration Rate < 30 mL/min/1.73m2 |
The study did not meet the criterion of medical experiment, thus the approval of the Institutional Bioethical Committee was not required. All participants provided verbal informed consent. All responses were anonymous.
Results
Overall, 138 physicians and 183 medical students completed the questionnaire. Detailed data on students’ and physicians’ responses are shown in Table 2. For clarity, percentage was shown for correct answers only. The percentage of correct answers “No renal precautions” ranged from 16.9% (fluoxetine) to 68.3% (pantoprazole) in the students and from 14.5% (valproic acid and dalteparin) to 81.2% (pantoprazole) in the physicians. The percentage of correct classifications of drugs requiring dose reduction ranged from 6% (rivaroxaban) to 67.2% (ciprofloxacin) in the students, and from 24.6% (ranitidine) to 85.5% (ciprofloxacin) in the physicians. For drugs that should be avoided in subjects with eGFR < 30 mL/min/1.73m2, the range was 6% (metoclopramide) to 27.3% (alendronic acid) in the students, and 8.7% (sotalol) to 76.1% (metformin) in the physicians. When the last two categories were pooled together (“drugs with renal recommendations”), the range was 37.2% (enoxaparin) to 87.4% (digoxin) in the students, and 28.3% (ranitidine) to 94.9% (ciprofloxacin and methotrexate) in the physicians. The percentage of lacking responses (interpreted as “I do not know”) was rather low (up to 3–6%), with the exception of topiramate and amantadine (8.0 and 9.4%) in the physicians, and famotidine, memantine, levetiracetam, amiloride, venlafaxine, topiramate, donepezil and rivastigmine (8.2–9.2%) in the students.
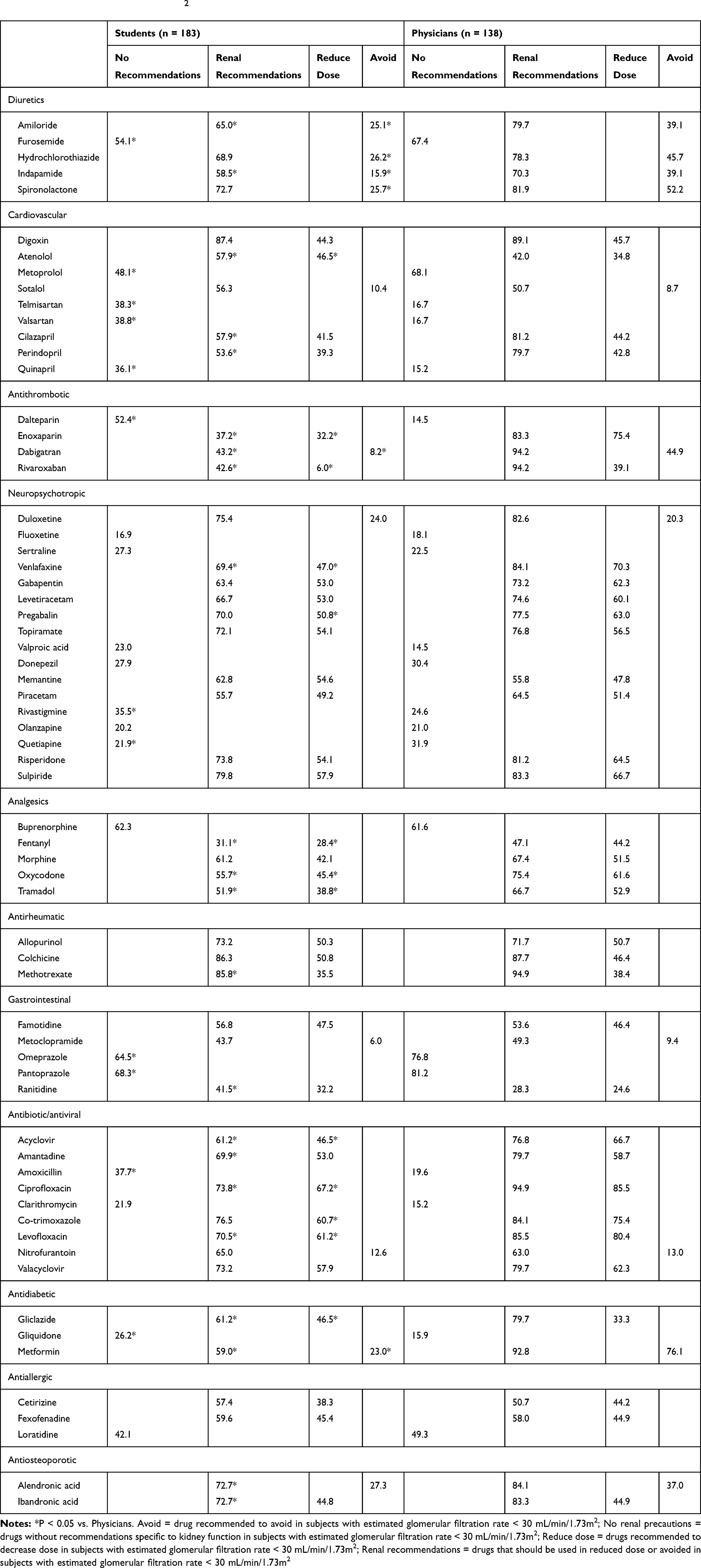 |
Table 2 Percentage of Correct Answers Concerning Drug Dosing Recommendations in Elderly Subjects with Estimated Glomerular Filtration Rate < 30 mL/min/1.73m2 |
Among 19 medications in the category “no renal precautions,” the physicians had higher percentage of correct responses than the students for 5 drugs (furosemide, metoprolol, quetiapine, omeprazole and pantoprazole), and lower for 7 drugs (telmisartan, valsartan, quinapril, dalteparin, rivastigmine, amoxicillin, and gliquidone). Among 33 medications requiring dose reduction, physicians had a higher percentage of correct answers for 12 drugs (enoxaparin, rivaroxaban, venlafaxine, pregabalin, fentanyl, oxycodone, tramadol, acyclovir, ciprofloxacin, co-trimoxazole, levofloxacin, and gliclazide), and lower for one drug (atenolol). Among 12 drugs that should be avoided in subjects with eGFR < 30 mL/min/1.73m2, the physicians had higher percentage of correct responses for 6 drugs (amiloride, hydrochlorothiazide, indapamide, spironolactone, dabigatran, and metformin). For the 45 drugs in the pooled category “renal recommendations,” the physicians had a higher percentage of correct answers for 20 medications (amiloride, indapamide, cilazapril, perindopril, enoxaparin, dabigatran, rivaroxaban, venlafaxine, fentanyl, oxycodone, tramadol, methotrexate, acyclovir, amantadine, ciprofloxacin, levofloxacin, gliclazide, metformin, alendronic acid, and ibandronic acid), and lower for 2 drugs (atenolol and ranitidine).
Discussion
Knowledge of recommended prescribing modifications in patients with impaired kidney function has rarely been investigated. We found only four papers, all reporting unsatisfactory levels of awareness and knowledge about renal prescribing recommendations among physicians.21–24 None of these reports referred specifically to older patients.
The results of our survey show a poor level of knowledge of recommended prescription modifications in older subjects with impaired kidney function among both 4th year medical students and physician-trainees in internal medicine (Table 2). The most striking examples are sotalol, metoclopramide and nitrofurantoin, correctly classified as drugs that should be avoided in such patients by only one of eight physicians and students. The extreme poor knowledge of these contraindications is the more surprising that all these three medications are quite commonly used in older patients.20 Frequent use of nitrofurantoin in patients with CKD was reported by Farag et al25 in a retrospective analysis of antibiotics prescribing in Canada.
Both physicians and students had difficulties with determination of drugs that do not need dose adjustment and do not require special precautions in patients with CKD. For example, less than 20% of physicians knew that telmisartan, valsartan, and quinapril can be safely administered in normal doses in such patients. A very low percentage of correct answers was also found for dalteparin, fluoxetine, valproic acid, amoxicillin, and clarithromycin. Moreover, the percentage of answers “no renal recommendations” within a given drug class was very similar regardless of the actual recommendations (eg, cilazapril and perindopril vs. quinapril; dalteparin vs. enoxaparin; amoxicillin and clarithromycin vs. levofloxacin). Taking unnecessary precautions may lead to underdosing of drugs, especially important in antibiotherapy.23
Although we did not directly compare the results between the medication classes, a particularly low percentage of correct answers was observed for gastrointestinal and antiallergic drugs in both physicians and students, and antithrombotic and antidiabetic medications in the students. A relatively high percentage of correct answers was found for rheumatologic drugs, opioids, and antibiotics requiring dose modification. Good awareness and knowledge about renal recommendations for antirheumatic medications in internal medicine house-staff has been reported by Surana et al,21 being explained by the awareness of harmful side effects of these drugs. The same applied to digoxin, a drug well-known for its adverse reactions and narrow therapeutic index, which was correctly classified as a drug with renal precautions in nearly 90% of physicians and students. In contrast, relatively good results for antibiotics requiring dose adjustment are contrary to previously reported findings.23,25 Interestingly, the level of knowledge of renal recommendations for opioids in the physician-trainees in internal medicine was very similar to the results that we have previously observed in a group of palliative care specialists.24
Despite the fact that our respondents were asked to classify drugs into three categories, we decided to analyze the 4th, pooled category “drugs with renal recommendations,” assuming that both “reduce dose” and “avoid” categories indicate that the respondents are aware of some renal precautions, which is potentially less harmful than incorrect classification as “drug without renal recommendations.” The other reason for such analysis was discordance between sources as to recommendations for some drugs, eg, ibandronic acid. According to The Renal Drug Handbook by Ashley and Dunleavy,7 this drug should be administered with extended time between doses in subjects with eGFR < 30 mL/min/1.73m2, which was classified as “dose reduction” for the purpose of this study. In contrast, this medication should be avoided in subjects with severe renal impairment according to the information on the Drugs.com web page.26 The use of the pooled category instead of “avoid” category resulted in an increase in correct answers for ibandronic acid form ~40 to 70–80%. A similar pattern could be seen for other drugs with divergent recommendations: sotalol and metoclopramide. The problem of conflicting dosing information between different pharmacotherapy sources has been previously described.27 To address this issue, the American Geriatric Society published consensus guidelines for 18 primarily renally cleared oral medications commonly taken by older adults; for a further 12 drugs the geriatric clinical pharmacist expert panel did not reach consensus.10 A list of 20 drugs (including 12 medications not listed in the consensus guidelines) that should be avoided or requiring dose adjustment in subjects with a specific degree of renal impairment was also added in 2015 to the American Geriatrics Society Beers criteria for potentially inappropriate medications in older adults.8 Three more drugs were added to the American Geriatrics Society 2019 Updated AGS Beers Criteria.9 However, drugs listed in the consensus guidelines and Beers criteria constitute only a small portion of all medications with renal precautions. The question also arises whether these documents are known to physicians who are not specialists in geriatrics.
As it might have been presumed, the percentage of correct answers was generally higher in physicians than in students, with the most striking difference for antithrombotic drugs (excluding dalteparin), diuretics that should be avoided, oxycodone, tramadol, metformin, and antibiotics requiring dose adjustment. The exceptions were the medications without renal precautions, which were better indicated by the students. Of note, the percentage of correct answers for these drugs was generally very low. In agreement with our results, Surana et al21 observed that internal medicine house-staff members’ awareness and knowledge about renal prescribing recommendations increased with years after graduation.
Limitations
The study was conducted in a single centre. However, physicians participating in the study were recruited from the whole country. Another limitation is selection of drugs, based on available literature and our subjective assessment of frequency of prescriptions.
Conclusion
Medical students and post-graduate trainees in internal medicine have poor knowledge of drug prescribing recommendations in older patients with renal impairment. As recommendations vary greatly between sources, it is necessary to prepare and popularize clear and complete guidelines of drug dosing in older patients with chronic kidney disease. The problem of dose adjustment in renal failure should be more emphasized during pre- and postgraduate education. Mobile- and computer-based supportive systems should be popularized to improve prescribing of drugs with renal recommendations.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Chapter 1: definition and classification of CKD. Kidney Int Suppl. 2013;3:19–62. doi:10.1038/kisup.2012.64
2. Schaeffner ES, Ebert N, Delanaye P, et al. Two novel equations to estimate kidney function in persons aged 70 years or older. Ann Intern Med. 2012;157:471–481. doi:10.7326/0003-4819-157-7-201210020-00003
3. Levey AS, Coresh J, Greene T, et al. Using standardized serum creatinine values in the modification of diet in renal disease study equation for estimating glomerular filtration rate. Ann Intern Med. 2006;145(4):247–254. doi:10.7326/0003-4819-145-4-200608150-00004
4. Coresh J, Astor BC, Greene T, Eknoyan G, Levey AS. Prevalence of chronic kidney disease and decreased kidney function in the adult US population. Third national health and nutrition examination survey. Am J Kidney Dis. 2003;41(1):1–12. doi:10.1053/ajkd.2003.50007
5. Chudek J, Wieczorowska-Tobis K, Zejda J, et al. The prevalence of chronic kidney disease and its relation to socioeconomic conditions in an elderly Polish population: results from the national population-based study PolSenior. Nephrol Dial Transplant. 2014;29(5):1073–1082. doi:10.1093/ndt/gft351
6. Naughton CA. Drug-induced nephrotoxicity. Am Fam Phys. 2008;78(6):743–750.
7. Ashley C, Dunleavy A. The Renal Drug Handbook. The Ultimate Prescribing Guide for Renal Practitioners.
8. American Geriatrics Society. 2015 updated beers criteria for potentially inappropriate medication use in older adults. J Am Ger Soc. 2015;63(11):2227–2246. doi:10.1111/jgs.13702
9. American Geriatrics Society. 2019 updated AGS beers criteria for potentially inappropriate medication use in older adults. J Am Ger Soc. 2019;67(4):674–694. doi:10.1111/jgs.15767
10. Hanlon J, Aspinall SL, Semla TP, et al. Consensus guidelines for oral dosing of primarily renally cleared medication in older adults. J Am Ger Soc. 2009;57(2):335–340. doi:10.1111/j.1532-5415.2008.02098.x
11. Hassan Y, Al-Ramahi R, Abd Aziz N, Ghazali R. Drug use and dosing in chronic kidney disease. Ann Acad Med Singapore. 2009;38(12):1095–1103.
12. Bates DW, Cullen DJ, Laird N, et al. Incidence of adverse drug events and potential adverse drug events. Implications for prevention. ADE prevention study group. J Am Med Assoc. 1995;74(1):29–34. doi:10.1001/jama.1995.03530010043033
13. Jones SA, Bhandari S. The prevalence of potentially inappropriate medication prescribing in elderly patients with chronic kidney disease. Postgrad Med J. 2013;89(1051):247–250. doi:10.1136/postgradmedj-2012-130889
14. Doody HK, Peterson GM, Watson D, Castelino RL. Retrospective evaluation of potentially inappropriate prescribing in hospitalized patients with renal impairment. Curr Med Res Opin. 2015;31(3):525–535. doi:10.1185/03007995.2015.1010036
15. Sonnerstam E, Sjolander M, Gustafsson M. Inappropriate prescription and renal function among older patients with cognitive impairment. Drugs Aging. 2016;33(12):889–899. doi:10.1007/s40266-016-0408-8
16. Yang P, Chen N, Wang -R-R, Li L, Jiang S-P. Inappropriateness of medication prescriptions about chronic kidney disease patients without dialysis therapy in a Chinese tertiary teaching hospital. Ther Clin Risk Manag. 2016;12:1517–1524. doi:10.2147/TCRM.S116789
17. Blix HS, Viktiol KK, Moger TA, Reikvam A. Use of renal risk drugs in hospitalized patients with impaired renal function – an underestimated problem? Nephrol Dial Transplant. 2006;21(11):3164–3171. doi:10.1093/ndt/gfl399
18. Drenth-van Maanen AC, van Marum RJ, Jansen PA, Zwart JE, van Solinge WW, Egberts TC. Adherence with dosing guideline in patients with impaired renal function at hospital discharge. PLoS One. 2015;10(6):e0128237. doi:10.1371/journal.pone.0128237
19. Dorks M, Allers K, Schmiemann G, Herget-Rosenthal S, Hoffmann F. Inappropriate medication in non-hospitalized patients with renal insufficiency: a systematic review. J Am Ger Soc. 2017;65(4):853–862. doi:10.1111/jgs.14809
20. Deskur-Smielecka E, Chudek J, Neumann-Podczaska A, Mossakowska M, Wizner B, Wieczorowska-Tobis K. Use of renal risk drugs in a nation-wide Polish older adult population: an analysis of PolSenior database. BMC Ger. 2019;19(1):70. doi:10.1186/s12877-019-1075-5
21. Surana S, Kumar N, Vassudeva A, et al. Awareness and knowledge among internal medicine house-staff for dose adjustment of commonly used medications in patients with CKD. BMC Nephrol. 2017;18:26. doi:10.1186/s12882-017-0443-7
22. Saad CY, Fogel J, Rubinstein S. Awareness and knowledge among internal medicine resident trainees for dose adjustment of analgesics and neuropsychotropic medications in CKD. South Med J. 2018;111(3):155–162. doi:10.14423/SMJ.0000000000000781
23. Maus S, Holch C, Chock D, Thalhammer F, Keller F, Hartmann B. Questionnaire surveying nephrologists on drug dose adjustment in patients with impaired kidney function. Wien Klin Wochenschr. 2010;122(15–16):479–485. doi:10.1007/s00508-010-1421-2
24. Kotlinska-Lemieszek A, Deskur-Smielecka E. Safe pharmacotherapy of symptoms in patients with end-stage kidney disease – results of a questionnaire performed on physicians working in palliative care units. Pall Med. 2017;9(3):139–151.
25. Farag A, Garg AX, Li L, Jain AK. Dosing errors in prescribed antibiotics for older persons with CKD: a retrospective time series analysis. Am J Kidney Dis. 2014;63(3):422–428. doi:10.1053/j.ajkd.2013.09.009
26. Ibandronate dosage. Renal dose adjustments. Available from: https://www.drugs.com/dosage/ibandronate.html#Renal_Dose_Adjustments.
27. Vidal L, Shavit M, Fraser A, Paul M, Leibovici L. Systematic comparison of drug information regarding adjustment of dose for renal function. Br Med J. 2005;331(7511):263–266. doi:10.1136/bmj.38476.471088.3A
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.