")
Back to Journals » Drug Design, Development and Therapy » Volume 14
Management of Pediatric Systemic Lupus Erythematosus: Focus on Belimumab
Authors Guzman M, Hui-Yuen JS
Received 7 March 2020
Accepted for publication 15 June 2020
Published 25 June 2020 Volume 2020:14 Pages 2503—2513
DOI https://doi.org/10.2147/DDDT.S216193
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jianbo Sun
Marla Guzman,1,2 Joyce S Hui-Yuen1– 3
1Division of Pediatric Rheumatology, Steven and Alexandra Cohen Children’s Medical Center of New York, Lake Success, NY, USA; 2Department of Pediatrics, Zucker School of Medicine at Hofstra/Northwell, Hempstead, NY, USA; 3Center for Autoimmune, Musculoskeletal, and Hematopoietic Diseases Research, Feinstein Institute for Medical Research, Manhasset, NY, USA
Correspondence: Joyce S Hui-Yuen
Division of Pediatric Rheumatology, Steven and Alexandra Cohen Children’s Medical Center, 1991 Marcus Avenue, Suite M100, New Hyde Park, NY 11040 Tel +1 516 472 3700
Fax +1 516 472 3752
Email [email protected]
Abstract: Belimumab (Benlysta®) is a fully humanized monoclonal antibody that inhibits B lymphocyte stimulator (BLyS, also known as B cell-activating factor of the tumor necrosis factor family) and was approved by the US Food and Drug Administration (FDA) and the European Medicines Evaluation Agency for the treatment of autoantibody-positive systemic lupus erythematosus (SLE) in adults with moderate disease activity. Belimumab was recently FDA approved for use in children with SLE between 5 and 17 years of age. This review discusses the key findings of the belimumab phase III trials in adult SLE (via intravenous and subcutaneous administrations), phase II trial in pediatric SLE (intravenous administration), and post hoc analyses. It also evaluates the current clinical trials of belimumab in specific SLE disease states and highlights the safety profile of belimumab. It discusses the clinical post-marketing use of belimumab in adults and children with SLE and concludes with our recommendations for the use of belimumab to treat pediatric SLE, including a look to the future with increased real-world use in children with SLE.
Keywords: belimumab, pediatric SLE, lupus treatment
Introduction
Systemic lupus erythematosus (SLE) is a chronic, multi-system, autoimmune disease of unknown etiology with a heterogeneous range of clinical and serological manifestations. It can affect multiple organ systems, and its hallmark is the production of autoantibodies.1–3 Classification criteria may aid in diagnosis.4–6 In adults, SLE predominantly affects women of child-bearing age, with a female-to-male ratio of 9:1;7 in pre-pubertal children, this ratio is closer to 4:1.8 SLE more commonly affects non-Caucasian individuals. Up to 20% of SLE patients are diagnosed prior to their 19th birthday (childhood-onset SLE, cSLE); this subset of SLE has a more severe disease course and severe organ involvement.9,10 Specifically, renal, pulmonary, and cardiac involvement appear to be more frequent in cSLE,10,11 and there is a shorter duration between diagnosis and first intensive care admission.9 The uniqueness of disease expression in each patient often results in treatment with multiple immunosuppressive medications. While these medications are meant to improve disease control, patients may also be put at risk for potential severe side effects from broad immunosuppression.12,13 In addition, the course of SLE is often complicated by its unpredictability of disease flares and accrual of organ damage, frequently while patients appear to be optimally treated. This often requires escalation of therapy including increasing doses of corticosteroids that can contribute to subsequent long-term damage.14 Thus, there remains a need for safer and more effective options for the treatment of cSLE.
Targeted immunosuppression may have beneficial therapeutic outcomes in SLE. SLE is a complex autoimmune disorder that involves both the innate and adaptive immune systems, resulting in a dysregulation of the immune response and the production of autoantibodies. B cells (the precursor cells for plasma cells) are activated by T cells and subsequently produce antibodies.15 B cells arise in the bone marrow and go through several stages of maturation and development prior to the production of antibodies. In healthy individuals, B cells play a large role in maintaining a functioning immune system, including the production of protective antibodies. In SLE, a large number of autoreactive B cells that react to self-antigens results in the production of autoantibodies that trigger an overwhelming inflammatory response.16 Additionally, there may be a paucity of or abnormality in regulatory immune cells, further enhancing B cell activation and proliferation.15
B lymphocyte stimulator (BlyS), also called B cell-activating factor (BAFF), is a growth factor that can bind to three different receptors that are critical for B cell maturation and survival.17,18 In particular, BlyS promotes the survival of autoreactive B cells during negative selection. SLE mouse models have been shown to have elevated levels of BlyS, likely resulting in the increased number of mature B cells and autoantibodies seen in these mice.19 Mice that overproduce BlyS were also found to have defective apoptotic signals, allowing B cells that recognize self-antigens to survive, thus evading negative selection and continuing to produce autoantibodies.19,20
Patients with SLE have been identified as having higher levels of soluble BlyS when compared to serum from healthy individuals;21 in addition, BlyS levels have been shown to rise during times of active disease.22 Thus, BlyS became an attractive target for therapeutic agents for SLE, leading to the development of belimumab (Benlysta®), a fully humanized, monoclonal antibody against BlyS/BAFF. This review provides an overview of the efficacy and safety of belimumab in the phase III trials in adult SLE and the phase II and III trials in cSLE. We discuss the current clinical real-world experience with belimumab use in adult and pediatric SLE to date. We conclude with a discussion of ongoing trials and our recommendations for the use of belimumab in the treatment of cSLE.
Clinical Efficacy of Intravenous Belimumab
The intravenous (IV) formulation of belimumab received approval by the Food and Drug Administration (FDA) and European Medicines Evaluation Agency (EMEA) in 2011. Belimumab was the first SLE specific medication to receive FDA approval in over 50 years. In the adult population, belimumab is approved for autoantibody-positive SLE in conjunction with standard of care (SOC) SLE treatment. Belimumab is not approved for use in those with active, severe lupus nephritis (LN) and/or severe, active neuropsychiatric lupus (NPSLE), as the initial trials did not include those patients. Dosing of IV belimumab is 10 mg/kg once every 2 weeks for 3 doses, then 10 mg/kg once every 4 weeks thereafter. Subcutaneous (SC) belimumab received FDA approval for the treatment of adult lupus in 2017. Dosing of SC belimumab is 200 mg once weekly, either via prefilled syringe or autoinjector. In pediatric SLE, IV belimumab was approved by the FDA in 2019 for the treatment of active, seropositive SLE in patients 5 to 17 years old, in conjunction with SOC SLE treatment. At the time of writing, SC belimumab is in phase II testing in cSLE (NCT 04179032)23 and does not yet have FDA approval to treat children with SLE.
The protocol for the phase III clinical trials for belimumab was adjusted based on the data from phase II trials. A novel outcome measure, SLE Responder Index (SRI), was developed after the phase II trials to evaluate clinical efficacy and to be used as a responder index and endpoint in SLE patients with ANA ≥1:80 and/or anti-double-stranded DNA antibodies (anti-dsDNA) ≥30 IU/mL receiving belimumab versus placebo.24 The SRI combines The Safety of Estrogens in Lupus Erythematosus: National Assessment version of the Systemic Lupus Erythematosus Disease Activity Index (SELENA-SLEDAI), the British Isles Lupus Assessment Group (BILAG), and the physician global assessment (PGA), all of which are disease activity or outcome measures. A responder in the SRI is defined as having a reduction of at least 4 points in the SELENA-SLEDAI, no new BILAG A organ domain score, no more than 1 new BILAG B organ domain score, and no worsening in PGA score at week 52.
Two multicenter, randomized, placebo-controlled clinical trials, BLISS-52 and BLISS-76, were conducted to assess the efficacy, safety, and tolerability of belimumab in addition to SOC therapy (e.g., other immunosuppressive medications commonly used to treat SLE) in patients with active SLE (Table 1).25,26 Patients included in the BLISS-52 and BLISS-76 trials had active SLE (≥6 on SELENA-SLEDAI), were ≥18 years old, and met ACR criteria for SLE. Included patients also had positive ANA (titer ≥1:80) or positive anti-dsDNA antibody (≥30 IU/mL) and were on SOC therapy. Patients with active, severe lupus nephritis or active, severe NPSLE were excluded.
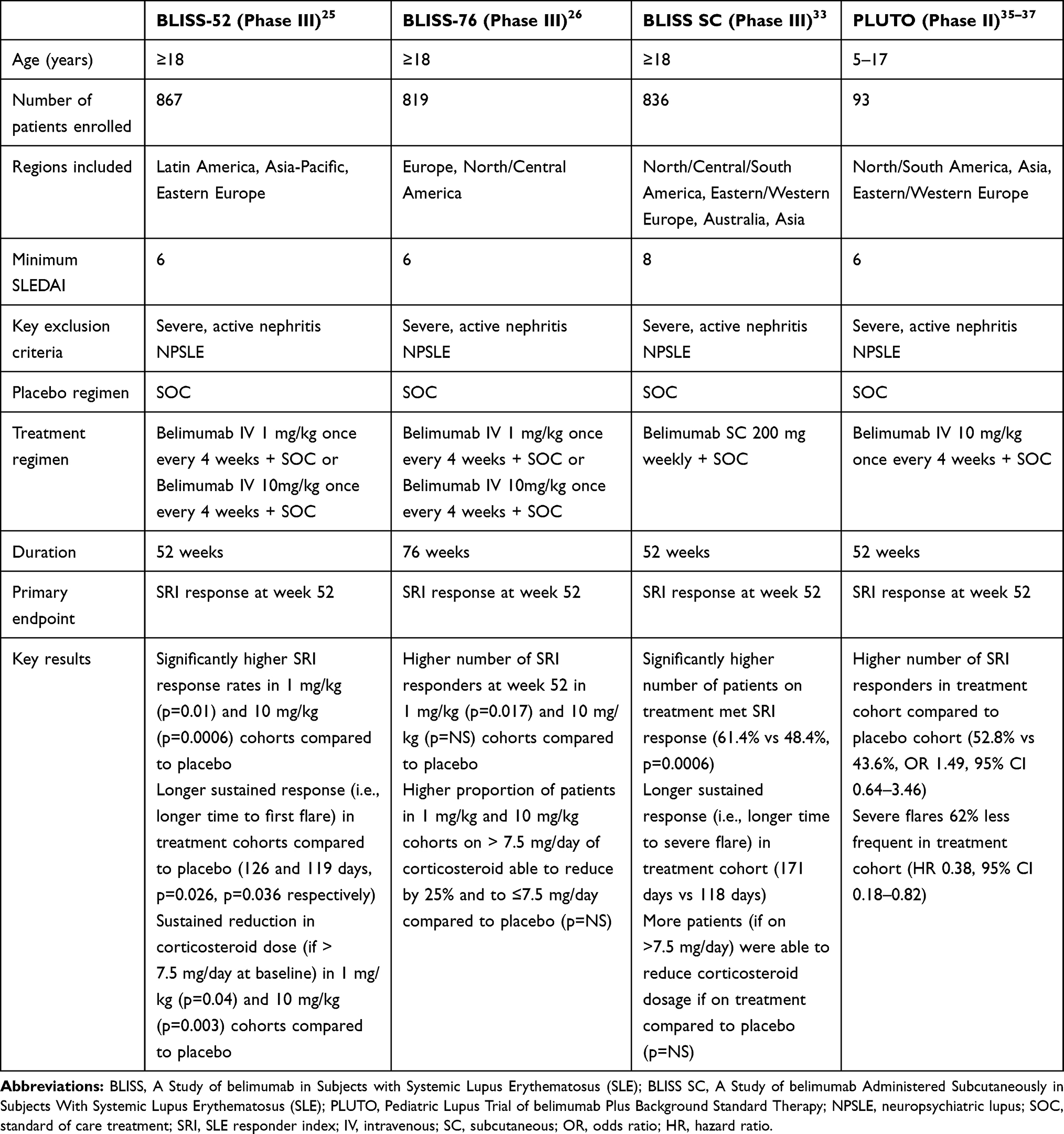 |
Table 1 Key Belimumab Trials in Adult and Pediatric Lupus |
The primary endpoint of BLISS-52, conducted in Eastern Europe, Asia, and Latin America, was the SRI response rate at week 52.25 In BLISS-52, 867 patients were enrolled and randomized to receive belimumab IV at 1 mg/kg, 10 mg/kg, or placebo, in addition to SOC SLE treatment. The primary disease manifestations of patients in the trial were mucocutaneous and musculoskeletal. Both treatment cohorts (1 mg/kg and 10 mg/kg doses) showed a statistically significant SRI response rate when compared to placebo at week 52: 58% of patients in the 10 mg/kg cohort responded (p=0.0006), 51% of patients in the 1 mg/kg cohort responded (p=0.0129), and 44% of patients in the placebo cohort responded. Secondary endpoints (time to first flare and reduction in prednisone dose) were also met. In the 1 mg/kg and 10 mg/kg cohorts, time to first flare was 126 and 119 days, respectively, compared to 84 days in the placebo cohort (p=0.0026, p=0.0036, respectively). In the 1 mg/kg and 10 mg/kg cohorts, 24% and 28% of patients, respectively, had a sustained reduction in prednisone dose from a baseline of >7.5 mg/day compared to 15% of placebo patients (p=0.0465, p=0.0032, respectively). Serious adverse events were similar in the treatment and placebo cohorts (see Safety).
BLISS-76 was conducted in North America, Central America, and Europe26 and enrolled 819 patients who were then randomized to receive belimumab IV at 1 mg/kg, 10 mg/kg, or placebo, in addition to SOC treatment. Similarly to BLISS-52, musculoskeletal and mucocutaneous involvement were the most common disease manifestations. The primary endpoint was the SRI response rate at week 52. Only the 10 mg/kg treatment cohort showed a statistically significant SRI response rate at week 52 when compared to placebo (43.2% versus 33.5%, p=0.017). However, there was no statistically significant difference in SRI response rate between cohorts at week 76, a secondary endpoint. The number of patients in the treatment groups that experienced a reduction in daily corticosteroid dose by ≥25% to ≤7.5 mg/day was higher when compared to placebo, although this value was not statistically significant. Of note, post hoc analyses using a higher SELENA-SLEDAI threshold showed a significant difference at week 76 in SRI response rates between the 10 mg/kg belimumab and placebo cohorts at all SELENA-SLEDAI reduction thresholds. Adverse events were similar in all three cohorts (see Safety). Additionally, a subgroup analysis identifying predictors of response in patients from the BLISS-52 and −76 trials with high disease activity (low complement/anti-dsDNA antibody positive) observed that there was a statistically significant improvement in SRI at week 52: 41.5% for the belimumab 1 mg/kg cohort, and 51.5% for the belimumab 10 mg/kg cohort, compared to 31.7% of patients on SOC therapy alone (p=0.002, p<0.001, respectively).27
Given the limited number of patients of Black race in the BLISS trials, a trial specifically evaluating efficacy and safety of belimumab in Black race patients with SLE (EMBRACE) was completed in 2019.28 The EMBRACE study (NCT 01632241)29 was a randomized, multi-center, double-blind, placebo-controlled trial of 448 patients randomized to receive either monthly belimumab 10 mg/kg IV or placebo, in addition to SOC treatment. Patients self-identified as Black and were included if they had active disease at screening (SELENA-SLEDAI ≥8). Of note, this enrollment SELENA-SLEDAI score is 2 points higher than that of the BLISS trials, perhaps accounting for higher disease activity in Black SLE patients. Similar to the BLISS trials, patients with severe active kidney or neuropsychiatric involvement were excluded. The primary endpoint was the SRI response rate with modified SLEDAI-2K (S2K) scoring for proteinuria at week 52 (SRI-S2K). Only 48.7% of the patients in the belimumab cohort compared to 41.6% of the placebo cohort responded by week 52 (p=NS); thus, the primary endpoint was not reached. However, subgroup analysis of Black patients with high disease activity (SELENA-SLEDAI ≥ 10) in both cohorts did demonstrate significant improvement in the belimumab cohort (52.5% response compared to 40.9% response in placebo cohort, p=0.03). Similarly, subgroup analysis of Black patients with serologically active disease (low complements and/or positive anti-dsDNA antibody levels) showed significant response by week 52 in the belimumab cohort (45.1%) compared to placebo (24%, p=0.007).
Since end-organ involvement, particularly LN, is a frequent manifestation of cSLE, new treatments are necessary to avoid side effects of cytotoxic medications (e.g., cyclophosphamide) currently used in the treatment of LN. Although there are no trials to date evaluating the efficacy of belimumab in cSLE LN, there are two trials in the adult population that are currently underway or recently completed. The rituximab and belimumab for lupus nephritis (CALIBRATE) study (NCT 02260934) is a prospective, randomized, open-label, Phase II trial of induction therapy with rituximab followed by maintenance therapy with belimumab in patients with active LN.30,31 Forty-three patients were randomized to receive either belimumab IV 10 mg/kg plus prednisone or prednisone alone 4 weeks after treatment with IV rituximab, cyclophosphamide, and methylprednisolone. Complete response was defined as urine protein:creatinine ratio <0.5, eGFR≥120 or, if eGFR<120, eGFR>80% of eGFR at the time of screening, and prednisone dose tapered to 10 mg/day. At week 24, the complete response rate was 24% in the belimumab plus prednisone cohort and 23% in the prednisone only cohort. Additionally, belimumab treatment delayed the reconstitution of B cells post-rituximab, although this was not associated with hypogammaglobulinemia or increase in serious infections. Further analysis as time progresses is needed to fully evaluate whether belimumab is a viable treatment option for patients with LN.
The BLISS-LN trial (NCT 01639339)32 is a currently active phase III trial evaluating the safety, efficacy, and tolerability of belimumab plus SOC treatment in adult patients with active LN. Results have not yet been published at the time of writing.
Clinical Efficacy of Subcutaneous Belimumab
Since IV medications can be logistically demanding and burdensome for many patients, requiring frequent visits to an infusion center or office, SC administration of belimumab is an appealing option. BLISS-SC was a phase III randomized, double-blinded, placebo-controlled multi-center study conducted to evaluate the safety and efficacy of SC belimumab.33 Although this trial was not meant to measure equivalence to the IV formulation, weekly SC dosing does have a similar pharmacokinetic profile to monthly IV dosing. Inclusion criteria were a diagnosis of SLE defined by ACR criteria, seropositivity prior to enrollment, and a SLEDAI of ≥8, which was a higher threshold than for entry into either BLISS-52 or BLISS-76. As with BLISS-52 and BLISS-76, patients with severe, active LN and/or NPSLE were excluded. BLISS-SC enrolled 836 patients from multiple continents, including North America. Patients were randomized to receive weekly doses of SC belimumab or placebo, plus SOC therapy, for 52 weeks. The study met its primary endpoint with a statistically significant SRI response in those receiving SC belimumab (61.4%) versus placebo (48.4%, p=0.0006). Similar to subgroup analysis of serologically active SLE patients in the BLISS trials, 356 of the 836 patients in BLISS-SC were identified as serologically active and found to have significant improvement on belimumab (64.4%) when compared with placebo (47.2%, p=0.0014).34 Time to severe flare, a secondary endpoint, was also longer in patients receiving SC belimumab when compared to patients receiving placebo (126.5 days versus 90 days). Additionally, more patients in the SC belimumab cohort were observed to reduce their corticosteroid dose when compared to the placebo cohort (p=NS). Patient-reported fatigue was also significantly reduced with SC belimumab treatment (p=0.0324). The safety profile was consistent with the safety profile of IV belimumab (see Safety).
Clinical Efficacy of Intravenous Belimumab in Childhood-Onset SLE
Use of belimumab IV in cSLE patients aged 5 years and older was approved by the FDA in 2019, making it the first FDA-approved drug for cSLE. The Pediatric Lupus Trial of Belimumab Plus Background Standard Therapy (PLUTO) is a Phase II, multicenter, randomized, double-blind trial evaluating the efficacy, safety, and pharmacokinetics of IV belimumab versus placebo plus SOC in cSLE patients aged 5–17 years, in which 93 patients were enrolled (NCT 01649765).35–37 Active disease (SELENA-SLEDAI ≥6) was part of the inclusion criteria. Patients with active, severe LN or NPSLE were excluded. Subjects were randomized to belimumab 10mg/kg (n=53) or placebo (n=40) IV monthly dosing, in addition to SOC therapy. The primary endpoint was SRI at week 52. Of note, due to the relative rarity of cSLE, much smaller numbers of patients were enrolled than in the adult phase III trials, and PLUTO was not powered for statistical analysis. Preliminary results showed that the 10 mg/kg dose of belimumab used in adult patients may be appropriate for patients with cSLE. Preliminary results also demonstrate that the belimumab cohort had more SRI and PRINTO/ACR responders compared to placebo patients at 52 weeks (52.8% versus 43.6%). Additionally, severe flares were less frequent in belimumab patients compared to placebo, and belimumab patients had longer median time to first severe flare (159.5 days versus 82 days). Sustained parent global assessment response was also higher in the belimumab cohort compared to placebo (68.2% versus 52.8%).
Specific demographics and characteristics of the patients in the PLUTO study, such as disease characteristics, serologies, or number of patients with LN or NPSLE, have not yet been published at the time of writing. Additionally, changes in corticosteroid dose and specific adverse events have not yet been reported. Long-term efficacy results and adverse event monitoring are ongoing.
Subcutaneous belimumab is not currently approved for use in patients under the age of 18 years. At the time of writing, there is an actively recruiting phase II multi-center, open-label, clinical trial based evaluating the safety and pharmacokinetics of belimumab SC in addition to SOC treatment in SLE patients 5–17 years of age (NCT 04179032).23 The administration schedule of SC belimumab is based on body weight. Patients with SELENA-SLEDAI score ≥6 are included, which is lower than the threshold in the adult SC trial, but the same as the threshold for adult and pediatric IV belimumab trials. Patients with active, severe LN or active NPSLE were excluded from the trial. No preliminary results are yet available, as the trial is still under active recruitment at the time of writing.
Use of Belimumab in the Real World: Long-Term Outcomes
Since the results of the phase III clinical trials, several large post-marketing observational and retrospective studies have been conducted in adult and pediatric SLE patients. An initial continuation study of the phase II studies evaluated the long-term efficacy and safety of IV belimumab over 7 years.38 There were 298 patients enrolled at the initiation of the continuation study, and 177 patients remained in the study until completion at year 7. Of these, 65% of patients achieved SRI response by Year 7, with an associated 55% decrease in existing corticosteroid doses. The longest observational study to date evaluating the efficacy and safety of IV belimumab was conducted by Wallace et al over the course of 13 years as part of a continuation study of the phase II trial.39 As in the 7-year continuation study, 298 patients were enrolled at initiation of the continuation study, and only 96 patients remained in the study until completion. As participants declined over the years, a higher percentage of patients achieved an SRI response (32.8% at baseline compared to 75.6% at year 12). Over 50% of patients receiving >7.5 mg/day of prednisone at baseline were able to achieve a dose of ≤7.5 mg/day of prednisone at year 12. Of note, anti-dsDNA and complement levels did not normalize in the large majority of patients over time, with anti-dsDNA antibodies normalizing in only 15.1% of patients, C3 normalizing in 8.0% of patients, and C4 normalizing in 12.1% of patients. However, normalized parameters did remain stable throughout the duration of the study. It is important to note that there was a large percentage of patients who did not remain in the study; this may suggest that patients who responded to belimumab initially may have preferred to discontinue the medication after their symptoms resolved. Moreover, patients who did not have an initial response may have withdrawn, potentially confounding results.
The OBSErve study was an international, multi-center study evaluating the real-world clinical efficacy of IV belimumab in adult SLE patients with refractory disease in the US, Canada, Switzerland, Germany, Argentina, and Spain. The international OBSErve studies assessed outcomes in adult SLE patients on belimumab treatment over the course of 640–43 to 1844 months, and the US study evaluated patients for as long as 24 months on treatment.45 The most common reasons to initiate belimumab therapy were musculoskeletal, mucocutaneous, and immunologic involvement. The studies conducted in the US, Switzerland, and Germany included patients with LN and/or NPSLE, though it is not known whether these manifestations were active at the time of initiation of belimumab.41,42,45 In the US study, patients with baseline elevated creatinine or urine protein-creatinine ratios suggestive of active kidney involvement, had significant decline in these values after 24 months of treatment (p<0.0001 for both). However, those with “very high” 24 hour urine protein collection values at baseline did not have a significant decrease in 24 hour urine protein, suggesting belimumab may not be useful in those with more severe renal involvement. Several countries reported SLEDAI scores that decreased by at least 5 points from baseline at the final follow-up (p value range <0.0001 to <0.001).42–45 Reductions in corticosteroid dose from baseline to end of follow-up were reported in all countries; in particular, in the Spanish cohort, 75% of patients had a decrease in their corticosteroid dose, and in the US cohort, the percentage of patients on >7.5 mg/day oral corticosteroids at baseline decreased from 67.5% to 18.4%.
We previously reported the use of belimumab in a cohort of 195 patients as part of a prospective, multicenter, observational study across 10 large academic SLE clinical practices.46 Similar to other reports, these patients primarily had musculoskeletal, mucocutaneous, and/or immunologic involvement, as well as an inability to taper corticosteroids at baseline. Clinical improvement in response to belimumab in addition to SOC treatment was detected as early as 3 months after initiation of therapy, and 51% of patients showed a response at 6 months. Clinical improvement was defined as the treating physician’s subjective assessment of at least 50% improvement in clinical manifestations.
In the large Italian cohorts reported by Iaccarino et al,47 scores measuring disease activity in joint and skin manifestations were significantly decreased over time. Additionally, anti-dsDNA antibody levels and 24 hour proteinuria significantly decreased with treatment (p<0.01 for both). In another study cohort of 188 patients reported by Iaccarino and colleagues,48 77% of patients achieved SRI at 12 months, and 45 of 54 patients (83.7%) remaining on belimumab at 24 months maintained SRI response. Predictors of SRI response at 12 and 24 months were SLEDAI-2K score ≥10 and polyarthritis.
Several smaller observational and retrospective cohort studies have also described the post-marketing use of belimumab in adult SLE.49–52 Their response rates, improvement in serologic measures, and ability to taper corticosteroids after initiation of belimumab are similar to those in the larger studies described above.
Use of Belimumab in the Real World: Childhood-Onset Lupus
We are the only group to date who has reported on the clinical use of belimumab in cSLE.46 Overall, the indications for treatment as well as response to treatment are similar when compared to the adult studies. We reported a subset of 39 cSLE patients treated with belimumab in addition to SOC; of these, 4 patients were under 18 years of age at the time of drug administration. The mean age at diagnosis was 14 (± 4) years. The most common indications for treatment in these patients were musculoskeletal and mucocutaneous manifestations; the patients under 18 years old were treated for rash, thrombocytopenia, and inability to taper corticosteroids. Clinical response was defined as the treating physician’s impression of ≥50% improvement in the initial manifestation(s) being treated and no worsening in other organ systems. Patient outcomes were promising: after 6 months of treatment, a greater proportion of cSLE patients responded clinically to belimumab (65%) as compared to adult SLE patients (45%), although this difference was not statistically significant. A 25% decrease in anti-dsDNA antibody levels was seen within 3 months of starting belimumab. Moreover, corticosteroids were discontinued in 35% of cSLE patients after 6 months of belimumab treatment as compared with 11% of adult-onset SLE patients (p=0.002).46
Safety of Belimumab
Adverse effects (AE) of belimumab are similar to those of other biologic agents (Table 2). As with any immunosuppressive drug, infection and lack of response appear to be common reasons for discontinuation.25,26,33,34,38,39,43-46,48–54 Infections, including upper respiratory tract infections, cellulitis, pneumonia, and urinary tract infections are common AEs reported on belimumab therapy.25–28,31,33,38-40,45–48,51–57,61 More serious infections including Group A streptococcal bacteremia,46 disseminated cytomegalovirus,26 and viral gastroenteritis51 have also been reported. A rare, but debilitating serious AE (SAE) is progressive multifocal leukoencephalopathy (PML), a serious and potentially fatal neurologic condition that is triggered by JC virus reactivation. To date, there are eight reports of PML after treatment with belimumab.55–57 All affected patients were female, with a mean age of 50.1 years and a 25% mortality rate. Two of these cases were reported in more detail and describe women with long-standing SLE who had not been diagnosed with NPSLE prior to starting belimumab. Both women were on at least one other immunosuppressive medication at the initiation of belimumab and had received at least 6 consecutive months of belimumab infusions at the onset of PML symptoms. There was evidence of JC virus in the sera of both patients and radiographic evidence supporting PML diagnosis.55,56
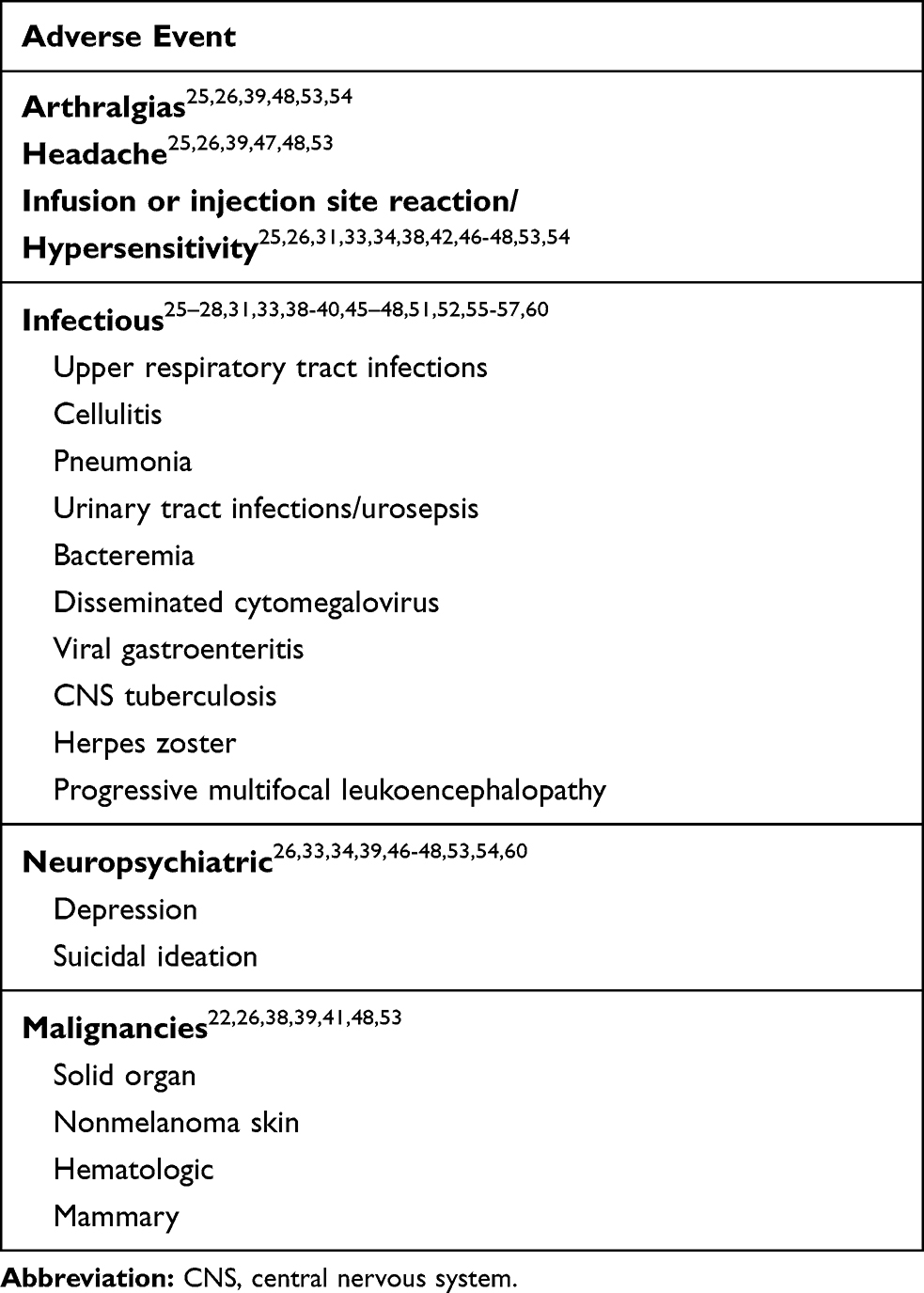 |
Table 2 Adverse Events in Adult and Pediatric Lupus Patients on Belimumab Treatment |
Infusion reactions/hypersensitivity are also frequently reported while on belimumab therapy.25,26,31,33,38,42,46-48,53,54 Other common non-serious AEs reported include arthralgias25,26,39,48,53,54 and headache.25,26,39,47,48,53 Certain malignancies have also been reported with varying frequency, including solid organ cancers, hematologic malignancies, and skin cancers.26,33,38,39,41,48,53
Psychiatric symptoms and/or development of NPSLE have also been reported in patients on belimumab therapy, including depression, anxiety, and suicidal ideation/completed suicides.26,33,34,39,46-48,53,54,61 Depression was reported in 3 of 188 Italian patients, one of which was severe.48 Of 195 patients, we reported 1 patient with severe depression, 1 with worsening depression, and 1 who developed psychosis while on belimumab therapy.46 In the Belimumab Assessment of Safety in SLE study (BASE), there was a higher incidence of depression in the treatment group while on treatment with belimumab, compared to placebo; these numbers were consistent with the incidence seen in other studies.58 Belimumab was discontinued in 2 of 401 patients after 6 months due to the onset of depression in the OBSErve US observational study.45 Thus, it is essential to monitor the mental health status of patients on belimumab, particularly if they have a history of psychiatric disease prior to belimumab treatment.
The AE profile in the SC belimumab trial is similar in comparison to the IV belimumab studies.33 Injection site reactions occurred in 6.1% of patients receiving SC belimumab. Hypersensitivity reactions were not more likely to occur in the treatment cohort in the SC trial. Infections including bacterial sepsis, urosepsis, tuberculosis affecting the central nervous system, and herpes zoster were reported. No serious episodes of depression were reported in the SC belimumab cohort, although 2.7% of patients on SC belimumab experienced depression, and 0.4% of patients reported serious suicidal ideation. In a 6-month extension study of the BLISS-SC trial, 190 out of 662 patients of patients on SC belimumab experienced an infection; 17 of these were considered serious infections. No patients developed malignancies. Depression was reported in 12 out of 662 patients, and suicidal ideation/suicidal behaviors were reported in 2 patients.54
Safety of Belimumab: Childhood-Onset SLE
Several types of SAEs were seen in the 39 childhood-onset SLE patients on belimumab therapy in our multicenter, observational study.46 Three patients developed or had worsening of LN. There were also multiple neuropsychiatric SAEs reported in our cohort. One cSLE patient developed seizures while on belimumab, one experienced worsening of her depressive symptoms and developed suicidal ideation, and one developed CNS vasculitis while on belimumab therapy that was confirmed with changes on brain imaging. Thus, caution should be taken when starting a patient with cSLE on belimumab since neuropsychiatric manifestations appear to be more frequent in childhood-onset SLE compared to adult-onset SLE.59 Additionally, children with chronic illness may be more prone to depression and anxiety as a result of frequent doctors’ visits, polypharmacy, and feelings of being “different” from their peers during a time of emotional vulnerability. These symptoms of depression are certainly inclusive of young adults with cSLE and should be fully evaluated before deciding to initiate belimumab therapy.60
In the PLUTO trial, 17% of cSLE patients treated with belimumab and SOC experienced an SAE compared to 35% of patients treated with placebo in addition to SOC. When compared to the adult BLISS trials, there was no difference between treatment cohorts in the number of malignant neoplasms and post-infusion systemic reactions reported.61 Overall, the rate and incidence of AEs were similar in the PLUTO and adult trials. Interestingly, there was a lower incidence of depression and suicide in treatment patients in the PLUTO study when compared to those in the BLISS trials (1.9% of belimumab patients in the PLUTO study experienced depression or suicide), though our real-world experience of 7.6% (described above) would suggest otherwise.
Future Promises
There is much future promise regarding the use of belimumab in the cSLE population. It remains unclear whether belimumab will be beneficial in treating active LN, despite the CALIBRATE trial results. Although we eagerly await the results from the BLISS-LN trial, studies are also underway to determine efficacy in other patients with abnormal kidney function, such as primary membranous nephropathy (NCT 03949855),62 whose results could potentially be extrapolated to patients with active LN.
Targeted therapies for NPSLE are severely lacking, but it remains unclear whether belimumab will be beneficial in the treatment of NPSLE, particularly since worsening depression and suicidal ideation have been reported in patients on treatment with belimumab.
We eagerly await the results of the PLUTO study on the efficacy of belimumab in cSLE. Response in Black cSLE patients will also be of interest, as this patient population comprises a large proportion of patients with cSLE. In addition, Black cSLE patients have been shown to have more severe disease and end-organ involvement than SLE patients of other races.63 Results from the EMBRACE trial in Black adult SLE patients are encouraging as they showed significant improvement in SLE patients with high disease activity on belimumab as compared to those on placebo in addition to SOC therapy.
Moreover, it has been proposed that using a combination of two different B cell-targeted therapies may improve treatment outcomes in SLE. The BLISS-BELIEVE trial (NCT 03312907) is a phase III trial evaluating the efficacy and safety of belimumab in combination with rituximab in adult SLE patients. Preliminary results demonstrate favorable outcomes at the time of writing.64
Additionally, the successful use of SC belimumab in the adult SLE population may be a predictor of its future successful use in cSLE. This will be of benefit to the pediatric population, with fewer school absences due to monthly infusions, and we look forward to preliminary results from the phase II SC belimumab trial. Finally, it will be of interest to follow all cSLE patients treated with belimumab into adulthood to determine long-term outcomes of belimumab therapy.
Conclusions
Belimumab has been shown to be useful in the treatment of serologically active, refractory SLE and is FDA-approved for use in SLE patients 5 years of age and older. Preliminary reports on both its efficacy and safety in the pediatric population are positive; however, its usefulness as a corticosteroid-sparing immunosuppressive agent in SLE patients with severe, active LN and/or active NPSLE remains unknown. This may limit its use in cSLE patients, as a large proportion of cSLE patients have renal and/or neuropsychiatric involvement. Belimumab may be most beneficial in cases of cSLE with seropositive, moderately active disease in which corticosteroids cannot be tapered or that are refractory to other immunosuppressive agents. We look forward to the results of the PLUTO study to further delineate long-term efficacy and safety, in addition to recommendations for the use of belimumab in the cSLE population.
Abbreviations
ACR, American College of Rheumatology; AE, adverse event; BAFF, B-cell activating factor; BILAG, British Isles Lupus Assessment Group; BLyS, B cell lymphocyte stimulator; CALIBRATE, Rituximab and belimumab for lupus nephritis; CNS, central nervous system; cSLE, childhood-onset systemic lupus erythematosus; dsDNA, double-stranded DNA; EMBRACE, Efficacy and safety of belimumab in Black race patients with systemic lupus erythematosus (SLE); EMEA, European Medicines Evaluation Agency; GFR, glomerular filtration rate; IV, intravenous; FDA, Food and Drug Administration; LN, lupus nephritis; NPSLE, neuropsychiatric lupus; PLUTO, Pediatric lupus trial of belimumab plus background standard therapy; PRINTO, Paediatric rheumatology international trials organisation; PML, progressive multifocal leukoencephalopathy; PGA, physician global assessment; SAE, serious adverse event; SELENA-SLEDAI, The Safety of Estrogens in Lupus Erythematosus: National Assessment version of the Systemic Lupus Erythematosus Disease Activity Index; SC, subcutaneous; SOC, standard of care; SRI, SLE responder index.
Acknowledgments
The authors thank Dr. B Anne Eberhard for her critical comments.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Choi J, Kim S, Craft J. The pathogenesis of systemic lupus erythematosus – an update. Curr Opin Immunol. 2012;24(6):651–657. doi:10.1016/j.coi.2012.10.004
2. D’Cruz D, Khamashta M, Hughes G. Systemic lupus erythematosus. Lancet. 2007;369(9561):587–596. doi:10.1016/S0140-6736(07)60279-7
3. Rahman A, Isenberg D. Systemic lupus erythematosus. N Engl J Med. 2008;358:929–939. doi:10.1056/NEJMra071297
4. Hochberg M. Updating the American College of Rheumatology revised criteria for the classification of systemic lupus erythematosus. Arthritis Rheum. 1997;40(9):1725. doi:10.1002/art.1780400928
5. Petri M, Orbai A, Alarcon G, et al. Derivation and validation of the systemic lupus international collaborating clinics classification criteria for systemic lupus erythematosus. Arthritis Rheum. 2012;64(8):2677–2686. doi:10.1002/art.34473
6. Aringer M, Costenbader K, Daikh D, et al. 2019 European League Against Rheumatism/American College of Rheumatology classification criteria for systemic lupus erythemtosus. Arthritis Rheum. 2019;71(9):1400–1412. doi:10.1002/art.40930
7. Costenbader K, Feskanich D, Stampfer M, Karlson EW. Reproductive and menopausal factors and risk of systemic lupus erythematosus in women. Arthritis Rheum. 2007;56(4):1251–1262. doi:10.1002/art.22510
8. Lahita RG. The role of sex hormones in systemic lupus erythematosus. Curr Opin Rheumatol. 1999;11(5):352–356. doi:10.1097/00002281-199909000-00005
9. Hui-Yuen JS, Imundo LF, Avitabile C, Kahn PJ, Eichenfeld AH, Levy DM. Early versus later onset childhood-onset systemic lupus erythematosus: clinical features, treatment, and outcome. Lupus. 2011;20(9):952–959. doi:10.1177/0961203311403022
10. Pineles D, Valente A, Warren B, Peterson MG, Lehman TJ, Moorthy N. Worldwide incidence and prevalence of pediatric onset systemic lupus erythematosus. Lupus. 2011;20(11):1182–1187. doi:10.1177/0961203311412096
11. Hersh AO, von Scheven E, Yazdany J, et al. Differences in long-term disease activity and treatment of adult patients with childhood- and adult-onset systemic lupus erythematosus. Arthritis Rheum. 2009;61(1):13–20. doi:10.1002/art.24091
12. Askanase A, Wallace D, Weisman M, et al. Use of pharmacogenetics, enzymatic phenotyping, and metabolic monitoring to guide treatment with azathioprine in patients with systemic lupus erythematosus. J Rheumatol. 2009;36(1):89–95. doi:10.3899/jrheum.070968
13. Carneiro J, Sato E. Double blind, randomized, placebo controlled clinical trial of methotrexate in systemic lupus erythematosus. J Rheumatol. 1999;26(6):1275–1279.
14. Urowitz MB, Gladman DD, Ibanez D, et al. Evolution of disease burden over five years in a multicenter inception systemic lupus erythematosus cohort. Arthritis Care Res. 2012;64(1):132–137. doi:10.1002/acr.20648
15. Hahn BH. Belimumab for systemic lupus erythematosus. N Engl J Med. 2013;368(16):1528–1535. doi:10.1056/NEJMct1207259
16. Nashi E, Wang Y, Diamond B. The role of B cells in lupus pathogenesis. Int J Biochem Cell Biol. 2010;42(4):543–550. doi:10.1016/j.biocel.2009.10.011
17. Baker KP, Edwards BM, Main SH, et al. Generation and characterization of Lymphostat-B, a human monoclonal antibody that antagonizes the bioactivities of B lymphocyte stimulator. Arthritis Rheum. 2003;48(11):3253–3265. doi:10.1002/art.11299
18. Vincent FB, Morand EF, Schneider P, Mackay F. The BAFF/APRIL system in SLE pathogenesis. Nat Rev Rheumatol. 2014;10(6):365–373. doi:10.1038/nrrheum.2014.33
19. Mackay F, Woodcock S, Lawton P. Mice transgenic for BAFF develop lymphocytic disorders along with autoimmune manifestations. J Exp Med. 1999;190(11):1697–1710. doi:10.1084/jem.190.11.1697
20. Figgett WA, Fairfax K, Vincent FB. The TACI receptor regulates T-cell-independent marginal zone B cell responses through innate activation-induced cell death. Immunity. 2013;39(3):573–583. doi:10.1016/j.immuni.2013.05.019
21. Zhang J, Roschke V, Baker KP. Cutting edge: a role for B lymphocyte stimulator in systemic lupus erythematosus. J Immunol. 2001;166(1):6–10. doi:10.4049/jimmunol.166.1.6
22. Petri M, Stohl W, Chatham W, et al. Association of plasma B lymphocyte stimulator levels and disease activity in systemic lupus erythematosus. Arthritis Rheum. 2008;58(8):2453–2459. doi:10.1002/art.23678
23. GlaxoSmithKline. Study of subcutaneous (SC) belimumab in pediatric participants with systemic lupus erythematosus (SLE). Available from: https://clinicaltrials.gov/ct2/show/NCT04179032. Clinicaltrials.gov identifier: NCT04179032.
24. Furie RA, Petri MA, Wallace DJ, et al. Novel evidence-based systemic lupus erythematosus responder index. Arthritis Rheum. 2009;61(9):1143–1151. doi:10.1002/art.24698
25. Navarra SV, Guzman RM, Gallacher AE, et al. Efficacy and safety of belimumab in patients with active systemic lupus erythematosus: a randomised, placebo-controlled, Phase 3 trial. Lancet. 2011;377(9767):721–731. doi:10.1016/S0140-6736(10)61354-2
26. Furie R, Petrie M, Zamani O, et al. A Phase III, randomized, placebo-controlled study of belimumab, a monoclonal antibody that inhibits B lymphocyte stimulator, in patients with systemic lupus erythematosus. Arthritis Rheum. 2011;63(12):3918–3930. doi:10.1002/art.30613
27. van Vollenhoven RF, Petri MA, Cervera R, et al. Belimumab in the treatment of systemic lupus erythematosus: high disease activity predictors of response. Ann Rheum Dis. 2012;71(8):1343–1349. doi:10.1136/annrheumdis-2011-200937
28. D’Cruz D, Maksimowicz-McKinnon K, Oates J, et al. Efficacy and safety of belimumab in patients of black race with systemic lupus erythematosus: results from the EMBRACE study. Lupus Sci Med. 2019;6(Suppl 1):A149–A150.
29. Human Genome Sciences Inc., a GSK Company. Efficacy and safety of belimumab in Black race patients with systemic lupus erythematosus (SLE) (EMBRACE). Available from: https://clinicaltrials.gov/ct2/show/NCT01632241. Clinicaltrials.gov identifier: NCT01632241.
30. National Institute of Allergy and Infectious Diseases (NIAID). Rituximab and belimumab for lupus nephritis (CALIBRATE). Available from: https://clinicaltrials.gov/ct2/show/NCT02260934. Clinicaltrials.gov identifier: NCT02260934.
31. Aranow C, Dall’Era M, Byron M, et al. Phase 2 trial of induction therapy with anti-cd20 (RITUXIMAB) followed by maintenance therapy with anti-baff (BELIMUMAB) in patients with active lupus nephritis. Ann Rheum Dis. 2018;77:690.
32. Human Genome Sciences, Inc. Efficacy and safety of belimumab in patients with active lupus nephritis (BLISS-LN). Available from: clinicaltrials.gov/c2/show/NCT01639339. Clinicaltrials.gov identifier: NCT01639339.
33. Stohl W, Schwarting A, Okada M, et al. Efficacy and safety of subcutaneous belimumab in systemic lupus erythematosus. Arthritis Rheum. 2017;69(5):1016–1027. doi:10.1002/art.40049
34. Doria A, Stohl W, Schwarting A, et al. Efficacy and safety of subcutaneous belimumab in anti-double-stranded DNA-positive, hypocomplementemic patients with systemic lupus erythematosus. Arthritis Rheum. 2018;70(8):1256–1264. doi:10.1002/art.40511
35. GlaxoSmithKine. Pediatric lupus trial of belimumab plus background standard therapy (PLUTO). Available from: clinicaltrials.gov/c2/show/NCT03949855. Clinicaltrials.gov identifier: NCT03949855.
36. Brunner HI, Abudo -mendoza C, Viola DO, et al. Efficacy and safety of intravenous belimumab in children with systemic lupus erythematosus [abstract]. Arthritis Rheum. 2018;70(Suppl 10).
37. Ruperto N, Abud-Mendoza C, Viola DO, et al. The Pluto study: intravenous belimumab in children with systemic lupus erythematosus [abstract]. Ann Rheum Dis. 2019;78(Supp 2):764–765.
38. Ginzler EM, Wallace DJ, Merrill JT, et al. Disease control and safety of belimumab plus standard therapy over 7 years in patients with systemic lupus erythematosus. J Rheumatol. 2014;41(2):300–309. doi:10.3899/jrheum.121368
39. Wallace DJ, Ginzler EM, Merrill JT, et al. Safety and efficacy of Belimumab plus standard therapy for up to thirteen years in patients with systemic lupus erythematosus. Arthritis Rheum. 2019;71(7):1125–1134. doi:10.1002/art.40861
40. Touma Z, Sayani A, Pineau CA, et al. Belimumab use, clinical outcomes and glucocorticoid reduction in patients with systemic lupus erythematosus receiving belimumab in clinical practice settings: results from the OBSErve Canada study. Rheumtaol Int. 2017;37(6):865–873. doi:10.1007/s00296-017-3682-9
41. Von Kempis J, Duetsch S, Reuschling N, et al. Clinical outcomes in patients with systemic lupus erythematosus treated with belimumab in clinical practice settings: a retrospective analysis of results from the OBSErve study in Switzerland. Swiss Med Wkly. 2019;149:w20022.
42. Schwarting A, Schroeder JO, Alexander T, et al. First real-world insights into belimumab use and outcomes in routine clinical care of systemic lupus erythematosus in Germany: results from the OBSErve Germany study. Rheumatol Ther. 2016;3(2):271–290. doi:10.1007/s40744-016-0047-x
43. Cortes J, Marras C, Andreu JL, et al. Evolution of patients with systemic lupus erythematosus treated with belimumab in clinical practice settings. Arthritis Rheum. 2014;66(Suppl 10):S291–S292.
44. Babini A, Garcia MA, Barreira JC, et al. Evaluation of use of belimumab in clinical practice settings: results in Argentina. Arthritis Rheum. 2016;68(Suppl 10).
45. Collins CE, Dall’Era M, Kan H, et al. Response to belimumab among patients with systemic lupus erythematosus in clinical practice settings: 24 month results from the OBSErve study in the USA. Lupus Sci Med. 2016;3(1):e000118. doi:10.1136/lupus-2015-000118
46. Hui-Yuen JS, Reddy A, Taylor J, et al. Safety and efficacy of belimumab to treat systemic lupus erythematosus in academic clinical practices. J Rheumatol. 2015;42(12):2288–2295. doi:10.3899/jrheum.150470
47. Iaccarino L, Bettio S, Reggia R, et al. Effects of belimumab on flare rate and expected damage progression in patients with active systemic lupus erythematosus. Arthritis Care Res. 2017;69(1):115–123. doi:10.1002/acr.22971
48. Iaccarino L, Andreoli L, Bocci EB, et al. Clinical predictors of response and discontinuation of belimumab in patients with systemic lupus erythematosus in real life setting. Results of a large, multicentric, nationwide study. J Autoimmun. 2018;86:1–8. doi:10.1016/j.jaut.2017.09.004
49. Yazdany J, Erkan D, Sanchez-Guerrero J, et al. Post-marketing experience with belimumab in US lupus centers: data from the lupus clinical trials consortium, INC (LCTC) National Patient Registry. Arthritis Rheum. 2013;65:S681.
50. Scheinberg M, de Melo FF, Bueno AN, Costa CM, de Azevedo Bahr ML, Reis ER. Belimumab for the treatment of corticosteroid-dependent systemic lupus erythematosus: from clinical trials to real-life experience after 1 year of use in 48 Brazilian patients. Clin Rheumatol. 2016;35(7):
51. Andreoli L, Reggia R, Pea L, et al. Belimumab for the treatment of refractory systemic lupus erythematosus: real-life experience in the first year of use in 18 Italian patients. Isr Med Assoc J. 2015;16(10):651–653.
52. Sthoeger Z, Lorber M, Tal Y, et al. Anti-BLyS treatment of 36 Israeli systemic lupus erythematosus patients. Isr Med Assoc J. 2017;19(1):45–48.
53. Merrill JT, Ginzler EM, Wallace DJ, et al. Long-term safety profile of belimumab plus standard therapy in patients with systemic lupus erythematosus. Arthritis Rheum. 2012;64(10):3364–3373. doi:10.1002/art.34564
54. Doria A, Bass D, Schwarting A, et al. A 6-month open-label extension study of the safety and efficacy of subcutaneous belimumab in patients with systemic lupus erythematosus. Lupus. 2018;27(9):1489–1498. doi:10.1177/0961203318777634
55. Fredericks CA, Kvam KA, Bear J, Crabtree GS, Josephson SA. A case of progressive multifocal leukoencephalopathy in a lupus patient treated with belimumab. Lupus. 2014;23(7):711–713. doi:10.1177/0961203314524292
56. Leblanc-Trudeau C, Masetto A, Bocti C. Progressive multifocal encephalopathy associated with belimumab in a patient with systemic lupus erythematosus. J Rheumatol. 2015;42(3):551–552. doi:10.3899/jrheum.140577
57. Raisch DW, Rafi JA, Chen C, Bennett CL. Detection of cases of progressive multifocal leukoencephalopathy associated with new biologicals and targeted cancer therapies from the FDA’s adverse event reporting system. Expert Opin Drug Saf. 2016;15(8):1003–1011. doi:10.1080/14740338.2016.1198775
58. Sheikh S, Scheinberg M, Cheng-Chung Wei J, et al. LB0012 Headline results for a phase 4, 52-week, randomised, double-blind, placebo-controlled study to assess adverse events of special interest (AESI) in adults with active, autoantibody-positive systemic lupus erythematosus (SLE) receiving belimumab. Ann Rheum Dis. 2019;78:266.
59. Tucker LB, Uribe AG, Fernandez M, et al. Adolescent onset of lupus results in more aggressive disease and worse outcomes: results of a nested matched case-control study within LUMINA, a multiethnic US cohort (LUMINA LVII). Lupus. 2008;17(4):314–322. doi:10.1177/0961203307087875
60. Knight AM, Trupin L, Katz P, Yelin E, Lawson EF. Depression risk in young adults with juvenile- and adult-onset lupus: twelve years of followup. Arthritis Care Res. 2018;70(3):475–480. doi:10.1002/acr.23290
61. Nino A, Bass DL, Eriksson G, et al. Efficacy and safety of intravenous belimumab in children with systemic lupus erythematosus: an across-trial comparison with the adult belimumab studies. [abstract]. Arthritis Rheum. 2019;71(suppl 10).
62. National Institute of Allergy and Infectious Diseases (NIAID). Belimumab with rituximab for primary membranous nephropathy. Available from: clinicaltrials.gov/ct2/show/NCT03949855.
63. Ginzler EM, Diamond HS, Weiner M, et al. A multicenter study of outcome in systemic lupus erythematosus. I. Entry variables as predictors of prognosis. Arthritis Rheum. 1982;25(6):601–611. doi:10.1002/art.1780250601
64. GlaxoSmithKline. A study to evaluate the efficacy and safety of belimumab administered in combination with rituximab to adult subjects with systemic lupus erythematosus (SLE)- BLISS-BELIEVE. Available from: https://clinicaltrials.gov/ct2/show/NCT03312907.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.